Revision Total Elbow Arthroplasty
- Primary total elbow arthroplasty fails by several modes that the revision must address: ASEPTIC LOOSENING (the commonest late indication), polyethylene BUSHING WEAR in linked (semi-constrained) implants - which generates particulate debris, osteolysis and progressive loosening - PERIPROSTHETIC FRACTURE, deep INFECTION, and instability or mechanical component failure (e.g. fractured stems); the elbow's small bones, thin cortices and high lever-arm loads make these problems common.
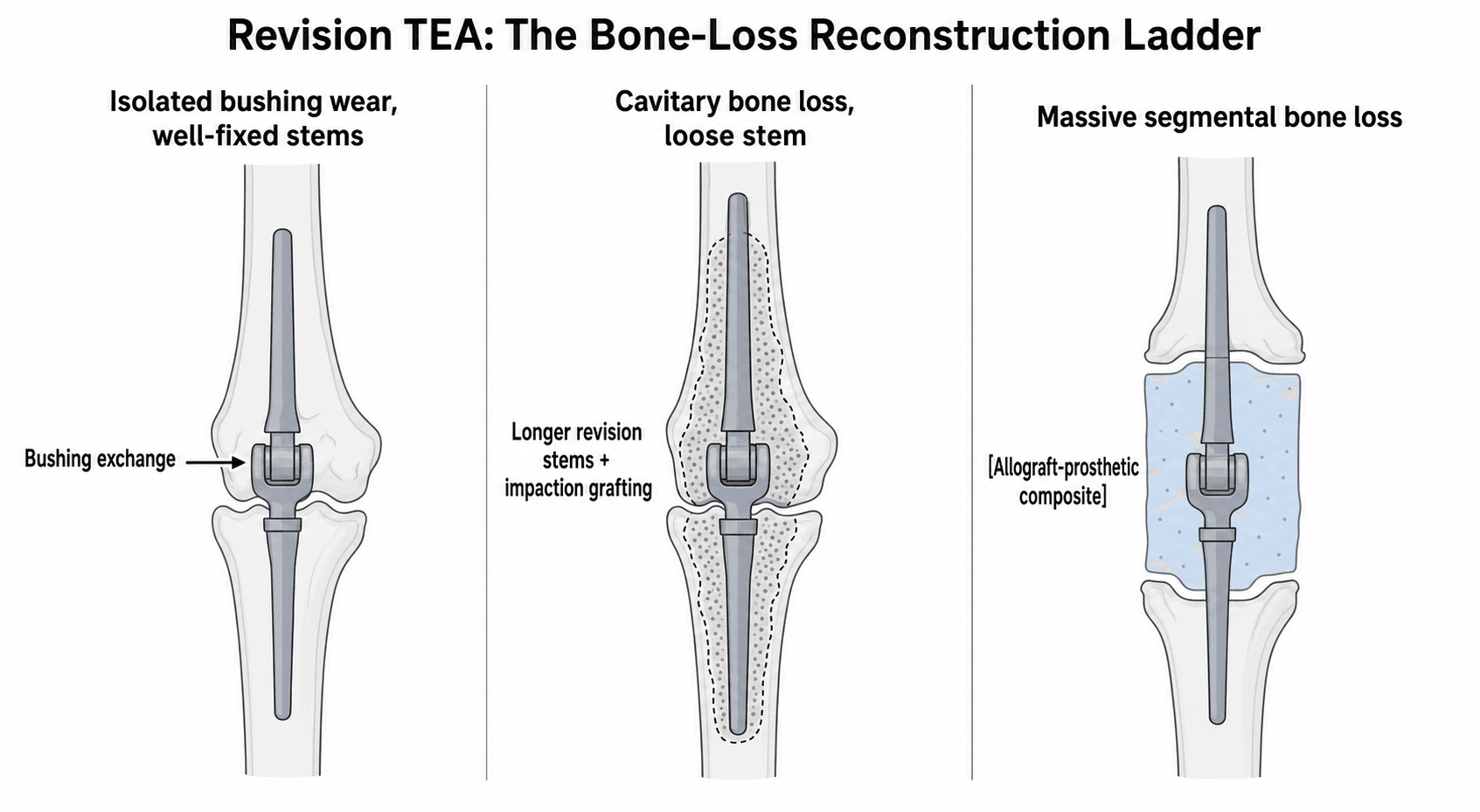
- PERIPROSTHETIC BONE LOSS is the central reconstructive problem and largely dictates the strategy: isolated polyethylene wear with well-fixed stems can be treated by BUSHING EXCHANGE; cavitary/contained loss around a loose stem is managed by re-cementing with LONGER (revision) STEMS and IMPACTION (cancellous) GRAFTING; and MASSIVE SEGMENTAL bone loss is reconstructed with an ALLOGRAFT-PROSTHETIC COMPOSITE (APC) as a salvage.
- The ALLOGRAFT-PROSTHETIC COMPOSITE is a salvage option for massive bone loss about the elbow, typically using a semi-constrained (Coonrad-Morrey-type) prosthesis cemented into a structural allograft; midterm series report satisfactory function with allograft incorporation in most, but a HIGH complication rate (periprosthetic fracture, ulnar neuropathy, wound problems) - so it is reserved for severe deficiency and counselled accordingly.
- Even primary linked TEA has a HIGH COMPLICATION rate with a comparatively low revision rate, and the concerning long-term signals are INCREASING radiolucent lines around the ulnar component and polyethylene BUSHING WEAR - so revision surgery, performed in already-compromised bone and soft tissues, carries an even higher complication burden including periprosthetic fracture, ULNAR NEUROPATHY, wound healing problems, re-loosening and re-revision.
- INFECTION must be actively excluded before any revision (it is a not-uncommon cause of a painful loose TEA): work up with inflammatory markers, aspiration and intra-operative samples; the INFECTED TEA is generally managed by a STAGED protocol - debridement and component removal with an antibiotic spacer, organism-directed antibiotics, and delayed re-implantation once the infection is controlled (with resection arthroplasty as a fallback when re-implantation is not feasible).
- Revision is to a LINKED (semi-constrained) implant, because deficient bone and incompetent collateral ligaments are the standing conditions of a revision and are exactly what an UNLINKED design cannot tolerate; the SLOPPY HINGE (about 7-10 degrees of varus-valgus and rotational laxity) transfers load to the soft tissues rather than concentrating it at the bone-cement interface that has already failed once.
- CEMENT EXTRACTION, not implantation, is the technical crux - it generates most of the bone loss and most of the periprosthetic fractures of the revision. The canals are narrow, curved and thin-walled (the ULNA especially), so work under direct vision with fine osteotomes and cement splitters rather than blind reaming, use ULTRASONIC tools for deep cement, and choose a PLANNED cortical window over an uncontrolled perforation. The defect you reconstruct is partly the defect you create.
- PERIPROSTHETIC FRACTURE about a TEA is classified by position relative to the STEM (O'Driscoll/Morrey, Mayo): TYPE I at the articulation (condyles, olecranon) - a linked implant does not need the condyles, so many are treated simply; TYPE II along the stem - and here the decisive question is whether the component is LOOSE, since a well-fixed stem means fix the fracture and retain, while a loose stem means revise to a longer stem that bypasses it; TYPE III beyond the stem tip - fix it, but OVERLAP the stem because its tip is a stress riser.
- DAIR performs POORLY at the elbow, and the numbers must be quoted at consent: 17 of 26 elbows failed, a 65% failure rate at two years, median 43 days to failure - about a 35% chance of success. It failed in EVERY case with a SINUS TRACT and EVERY CULTURE-NEGATIVE case, so either finding is a contraindication to retention rather than a caution. The thin posterior soft-tissue envelope also makes wound dehiscence prominent, and RESECTION ARTHROPLASTY is a legitimate endpoint giving pain relief at the cost of a flail elbow.
- Outcomes of revision TEA are MODEST and the risks substantial, so SELECTION and PLANNING matter: define the failure mode and bone loss (CT), exclude infection, plan the implant and graft strategy, protect the ulnar nerve and triceps, and counsel the patient realistically about function and the elevated complication and re-revision rates - with permanent activity restrictions (typically a low lifting limit) to protect the reconstruction.
- “Primary TEA fails by ASEPTIC LOOSENING (commonest late), BUSHING WEAR (linked implants -> osteolysis), PERIPROSTHETIC FRACTURE, INFECTION, instability.
- “PERIPROSTHETIC BONE LOSS dictates revision: bushing exchange -> longer stems + impaction grafting -> allograft-prosthetic composite (APC) for massive loss.
- “ALWAYS exclude infection first; revision TEA is complication-heavy (periprosthetic fracture, ulnar neuropathy, re-revision) - select and counsel carefully. Lifelong 2-5 kg lifting limit.
- “DAIR at the elbow succeeds only ~35% of the time (17/26 failed, 65% at 2 years, median 43 days); it failed in EVERY sinus-tract and EVERY culture-negative case - so staged revision is the default.
- “Revise to a LINKED implant (sloppy hinge, 7-10 deg laxity) - deficient bone and incompetent ligaments are what an unlinked design cannot tolerate. CEMENT REMOVAL is the crux and creates much of the bone loss.
- “Periprosthetic fracture (Mayo, O'Driscoll/Morrey): I at the articulation, II along the stem (LOOSE or not decides fix-versus-revise), III beyond the tip (overlap the stem - it is a stress riser).
Aseptic loosening, bushing wear, periprosthetic fracture, infection, instability - define the mode (and exclude infection) before planning.
Periprosthetic bone loss: bushing exchange -> longer stems + impaction grafting -> allograft-prosthetic composite for massive loss.
Modes of Failure & the Bone-loss Problem
Total elbow arthroplasty fails by aseptic loosening (the commonest late cause), polyethylene bushing wear in linked implants (driving osteolysis and loosening), periprosthetic fracture, deep infection, and instability/component failure - all made common by the elbow's small bones, thin cortices and high loads. The revision strategy is dictated by periprosthetic bone loss: isolated wear with well-fixed stems needs only a bushing exchange; contained/cavitary loss around a loose stem needs longer revision stems with impaction grafting; and massive segmental loss needs an allograft-prosthetic composite (APC). Even primary linked TEA carries a high complication rate, and increasing ulnar radiolucent lines and bushing wear are the worrying long-term signals - so revision in compromised bone and soft tissues is complication- heavy, and infection must be excluded first.
Classifying the Bone Loss - and the Periprosthetic Fracture
How Bone Loss Is Actually Described at the Elbow
Unlike the hip, the elbow has no single universally adopted bone-loss classification in the way Paprosky is used for the femur and acetabulum. The practical consequence is that the deficiency has to be described rather than assigned a grade, and four questions do the describing. Answer them from a CT with metal-artefact reduction and the reconstruction largely chooses itself.
- Why it decides
- The ulna is the smaller, thinner-walled bone with the least reserve, so ulnar deficiency is the harder problem and the canal where a perforation during cement removal is most easily made
- What it changes
- Determines which canal needs the long stem and where the graft goes
- Why it decides
- An intact cortical tube can hold impacted graft; a segmental defect has no wall to contain it
- What it changes
- Contained loss -> impaction grafting; segmental loss -> structural graft or allograft-prosthetic composite
- Why it decides
- Fixation in revision comes from the diaphysis, not the destroyed metaphysis - a stem must reach past the deficient bone into a competent tube
- What it changes
- Sets the stem length; too little remaining diaphysis is what pushes the case towards an APC
- Why it decides
- A linked implant does not need the columns for stability, but the olecranon carries the triceps and the extensor mechanism cannot be reconstructed from nothing
- What it changes
- Loss of the olecranon/triceps insertion is a functional problem the implant cannot solve, and may need allograft with tendon attached
The elbow has no Paprosky equivalent, so describe rather than grade: which bone, contained versus segmental, how much competent diaphysis remains beyond the defect, and is the olecranon/triceps insertion intact. Fixation in revision comes from the diaphysis - the stem must bypass the deficient bone into a competent tube.
Periprosthetic Fracture: the Mayo Classification
Periprosthetic fracture is both a reason a primary arthroplasty comes to revision and the commonest single complication of the revision itself, so it needs its own framework. The classification in general use comes from O'Driscoll and Morrey's Mayo experience of more than 1,000 total elbow arthroplasties, and it is built on where the fracture lies relative to the stem - applied the same way on the humeral and the ulnar side.
- Location
- About the articulation - humeral condyles, or olecranon/coronoid - not involving the stem
- Principle of treatment
- A linked implant does not depend on the condyles for stability, so many are treated non-operatively or by simple fragment fixation; olecranon fractures matter more because they carry the triceps
- Location
- Along the length of the stem
- Principle of treatment
- The decisive question is whether the component is LOOSE. Well-fixed -> fix the fracture and retain the implant (plate, cortical strut allograft, cerclage). Loose -> revise to a longer stem that bypasses the fracture, which treats both problems at once
- Location
- Beyond the tip of the stem, in the diaphysis
- Principle of treatment
- Treated as a fracture in its own right, but the stem tip immediately adjacent to it is a stress riser - so fixation must OVERLAP the stem rather than end level with its tip, or a second fracture is created at the junction
A Type II fracture with a well-fixed component is a fracture problem: fix it and keep the implant. The same fracture with a loose component is an arthroplasty problem: a long revision stem bypassing the fracture solves both, and plating around a loose stem simply fails again. Deciding this needs the pre-injury radiographs for comparison and, at operation, a direct assessment of stem stability - not an assumption.
Reconstruction Options & the Infected TEA
- Bushing exchange. For isolated polyethylene wear with well-fixed stems - exchange the bushings (and treat any osteolysis), the least invasive revision.
- Re-stemming with impaction grafting. For a loose stem with contained/cavitary bone loss - re-cement longer revision stems with impaction (cancellous) grafting to restore the canal.
- Allograft-prosthetic composite (APC). For massive segmental bone loss - a semi-constrained prosthesis cemented into a structural allograft; satisfactory midterm function with allograft incorporation in most, but a high complication rate.
- The infected TEA - staged revision. Exclude infection in every painful/loose TEA (markers, aspiration, intra-operative samples); manage infection by debridement and component removal with an antibiotic spacer, organism-directed antibiotics, and delayed re-implantation once controlled (resection arthroplasty as fallback).
- Protect nerve and triceps. Identify/protect the ulnar nerve and preserve the triceps mechanism throughout.
The two errors that wreck a revision TEA are operating without excluding infection and operating without knowing the bone loss. Infection is a not-uncommon cause of a painful, loose TEA, and revising an unrecognised infected implant as if it were aseptic loosening will fail - so every painful/loose TEA needs inflammatory markers, aspiration and intra-operative samples, with a STAGED revision if infected. Equally, the reconstruction is chosen by the periprosthetic bone loss, so define it (usually on CT) before surgery to plan whether a bushing exchange, longer cemented stems with impaction grafting, or an allograft-prosthetic composite is needed and to have the implants and graft available. Throughout, protect the ulnar nerve and triceps, counsel the patient that revision TEA is complication-heavy with a real re-revision rate, and impose a permanent lifting restriction of 2-5 kg to protect the construct - the same lifelong limit that applies after a primary TEA.
The Infected TEA in Detail
Debridement with implant retention (DAIR) works far less well at the elbow than the phrase "acute infection, retain the implant" suggests. In a Mayo cohort of 26 elbows with periprosthetic joint infection managed by DAIR, the procedure failed in 17 - a failure rate of 65% at two years (95% CI 41.3-79.6%) - with a median time to failure of only 43 days. The authors' own conclusion is that a patient being offered DAIR must be told the chance of success is approximately 35%. That is the number that makes the consent honest, and it is why the staged route is the default here in a way it is not at the hip or knee.
Two findings in that series were absolute rather than relative: DAIR failed in every case with a sinus tract and in every case that was culture-negative. Either finding should therefore be read as a contraindication to retention rather than as a reason for caution. A shorter symptom duration and a monomicrobial infection characterised the patients who did well, though with those numbers the associations did not reach statistical significance.
The staged protocol. First stage: remove all components and cement, radical debridement, deep samples from several sites before antibiotics, and an antibiotic-loaded cement spacer. Organism-directed intravenous therapy follows, guided by microbiology and infection-disease input. Re-implantation is delayed until the infection is controlled clinically and biochemically. Two features specific to the elbow shape this:
- The soft-tissue envelope is thin and posterior, with little subcutaneous cover over the implant and often several previous incisions. Wound dehiscence is a prominent complication in the published revision series, so use the previous incision where possible, avoid parallel incisions that devascularise the skin bridge, handle the edges minimally, and involve plastic surgery early where cover is doubtful.
- Resection arthroplasty is a legitimate endpoint, not simply a failure. Where re-implantation is not feasible - uncontrolled infection, unreconstructable bone, or a patient unfit for further surgery - a resection gives reasonable pain relief at the cost of a flail, unstable elbow, and that trade should be described to the patient in those terms rather than as a fallback of last resort.
Executing the Revision: Implant Choice and Cement Removal
Revise to a Linked Implant
The revision elbow is, almost by definition, the elbow with deficient bone, incompetent collateral ligaments, or both - which is precisely the situation an unlinked (resurfacing) design cannot tolerate, because it depends on the soft tissues for stability. So a failed unlinked implant, and a failed linked implant being re-done, are in practice both revised to a linked (semi-constrained) device. The linkage is a sloppy hinge permitting about 7-10 degrees of varus-valgus and rotational laxity, which matters here because it lets load be shared with the surrounding soft tissues rather than concentrated at the bone-cement interface - the very interface that has already failed once.
Revision TEA is linked TEA. Deficient bone and incompetent ligaments are the standing conditions of a revision, and those are exactly the conditions an unlinked implant cannot meet. The sloppy hinge (about 7-10 degrees of varus-valgus laxity) is not a compromise but the point: it transfers load to the soft tissues instead of the bone-cement interface that already failed.
Getting the Old Cement Out
Cement extraction, not implantation, is the technical crux of the revision and the step that generates most of the bone loss and most of the periprosthetic fractures.
- The canals are narrow, curved and thin-walled, and the ulna especially offers very little margin between a cement lump and the cortex. Perforation and iatrogenic fracture are made here, not at the moment of implantation.
- Work under direct vision as far as possible, using long, fine osteotomes and cement splitters down the canal rather than blind reaming, and take the cement out in fragments from the inside rather than levering against the endosteum.
- Ultrasonic cement removal tools allow deep cement to be softened and withdrawn along the canal with less cortical damage than mechanical instruments, and are the standard aid where they are available.
- A controlled cortical window or extended osteotomy is preferable to an uncontrolled perforation when distal cement cannot be reached - plan it, place it where it can be plated or strut-grafted, and repair it.
- Take deep samples before any of this if there is the slightest question of infection, and treat the case as potentially infected until they are negative.
The deficiency that dictates the reconstruction is not fixed when the patient comes to theatre - a large part of it is created during cement and component extraction. Every technique above exists to keep the defect the size it was on the pre-operative CT. Plan the extraction as carefully as the implantation, have long stems, strut allograft and cerclage available before starting, and be prepared for the reconstruction to escalate a rung on the ladder if the canal is breached.
The Ulnar Nerve: Why It Is at Risk and How to Protect It
- The anatomy at risk: the ulnar nerve runs in the cubital tunnel behind the medial epicondyle, right at the medial margin of the elbow surgical field. In a revision it is encased in scar from the prior surgery (and may already have been transposed), so it is distorted, tethered and hard to find - and at high risk from exposure, retraction/traction and thermal injury (full anatomy in Ulnar Nerve Anatomy and Cubital Tunnel Syndrome).
- Document it first: record any pre-existing ulnar neuropathy before surgery (so a post-operative deficit is not wrongly attributed to the revision).
- Identify and protect early: formally expose the nerve in healthy tissue proximal and distal to the scarred zone, follow it into the field, handle it gently, and decide between in-situ protection and anterior transposition (often transposed if previously transposed or tethered).
- Counsel for it: ulnar neuropathy (often transient/neurapraxic, occasionally permanent) is among the commonest complications of revision elbow surgery.
The ulnar nerve sits behind the medial epicondyle at the edge of the field and in revision is scarred, tethered and possibly already transposed - so document a pre-existing deficit, find and protect it proximal-to-distal through healthy tissue, consider transposition, and counsel that ulnar neuropathy is one of the commonest complications.
The Triceps: Approach and the Insufficiency Problem
- The approach options: TEA and its revision must deal with the triceps insertion on the olecranon - via a triceps-reflecting approach (e.g. Bryan-Morrey, reflecting the triceps medial-to-lateral in continuity with the forearm fascia/periosteum), a triceps-splitting approach, or a triceps-on / paratriceps (triceps-sparing) approach that leaves the insertion intact; if the triceps is taken down it must be securely reattached transosseously.
- Triceps insufficiency - a recognised revision complication: repeated approaches (and the poor tissue of rheumatoid or multiply-operated elbows) can leave the triceps detached or attenuated, causing weak or absent active extension and difficulty pushing up from a chair. It is managed by direct repair or reconstruction (e.g. anconeus rotation or Achilles tendon allograft) - the rupture itself is covered in Triceps Tendon Rupture.
- The principle: choose the least-disruptive approach that gives adequate access, and protect and securely repair the extensor mechanism - it is as important to the outcome as the implant.
Manage the triceps insertion by a triceps-reflecting (Bryan-Morrey), triceps-splitting, or triceps-on approach, and reattach it transosseously if taken down. Triceps insufficiency (weak extension, can't push up from a chair) is a recognised complication of repeated/revision approaches and poor tissue - repair or reconstruct (anconeus rotation, Achilles allograft).
Mnemonics & Memory Aids
LOOSE TEA
Hook:LOOSE TEA: Loosening, Osteolysis (bushing), Other modes, Sepsis excluded, Evaluate bone loss, Tactics by bone loss, Eyes on ulnar nerve, Advise on risks.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Why do total elbow arthroplasties fail, and how do you work up a painful TEA before revision?”
“How does periprosthetic bone loss guide your revision TEA reconstruction?”
“A 68-year-old presents three weeks after a total elbow arthroplasty with a discharging wound and a raised CRP. Would you wash it out and keep the implant?”
“A patient with a total elbow arthroplasty falls and sustains a fracture along the ulnar stem. How do you classify and manage it?”
Why TEAs fail
- Aseptic loosening (commonest late)
- Polyethylene bushing wear -> osteolysis (linked implants)
- Periprosthetic fracture, infection, instability/component failure
Work-up
- Define failure mode; EXCLUDE infection (markers, aspiration, intra-operative samples)
- CT to map periprosthetic bone loss
- Assess ulnar nerve and triceps
Describing bone loss (no Paprosky equivalent)
- Which bone - humerus, ulna, or both? (ulna is thinner-walled, least reserve)
- Contained (cavitary) or uncontained (segmental)?
- How much competent diaphysis remains beyond the defect? (fixation comes from the diaphysis)
- Are the columns, olecranon and triceps insertion intact?
Reconstruction (by bone loss)
- Isolated wear, fixed stems -> bushing exchange
- Loose stem, cavitary loss -> longer cemented stems + impaction grafting
- Massive segmental loss -> allograft-prosthetic composite (salvage)
- Always to a LINKED implant (sloppy hinge, 7-10 deg laxity)
Periprosthetic fracture (Mayo)
- Type I - at the articulation (condyles, olecranon); linked implant does not need the condyles
- Type II - along the stem; LOOSE or not decides fix-and-retain versus revise to a long stem
- Type III - beyond the stem tip; fix it but OVERLAP the stem (stress riser)
Infection & counselling
- DAIR: ~35% success (17/26 failed, 65% at 2 yrs, median 43 days) - quote this at consent
- Sinus tract or culture-negative -> DAIR failed in EVERY case; do not retain
- Staged revision (spacer, organism-directed antibiotics, delayed re-implant)
- Thin posterior envelope - use previous incision, no parallel incisions, plastics early
- Resection arthroplasty: real pain relief, flail elbow - a legitimate endpoint
- Lifelong 2-5 kg lifting restriction to protect the construct
Evidence & Key Studies
Coonrad-Morrey total elbow arthroplasty: 78 elbows at mean 5 years (failure signals)
- Linked (Coonrad-Morrey) TEA treated a broad spectrum (inflammatory arthritis and trauma) with better results in rheumatoid than traumatic cases; survivorship was 97.7% at 5 years and 91.0% at 10 years with aseptic loosening as the endpoint.
- Despite a low revision rate, the complication rate was high (27 complications; 9 revised).
- Increasing radiolucent lines around the ulnar component over time and polyethylene bushing wear were specific concerns - the signals that precede revision.
Allograft-prosthetic composite reconstruction for massive bone loss at the elbow
- Revision of a loose TEA with massive bone loss is challenging; an allograft-prosthetic composite (with a semi-constrained Coonrad-Morrey prosthesis) is a salvage option - here aseptic loosening was the indication in all cases.
- Midterm functional outcomes were satisfactory with allograft incorporation in most (83%) and all prostheses well-fixed, and no further revisions were required.
- Complications were frequent (periprosthetic fracture, ulnar neuropathy, aseptic loosening, wound dehiscence), underlining the high complication burden of elbow revision for massive bone loss.
Debridement, antibiotics and implant retention (DAIR) for elbow periprosthetic joint infection - outcomes and risk factors for failure
- Of 26 elbows with periprosthetic joint infection managed by DAIR, the procedure failed in 17 - a failure rate of 65% at two years (95% CI 41.3-79.6%) - with a median time to failure of only 43 days.
- DAIR failed in every case with a sinus tract and in every culture-negative case; favourable outcomes were associated with shorter symptom duration and monomicrobial infection, though not significantly with these numbers.
- The authors conclude that a patient considered for DAIR must be told the chance of success is approximately 35%.
Periprosthetic fractures about the elbow - principles of classification and treatment
- Sets out the classification and treatment principles for periprosthetic fractures about the elbow, drawn from an institutional experience of more than 1,000 total elbow arthroplasties.
- Fractures are grouped by their position relative to the stem, which is what separates a fracture that can be fixed around a retained implant from one that requires revision to a longer stem.
- Written because the elbow literature offered little guidance compared with the hip and knee - a gap that still shapes how the injury is described today.
The failure signals of linked TEA - aseptic loosening as the survivorship endpoint, the high complication rate despite a low revision rate, and the specific concerns of increasing ulnar radiolucent lines and bushing wear - come from the cited Mansat series; the allograft-prosthetic composite as a salvage for massive bone loss, with satisfactory midterm function (allograft incorporation in 83%) but frequent complications, from the cited Laumonerie series. The DAIR figures - 17 failures in 26 elbows, 65% failure at two years, median 43 days to failure, universal failure with a sinus tract or a negative culture, and the roughly 35% success figure for consent - are Tai. The classification of periprosthetic fractures by position relative to the stem is O'Driscoll and Morrey.
The 2-5 kg lifelong lifting restriction and the 7-10 degrees of varus-valgus laxity in a sloppy-hinge linked implant are taken in substance from Total Elbow Arthroplasty, where they are set out for the primary operation with their own sources; both apply unchanged after a revision. The statement that the elbow has no single universally adopted bone-loss classification comparable to Paprosky at the hip is made deliberately rather than by omission - the four descriptive questions given in its place, the reconstruction ladder (bushing exchange, longer stems with impaction grafting, APC), the principles of cement extraction, and the staged management of the infected TEA are standard, well-established teaching rather than a graded system. (See also Periprosthetic Joint Infection.)