SINS Classification | NOMS Framework | Bilsky Grading | Surgical Management
- SINS score determines mechanical stability (0-6 stable, 7-12 consult, 13-18 unstable)
- Bilsky grading assesses epidural cord compression (0-3, 1c or higher needs evaluation)
- NOMS framework integrates Neurologic, Oncologic, Mechanical, Systemic factors
- Radioresistant tumors: RCC, thyroid, melanoma require SBRT not conventional RT
- Separation surgery enables post-op SBRT for high-grade epidural disease
- “SINS 13 or higher = unstable spine requiring surgical stabilization
- “Bilsky 1c or higher in radioresistant tumor = surgical evaluation
- “MESCC is oncological emergency - steroids immediately, surgery within 24-48h
- “Ambulatory status at presentation predicts neurological outcome
Calculate SINS in every viva - know the 6 components: Location (junctional=3), Pain (mechanical=3), Bone lesion (lytic=2), Alignment (subluxation=4), VB collapse (over 50%=3), Posterolateral (bilateral=3). Score 13 or higher = unstable requiring surgery.
Bilsky 1c is key threshold - cord contact without compression. In radioresistant tumors (RCC, thyroid, melanoma), Bilsky 1c or higher needs surgical evaluation for separation surgery to enable SBRT.
Systematic approach - N: Neurologic (Bilsky, deficit), O: Oncologic (radiosensitivity), M: Mechanical (SINS), S: Systemic (ECOG, life expectancy). Each component independently influences treatment decisions.
Know tumor types - Radiosensitive: lymphoma, myeloma, SCLC. Radioresistant: RCC, thyroid, melanoma, sarcoma, HCC. Radioresistant tumors have 30-40% local failure with conventional RT.
- Radiosensitive
- Lymphoma, myeloma, SCLC, seminoma
- Radioresistant
- RCC, thyroid, melanoma, sarcoma, HCC
- Radiosensitive
- Effective (60-70% local control)
- Radioresistant
- Poor (30-40% failure at 1 year)
- Radiosensitive
- No (unless progression)
- Radioresistant
- Yes for durable control
- Radiosensitive
- May observe/RT
- Radioresistant
- Separation surgery + SBRT
- Radiosensitive
- Not typically needed
- Radioresistant
- Essential for RCC, thyroid (hypervascular)
Overview and Epidemiology
Metastatic spine disease is the most common neoplasm of the spine, representing 90% of all spinal tumors. It significantly impacts quality of life through pain, neurological dysfunction, and mechanical instability.
Epidemiology:
- 10-30% of cancer patients develop spinal metastases
- Spine is the most common site of skeletal metastasis (Batson's plexus)
- Thoracic spine most common (70%), followed by lumbar (20%), cervical (10%)
- 5-10% of metastatic spine patients develop MESCC
- Breast, prostate, lung, thyroid, kidney (BPLTK) = 80% of cases
Distribution by Level:
- Frequency
- 70%
- Unique Considerations
- Kyphotic deformity, rib involvement
- Frequency
- 20%
- Unique Considerations
- Cauda equina, psoas involvement
- Frequency
- 10%
- Unique Considerations
- High morbidity, vertebral artery
- Frequency
- Rare
- Unique Considerations
- Pelvic organs, sacral nerve roots
Anatomical Pattern of Involvement:
- Vertebral body: 85% of lesions (anterior column)
- Pedicles: 60% involvement
- Posterior elements: 40% involvement
- Isolated posterior elements: Under 5%
The valveless paravertebral venous plexus allows direct retrograde tumor spread from pelvic/abdominal organs to spine, bypassing the pulmonary filter. This explains the high frequency of spine metastases from prostate, breast, and lung primaries.
Pathophysiology
Metastatic Cascade
The metastatic process to spine involves:
- Local invasion - Primary tumor invades local vasculature
- Intravasation - Tumor cells enter circulation
- Survival - Evade immune surveillance in bloodstream
- Extravasation - Exit at distant sites (Batson's plexus key role)
- Colonization - Establish micrometastasis in marrow
- Angiogenesis - Develop blood supply for growth
Bone Lesion Types
Osteolytic Metastases (Most Common)
Characterized by bone destruction via osteoclast activation:
- Mechanism: Tumor secretes PTHrP, IL-6, IL-11 activating osteoclasts
- Radiographic appearance: Punched-out lesions, cortical destruction
- Common primaries: Lung, thyroid, renal cell, melanoma
- SINS implication: Score 2 (higher instability risk)
- Pathological fracture: High risk with over 50% VB involvement
Lytic lesions cause rapid structural compromise and high fracture risk.
Primary Tumor Characteristics
- Lesion Type
- Mixed/Lytic
- Vascularity
- Moderate
- Radiosensitivity
- Moderate
- Median Survival
- 24-36 months
- Lesion Type
- Blastic
- Vascularity
- Low
- Radiosensitivity
- Moderate
- Median Survival
- 24-36 months
- Lesion Type
- Lytic
- Vascularity
- Moderate
- Radiosensitivity
- Radiosensitive
- Median Survival
- 6-12 months
- Lesion Type
- Lytic
- Vascularity
- HIGH
- Radiosensitivity
- Radioresistant
- Median Survival
- 12-24 months
- Lesion Type
- Lytic
- Vascularity
- HIGH
- Radiosensitivity
- Radioresistant
- Median Survival
- 24-48 months
- Lesion Type
- Lytic
- Vascularity
- Low
- Radiosensitivity
- Radiosensitive
- Median Survival
- 24-36 months
- Lesion Type
- Lytic
- Vascularity
- Moderate
- Radiosensitivity
- Radioresistant
- Median Survival
- 6-12 months
RCC and thyroid metastases are highly vascular. Preoperative embolization is essential to reduce intraoperative blood loss. Consider embolizing 24-48 hours before surgery when operatively managing these tumors.
Classification Systems
SINS - Spinal Instability Neoplastic Score
SINS Score Components (Maximum 18 points):
- Score
- Description
- Score
- 3
- Description
- Highest instability risk
- Score
- 2
- Description
- Moderate risk
- Score
- 1
- Description
- Lower risk (rib cage support)
- Score
- 0
- Description
- Minimal risk
- Score
- Description
- Score
- 3
- Description
- Suggests structural compromise
- Score
- 1
- Description
- Less concerning
- Score
- 0
- Description
- Favorable
- Score
- Description
- Score
- 2
- Description
- Highest fracture risk
- Score
- 1
- Description
- Intermediate
- Score
- 0
- Description
- More stable
- Score
- Description
- Score
- 4
- Description
- Critical instability
- Score
- 2
- Description
- Significant
- Score
- 0
- Description
- Favorable
- Score
- Description
- Score
- 3
- Description
- Severe compromise
- Score
- 2
- Description
- Moderate
- Score
- 1
- Description
- At risk
- Score
- 0
- Description
- Intact
- Score
- Description
- Score
- 3
- Description
- Highest instability
- Score
- 1
- Description
- Moderate
- Score
- 0
- Description
- Stable
SINS Interpretation:
- 0-6: Stable - no surgical consultation required
- 7-12: Potentially unstable - surgical consultation recommended
- 13-18: Unstable - surgical stabilization required
Bilsky Epidural Compression Scale
- Description
- Bone-only disease
- Management
- Radiation if indicated
- Description
- Epidural impingement, no thecal deformation
- Management
- Radiation alone
- Description
- Thecal sac deformed, no cord contact
- Management
- Radiation alone
- Description
- Cord contact without compression
- Management
- Surgical evaluation
- Description
- Cord compression, CSF visible
- Management
- Surgical decompression
- Description
- Cord compression, no CSF (circumferential)
- Management
- Urgent surgery
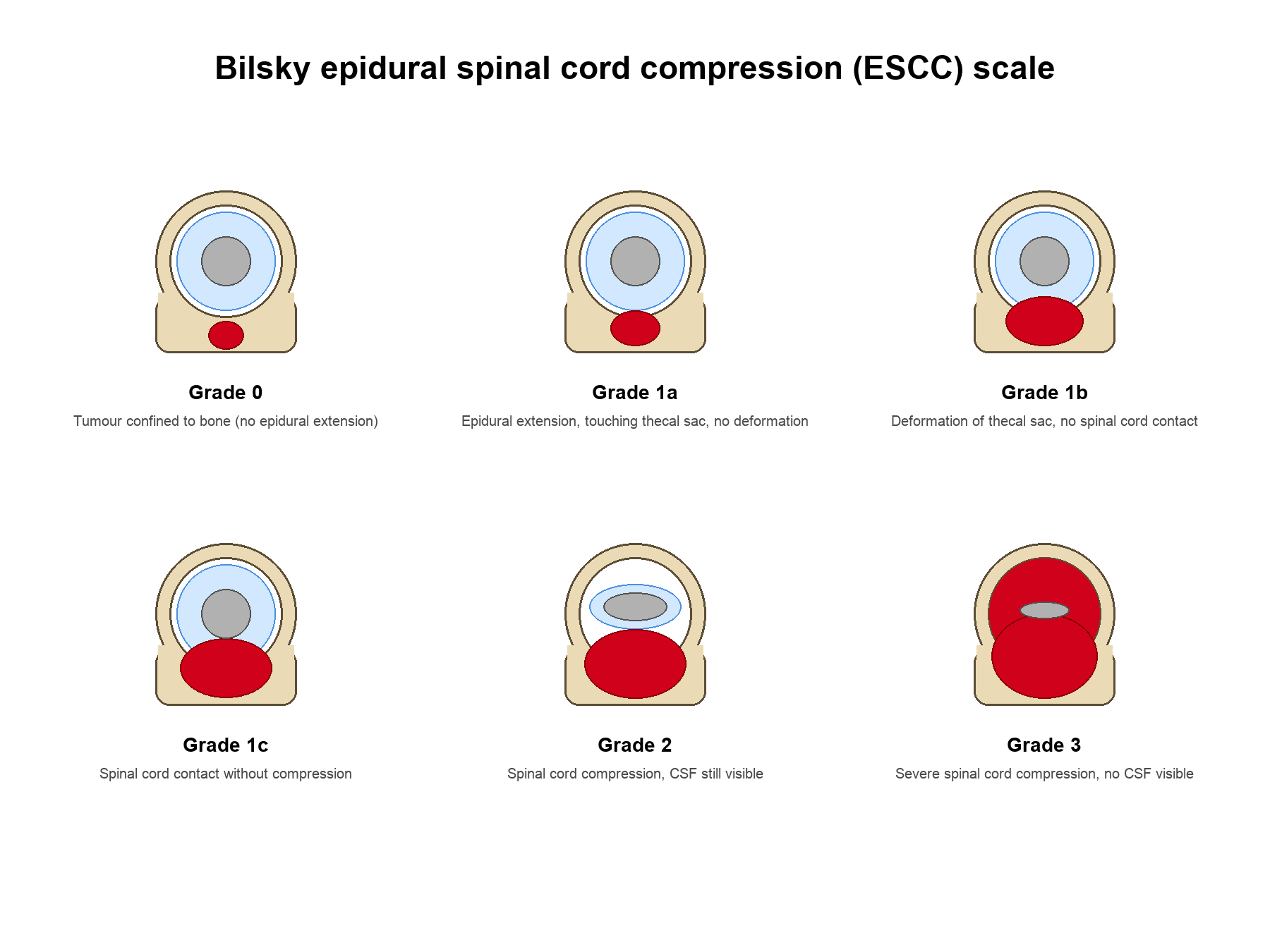
Bilsky 1c is the critical decision point. In radioresistant tumors (RCC, thyroid, melanoma), Bilsky 1c or higher requires surgical evaluation for separation surgery to enable safe delivery of SBRT.
NOMS Decision Framework
N - Neurologic Assessment
Evaluates neural compression and functional status:
- Grade 0-1b: No significant neural compromise
- Grade 1c-3: Progressive compression requiring intervention
- Frankel/ASIA Grade (A-E)
- Ambulatory status (critical prognostic factor)
- Bladder/bowel function
- Rapid progression under 48 hours = urgent decompression
- Motor deficit under 48 hours = best surgical outcomes
- Complete paralysis over 24-48 hours = poor recovery
Ambulatory status at presentation is strongest predictor of outcome.
Clinical Presentation
History
- Mechanical pain: Worse with movement - suggests instability (SINS +3)
- Biological pain: Night pain, constant, progressive - tumor burden
- Radicular pain: Dermatomal distribution - nerve root compression
- Myelopathic symptoms: Gait difficulty, coordination problems
- Age over 50 with new back pain
- Known cancer history (even remote)
- Unexplained weight loss (over 10% in 6 months)
- Night pain unrelieved by position
- Progressive neurological symptoms
- Pain unresponsive to conservative treatment
Physical Examination
- Motor: Myotomal testing, document Frankel/ASIA grade
- Sensory: Dermatomal assessment, sensory level
- Reflexes: Hyperreflexia (UMN) vs hyporeflexia (LMN)
- Long tract signs: Hoffman's, Babinski, clonus
- Gait: Ambulatory status is critical prognostic factor
- Tenderness over involved levels
- Palpable step-off or deformity
- Paraspinal muscle spasm
MESCC - Oncological Emergency
Metastatic Epidural Spinal Cord Compression:
- 5-10% of cancer patients develop MESCC
- Neurological deterioration can be rapid (hours to days)
- Time to treatment = neurological outcome
MESCC is an oncological emergency. Patients ambulatory at presentation have 75-90% chance of remaining ambulatory with treatment. Non-ambulatory patients have only 10-30% chance of regaining ambulation. Start steroids immediately, expedite imaging and surgical consultation.
Investigations
Laboratory Studies
Essential Tests:
- CBC, CMP, LFTs (baseline, nutritional status)
- Calcium (hypercalcemia common in bone mets)
- Tumor markers (PSA, CEA, CA 19-9, AFP)
- SPEP/UPEP (exclude myeloma)
- HIV (if unknown primary)
Imaging
- Sensitivity: 98.5% for osseous metastases
- Specificity: 98.9%
- Sequences: T1, T2, STIR, post-gadolinium
- Findings:
- T1 hypointense (marrow replacement)
- T2 hyperintense (tumor/edema)
- Gadolinium enhancement
- Epidural extension (Bilsky grading)
- Bone architecture assessment
- Cortical destruction visualization
- Surgical planning (pedicle trajectory)
- CT-guided biopsy
- Limited sensitivity (30-50% bone loss required)
- Alignment assessment
- Standing views for sagittal balance
- Bone scan: Sensitive but non-specific
- PET-CT: Staging, treatment response
- SPECT: Improved localization
Biopsy
Indications:
- Unknown primary
- Solitary lesion (exclude primary tumor)
- Atypical imaging features
- No other accessible biopsy site
In a patient with no known primary or a solitary lesion, obtain a tissue diagnosis (CT-guided or open) before instrumented surgery or radiotherapy. Operating on or irradiating an undiagnosed lesion can compromise a primary bone tumour (e.g. plasmacytoma, lymphoma, chordoma) that would have a different, potentially curative treatment plan.
Differential Diagnosis
A destructive or marrow-replacing vertebral lesion is not always a carcinoma metastasis. The key differentials and discriminating features are:
- Typical clue
- Known primary, age over 50, multiple levels
- Discriminating feature
- Multiplicity; pedicle ('winking owl') destruction; T1 marrow replacement
- Typical clue
- Diffuse lytic 'punched-out' lesions, anaemia, renal impairment
- Discriminating feature
- SPEP/UPEP and serum free light chains positive; bone scan often COLD
- Typical clue
- Bulky soft-tissue mass, relatively preserved bone outline
- Discriminating feature
- Encasing 'wrap-around' epidural mass; markedly radiosensitive/chemosensitive
- Typical clue
- Elderly, no destruction, fluid sign / preserved posterior cortex
- Discriminating feature
- Retropulsion without soft tissue mass; benign marrow on chemical-shift MRI
- Typical clue
- Fever, raised CRP, endplate and disc destruction
- Discriminating feature
- DISC involvement (spared by most tumours); paraspinal/psoas abscess in TB
- Typical clue
- Solitary, younger patient, characteristic location (sacrum/clivus for chordoma)
- Discriminating feature
- Biopsy mandatory before any intervention; en bloc resection may be curative
Metastases characteristically spare the intervertebral disc and may destroy a single pedicle (the 'winking owl' sign on AP radiograph), whereas infection crosses the disc space and destroys adjacent endplates. Myeloma is the classic lesion that is lytic on radiograph yet cold (negative) on technetium bone scan because it lacks osteoblastic reaction.

Management
Corticosteroid Protocol
Dexamethasone for MESCC:
- Indication
- Initial presentation
- Indication
- Maintenance until definitive Rx (NICE-recommended regimen)
- Indication
- Historical/selected rapid progression - largely abandoned due to higher toxicity without clear benefit
Mechanism: Reduces vasogenic edema, possible tumoricidal effect on lymphoma. Co-prescribe gastric protection and monitor glucose; taper once definitive treatment is established.
Bone-Modifying Agents
Every patient with solid-tumour bone metastases (and myeloma) should be considered for a bone-modifying agent to reduce skeletal-related events (SREs: pathological fracture, cord compression, need for radiotherapy or surgery to bone, and hypercalcaemia):
- Bisphosphonates (zoledronic acid) - inhibit osteoclast-mediated resorption; reduce SREs across solid tumours and myeloma; renally cleared, so avoid or dose-reduce in renal impairment.
- Denosumab - a monoclonal RANKL inhibitor, at least as effective as zoledronic acid for SRE reduction, given subcutaneously and not renally cleared, but its effect is reversible.
- Both require a dental review before starting and calcium plus vitamin D supplementation.
Know the three complications examiners probe: osteonecrosis of the jaw (ONJ) - hence a dental check and good oral hygiene before starting; atypical (subtrochanteric) femoral fractures with prolonged use - ask about prodromal thigh pain; and hypocalcaemia - always replete calcium and vitamin D first. Denosumab is preferred in renal impairment (not renally cleared) but its effect is reversible, so abrupt cessation causes a rebound of bone turnover and a risk of multiple vertebral fractures - transition to a bisphosphonate if stopping.
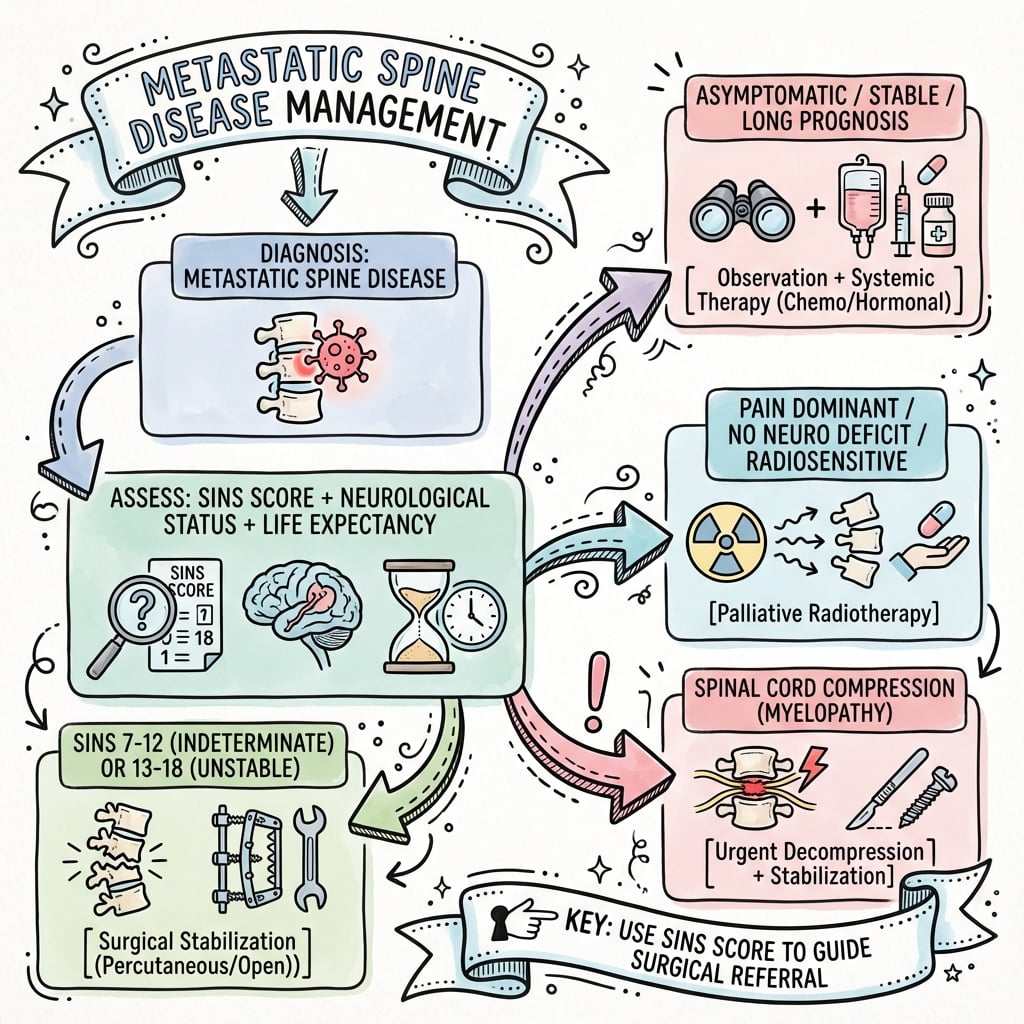
Non-Operative Management
Indications:
- SINS 0-6 (stable)
- Bilsky 0-1b with radiosensitive tumor
- Poor surgical candidate (ECOG 3-4)
- Life expectancy under 3 months
External Beam Radiation (cEBRT)
- 30 Gy in 10 fractions (standard)
- 20 Gy in 5 fractions (hypofractionated)
- 8 Gy single fraction (palliation)
- Pain relief: 70-80%
- Motor improvement: 40-60%
- Local control (radiosensitive): 60-70%
- 30-40% failure for radioresistant tumors
- Dose constraint near spinal cord
cEBRT effective for radiosensitive tumors and pain palliation.
Two landmark RCTs frame the radiotherapy discussion. SCORAD (Hoskin, JAMA 2019) showed single 8 Gy is a reasonable convenient option versus 20 Gy in 5 fractions for MSCC (ambulatory benefit broadly similar; high early mortality). NRG/RTOG 0631 (Ryu, JAMA Oncol 2023) found that spine SRS did NOT improve patient-reported pain at 3 months over single-fraction 8 Gy cEBRT (41% vs 60%). The take-home: for simple pain palliation in radiosensitive disease, conventional EBRT suffices; reserve SRS/SBRT for radioresistant histology, oligometastatic disease, re-irradiation, or postoperative durable local control.
Surgical Management
- Mechanical instability (SINS 13-18)
- High-grade ESCC (Bilsky 2-3) with deficit
- Radioresistant tumor with Bilsky 1c or higher
- Progressive deficit despite radiation
- Pathological fracture with canal compromise
- Tissue diagnosis needed
- Create 2-3mm gap around cord for safe high-dose SBRT/SRS
- Posterior approach with instrumentation
- Circumferential decompression (not gross total / en bloc resection)
- Post-op SBRT typically within 2-4 weeks
- 1-year local control ~84% overall in the Laufer series, rising to ~96% with high-dose hypofractionated SRS (24-30 Gy in 3 fractions)
Separation surgery (palliative decompression plus SBRT) is the default for most epidural metastases, but a small group warrants aggressive en bloc (total) spondylectomy with wide or marginal margins - the oncological resection more usually reserved for primary tumours. Consider it for the fit patient (good ECOG, long predicted survival, Tomita 2-3) with a solitary spinal metastasis, a controlled or absent primary, and no visceral metastases, especially from a biologically favourable, often radioresistant primary (renal cell, thyroid, or a solitary breast metastasis) where durable local control may change the disease course. The benefit (lower local recurrence, a possible survival advantage) is weighed against the high morbidity and major blood loss of total spondylectomy, so it remains the exception, justified only when prognosis is genuinely long. This is the answer to "what if she had a solitary metastasis with no visceral disease?" - shift from palliation toward oncological resection.
- Posterior: Most common, extensile, pedicle screws
- Anterior: Corpectomy, cervical plating
- MIS: Percutaneous screws, vertebroplasty
- Minimum 2 levels above/below lesion
- Cement augmentation in poor bone
- Expandable cages for anterior column
Complications
Surgical Complications
- Wound infection: 5-10%
- DVT/PE: 5-15%
- Medical complications: 10-20%
- 30-day mortality: 5-10%
- Hardware failure: 5-10%
- Adjacent level fracture: 5-15%
- Neurological deterioration: 2-5%
- CSF leak: 2-5%
- Higher risk with prior radiation
- May require plastic surgery
Radiation Complications
- Radiation dermatitis
- Esophagitis (thoracic)
- Nausea, fatigue
- Radiation myelopathy (rare with modern techniques)
- Vertebral compression fracture (10-15% post-SBRT)
Disease Progression
Local Recurrence:
- cEBRT alone (radioresistant): 30-40% at 1 year
- SBRT: 5-15% at 1 year
- Separation surgery + SBRT: 5-10% at 1 year
Guidelines, Registries & Global Practice
Global Epidemiology
Spine is the most common site of skeletal metastasis worldwide, and the spine is involved in the majority of patients with bone metastases at autopsy. Roughly 10-30% of cancer patients develop clinically relevant spinal metastases during their disease, and around 5-10% develop metastatic epidural spinal cord compression (MESCC). As cancer survival improves globally with modern systemic therapy, the population living with spinal metastases is growing, increasing demand for spine oncology services. Across high-income health systems the dominant primaries are consistent: in the SCORAD cohort (UK and Australia) prostate (44%), lung (19%) and breast (12%) accounted for most MSCC, mirroring the BPLTK pattern (Hoskin, JAMA 2019, PMID 31794625).
Side-by-Side Guidance
- Core recommendation
- Treat suspected MSCC as an emergency; whole-spine MRI within 24h, dexamethasone 16 mg/day, definitive treatment within 24h of diagnosis; surgery for suitable patients then radiotherapy
- Evidence basis
- Underpinned by Patchell RCT (Level I)
- Core recommendation
- Integrate Neurologic (Bilsky), Oncologic (radiosensitivity), Mechanical (SINS), Systemic status to choose RT, SRS or separation surgery + SRS
- Evidence basis
- Expert synthesis (Barzilai, JCO 2017)
- Core recommendation
- Use SINS to trigger surgical consultation (score 7 or higher) and the Bilsky ESCC scale to grade compression
- Evidence basis
- Consensus + reliability data (Fisher 2010; Fourney 2011)
- Core recommendation
- Single-fraction 8 Gy cEBRT for simple pain palliation/short prognosis; reserve SBRT/SRS for radioresistant histology, oligometastases, re-irradiation or postoperative durable control
- Evidence basis
- SCORAD and RTOG 0631 (Level I)
- Core recommendation
- Zoledronic acid or denosumab to reduce skeletal-related events in solid-tumour bone metastases and myeloma, with dental review and calcium/vitamin D
- Evidence basis
- RCT evidence
Registry and Trial Evidence
There is no single dominant international spinal-metastasis registry equivalent to arthroplasty registries; the evidence base rests on landmark RCTs (Patchell 2005, SCORAD 2019, RTOG 0631 2023) plus large institutional cohorts (e.g. the Laufer separation-surgery series) and prospective prognostic-score validation (Tokuhashi, Tomita). The Global Spine Tumour Study Group and AO Spine Knowledge Forum Tumour have driven prospective multinational data collection on surgical outcomes, quality of life and prognostic modelling, increasingly favouring patient-reported outcomes over survival alone.
Practice Variation
Real-world practice varies with access to technology and multidisciplinary infrastructure. SBRT/SRS and separation surgery are concentrated in tertiary centres with image-guided radiotherapy and spinal navigation; in lower-resource settings conventional EBRT and posterior decompression-stabilisation remain the mainstay. Timeliness also varies: NICE-style emergency pathways with 24-hour MRI access are not universally available, and delayed diagnosis remains a major determinant of poorer ambulatory outcome globally.
MCQ Practice Points
Q: What is the SINS (Spinal Instability Neoplastic Score) threshold for surgical stabilization? A: SINS 7-12 is indeterminate (requires surgical consultation); SINS greater than 12 indicates instability requiring surgical stabilization. SINS assesses location, pain, lesion type, alignment, vertebral body collapse, and posterolateral element involvement.
Q: What are the components of the NOMS framework for metastatic spine treatment decisions? A: N = Neurologic status, O = Oncologic (tumor radiosensitivity and systemic disease burden), M = Mechanical instability (SINS), S = Systemic disease and medical comorbidities. This framework guides the choice between surgery, radiation, or conservative management.
Q: What is the Tomita scoring system used for? A: Predicting survival and guiding surgical extent in metastatic spine disease. Scores 2-3 favor wide/marginal excision, 4-5 favor marginal/intralesional surgery, 6-7 favor palliative surgery, and 8-10 suggest non-operative care. Factors include primary tumor type, visceral metastases, and bone metastases number.
Q: What is separation surgery in metastatic spine disease? A: Decompression and stabilization to create a 2-3mm gap between tumor and spinal cord, allowing safe delivery of high-dose stereotactic body radiotherapy (SBRT). It is not an oncologic resection but enables effective radiation while protecting neural structures.
At a Glance
Metastatic spine disease affects 10-30% of cancer patients, with 70% occurring in the thoracic spine due to red marrow distribution. The SINS score (6 components: location, pain, lesion type, alignment, vertebral body collapse, posterolateral involvement) determines mechanical stability—scores ≥13 require surgical stabilization. The NOMS framework integrates Neurologic (Bilsky grading), Oncologic (radiosensitivity), Mechanical (SINS), and Systemic factors for treatment decisions. BPLTK primaries (Breast, Prostate, Lung, Thyroid, Kidney) account for 80% of cases. Radioresistant tumors (RCC, thyroid, melanoma) require separation surgery with SBRT rather than conventional radiation for durable local control.
SINSSINS Score Components
Hook:SINS-CP: Score 0-6 stable, 7-12 consult, 13-18 unstable (requires surgery)
NOMSNOMS Framework
Hook:Never Operate without Multidisciplinary Support - integrate all factors
BPLTKBPLTK Primary Tumors
Hook:BPLTK account for 80% of all spine metastases
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old man with metastatic prostate cancer has T8 vertebral body lesion with 30% collapse, no epidural extension, 4 weeks of mechanical back pain. No neurological symptoms.”
“The same patient returns 3 months later with 2 days of progressive leg weakness. Examination: 3/5 bilateral LE power, hyperreflexia, upgoing plantars. MRI shows T8 with Bilsky grade 2.”
“A 62-year-old woman with metastatic RCC has L2 lytic lesion, 60% collapse, kyphotic deformity, Bilsky 1c. Intact neurology. Calculate SINS and outline management.”
“A 75-year-old with ECOG 3, multiple visceral metastases from lung cancer, life expectancy 6-8 weeks. Severe mechanical back pain from L3 pathological fracture. SINS 10, Bilsky 0.”
SINS Score Components
- Location: Junctional=3, Mobile=2, Semi-rigid=1, Rigid=0
- Pain: Mechanical=3, Non-mechanical=1, None=0
- Bone: Lytic=2, Mixed=1, Blastic=0
- Alignment: Subluxation=4, Deformity=2, Normal=0
- VB Collapse: Over 50%=3, Under 50%=2, Over 50% involved=1, None=0
- Posterolateral: Bilateral=3, Unilateral=1, None=0
- INTERPRETATION: 0-6 stable, 7-12 consult, 13-18 unstable
Bilsky Grading
- Grade 0: Bone only
- Grade 1a: Epidural impingement
- Grade 1b: Thecal deformation, no cord contact
- Grade 1c: Cord contact (KEY THRESHOLD)
- Grade 2: Cord compression, CSF visible
- Grade 3: Circumferential compression, no CSF
- 1c or higher in radioresistant tumor = surgery
NOMS Framework
- N = Neurologic: Bilsky grade, deficit, ambulatory status
- O = Oncologic: Radiosensitivity determines RT approach
- M = Mechanical: SINS score guides stabilization
- S = Systemic: ECOG, life expectancy
- Radiosensitive: Lymphoma, myeloma, SCLC
- Radioresistant: RCC, thyroid, melanoma, sarcoma
Surgical Indications
- SINS 13-18 (unstable) - even without neurology
- Bilsky 2-3 with neurological deficit
- Bilsky 1c or higher in radioresistant tumor
- Progressive deficit despite radiation
- Pathological fracture with instability
Key Numbers
- Dexamethasone: 10mg bolus then 4mg q6h
- SBRT/SRS: 24 Gy single or 24-30 Gy/3# or 30-35 Gy/5#
- Pedicle screws: Minimum 2 levels above/below
- Patchell (Lancet 2005): Surgery+RT 84% ambulatory vs RT 57%
- RTOG 0631 (JAMA Oncol 2023): cEBRT 60.5% vs SRS 41.3% pain response - SRS not superior for pain
- Separation surgery + high-dose SRS: ~96% 1-year local control
Examiner Favorites
- Calculate SINS explicitly in viva
- MESCC = emergency - steroids first
- RCC and thyroid need embolization
- Separation surgery = decompression for SBRT
- Match treatment to life expectancy
Evidence Base
Patchell Trial - Direct Decompressive Surgery + RT vs RT Alone
- Multicentre RCT, 101 patients with MESCC (single compressive site); both arms received 30 Gy in 10 fractions
- Ambulatory after treatment: surgery + RT 84% (42/50) vs RT alone 57% (29/51); OR 6.2 (95% CI 2.0-19.8), p=0.001
- Retained ambulation longer: median 122 vs 13 days (p=0.003)
- Of those non-ambulatory at entry, 62% regained walking with surgery vs 19% with RT (p=0.01); reduced steroid and opioid need
- Excluded radiosensitive tumours (lymphoma, myeloma, germ cell) and total paraplegia over 48h
NRG/RTOG 0631 - Spine SRS vs Conventional EBRT for Pain
- Phase 3 RCT, 339 analysed; 1-3 vertebral metastases randomised 2:1 to SRS (single 16-18 Gy) vs cEBRT (single 8 Gy)
- Primary endpoint (patient-reported pain response at 3 months) FAVOURED cEBRT: 41.3% SRS vs 60.5% cEBRT (difference -19 points, 95% CI -32.9 to -5.5; 2-sided p=0.01)
- Superiority of SRS for pain was NOT demonstrated; no difference in acute/late toxicity
- Vertebral compression fracture at 24 months: 19.5% SRS vs 21.6% cEBRT (p=0.59); no spinal cord complications at 2 years
SINS - Development and Expert Consensus (Spine Oncology Study Group)
- Systematic review plus modified Delphi consensus from the Spine Oncology Study Group
- Six weighted components: location, pain, bone lesion quality, alignment, vertebral body collapse, posterolateral involvement (0-18)
- Categories: 0-6 stable, 7-12 potentially unstable, 13-18 unstable
- Designed to flag when patients warrant surgical consultation, not to mandate surgery
SINS - Reliability and Validity
- 30 spinal tumour cases scored twice by Spine Oncology Study Group members
- Total-score reliability near-perfect: ICC 0.846 (inter-observer) and 0.886 (intra-observer)
- Predictive validity vs consensus gold standard: kappa 0.712
- Sensitivity 95.7% and specificity 79.5% for detecting potentially unstable or unstable lesions
Separation Surgery + Postoperative Stereotactic Radiosurgery
- Retrospective series of 186 patients with high-grade ESCC treated by decompression, instrumentation and postoperative SRS
- Overall cumulative local progression 16.4% at 1 year (i.e. ~84% local control)
- High-dose hypofractionated SRS (24-30 Gy in 3 fractions) gave 1-year local progression of only 4.1% vs 22.6% for low-dose hypofractionated SRS
- Local control was independent of tumour radiosensitivity, ESCC grade and extent of decompression
SCORAD - Single vs Multifraction RT for Spinal Cord Compression
- Noninferiority RCT in 42 UK and 5 Australian centres; 686 patients with MSCC and life expectancy over 8 weeks
- Single 8 Gy vs 20 Gy in 5 fractions; ambulatory grade 1-2 at week 8: 69.3% vs 72.7% (difference -3.5%)
- Noninferiority of single fraction at 8 weeks was NOT formally met (p=0.06) but the CI overlapped the margin; noninferiority was met at weeks 1, 4 and 12
- No survival difference (12-week survival 50% vs 55%); roughly half the cohort died before the 8-week assessment
NOMS Decision Framework
- Integrative framework synthesising evidence across Neurologic, Oncologic, Mechanical and Systemic domains
- Incorporates spinal SRS, allowing ablative dose delivery and a shift toward less aggressive, often minimally invasive surgery
- Couples Bilsky ESCC grade with tumour radiosensitivity to choose RT alone, SRS or separation surgery + SRS
- Emphasises multidisciplinary decision-making rather than a fixed algorithm
Tomita Prognostic Score and Surgical Strategy
- Prognostic score (2-10) from three factors: grade of malignancy, visceral metastases, and number of bone metastases
- Score 2-3 wide/marginal excision; 4-5 marginal/intralesional; 6-7 palliative surgery; 8-10 supportive care
- Mean survival: 38.2 months after wide/marginal excision vs 5.3 months with terminal care in the original cohort
- Lower Tomita score indicates a better prognosis (opposite direction to Tokuhashi)
Revised Tokuhashi Prognostic Score
- Six parameters, each 0-5, total 0-15 (general condition, extraspinal mets, vertebrae involved, visceral mets, primary site, neurology)
- Score 0-8 predicts under 6 months (conservative/palliative); 12-15 predicts 1 year or more (excision justified)
- Prospective consistency between predicted and actual survival 86.4% (n=118)
- Higher Tokuhashi score indicates a better prognosis (opposite direction to Tomita)
References
- Fisher CG, DiPaola CP, Ryken TC, et al. A novel classification system for spinal instability in neoplastic disease: an evidence-based approach and expert consensus from the Spine Oncology Study Group. Spine (Phila Pa 1976). 2010;35(22):E1221-9. PMID 20562730. doi:10.1097/BRS.0b013e3181e16ae2
- Fourney DR, Frangou EM, Ryken TC, et al. Spinal instability neoplastic score: an analysis of reliability and validity from the Spine Oncology Study Group. J Clin Oncol. 2011;29(22):3072-7. PMID 21709187. doi:10.1200/JCO.2010.34.3897
- Bilsky MH, Laufer I, Fourney DR, et al. Reliability analysis of the epidural spinal cord compression scale. J Neurosurg Spine. 2010;13(3):324-8. PMID 20809724. doi:10.3171/2010.3.SPINE09459
- Patchell RA, Tibbs PA, Regine WF, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: a randomised trial. Lancet. 2005;366(9486):643-8. PMID 16112300. doi:10.1016/S0140-6736(05)66954-1
- Laufer I, Iorgulescu JB, Chapman T, et al. Local disease control for spinal metastases following "separation surgery" and adjuvant hypofractionated or high-dose single-fraction stereotactic radiosurgery. J Neurosurg Spine. 2013;18(3):207-14. PMID 23339593. doi:10.3171/2012.11.SPINE12111
- Ryu S, Deshmukh S, Timmerman RD, et al. Stereotactic radiosurgery vs conventional radiotherapy for localized vertebral metastases of the spine: phase 3 results of NRG Oncology/RTOG 0631 randomized clinical trial. JAMA Oncol. 2023;9(6):800-7. PMID 37079324. doi:10.1001/jamaoncol.2023.0356
- Hoskin PJ, Hopkins K, Misra V, et al. Effect of single-fraction vs multifraction radiotherapy on ambulatory status among patients with spinal canal compression from metastatic cancer: the SCORAD randomized clinical trial. JAMA. 2019;322(21):2084-94. PMID 31794625. doi:10.1001/jama.2019.17913
- Barzilai O, Laufer I, Yamada Y, et al. Integrating evidence-based medicine for treatment of spinal metastases into a decision framework: neurologic, oncologic, mechanical stability, and systemic disease. J Clin Oncol. 2017;35(21):2419-27. PMID 28640703. doi:10.1200/JCO.2017.72.7362
- Tomita K, Kawahara N, Kobayashi T, et al. Surgical strategy for spinal metastases. Spine (Phila Pa 1976). 2001;26(3):298-306. PMID 11224867. doi:10.1097/00007632-200102010-00016
- Tokuhashi Y, Matsuzaki H, Oda H, et al. A revised scoring system for preoperative evaluation of metastatic spine tumor prognosis. Spine (Phila Pa 1976). 2005;30(19):2186-91. PMID 16205345. doi:10.1097/01.brs.0000180401.06919.a5