The Musician's Nerve (Fine Motor Control)
- Originates from Medial Cord (C8-T1)
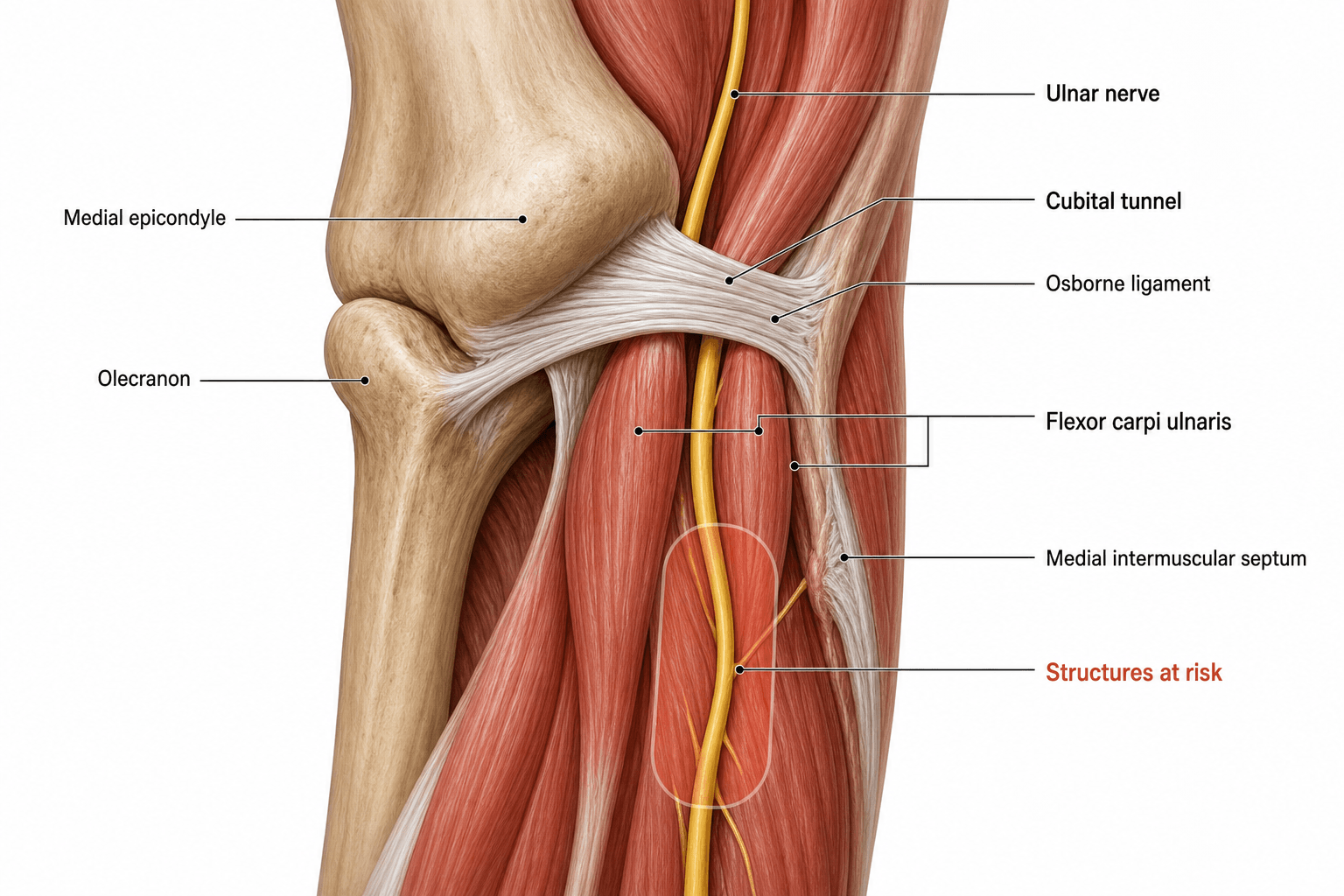
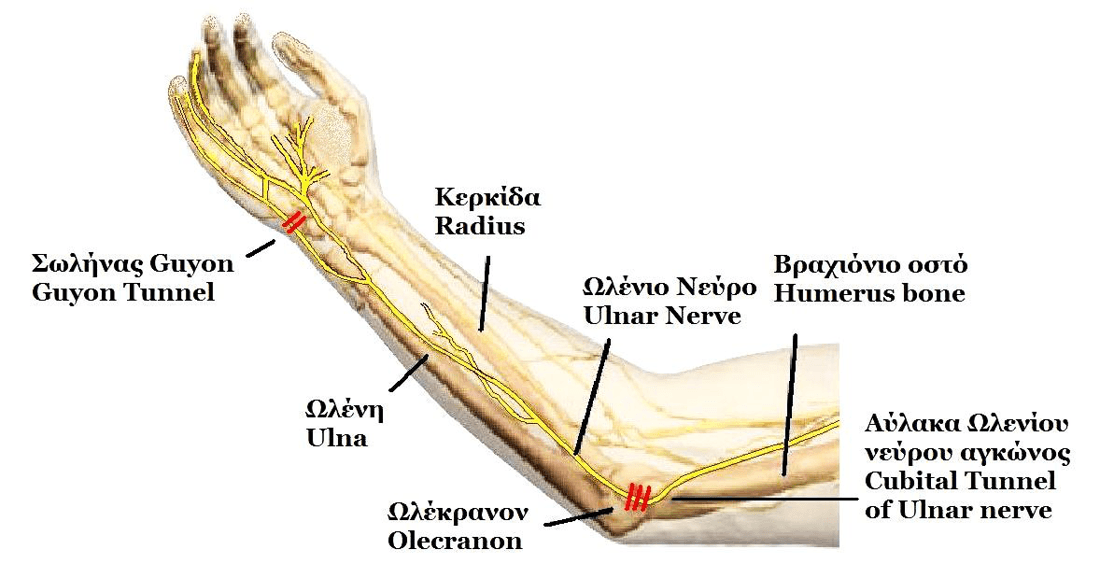
- Passes POSTERIOR to Medial Epicondyle
- Enters forearm between two heads of FCU
- Supplies all intrinsics EXCEPT LOAF (Lumb 1/2, Opponens, AbdPB, FlexPB)
- Sensory to medial 1.5 fingers
- “Ulnar Paradox: High lesions claw LESS than low lesions (FDP paralysis)
- “Froment's Sign tests Adductor Pollicis (Ulnar), compensation by FPL (Median/AIN)
- “Struthers Arcade is in the ARM (Ulnar), Struthers Ligament is Supracondylar (Median)
- “Martin-Gruber Anastomosis: Median → Ulnar communication in forearm
"High lesion = Less Clawing." In a high lesion (elbow), the FDP to the ring/little fingers is paralyzed, so the IP joints do not flex, masking the claw deformity. In a low lesion (wrist), FDP is intact, causing unopposed flexion of IP joints → Severe Clawing.
Tests Adductor Pollicis. Patient asked to hold paper between thumbs. If Adductor is weak (Ulnar), patient flexes IPJ (FPL - Median) to compensate. This is a positive sign.
The floor is the MCL (Ulnar Collateral Ligament). Transposition is often indicated if the nerve subluxes or the bed is irregular (arthritic osteophytes).
Abducted Little Finger. Due to weakness of Palmar Interossei (Adduction) and unopposed action of EDM (Radial) and Abductor Digiti Minimi (Ulnar - but often spared or less affected relative to mechanics). Note: Wartenberg's Syndrome is Radial sensory, Wartenberg's Sign is Ulnar motor.
- Key Detail
- Medial Cord (C8-T1)
- Clinical Significance
- Lower Trunk Plexopathy mimics Ulnar nerve
- Key Detail
- Cubital Tunnel
- Clinical Significance
- #1 Compression site
- Key Detail
- FCU + FDP (Medial 1/2)
- Clinical Significance
- Flexion of wrist/digits 4,5
- Key Detail
- Guyon's Canal
- Clinical Significance
- #2 Compression site
- Key Detail
- Arcade of Struthers (8cm)
- Clinical Significance
- Proximal to medial epicondyle
LOAFExceptions (Median Supplied)
Hook:Median nerve supplies the LOAF, Ulnar supplies the rest.
ULNARClaw Hand Causes
Hook:Differential diagnosis for clawing.
Overview and Function
The Ulnar Nerve is the nerve of fine manipulation. It powers the intrinsic muscles that allow for grip strength, pinch, and complex finger movements. "Power Grip" relies heavily on ulnar-innervated intrinsic function to stabilize the MCP joints.
Motor Innervation Summary
- Forearm: Flexor Carpi Ulnaris (FCU), FDP (Ring, Little).
- Hypothenar: Abductor Digiti Minimi, Flexor Digiti Minimi, Opponens Digiti Minimi.
- Hand: Palmar Interossei (3), Dorsal Interossei (4), Lumbricals (3, 4), Adductor Pollicis, Deep head FPB.
Total: 1.5 Forearm muscles + Most Hand Intrinsics.
The profound impact of this innervation is seen in the 'Intrinisic Minus' hand.
Neurovascular
Axilla & Arm Course
- Terminal branch of Medial Cord (C8, T1).
- Often receives C7 fibers (from Lateral Cord).
- Lies medial to axillary and brachial arteries.
- Runs in anterior compartment initially.
- At mid-arm, it pierces the Medial Intermuscular Septum to enter the posterior compartment.
- Arcade of Struthers: A band of fascia approx. 8cm proximal to medial epicondyle. A potential compression site (esp after transposition).
- Runs distally towards the groove behind the medial epicondyle.
This proximal course is relatively safe from compression.
Riche-Cannieu Anastomosis and Anomalous Innervation
The Martin-Gruber anastomosis (median-to-ulnar in the forearm) has a hand-level counterpart. The Riche-Cannieu anastomosis is a communication in the palm between the recurrent (motor) branch of the median nerve and the deep (motor) branch of the ulnar nerve. It is common in anatomical studies and, when extensive, can produce an "all-ulnar hand" in which the ulnar nerve effectively supplies all the intrinsic muscles, including the thenar group.
- Location
- Forearm
- Direction
- Median (or AIN) to ulnar
- Clinical effect
- High ulnar lesions may spare hand intrinsics (pseudo-preservation); confounds nerve conduction studies
- Location
- Palm / hand
- Direction
- Median recurrent branch to ulnar deep branch
- Clinical effect
- Can produce an 'all-ulnar hand'; confounds median/ulnar localisation and conduction studies
- Location
- Forearm
- Direction
- Ulnar to median (reverse of Martin-Gruber)
- Clinical effect
- Rare; produces atypical median-territory findings
Martin-Gruber is a median-to-ulnar crossover in the forearm; Riche-Cannieu is a median-to-ulnar crossover in the hand (recurrent median branch to the deep ulnar branch). Both can blur the expected motor map, occasionally producing an "all-ulnar hand," and both can confound nerve conduction studies.
Classification Systems
McGowan Classification (Cubital Tunnel)
The original three-grade clinical staging system for ulnar nerve compression at the elbow, used to guide management and predict outcome.
- Clinical Findings
- Mild: intermittent paraesthesia in ulnar digits, subjective weakness, no measurable motor loss or wasting
- Prognosis
- Good with conservative or surgical treatment
- Clinical Findings
- Moderate: measurable intrinsic weakness, persistent paraesthesia, wasting may be early/absent
- Prognosis
- Good outcome likely if treated before fixed atrophy
- Clinical Findings
- Severe: marked weakness, established intrinsic atrophy and clawing, often constant numbness
- Prognosis
- Guarded; permanent deficit common despite surgery
Clinical Assessment
- Wasting: Hypothenar eminence and First Dorsal Interosseous (dorsum of webspace).
- Clawing: Hyperextension of MCPJ and Flexion of IPJ (Ring/Little).
- Wartenberg's Sign: Little finger sits abducted.
- Tinel's: Tap over cubital tunnel and Guyon's canal.
- Elbow Flexion Test: Patient flexes elbow fully, wrist extended. Hold 60s. Reproduction of symptoms (+ve).
- Scratch Collapse Test: Sensitivity controversial.
- Patient grasps paper between thumbs.
- Positive: Flexion of IPJ (FPL) to compensate for weak Adductor Pollicis.
- Jeanne's Sign: Hyperextension of MCPJ during pinch (instability).
- Dorsal ulnar sensation SPARED in Guyon's canal / Wrist lesions.
- LOST in Cubital Tunnel / High lesions.
Differential Diagnosis
- Differentiating Features
- Neck pain, All medial hand muscles affected (incl Median)
- Key Test
- Spurling's Test / MRI Neck
- Differentiating Features
- T1 fibers affected (AP loss), Horner's Syndrome (sometimes)
- Key Test
- Chest X-Ray (Pancoast)
- Differentiating Features
- Vascular signs, Positional provocation
- Key Test
- Adson's Test / Doppler
- Differentiating Features
- Painless wasting, Fasciculations, Hyperreflexia
- Key Test
- EMG (Widespread denervation)

Investigations
Radiology
- X-rays: Check for bone spurs, cubitus valgus deformity, supracondylar spur (rare), or hook of hamate fracture (Guyon).
- Ultrasound: Cross-sectional area over 10mm² suggests compression. Can see nerve instability (subluxation) in real-time.
- MRI: Space-occupying lesions (ganglion cystic in Guyon's).
Advanced imaging is reserved for atypical cases or recurrences.
Management Strategy
Non-Operative Management
- Indication: Mild symptoms (McGowan I), intermittent paresthesia.
- Night Splinting: Prevents elbow flexion over 45 degrees. Keep arm straight-ish.
- Activity Modification: Avoid resting elbows on tables, headset use.
- NSAIDs: Adjunct.
- Success: ~50% effective in mild cases.
Patient compliance is key to conservative success.
Surgical Technique: Decompression
In Situ Decompression
Op Tech: In Situ Decompression
Curvilinear incision over cubital tunnel, centered on epicondyle. Protect MABCN (Medial Antebrachial Cutaneous Nerve) crossing the field.
- Distal: Aponeurosis of FCU (two heads).
- Tunnel: Osborne's Ligament (Roof).
- Proximal: Arcade of Struthers and Medial Intermuscular Septum.
Flex elbow. Does nerve sublux? If yes → Transpose. If no → Close.
The MABCN branches cross the surgical field. Injury causes painful neuroma and numbness over the olecranon/posterior proximal forearm.
Room Setup & Logistics
- Position: Supine, Arm board, Tourniquet high on arm
- Anesthesia: General or Regional (Block)
- Equipment: Loupes/Microscope (optional but recommended), Nerve stimulator
- Instruments: Basic plastic set, Tenotomy scissors, Vessel loops
Clinical Handoff
- Action
- Mark incision, Confirm symptoms side
- Goal
- Avoid wrong site
- Action
- Identify MABCN, Release all 5 sites
- Goal
- Complete decompression
- Action
- Soft dressing, Early ROM
- Goal
- Prevent stiffness
Complications
- Cause
- Surgical trauma
- Management
- Excision / Burying
- Cause
- Incomplete release (septum/FCU)
- Management
- Revision Decompression
- Cause
- Excessive release anteriorly
- Management
- Transposition
- Cause
- Destabilized origin
- Management
- Physio / Repair
Rehabilitation
- Decompression: Early motion. Soft dressing. Avoid direct pressure.
- Transposition: Immobilize 1-2 weeks to allow position to stabilize, then ROM.
- Strengthening: Start at 6 weeks.
Rehabilitation Protocol
- Timeframe
- 0-2 Weeks
- Goals
- Wound healing, Edema control, Nerve gliding
- Precautions
- Avoid resisted flexion
- Timeframe
- 2-6 Weeks
- Goals
- Full ROM, Scar management, Isometrics
- Precautions
- No heavy lifting
- Timeframe
- 6-12 Weeks
- Goals
- Progressive strengthening, Work hardening
- Precautions
- Monitor for recurrence
Outcomes
- Sensory recovery typically precedes motor.
- Motor recovery: Unpredictable in severe cases (McGowan III). "Time is muscle." Intrinsic atrophy acts as a poor prognostic sign.
- Intrinsic function may not fully return in elderly or long-standing cases (over 1 year).
Factors Influencing Recovery
- Age: Patients over 50 years have poorer outcomes.
- Duration: Symptoms over 1 year correlate with incomplete recovery.
- Severity: Pre-operative muscle atrophy is difficult to reverse.
- Site: Distal lesions (wrist) reinnervate faster than proximal (elbow), but intrinsic demand is high.
Expect paresthesia resolution first, then strength. Sensation may take months.
Guidelines, Registries & Global Practice
Global Epidemiology
- Cubital tunnel syndrome is the second most common compressive (entrapment) neuropathy of the upper limb, after carpal tunnel syndrome.
- Reported population incidence is approximately 20-30 per 100,000 person-years, with a male predominance and a peak in the 5th-6th decades.
- Strong associations: prolonged or repetitive elbow flexion, prolonged direct pressure on the elbow, diabetes, smoking, manual/vibrating-tool occupations and prior elbow trauma (tardy ulnar palsy after cubitus valgus).
- Guyon's canal (ulnar tunnel) syndrome is far less common; ganglion cyst is the single most frequent space-occupying cause, followed by hook-of-hamate pathology and ulnar artery aneurysm/thrombosis (hypothenar hammer syndrome).
Side-by-Side Guideline Comparison
- Position on Conservative Care
- First-line for mild/intermittent disease: activity modification, night extension splinting
- Position on Surgery
- Surgery for failed conservative care or motor involvement; in-situ release first-line for idiopathic disease
- Position on Conservative Care
- Trial of nerve-protection advice and splinting in mild cases
- Position on Surgery
- Simple decompression preferred for primary idiopathic CuTS; transposition reserved for instability/deformity
- Position on Conservative Care
- Advice on avoiding provocative positions improves mild symptoms; added splinting/gliding no extra benefit
- Position on Surgery
- Decompression and transposition equivalent in efficacy; decompression has fewer wound complications
- Position on Conservative Care
- Limited role once structural deformity present
- Position on Surgery
- Transposition favoured when nerve sits in a scarred or deformed (valgus) bed or after distal humerus fixation
Across AAOS/ASSH, BOA/BSSH, the Cochrane review and European consensus, the core message is identical: for primary idiopathic cubital tunnel syndrome, simple in-situ decompression is first-line surgery. Transposition (subcutaneous or submuscular) is reserved for a subluxating nerve, cubitus valgus / post-traumatic deformity, a scarred bed, or revision.
Registry & High-Volume Evidence
- There is no large dedicated international registry for peripheral nerve decompression equivalent to the joint-replacement registries (NJR, AJRR, AOANJRR), so practice rests on RCTs and systematic reviews rather than registry survivorship data.
- Large administrative and insurance datasets consistently show cubital tunnel surgery is among the most frequently performed elective hand operations worldwide, with low but non-trivial revision rates (incomplete release and persistent symptoms being the leading reasons for reoperation).
High- vs Limited-Resource Practice Variation
- High-resource settings: ready access to nerve conduction studies/EMG and high-resolution ultrasound for diagnosis and lesion localisation; endoscopic in-situ release available in selected centres; day-case surgery under regional or local anaesthesia.
- Limited-resource settings: diagnosis is predominantly clinical (Tinel's, elbow flexion test, Froment's, pattern of wasting) with selective or no electrodiagnostics; open simple decompression under local anaesthesia is the pragmatic default — low-cost, effective, and avoids dependence on imaging or specialised endoscopic equipment.
- Globally, the threshold to operate is driven by motor involvement and failure of conservative measures, not by access to advanced imaging.
Special Scenarios
Ulnar Tunnel Syndrome
- Causes: Ganglion cyst (most common - 50%), Hook breakdown (Golfer), Ulnar Artery Aneurysm (Hammer syndrome), Cyclist Palsy.
Akahori Classification
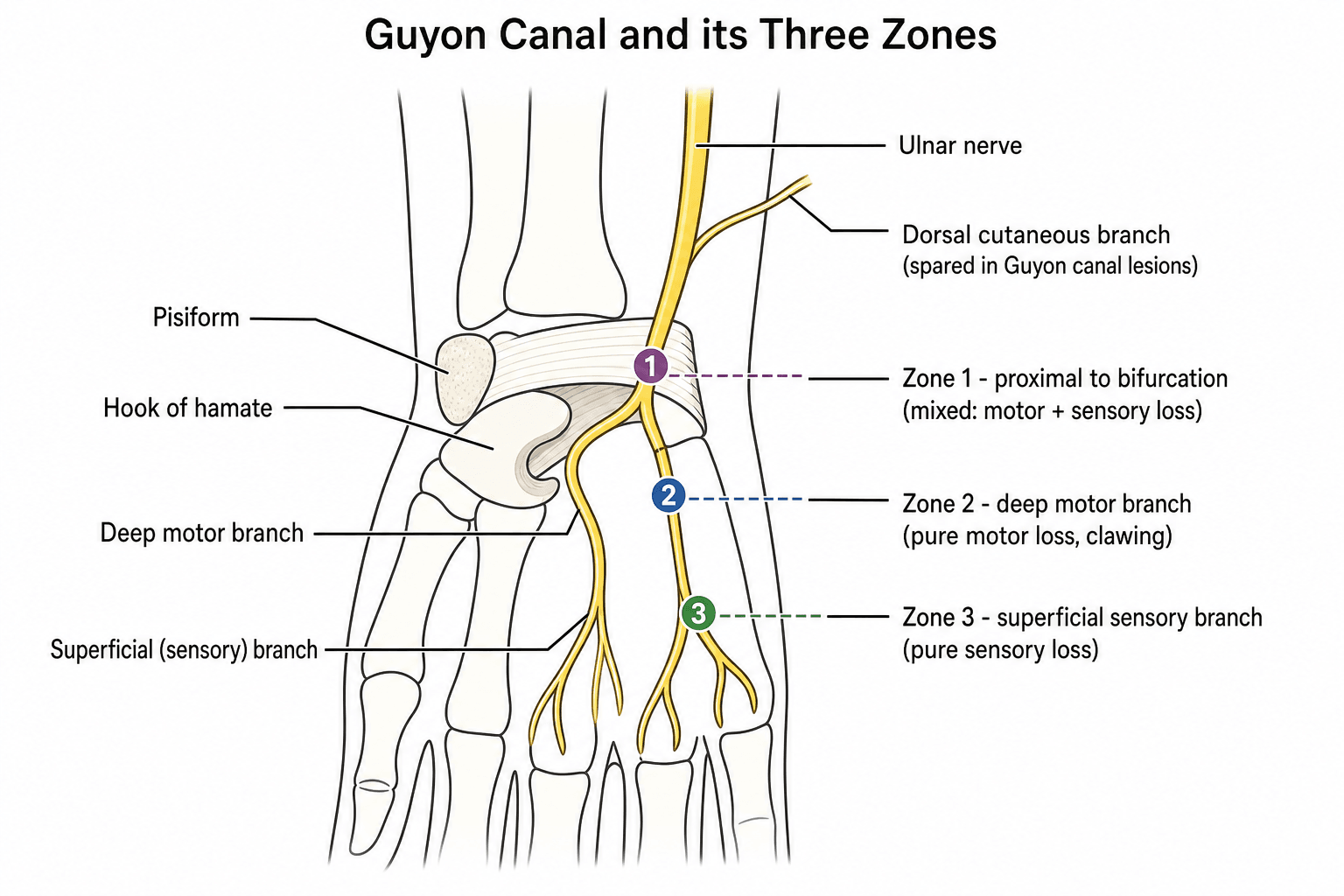
- Location
- Proximal to bifurcation
- Contents
- Motor + Sensory
- Symptoms
- Muscle weakness + Sensory loss (digits)
- Location
- Distal to bifurcation (Around hook)
- Contents
- Deep Motor Branch
- Symptoms
- Motor weakness ONLY (Claw hand)
- Location
- Distal (Superficial)
- Contents
- Superficial Sensory Branch
- Symptoms
- Sensory loss ONLY (No motor deficit)
- Treatment: Decompression of tunnel, address pathology (remove cyst).
Anatomical knowledge of these zones aids in localizing the lesion.
Tardy Ulnar Nerve Palsy
Tardy ulnar nerve palsy is a delayed ulnar neuropathy at the elbow that develops months to years after an old elbow injury. The classic cause is a childhood lateral condyle fracture that goes to nonunion or malunion, producing a progressive cubitus valgus deformity; the increased carrying angle stretches and tethers the ulnar nerve over the medial epicondyle, causing a slow traction and friction neuropathy. Supracondylar malunion, old distal humeral fractures and chronic elbow osteoarthritis can do the same.
The presentation is a gradual ulnar neuropathy - paraesthesia in the ulnar digits, intrinsic weakness and wasting, and clawing - appearing long after an injury the patient may have forgotten. The key examination clue is a valgus elbow with a positive Tinel's sign over a nerve that is often palpably subluxing or thickened.
Because the nerve sits in a deformed and often scarred bed, anterior transposition (subcutaneous or submuscular) is generally preferred over simple in-situ decompression, sometimes alongside correction of the underlying deformity.
A late ulnar neuropathy in a patient with a valgus elbow points to tardy ulnar nerve palsy from an old fracture, classically a childhood lateral condyle nonunion. Because the nerve lies in a deformed, scarred bed, transposition is usually preferred over simple in-situ release.
HILAHand Intrinsics (Ulnar Supplied)
Hook:Ulnar nerve is HILA-rious (supplies the HILA muscles).
Controversies & Areas of Uncertainty
For idiopathic disease, RCTs and the Cochrane review show equivalence, and decompression wins on complications. Genuine debate remains over the subluxating nerve — Bartels found decompression effective even with subluxation, yet many surgeons still transpose an unstable nerve to avoid a mobile, vulnerable target.
Systematic-review data favour endoscopic release on outcomes and complications, but the evidence is non-randomised and learning-curve sensitive. Open in-situ release remains the global default; endoscopy is centre- and surgeon-dependent.
Whether ultrasound or MRI should be routine rather than selective is unsettled. Ultrasound has only modest sensitivity (Pompe/Beekman), so a normal scan cannot exclude disease; many advocate reserving imaging for atypical, recurrent or mass-suspicious cases.
There is no agreed cut-off for how long to persist with conservative care, or a precise electrodiagnostic threshold mandating surgery. The pragmatic consensus: operate for progressive motor loss, wasting, or failure of 3-6 months of nerve-protection measures.
MCQ Practice Points
Q: What is the most common anomaly of upper limb innervation? A: Martin-Gruber Anastomosis. (Median to Ulnar in forearm). Occurs in 15-20% of people.
Q: Which nerve innervates the First Dorsal Interosseous (1st DI)? A: Ulnar Nerve (deep motor branch). The 1st DI abducts the index finger and is a key contributor to pinch strength. Its bulk in the first web space is one of the earliest sites of visible wasting in ulnar neuropathy. (Do not confuse with Wartenberg's sign, which reflects unopposed little-finger abduction.)
Q: Which muscle is tested by Froment's Sign? A: Adductor Pollicis. It is the only hypothenar/thumb muscle supplied by the Ulnar nerve (besides deep head of FPB).
Q: What distinguishes Zone I from Zone II injury at Guyon's Canal? A: Zone I (proximal to bifurcation) causes mixed motor and sensory loss. Zone II (deep branch only) causes pure motor weakness of interossei with sparing of hypothenar sensation.
Q: What is the positive finding in the elbow flexion test for cubital tunnel syndrome? A: Paresthesias in the ring/small fingers within 60 seconds of holding the elbow maximally flexed with the wrist extended.
Ulnar Nerve Vivas
Practise clinical reasoning and management decisions out loud
“A patient presents with clawing of the ring and little fingers. Explain the mechanism and the 'Ulnar Paradox'.”
“You are performing a cubital tunnel decompression. What are the key sites of compression you must release?”
“A cyclist complains of numbness in the little finger but has normal grip strength. Localization?”
“Post-operatively, your patient complains of numbness over the medial proximal forearm and pain when resting the elbow on a table. What has happened?”
Key Anatomy
- C8-T1 Origin
- Arcade of Struthers (8cm proximal)
- Osborne's Ligament (Cubital Tunnel)
- FCU Heads (Entry to forearm)
- Guyon's Canal (Pisohamate ligament)
Branches
- No branches in Arm
- Muscular: FCU, FDP (Medial 1/2)
- Dorsal Cutaneous: 5cm proximal to wrist (Spared in wrist lesions)
- Deep Branch: Motor to intrinsics
- Superficial Branch: Sensory to digits
Clinical Signs
- Froment's Sign (Thumb IP flexion)
- Wartenberg's Sign (Pinky abduction)
- Jeanne's Sign (Thumb MCP hyperextension)
- Duchenne's Sign (Clawing of ring/little)
Surgical Pearls
- Protect MABCN
- Release 5-8cm proximal (septum)
- Release FCU fascia distal
- Check for subluxation
Evidence Base
Bartels RCT: Simple Decompression vs Anterior Subcutaneous Transposition
- Single-blind RCT, 152 patients (75 simple decompression, 77 anterior subcutaneous transposition), 1-year follow-up
- Good/excellent outcome equivalent: 49/75 (SD) vs 54/77 (AST), not statistically different
- Complication rate significantly lower with simple decompression (9.6% vs 31.1%; risk ratio 0.32, 95% CI 0.14-0.69)
- Outcome was equivalent even in the presence of nerve subluxation
Zlowodzki Meta-analysis of RCTs
- Meta-analysis of 4 randomized controlled trials (2 submuscular, 2 subcutaneous transposition)
- No difference in clinical scores (standardised mean difference -0.04, 95% CI -0.36 to 0.28) across 261 patients
- No difference in postoperative motor nerve-conduction velocity (100 patients)
- Narrow confidence intervals exclude any clinically meaningful difference
Cochrane Review: Treatment for Ulnar Neuropathy at the Elbow
- Six RCTs, 430 participants, moderate-quality evidence
- No difference between simple decompression and transposition for clinical improvement (RR 0.93, 95% CI 0.80-1.08) or nerve conduction
- Transposition associated with more wound infections (RR 0.32, 95% CI 0.12-0.85)
- In mild disease, advice on avoiding provocative positions improved symptoms; added splinting/nerve gliding gave no further benefit
Open vs Endoscopic In-Situ Decompression
- Systematic review of outcomes (494 patients) and complications (1108 patients)
- Pooled good/excellent outcome 92.0% endoscopic vs 82.7% open in-situ
- Lower odds of complications with endoscopic release (pooled odds ratio 0.28, 95% CI 0.125-0.625)
- Evidence base limited to small, mostly non-randomised case series
Ultrasonographic Diagnosis: CSA, Diameter and Swelling Ratio
- Prospective cohort: 191 patients (137 with ulnar neuropathy at the elbow) plus 73 healthy controls
- Enlarged ulnar nerve diameter, cross-sectional area and swelling ratio all distinguished cases (p less than 0.01)
- Specificity 78-87%, sensitivity 42-61%, area under ROC curve 0.75-0.77 — comparable across the three measures
- Real-world diagnostic accuracy lower than earlier optimistic reports
Critical Review of Ultrasonography in UNE
- Systematic review of ultrasonography clinical trials in ulnar neuropathy at the elbow
- Increased cross-sectional area at the elbow is the most consistently reported abnormality
- Diagnostic accuracy appears good but several studies had methodological flaws and differing CSA cut-offs
- Role of ultrasound is promising but not yet firmly established