Basic Calcium Phosphate | Apatite-Associated Destructive Arthritis | Elderly Women
- Milwaukee shoulder = basic calcium phosphate (BCP / hydroxyapatite) crystal-driven rapidly destructive arthropathy - a distinct entity from monosodium urate (gout) and calcium pyrophosphate (CPPD)
- Classic patient: elderly woman, dominant shoulder, large recurrent effusion, weakness and a massive rotator cuff tear
- The effusion is large, often bloody, but NON-inflammatory (low white cell count) - this surprises candidates
- BCP crystals are tiny and NON-birefringent - they are MISSED on routine polarised microscopy; use alizarin red staining or electron microscopy
- Crystals drive joint destruction by stimulating synoviocytes to release proteases (collagenases / matrix metalloproteinases), not by classic acute inflammation
- “BCP crystals are non-birefringent - a 'negative' polarised microscopy does NOT exclude crystal disease
- “Alizarin red S stains calcium - a cheap, sensitive screen for BCP in synovial fluid
- “A large bloody shoulder effusion with a low cell count in an elderly woman is Milwaukee until proven otherwise
- “Always exclude SEPTIC arthritis first - aspirate and send for Gram stain, culture and cell count
BCP crystals are non-birefringent and individually below the resolution of light microscopy. A standard polarised microscopy report of "no crystals" does NOT exclude Milwaukee shoulder. Use alizarin red S staining (screens for any calcium) or electron microscopy / X-ray diffraction to confirm. This is the single most-tested trap.
The shoulder effusion is large and frequently blood-stained, yet the synovial white cell count is low (typically a few hundred to low thousands, mononuclear-predominant). A bloody, low-cell-count effusion is the classic picture - very different from the high neutrophil counts of gout, CPPD or sepsis.
A hot, swollen, destroyed shoulder in an elderly patient is septic arthritis until proven otherwise. Aspirate and send for Gram stain, culture and cell count before attributing destruction to crystals. Crystal disease and infection can coexist.
Mechanical cuff tear arthropathy is end-stage failure of a massive tear with superior migration and acetabularization. Milwaukee shoulder is the crystal-driven, enzymatically destructive variant - the same final radiograph, but a different driving mechanism (BCP crystals + protease release). Examiners reward naming the crystal pathway.
Overview and Epidemiology
Milwaukee shoulder (also called apatite-associated destructive arthritis or basic calcium phosphate crystal arthropathy) is a rapidly destructive arthropathy of the shoulder driven by the deposition and shedding of basic calcium phosphate (BCP) crystals - principally hydroxyapatite, with carbonate-substituted apatite and octacalcium phosphate. It was characterised in the early 1980s in Milwaukee, hence the eponym. According to PubMed, BCP crystals are recognised both as contributors to osteoarthritis and as the cause of this highly destructive shoulder arthritis.
- Elderly patients, with a strong female predominance - classically women over 70 years
- Usually affects the dominant shoulder; may be bilateral
- The knee (especially the lateral compartment) is the second classic large-joint site
- It is the prototypical BCP crystal disease of a large joint - examiners use it to test crystal identification
- It overlaps clinically and radiographically with mechanical cuff tear arthropathy, so candidates must explain the crystal-driven mechanism that distinguishes it
- The bloody, non-inflammatory effusion and the non-birefringent crystals are favourite traps
The name comes from the 1981 description by McCarty and colleagues in Milwaukee. Knowing it is a basic calcium phosphate (apatite) disease - not urate or pyrophosphate - is the key discriminator examiners want.
It Is Not Only the Shoulder: The Milwaukee Shoulder-Knee Syndrome
The mnemonic, the epidemiology and a viva follow-up all flag that "the knee can be involved too", but the topic never develops it — and the omission misses the point that this is a systemic crystal diathesis, not a purely local shoulder problem. McCarty's original 1981 description was in fact the "Milwaukee shoulder-knee syndrome", because the same elderly women characteristically destroy the knee as well.
- The knee pattern is distinctive. BCP-driven destruction characteristically targets the lateral tibiofemoral compartment (and the patellofemoral joint), producing a rapidly destructive osteoarthritis with the same large, often blood-stained, low-cell-count effusion and the same crystal-protease mechanism as the shoulder.
- The deformity is the giveaway: lateral-compartment loss tends to drive a valgus (genu valgum) knee — the opposite of the medial-compartment, varus-producing primary osteoarthritis. A rapidly destructive valgus knee with a big bloody quiet effusion in an elderly woman is the knee equivalent of the Milwaukee shoulder.
- It is frequently bilateral and polyarticular — both shoulders and both knees can be involved — so a destructive shoulder should prompt you to examine the knees, and vice versa.
- Shoulder
- Glenohumeral, dominant side
- Knee
- Lateral tibiofemoral + patellofemoral compartment
- Shoulder
- Massive rotator cuff tear
- Knee
- Rapidly destructive lateral-compartment OA
- Shoulder
- Superior migration, acetabularization
- Knee
- Genu valgum (lateral-compartment collapse)
- Shoulder
- Large, bloody, low cell count; BCP
- Knee
- Large, bloody, low cell count; BCP
- Shoulder
- Reverse total shoulder arthroplasty
- Knee
- Total knee arthroplasty (bone loss can complicate it)
Diagnosis and management at the knee mirror the shoulder: aspirate (large, bloody, low cell count), alizarin red for BCP, exclude sepsis, conservative measures first (aspiration plus intra-articular steroid), and arthroplasty for the end-stage joint.
Q: An elderly woman has a Milwaukee shoulder — which other joint do you examine and what would you expect? A: The knee — the original entity is the Milwaukee shoulder-knee syndrome. Expect rapidly destructive lateral-compartment OA producing a valgus knee with a large, bloody, non-inflammatory effusion. The disease is often bilateral and polyarticular, so it is a systemic BCP crystal diathesis, not a local shoulder problem.
Pathophysiology
The destruction in Milwaukee shoulder is enzymatic, not primarily inflammatory. BCP crystals act as a stimulus that converts the synovium into a tissue that digests its own joint.
The Crystal-Protease Cycle
- BCP crystals deposit in cartilage, the joint capsule and the rotator cuff (often with pre-existing degeneration and a massive cuff tear).
- Crystals are shed into the joint and phagocytosed by synoviocytes and macrophages.
- Activated synovial cells release proteolytic enzymes - especially collagenases and other matrix metalloproteinases (MMPs) - together with prostaglandins and cytokines.
- These enzymes degrade collagen and cartilage matrix, releasing further crystals and matrix fragments.
- The released crystals re-stimulate the synovium, creating a self-amplifying loop of crystal shedding and enzymatic destruction.
Why the Effusion Is Bloody but Quiet
- Progressive capsular and synovial breakdown plus repeated microtrauma against a deficient cuff produces a large, blood-stained effusion.
- Yet because the dominant mechanism is protease-mediated matrix digestion rather than a neutrophil-driven inflammatory flare, the synovial white cell count remains low (mononuclear-predominant). This explains the characteristic "large but non-inflammatory" aspirate.
The Mechanical Contribution
- A massive/complete rotator cuff tear removes the depressing force couple, allowing superior migration of the humeral head.
- The head erodes the undersurface of the acromion (acetabularization) and rounds off (femoralization) - the same end-stage radiograph as mechanical cuff tear arthropathy.
- In Milwaukee shoulder, the BCP crystal-protease cycle accelerates this destruction.
Candidates often assume "crystal arthropathy" means an acute neutrophilic flare like gout. In Milwaukee shoulder the destruction is driven by synovial release of collagenases and MMPs - which is why the joint is destroyed but the synovial fluid cell count is low.
The Other End of the Spectrum: BCP Crystals and Osteoarthritis
The Classification section lists "apatite-associated osteoarthritis" as part of the BCP spectrum and two of the evidence cards are about BCP crystals in osteoarthritis, but the relationship is never developed. It matters because Milwaukee shoulder sits at the destructive extreme of a continuum that runs through ordinary BCP-laden osteoarthritis.
- BCP crystals are common in the osteoarthritic joint. They are found in the synovial fluid of a high proportion of osteoarthritic joints, particularly advanced disease, and their presence is associated with more severe radiographic change and larger effusions. According to PubMed, calcium-containing crystals (CPPD and BCP — hydroxyapatite, carbonate-apatite and octacalcium phosphate) are the most common crystals in the osteoarthritic joint (Ea & Lioté) (DOI).
- Innocent bystander or active driver? This is the genuine controversy. The crystals could be a marker of cartilage breakdown (shed from damaged cartilage and bone — an epiphenomenon), or an active driver of progression. The evidence for a pathogenic role is strong: according to PubMed, BCP crystals injected into mouse knees induce osteoarthritis-like changes, and they activate inflammatory pathways — interleukin-6 and crystal-induced osteoclastogenesis — that degrade cartilage and resorb bone (Stack & McCarthy) (DOI). This is the same protease-and-cytokine biology that, taken to the extreme, produces the Milwaukee shoulder.
- Detection is the same problem as in the shoulder: BCP crystals are non-birefringent and hard to detect, so their role in osteoarthritis is under-recognised; dual-energy CT (DECT) is emerging as a non-invasive way to quantify intra-articular calcium-crystal deposition.
- Clinical implication: there is still no proven crystal-targeted or disease-modifying therapy, so a BCP-laden osteoarthritic joint is managed with the same symptomatic approach — but the IL-6 and osteoclast pathways are the obvious future targets.
Q: How do BCP crystals relate to ordinary osteoarthritis? A: They are found in a high proportion of osteoarthritic joints (especially advanced disease) and are linked to faster progression. Whether they are an innocent bystander or an active driver is debated, but BCP crystals injected into animal joints cause OA-like change via IL-6 and osteoclastogenesis — so Milwaukee shoulder is the rapidly destructive extreme of the same BCP-crystal continuum that runs through everyday OA.
Classification
Milwaukee shoulder is best placed within the broader family of calcium-containing crystal diseases and the spectrum of BCP-related musculoskeletal syndromes. Using the tabs below helps separate the crystal types and the BCP disease spectrum.
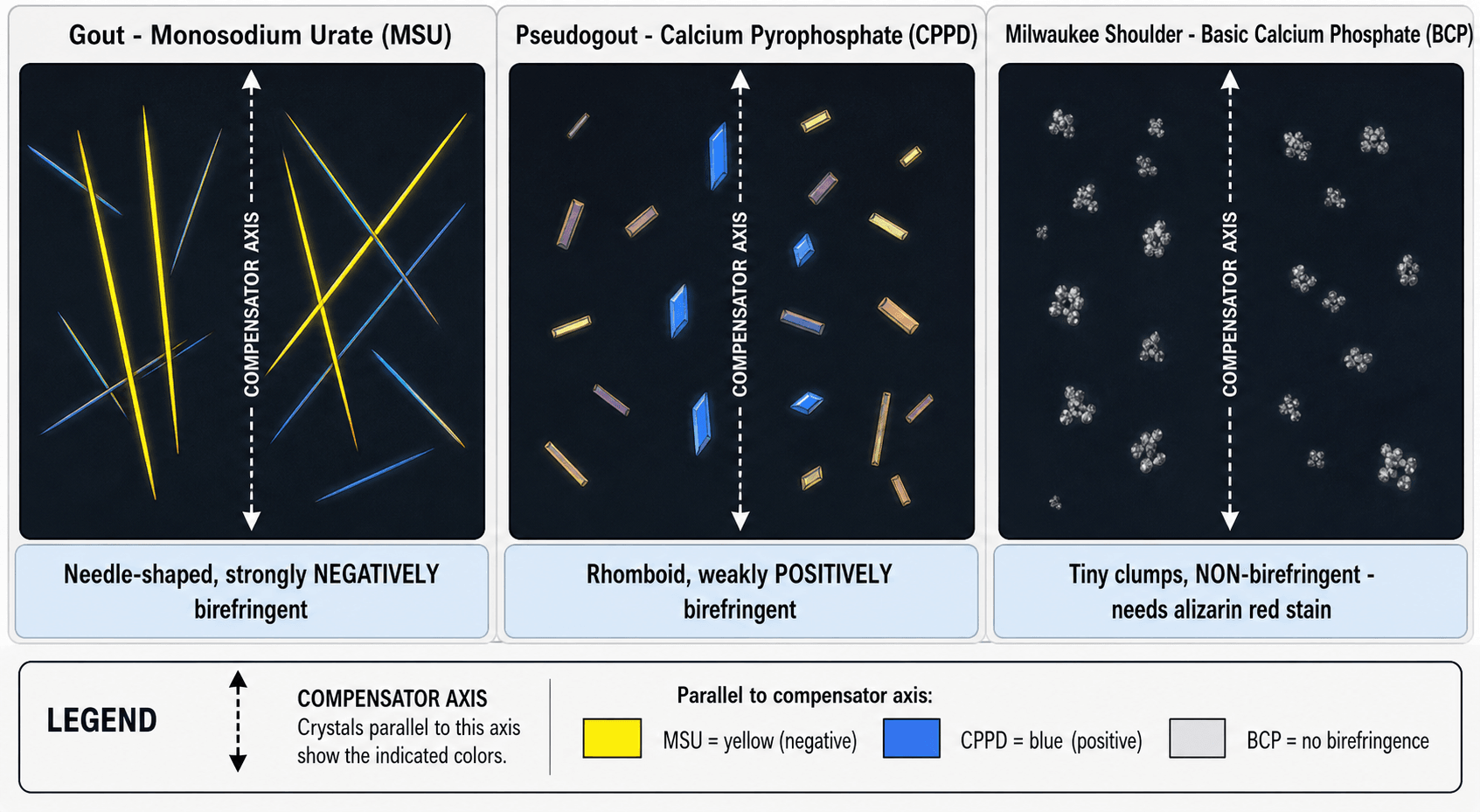
The three crystals every candidate must separate:
- Monosodium urate (MSU) - gout: needle-shaped, strongly negatively birefringent. Acute, intensely inflammatory.
- Calcium pyrophosphate dihydrate (CPPD) - pseudogout: rhomboid/rod-shaped, weakly positively birefringent. Chondrocalcinosis on X-ray.
- Basic calcium phosphate (BCP) - Milwaukee shoulder / calcific tendinitis: tiny, clump-forming, non-birefringent. Requires alizarin red or electron microscopy.
Clinical Presentation
History
- Elderly woman with chronic shoulder pain, often worse at night
- Recurrent swelling of the shoulder - patients may describe the joint "filling up" repeatedly
- Weakness and loss of active elevation reflecting the underlying massive cuff tear
- Symptoms in the dominant shoulder; the contralateral side and the knees may be involved
Examination
- Large effusion / fullness around the shoulder, sometimes with a fluctuant anterosuperior swelling
- Restricted and weak active elevation, with relatively preserved passive range early on
- Signs of a massive rotator cuff tear: positive drop-arm, weak external rotation, possible anterosuperior escape
- Crepitus and deformity as destruction advances; warmth is usually mild (not a hot inflamed joint like sepsis or gout)
Key Discriminators at the Bedside
- The disproportion between a large, sometimes bloody effusion and a relatively quiet, non-erythematous joint points to Milwaukee rather than sepsis or gout.
- The female sex, advanced age and dominant shoulder pattern is highly characteristic.
A big, recurrent, sometimes blood-stained shoulder effusion in an elderly woman with a massive cuff tear and only modest inflammatory signs is the classic Milwaukee presentation - but always aspirate to exclude infection.
Investigations
Synovial Fluid Analysis (The Key Test)
- Aspirate the joint - this is both diagnostic and therapeutic.
- Appearance: large volume, often blood-stained or xanthochromic.
- Cell count: characteristically LOW (non-inflammatory; mononuclear-predominant) - a vital discriminator.
- Crystal identification:
- BCP crystals are non-birefringent and individually too small for light microscopy - they form clumps that look like "shiny coins".
- Alizarin red S staining screens for calcium - a cheap, sensitive bedside-laboratory test for BCP. According to PubMed, a positive alizarin-red stain on synovial fluid is an important, inexpensive step in confirming the diagnosis.
- Definitive confirmation is by electron microscopy or X-ray diffraction in specialist settings.
- Always send for Gram stain, culture and a cell count to exclude septic arthritis.
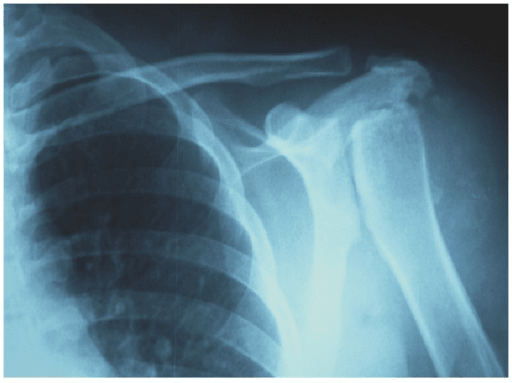
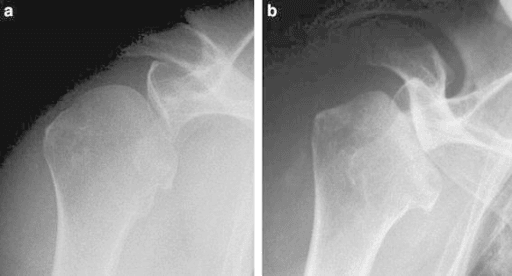
Plain Radiographs
- Superior migration of the humeral head with reduced acromiohumeral distance
- Glenohumeral joint space loss, subchondral sclerosis and rapid bone destruction / collapse of the humeral head
- Acetabularization of the acromion and femoralization of the tuberosity in end-stage disease
- Soft-tissue and intra-articular calcification may be visible
- Findings are often radiographically indistinguishable from advanced mechanical cuff tear arthropathy
Cross-Sectional Imaging
- Ultrasound / MRI: confirm the massive rotator cuff tear, demonstrate the large effusion and synovial thickening, and assess remaining muscle quality before any reconstruction.
- CT: defines bone loss and glenoid morphology when arthroplasty is being planned.
If asked how to confirm Milwaukee shoulder when polarised microscopy is negative, say: BCP crystals are non-birefringent - request alizarin red staining (and electron microscopy if available), and exclude infection in parallel.

Management
Management is predominantly conservative, escalating to arthroplasty for end-stage joints with intractable pain or loss of function. Use the tabs to structure the options.
- Therapeutic aspiration of the large effusion - relieves symptoms and confirms the diagnosis; may be repeated.
- Intra-articular corticosteroid after aspiration can reduce synovial activity and effusion recurrence.
- Analgesia and NSAIDs for symptom control (mindful of renal and GI risk in the elderly).
- Activity modification and physiotherapy to maintain whatever function the deficient cuff allows.
- According to PubMed, first-line treatment centres on analgesia and repeated arthrocentesis with intra-articular steroid; tidal (closed-needle) irrigation has also been reported as useful.
Never inject corticosteroid into a destroyed elderly shoulder until septic arthritis has been excluded with aspirate cell count, Gram stain and culture. Crystal disease and infection can coexist, and a missed joint sepsis is catastrophic.
Complications and Prognosis
Complications
- Progressive joint destruction with chronic pain and loss of function (pseudoparalysis once the cuff and fulcrum fail)
- Recurrent large effusions requiring repeated aspiration
- Massive irreparable cuff tear with anterosuperior escape
- Rapid humeral head collapse in the aggressive variant
- For those undergoing reverse arthroplasty: standard prosthetic risks (instability, scapular notching, infection, glenoid loosening)
Prognosis
- The natural history is one of slow but relentless destruction over months to years, occasionally punctuated by rapid deterioration.
- Conservative measures control symptoms but do not halt structural progression.
- Reverse total shoulder arthroplasty offers reliable pain relief and improved function in carefully selected end-stage patients.
- Because there is no disease-modifying therapy for the crystals, the focus is symptom control and timely arthroplasty rather than cure.
Clinical Relevance and Exam Application
Milwaukee shoulder is a high-value teaching case because it forces the candidate to integrate crystal biology, synovial fluid analysis and shoulder reconstruction.
- Differentiate the crystals: be slick on MSU vs CPPD vs BCP and the birefringence patterns - then add that BCP is non-birefringent and needs alizarin red.
- Explain the mechanism: crystals stimulate synovial release of collagenases/MMPs - enzymatic, not neutrophilic, destruction. This explains the low-cell-count bloody effusion.
- Run the destroyed-shoulder differential safely: sepsis first, then crystal, arthropathy (mechanical/neuropathic) and inflammatory disease.
- Link to reconstruction: a massive irreparable cuff plus end-stage destruction is the indication for reverse total shoulder arthroplasty.
Guidelines, Registries & Global Practice
Milwaukee shoulder is a rare condition without dedicated international management guidelines; practice is guided by rheumatology consensus on crystal arthropathies and by shoulder arthroplasty evidence.
Diagnostic Consensus (Global Rheumatology Practice)
- Synovial fluid analysis is the cornerstone worldwide: cell count plus crystal identification, with alizarin red S as the accessible screen for calcium (BCP) crystals because they are non-birefringent.
- Confirmation by electron microscopy / X-ray diffraction is reserved for specialist or research settings, reflecting limited availability globally.
Management Principles
- International rheumatology guidance for calcium crystal disease emphasises symptomatic treatment - analgesia, aspiration and intra-articular corticosteroid - as there is no disease-modifying therapy for BCP crystals.
- For end-stage destruction with an irreparable cuff, shoulder arthroplasty guidance (AAOS, BOA/BESS in the UK, and international shoulder societies) supports reverse total shoulder arthroplasty as the reconstruction of choice when the cuff is deficient.
Registry Evidence (Shoulder Arthroplasty)
- National joint registries (e.g. AOANJRR in Australia, NJR in the UK, AJRR in the US) report rising reverse total shoulder arthroplasty volumes for cuff-deficient destructive arthropathies, with reverse designs showing durable pain relief; scapular notching and instability are the implant-specific concerns tracked over time.
- Milwaukee shoulder is typically captured within the broader cuff tear arthropathy / massive cuff tear indication rather than as a separate registry category, so disease-specific survivorship data are limited.
Memory aids
MILWAUKEEMilwaukee Shoulder Features
Hook:MILWAUKEE = invisible crystals, big bloody quiet effusion, enzymes eat the joint
GPMThree Crystals to Separate
Hook:Gout, Pseudogout, Milwaukee - the last one is invisible to the polariser
SCARDestructive Shoulder Differential
Hook:A destroyed shoulder leaves a SCAR - Sepsis, Crystal, Arthropathy, Rheumatoid
MCQ and Exam Practice Points
- BCP (Milwaukee) crystals are non-birefringent - confirm with alizarin red S, not polarised light.
- The shoulder effusion is large and bloody but has a LOW cell count (non-inflammatory).
- Destruction is enzymatic - synovial collagenases / MMPs stimulated by crystals.
- Elderly woman, dominant shoulder, massive cuff tear is the classic triad.
- Management is conservative first (aspiration, steroid, irrigation); reverse TSA for end-stage.
- Always exclude septic arthritis before attributing a destroyed shoulder to crystals.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 74-year-old woman has a 6-month history of a painful, repeatedly swelling right (dominant) shoulder with weakness. Aspiration yields 60 mL of blood-stained fluid. How do you approach this?”
“What is the difference between Milwaukee shoulder and mechanical cuff tear arthropathy, and why does it matter?”
“On the synovial fluid microscopy the laboratory reports no crystals under polarised light, but you still suspect a crystal arthropathy. Explain the crystal biology and how you would proceed.”
Definition
- Rapidly destructive shoulder arthropathy driven by basic calcium phosphate (hydroxyapatite) crystals
- Also called apatite-associated destructive arthritis
- Distinct from gout (MSU) and pseudogout (CPPD)
Classic Patient
- Elderly woman, often over 70
- Dominant shoulder, massive cuff tear, weakness
- Large recurrent, often blood-stained effusion
Diagnosis
- Aspirate: large, bloody, LOW cell count (non-inflammatory)
- BCP crystals are NON-birefringent - use alizarin red S
- Exclude sepsis: Gram stain, culture, cell count
- X-ray: superior migration, glenohumeral destruction, acetabularization
Mechanism
- Crystals stimulate synoviocytes to release collagenases / MMPs
- Enzymatic matrix digestion, not neutrophilic inflammation
- Self-amplifying crystal-protease cycle
Management
- Conservative first: aspiration + intra-articular steroid + analgesia
- Tidal irrigation in refractory cases
- No disease-modifying drug for BCP crystals
- Reverse total shoulder arthroplasty for end-stage disease
Evidence Base
BCP crystal-associated musculoskeletal syndromes: an update
- Intra-articular BCP crystals contribute to osteoarthritis and cause the highly destructive arthritis known as Milwaukee Shoulder Syndrome
- BCP crystals deposited in tendons and bursae cause calcific periarthritis - the same crystal family with a different presentation
- Epidemiology and natural history remain poorly defined and few targeted therapies exist because the pathogenesis is incompletely understood
Basic calcium phosphate crystals and osteoarthritis pathogenesis: novel pathways and potential targets
- BCP crystals injected into mouse knees induce osteoarthritis-like changes, supporting a directly pathogenic role
- Interleukin-6 and crystal-induced osteoclastogenesis are key pathways linking BCP crystals to cartilage degradation and bone destruction
- Dual-energy CT is emerging as a non-invasive way to quantify intra-articular calcium crystal deposition
Calcium pyrophosphate dihydrate and basic calcium phosphate crystal-induced arthropathies: update on pathogenesis, clinical features, and therapy
- Calcium-containing crystals (CPPD and BCP - hydroxyapatite, carbonate-apatite, octacalcium phosphate) are the most common crystals in the osteoarthritic joint
- Crystal-induced inflammation arises from direct synovial tissue and cartilage activation, with extracellular pyrophosphate dysregulation underlying calcification
- Milwaukee shoulder arthropathy is named alongside knee and wrist pseudogout as a key calcium crystal presentation; effective anti-crystal therapies are lacking
Milwaukee shoulder syndrome (apatite associated destructive arthritis): therapeutic aspects
- Milwaukee shoulder is a destructive arthropathy of older women with a large synovial effusion and a complete rotator cuff tear
- First-line treatment is analgesia plus repeated arthrocentesis followed by intra-articular steroid, with closed-needle tidal irrigation reported as useful
- Late disease shows acromiohumeral and glenohumeral narrowing with humeral head degeneration; total shoulder arthroplasty may be considered