Linked vs Unlinked Design | Rheumatoid Arthritis Classic Indication | Ulnar Nerve Protection Critical | Triceps Management Essential
- Classic indication: Rheumatoid arthritis with severe joint destruction and minimal bone loss
- Ulnar nerve management: Must be identified, protected, and often transposed anteriorly
- Triceps-sparing approach: Preserves extensor mechanism, allows early rehabilitation
- Weight restriction: Lifetime limit of 2-5kg lifting to reduce bushing wear and loosening
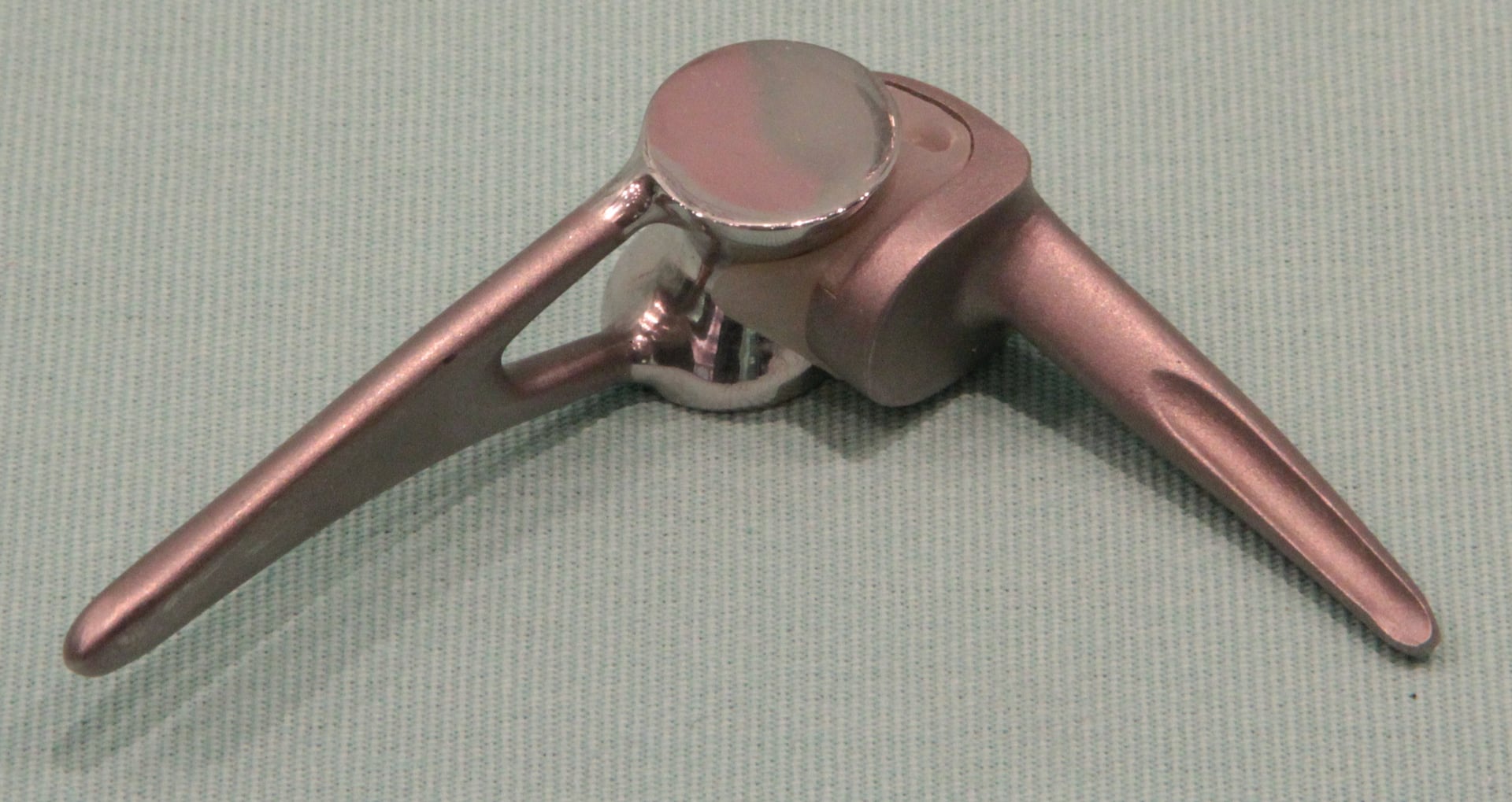
- Linked implants: Sloppy hinge design allows 7-10 degrees varus-valgus laxity to reduce stress
- “Linked TEA is preferred for bone loss, instability, or revision - relies on hinge for stability
- “Ulnar nerve palsy is the most common neurological complication - always identify and protect
- “Triceps insufficiency causes significant functional deficit - extensor mechanism is critical
- “Aseptic loosening at ulna is more common than humerus due to smaller bone stock
Linked (semi-constrained) implants have a sloppy hinge mechanism allowing 7-10 degrees varus-valgus laxity. Used when soft tissues are incompetent or bone loss is significant. Unlinked implants rely on intact ligaments and soft tissues for stability. Similar concepts to constrained vs unconstrained knee arthroplasty.
The ulnar nerve must be identified, protected, and often transposed anteriorly during TEA. It runs posterior to the medial epicondyle and is at risk during surgical approach. Ulnar nerve palsy is the most common neurological complication (5-10%). Pre-existing neuropathy is common in RA patients.
The triceps extensor mechanism is critical for elbow function. Approaches include triceps-on (Kocher), triceps-sparing (Bryan-Morrey), and triceps-reflecting (paratricipital). Triceps insufficiency causes significant functional limitation. Triceps-sparing approach allows earlier rehabilitation.
Patients must adhere to lifelong weight restrictions (2-5kg) to minimize stress on the prosthesis. This prevents accelerated bushing wear and loosening. TEA is a semi-permanent solution - patients must understand activity limitations. Non-compliance leads to early failure.
- Bone/Soft Tissue Status
- Intact bone stock, competent ligaments
- Implant Choice
- Unlinked (resurfacing) TEA
- Key Pearl
- Preserves bone, relies on soft tissues
- Bone/Soft Tissue Status
- Deficient bone, incompetent collaterals
- Implant Choice
- Linked (semi-constrained) TEA
- Key Pearl
- Hinge provides stability when soft tissues fail
- Bone/Soft Tissue Status
- Comminuted, osteoporotic bone
- Implant Choice
- TEA (linked) or hemiarthroplasty
- Key Pearl
- Better outcomes than ORIF in elderly with comminution
- Bone/Soft Tissue Status
- Significant bone deficiency
- Implant Choice
- Revision TEA with long stems and allograft
- Key Pearl
- Complex revision with bone grafting
LINCLINC - Linked TEA Indications
Hook:Use LINKed TEA when there is LINC - Ligament incompetence, Instability, No bone, Complex revision
Overview and Epidemiology
Total elbow arthroplasty (TEA) replaces the ulnohumeral and radiocapitellar articulations to restore a pain-free, functional arc of motion. It is performed less frequently than hip or knee arthroplasty due to the elbow's complex biomechanics and higher complication rates.
Epidemiology:
- Rheumatoid arthritis historically the most common indication (60-70%)
- Post-traumatic arthritis and acute distal humerus fractures increasing
- More common in females due to higher RA prevalence
- Complex anatomy and biomechanics make surgery technically demanding
Functional arc of motion for activities of daily living is 30-130 degrees flexion and 50 degrees each of pronation and supination. TEA aims to restore this arc while providing stability and pain relief. Most patients achieve a functional arc post-operatively.
Etiology - Indications for TEA:
- Rheumatoid arthritis: Classic indication with severe joint destruction
- Primary osteoarthritis: Less common, typically with stiffness
- Post-traumatic arthritis: Following distal humerus fracture malunion
- Hemophilic arthropathy: Severe recurrent hemarthrosis
- Distal humerus fracture in elderly: Comminuted, osteoporotic bone
- Failed ORIF: Non-union or malunion with arthritis
- Unreconstructable fracture: When ORIF not possible
- Age greater than 65 with low demand and comminution: Better outcomes than ORIF
Contraindications:
- Absolute: Active infection, inadequate soft tissue coverage, non-functional upper limb (e.g., stroke)
- Relative: Young age (under 60), high activity level, prior septic arthritis, severe bone loss without reconstruction options
Anatomy and Biomechanics
The Elbow Joint Complex:
The elbow is a trochoginglymoid joint consisting of three articulations:
- Bones
- Trochlea - trochlear notch
- Motion
- Flexion-extension (hinge)
- Stability Contribution
- Primary stability in extension
- Bones
- Capitellum - radial head
- Motion
- Pronation-supination (pivot)
- Stability Contribution
- Secondary stabilizer, axial load (40%)
- Bones
- Radial head - radial notch of ulna
- Motion
- Forearm rotation
- Stability Contribution
- Minimal contribution to elbow stability
Stability - Primary and Secondary Stabilizers:
Primary stabilizers: Ulnohumeral articulation (coronoid is critical), medial collateral ligament (MCL - anterior bundle), lateral collateral ligament complex (LUCL). Secondary stabilizers: Radial head, capsule, common flexor and extensor origins. Loss of primary stabilizers leads to instability that may require linked TEA.
- Anterior bundle: Most important, origin at medial epicondyle, inserts on sublime tubercle of coronoid
- Posterior bundle: Tightens in flexion
- Transverse ligament: Minimal contribution
- Radial collateral ligament
- Lateral ulnar collateral ligament (LUCL): Most important, prevents posterolateral rotatory instability
- Annular ligament: Stabilizes proximal radioulnar joint
The ulnar nerve passes posterior to the medial epicondyle in the cubital tunnel. It lies between the medial epicondyle and olecranon, covered by Osborne's ligament (arcuate ligament). The nerve is at risk during medial approach and must be identified early. Pre-existing ulnar neuropathy is common in RA patients (15-25%).
Triceps Mechanism:
- Three heads: Long head (scapula), lateral head (humerus), medial head (deep, humerus)
- Inserts on olecranon via common triceps tendon
- Critical for elbow extension and function
- Preservation or secure repair essential for TEA success
Classification Systems
TEA Implant Design Classification
Based on constraint and stability mechanism:
- Mechanism
- Sloppy hinge with 7-10 degrees varus-valgus
- Indications
- Bone loss, instability, RA, revision
- Key Features
- Coonrad-Morrey, Discovery Elbow
- Mechanism
- Ball and socket, relies on soft tissues
- Indications
- Primary OA, intact ligaments
- Key Features
- Kudo, Capitellocondylar
- Mechanism
- Can switch between linked and unlinked
- Indications
- Intraoperative flexibility
- Key Features
- Latitude, Nexel
- Mechanism
- Distal humerus replacement only
- Indications
- Acute fracture in elderly
- Key Features
- Stryker Discovery Hemi
Linked (semi-constrained) TEA uses a sloppy hinge mechanism with 7-10 degrees of varus-valgus laxity. This is NOT a fully constrained hinge - the laxity allows stress transfer to soft tissues rather than concentrating all forces at the bone-cement interface, reducing loosening risk.
The implant table lists hemiarthroplasty but never develops it - and it is the key examinable alternative for the younger or higher-demand patient in whom both ORIF and TEA are unattractive.
- What it is: replacement of only the distal humeral articular surface (trochlea and capitellum), articulating against the native ulna and radial head.
- Indication: an isolated, unreconstructable distal humeral articular fracture (or selected AVN/nonunion) in a patient who is too young or active for the lifelong restrictions of TEA but in whom stable ORIF is not feasible.
- Prerequisites (critical): the medial and lateral columns must be intact or reconstructable (the implant has no cross-column stem fixation and depends on the columns and ligament origins), and the collateral ligaments must be competent or repairable - if the columns or ligaments are deficient, a linked TEA is the correct choice instead.
- The key advantage over TEA: it preserves bone and, crucially, has no lifelong 2-5 kg weight restriction, making it suited to the more active patient.
- The main concern: progressive wear/erosion of the native articulating surfaces (the ulnar greater sigmoid notch and radial head) over time, plus the technical difficulty of matching native trochlear sizing; the evidence base is smaller than for TEA.
Exam point: distal humeral hemiarthroplasty is the option for the younger/active patient with an unreconstructable articular distal humeral fracture and intact columns and ligaments - its big advantage over TEA is no weight restriction, but it requires competent columns/ligaments and risks native-side wear; deficient columns or ligaments mandate a linked TEA.
Clinical Assessment
History:
- Location: Diffuse elbow pain, may radiate to forearm
- Timing: Activity-related and rest pain (advanced arthritis)
- Character: Grinding, mechanical symptoms
- Function: Difficulty with ADLs (dressing, eating, hygiene)
- Stiffness: Loss of extension common, functional arc compromised
- Weakness: Grip strength reduced, difficulty lifting
- Instability: Giving way, recurrent dislocations
- Neurological: Numbness in ulnar distribution (ring, little fingers)
Physical Examination:
Inspection and Range of Motion
- Inspect: Swelling, muscle wasting (forearm), rheumatoid nodules, surgical scars, carrying angle
- Active ROM: Flexion (normally 145 degrees), extension (0-5 degrees hyperextension), pronation (80 degrees), supination (85 degrees)
- Passive ROM: May be preserved despite pain
- Functional arc: 30-130 degrees flexion, 50 degrees pronation/supination
Specific Tests
- Purpose
- MCL integrity
- Technique
- Elbow at 20-30 degrees flexion, apply valgus stress
- Positive Finding
- Medial opening, pain
- Purpose
- LUCL integrity / PLRI
- Technique
- Supination, valgus, axial load while extending from flexion
- Positive Finding
- Clunk or apprehension
- Purpose
- Extensor mechanism function
- Technique
- Resist elbow extension against gravity
- Positive Finding
- Weakness indicates triceps pathology
- Purpose
- Ulnar nerve irritation
- Technique
- Tap posterior to medial epicondyle
- Positive Finding
- Tingling in ulnar distribution
Pre-operative ulnar nerve evaluation is essential. Document any pre-existing sensory or motor deficits. Consider nerve conduction studies if neuropathy is suspected. Pre-existing ulnar neuropathy is common in RA (cubital tunnel syndrome). This affects surgical planning and informed consent.
Systemic Assessment for RA Patients
- Cervical spine: Atlantoaxial instability - flexion/extension radiographs if suspected
- Other joints: Hip, knee, shoulder involvement may affect priorities
- Medications: DMARDs, biologics may need adjustment peri-operatively
- Skin quality: Rheumatoid nodules, fragile skin at surgical site
PRIMEPRIME - Pre-Op Assessment
Hook:Before TEA, patients must be in PRIME condition - Prior surgery, Range, Infection, Muscle, Electrical nerve
Investigations
Imaging Studies:
Essential first-line imaging:
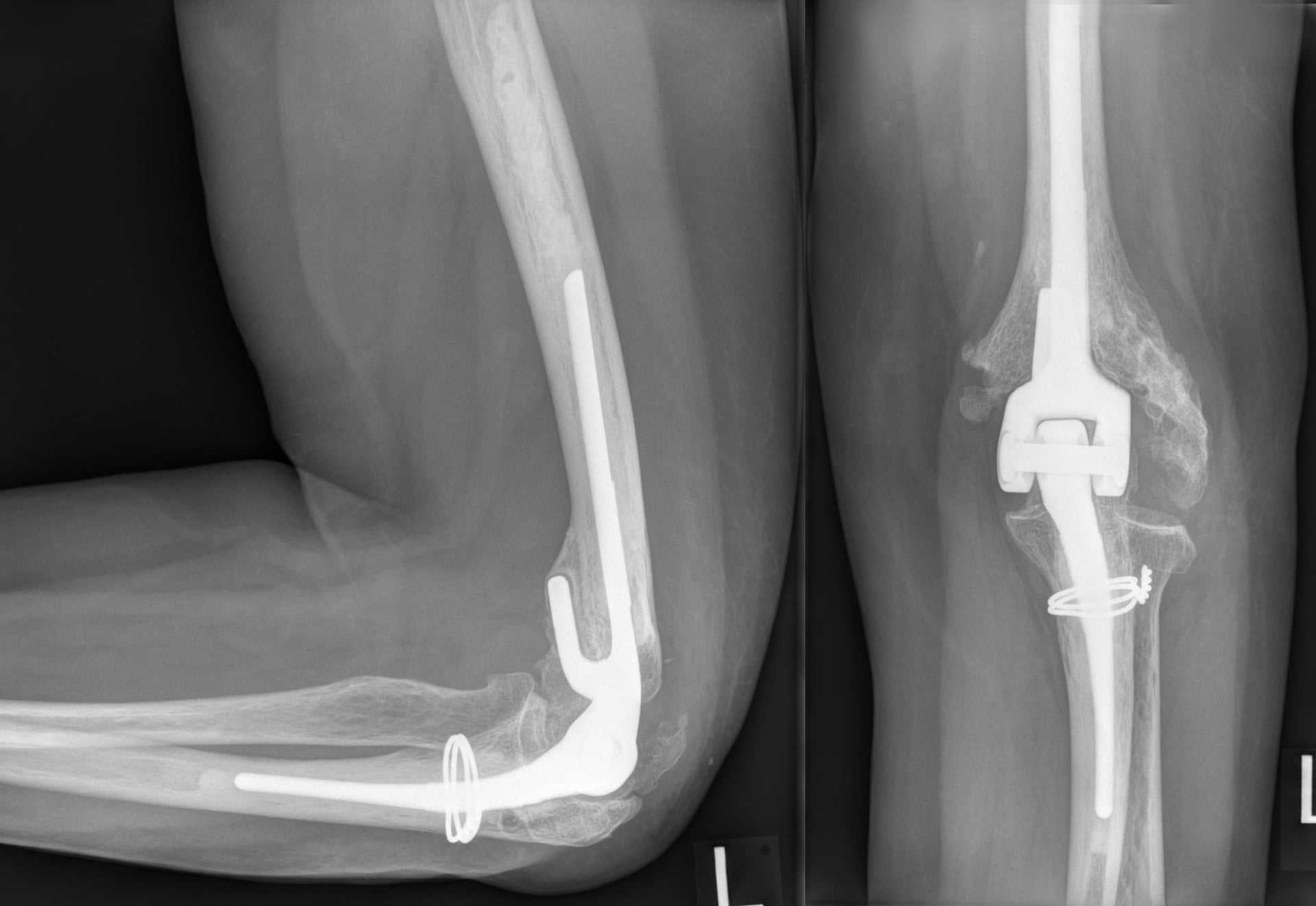
- AP and lateral elbow radiographs
- Assess joint space, bone quality, deformity
- Measure carrying angle, alignment
- Look for loose bodies, osteophytes
- Assess bone stock for implant sizing
Advanced bony assessment:
- 3D reconstruction for complex deformity
- Bone stock assessment for revision
- Templating for implant selection
- Assess previous hardware if present
- Useful for acute fractures
Radiographic Features of Elbow Arthritis:
- Joint Space
- Minimal narrowing
- Osteophytes
- Small osteophytes
- Bone Changes
- Minimal sclerosis
- Joint Space
- Moderate narrowing
- Osteophytes
- Moderate osteophytes
- Bone Changes
- Subchondral sclerosis and cysts
- Joint Space
- Bone on bone
- Osteophytes
- Large osteophytes / ankylosis
- Bone Changes
- Severe destruction, bone loss
Differential Diagnosis of the Painful Arthritic Elbow:
- Typical Patient
- Female, polyarticular, seropositive
- Distinguishing Features
- Symmetrical erosions, periarticular osteopenia, synovitis, nodules; raised RF/anti-CCP
- Implication for TEA
- Classic indication; linked design for ligament/bone deficiency
- Typical Patient
- Male, manual worker, dominant arm
- Distinguishing Features
- Osteophytes, preserved joint space, terminal-extension block, mechanical locking
- Implication for TEA
- Unlinked or debridement (O-K) if ligaments intact
- Typical Patient
- Any age, prior fracture/surgery
- Distinguishing Features
- Asymmetric destruction, deformity, hardware, heterotopic ossification
- Implication for TEA
- Higher revision/complication risk; linked design
- Typical Patient
- Immunosuppressed, RA, diabetic
- Distinguishing Features
- Acute pain, warmth, raised ESR/CRP, positive aspirate
- Implication for TEA
- Absolute contraindication until eradicated
- Typical Patient
- Older, metabolic risk factors
- Distinguishing Features
- Acute flares, tophi, chondrocalcinosis, crystals on aspirate
- Implication for TEA
- Treat medically; arthroplasty rarely needed
Laboratory Studies:
- Inflammatory markers: ESR, CRP - rule out infection, assess disease activity
- Rheumatoid factor, anti-CCP: Confirm RA diagnosis
- HbA1c: Diabetes control (infection risk)
- Nutritional markers: Albumin, lymphocyte count (healing capacity)
- Joint aspiration: If any concern for infection - cell count, culture, crystals
Infection must be excluded before proceeding with elective TEA. History of prior septic arthritis is a relative contraindication. If any suspicion, aspirate the joint and send for cell count, culture, and inflammatory markers. Proceed with surgery only when infection is definitively ruled out.
Management Algorithm
Stepwise Management of Elbow Arthritis
Management Pathway for Elbow Arthritis
Conservative treatment trial:
- Activity modification and lifestyle counselling
- NSAIDs for pain and inflammation
- Physiotherapy for range of motion and strength
- Intra-articular corticosteroid injection (limited effect)
- Disease-modifying therapy for RA (optimize medical treatment)
Options before arthroplasty:
- Arthroscopic debridement: Remove loose bodies, osteophytes
- Outerbridge-Kashiwagi (O-K) procedure: Fenestration of olecranon fossa
- Synovectomy: RA with recurrent synovitis but minimal joint destruction
- Interposition arthroplasty: Distraction with fascia lata graft (young active)
Indications for TEA:
- Failed conservative management
- Severe joint destruction with pain and functional limitation
- Low-demand patient (age greater than 60 typical)
- Accepts lifelong weight restriction
- Adequate soft tissue coverage
For most patients with end-stage elbow arthritis who meet appropriate criteria, TEA provides reliable pain relief and functional improvement.
Surgical Technique
Pre-Operative Preparation
- Size humeral and ulnar components on radiographs
- Assess for bone loss requiring augmentation
- Plan approach based on prior surgery, soft tissue quality
- Optimize RA disease activity (coordinate with rheumatologist)
- Consider DMARD/biologic holiday peri-operatively (controversial)
- Glycaemic control for diabetics
- Nutrition assessment and optimization
Biologic agents (TNF inhibitors, rituximab) are associated with increased infection risk. Consider withholding 2-4 weeks pre-operatively depending on agent half-life. Balance infection risk against disease flare. Multidisciplinary decision with rheumatology.
Informed Consent:
- Weight restriction lifelong (2-5kg)
- Potential for ulnar nerve symptoms
- Infection risk (2-5%)
- Loosening and revision possibility
- Triceps weakness possibility
- Periprosthetic fracture risk
Document all consent points and ensure patient understands activity restrictions.
Complications
- Incidence
- 10-15% at 10 years
- Risk Factors
- High activity, obesity, poor cement technique
- Management
- Revision TEA with long stems and bone graft
- Incidence
- 2-5%
- Risk Factors
- RA, diabetes, immunosuppression, prior surgery
- Management
- I&D vs two-stage revision vs resection arthroplasty
- Incidence
- 5-10%
- Risk Factors
- Pre-operative neuropathy, traction injury, direct injury
- Management
- Observation (most resolve), exploration if no recovery
- Incidence
- 5%
- Risk Factors
- Poor repair, avulsion, RA with poor tissue
- Management
- Revision repair, tendon reconstruction
- Incidence
- 5-10%
- Risk Factors
- Soft tissue incompetence, component malposition
- Management
- Convert to linked TEA or revision
- Incidence
- 5-10%
- Risk Factors
- High activity, non-compliance with weight restriction
- Management
- Bushing exchange if components stable
- Incidence
- 5%
- Risk Factors
- Trauma, osteoporosis, stress risers
- Management
- Fixation or revision depending on site
Deep infection after TEA is a serious complication. Options include: (1) I&D with polyethylene exchange for acute infection with stable components, (2) Two-stage revision with antibiotic spacer for chronic infection, (3) Resection arthroplasty (flail elbow) if unable to eradicate infection. Antibiotic suppression may be considered in selected cases.
Aseptic Loosening:
- Most common mode of failure long-term
- Ulnar component loosens more often than humeral (smaller bone stock)
- Presents with pain, decreased motion, radiographic lucency
- Revision with long-stemmed components and bone grafting
Periprosthetic fracture is listed above as a complication, but a viva will expect a classification to structure management. The Mayo (O'Driscoll) classification is based on the fracture location relative to the components and incorporates implant fixation and bone stock.
- Type I - condyles/columns: fracture of the articular condyles or columns (the bone around, but not along, the stem). The components are stable, so these are usually managed non-operatively (or by symptomatic fragment excision).
- Type II - along the stem: fracture of the humeral or ulnar shaft alongside a stemmed component. Subclassified by bone stock and fixation - good bone with a well-fixed stem -> ORIF; poor bone or a loose stem -> revision with a longer-stemmed component plus or minus strut allograft.
- Type III - beyond the stem tip: a diaphyseal fracture distal/proximal to the tip of the stem. With a well-fixed stem, treat it like a standard diaphyseal fracture (ORIF); with a loose stem, revise.
The governing principle for any periprosthetic fracture is to assess three things - location, implant fixation (loose vs well-fixed), and bone stock: a well-fixed stem with good bone is fixed, whereas a loose stem or poor bone stock is revised with a long-stemmed component and bone graft.
Exam point: classify TEA periprosthetic fractures by the Mayo system - Type I (condyle/column, usually non-operative), Type II (along the stem, ORIF if well-fixed/good bone vs revision if loose/poor bone), Type III (beyond the stem tip, treat as a diaphyseal fracture if the stem is well-fixed) - the decision always hinges on stem fixation and bone stock.
TEARSTEARS - TEA Complications
Hook:Total Elbow Arthroplasty Results in TEARS if complications occur - Triceps, Erosion, Aseptic loosening, Rupture, Sepsis
Rehabilitation
Post-Operative Rehabilitation Protocol
Protection phase:
- Posterior splint in 90 degrees flexion
- Elevation for swelling control
- Finger and wrist motion encouraged
- Wound care and monitoring
- Ulnar nerve function assessment
Gentle mobilization:
- Begin active-assisted range of motion
- Gravity-assisted extension
- Forearm rotation exercises
- Avoid resisted extension (protects triceps repair)
- Hinged brace may be used
Controlled strengthening:
- Progress to active motion
- Light resistance exercises
- Continue avoiding heavy lifting (weight restriction education)
- Functional activities for ADLs
- Continue triceps protection
Maintenance phase:
- Transition to home exercise program
- Reinforce lifelong weight restriction (2-5kg)
- Return to low-demand activities
- Regular clinical and radiographic follow-up
- Annual surveillance recommended
Lifelong weight restriction (2-5kg) is critical for TEA longevity. Patient education and compliance are essential. Repetitive or single heavy lifting accelerates bushing wear, component loosening, and periprosthetic fracture risk. This must be discussed at consent and reinforced at every follow-up visit.
Outcomes
Results and Survivorship:
Functional Outcomes:
- Significant pain relief in greater than 90% of patients
- Improvement in range of motion (typically 30-130 degree arc achieved)
- Improved ability to perform activities of daily living
- Patient satisfaction generally high when expectations managed
Comparison by Indication:
- Pain Relief
- Excellent
- ROM Improvement
- Good
- Survivorship
- 85-90% at 10 years
- Notes
- Best studied indication
- Pain Relief
- Good
- ROM Improvement
- Fair
- Survivorship
- 75-85% at 10 years
- Notes
- Higher revision rate
- Pain Relief
- Good
- ROM Improvement
- Variable
- Survivorship
- 80-90% at 5 years
- Notes
- Better than ORIF in elderly
- Pain Relief
- Fair-Good
- ROM Improvement
- Fair
- Survivorship
- 60-70% at 10 years
- Notes
- Complex, higher failure
Factors Affecting Outcome:
- Patient selection (low-demand, compliant with restrictions)
- Surgical technique and implant position
- Bone quality and soft tissue health
- Adherence to weight restrictions
- Underlying diagnosis (RA better than post-traumatic)
Guidelines, Registries & Global Practice
Global Epidemiology and Practice Variation:
Total elbow arthroplasty is a low-volume procedure worldwide, typically 1-2% of the volume of hip or knee arthroplasty. Historically rheumatoid arthritis dominated the case mix, but improved disease-modifying and biologic therapy has steadily reduced the rheumatoid burden, and most national series now report a rising proportion of acute distal humeral fractures and post-traumatic arthritis. Linked semiconstrained designs predominate in most high-income health systems, with unlinked resurfacing implants reserved for selected primary osteoarthritis or younger patients with competent soft tissues.
- Position on TEA
- Endorses TEA for end-stage inflammatory and selected post-traumatic arthritis, and primary TEA for non-reconstructable distal humeral fractures in low-demand elderly
- Evidence Basis / Comment
- Supported by Level 1 RCT evidence (McKee) for the fracture indication
- Position on TEA
- Recommends TEA be concentrated in specialist upper-limb units; primary TEA reasonable for unreconstructable elderly distal humeral fractures
- Evidence Basis / Comment
- Reflects NJR low-volume data and the volume-outcome relationship
- Position on TEA
- Mandatory recording of every elbow replacement in the National Joint Registry; supports informed consent with registry survival data
- Evidence Basis / Comment
- Registry surveillance rather than a clinical guideline per se
- Position on TEA
- Linked semiconstrained TEA favoured for fracture and revision settings; emphasises soft-tissue and ulnar nerve handling
- Evidence Basis / Comment
- Consensus and registry-informed (Nordic, Norwegian, Danish registries)
- The Danish registry cohort (Plaschke 2014) reported 90% 5-year and 81% 10-year survival, with higher revision for unlinked and fracture-sequelae cases
- The Norwegian Arthroplasty Register and Nordic Arthroplasty Register Association confirm low national volumes and higher revision burden than large-joint arthroplasty
- The National Joint Registry (England, Wales, NI, IoM) captures every elbow replacement and demonstrates a clear volume-outcome relationship favouring high-volume centres
- The AOANJRR (Australia) reports TEA outcomes annually, with linked designs predominant and rheumatoid/post-traumatic arthritis the leading indications
- In many countries, access to specialised upper-limb and revision elbow surgeons is limited in rural and remote regions, with transfer to metropolitan or specialist centres required for complex revision; telehealth increasingly supports pre-operative assessment and long-term surveillance of regional patients
- TEA appears in both written and viva components of the fellowship examination
- Focus on indications, implant selection (linked vs unlinked), surgical approach, and complications
- Level 1 evidence comparing TEA with ORIF for elderly distal humeral fractures (McKee RCT) is frequently examined
MCQ Practice Points
Q: What is the key difference between linked and unlinked total elbow arthroplasty? A: Linked (semi-constrained) TEA has a sloppy hinge mechanism connecting humeral and ulnar components, providing inherent stability. It allows 7-10 degrees of varus-valgus laxity. Unlinked TEA relies on intact soft tissues (collateral ligaments) for stability. Linked is preferred for RA, bone loss, instability; unlinked for primary OA with intact ligaments.
Q: What is the most common neurological complication of total elbow arthroplasty? A: Ulnar nerve palsy (5-10%). The ulnar nerve runs posterior to medial epicondyle and is at risk during medial exposure. Pre-existing ulnar neuropathy is common in RA patients (15-25%). Most post-operative palsies are neurapraxia and recover spontaneously. The nerve should be identified early, protected, and often transposed anteriorly.
Q: What is the expected 10-year survivorship of total elbow arthroplasty for rheumatoid arthritis? A: 85-90% 10-year survivorship. Rheumatoid arthritis remains the best indication for TEA with the most predictable outcomes. Post-traumatic arthritis and younger patients have lower survivorship. Most failures are due to aseptic loosening or infection.
Q: Why is preservation or secure repair of the triceps mechanism critical in total elbow arthroplasty? A: The triceps is the only extensor of the elbow. Triceps insufficiency leads to significant functional deficit with inability to extend against gravity. Unlike the knee where quadriceps weakness is partly compensated, there is no alternative elbow extensor. Secure repair with transosseous sutures is essential.
Q: What is the recommended lifelong weight restriction after total elbow arthroplasty? A: 2-5 kg repetitive or single lifting. This is critical for implant longevity. The elbow transmits 3-4x body weight during activities, and the prosthesis is subject to significant forces. Non-compliance leads to accelerated bushing wear, loosening, and periprosthetic fracture. This must be emphasized at every follow-up.
Medicolegal Considerations
Key medicolegal points for total elbow arthroplasty:
-
Informed consent must include:
- Lifelong weight restriction (2-5kg) and activity limitations
- Ulnar nerve palsy risk (5-10%), often temporary
- Infection risk (2-5%), may require multiple surgeries
- Aseptic loosening and need for future revision
- Triceps weakness possibility
- Periprosthetic fracture risk
-
Pre-operative documentation:
- Comprehensive neurological examination including ulnar nerve
- Document pre-existing ulnar symptoms (common in RA)
- Assessment of previous surgery, skin quality, infection history
- Radiographs and CT showing bone stock
-
Operative notes:
- Ulnar nerve identification, management, transposition if performed
- Triceps management and repair technique
- Implant details, cement technique
- Range of motion at completion
-
Post-operative care:
- Clear rehabilitation protocol provided
- Weight restriction counselling documented
- Follow-up plan with annual surveillance
Additional Clinical and Access Considerations:
- Higher body mass index and heavy manual occupation are relative contraindications to weigh in patient selection
- Access to specialised revision elbow surgery may be limited in regional, rural, or remote areas, with onward referral to specialist centres for complex cases
- Where occupational injury or compensation is involved, document occupational demands and activity restrictions thoroughly
- Coordinate peri-operative biologic and DMARD management with rheumatology for inflammatory arthritis patients
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman with a 30-year history of rheumatoid arthritis presents with severe right elbow pain and stiffness. She has difficulty with activities of daily living including feeding and hygiene. She has failed medical management including biologics and has had one intra-articular steroid injection with minimal relief. On examination, range of motion is 50-100 degrees, she has a 10-degree fixed flexion deformity, and there is crepitus with motion. Radiographs show bone-on-bone narrowing of the ulnohumeral joint with erosions and cyst formation. How would you manage this patient?”
“An 82-year-old woman presents after a fall with a displaced comminuted intra-articular distal humerus fracture. CT scan shows a highly comminuted C3 fracture with significant articular involvement and osteoporotic bone. She lives independently, is right-hand dominant, and has well-controlled diabetes. Her pre-injury function was normal. What are your treatment options and which would you recommend?”
“A 70-year-old woman is 48 hours post total elbow arthroplasty for rheumatoid arthritis. She reports numbness in her ring and little fingers and is unable to spread her fingers apart. On examination, she has intrinsic weakness with loss of finger abduction. Her wound is healing well with no signs of hematoma. How do you assess and manage this complication?”
Key Anatomy and Biomechanics
- Elbow: Trochoginglymoid joint - ulnohumeral (hinge), radiocapitellar (pivot), proximal radioulnar
- Primary stabilizers: Ulnohumeral joint (coronoid critical), MCL anterior bundle, LUCL
- Secondary stabilizers: Radial head, capsule, common flexor/extensor origins
- Ulnar nerve: Posterior to medial epicondyle in cubital tunnel - at risk during surgery
- Functional arc: 30-130 degrees flexion, 50 degrees pronation/supination
Implant Selection
- Linked (semi-constrained): Sloppy hinge with 7-10 degrees varus-valgus laxity - for RA, bone loss, instability
- Unlinked (resurfacing): Relies on soft tissues - for primary OA with intact ligaments
- Cemented fixation: Gold standard especially for poor bone quality (RA, osteoporosis)
- Linked preferred for trauma (ligament integrity uncertain), revision, bone deficiency
Surgical Approach
- Bryan-Morrey: Triceps-reflecting - good exposure, most commonly used for primary TEA
- Triceps-sparing (paratricipital): Preserves extensor mechanism, limited exposure
- Ulnar nerve: Identify early, protect, transpose anteriorly subcutaneously
- Triceps repair: Critical for function - crossed cruciate suture through drill holes
Complications
- Aseptic loosening: 10-15% at 10 years, ulna loosens more than humerus
- Infection: 2-5%, two-stage revision or resection arthroplasty if cannot eradicate
- Ulnar nerve palsy: 5-10%, most neurapraxia that recovers
- Triceps insufficiency: 5%, significant functional deficit if occurs
- Bushing wear: Linked TEA complication from high activity or non-compliance
Outcomes and Key Pearls
- Survivorship: 85-90% at 10 years, 75-80% at 15 years
- RA has best outcomes, post-traumatic arthritis has higher failure
- Weight restriction: 2-5kg lifelong - critical for implant longevity
- TEA vs ORIF for elderly distal humerus fracture: TEA has better outcomes (McKee RCT)
- Document pre-operative ulnar nerve status - medicolegal importance
Evidence Base
TEA vs ORIF for Distal Humeral Fractures in the Elderly (Landmark RCT)
- Multicentre prospective RCT comparing primary semiconstrained TEA with ORIF for displaced intra-articular (OTA 13C) distal humeral fractures in patients over 65
- 42 patients randomised (21 per arm); 5 patients allocated to ORIF were converted to TEA intra-operatively because stable fixation could not be achieved
- TEA produced significantly better Mayo Elbow Performance Scores at 3, 6, 12 and 24 months (e.g. 86 vs 73 at 2 years, p=0.015)
- Operative time averaged 32 minutes shorter with TEA (p=0.001)
- Reoperation rate 12% (3/25) for TEA vs 27% (4/15) for ORIF (not statistically significant)
Long-Term Survivorship of Coonrad-Morrey TEA in Rheumatoid Arthritis (461 Elbows, Mayo Clinic)
- Single-institution series of 461 primary Coonrad-Morrey linked semiconstrained TEAs for rheumatoid arthritis (387 patients), median follow-up 10 years (range 2-30)
- Survivorship free of revision or removal for any reason: 92% at 10 years, 83% at 15 years and 68% at 20 years
- Survivorship with aseptic loosening as the endpoint was 88% at 20 years
- Radiographic bushing wear in 23% but revision for isolated bushing wear in only 2%
- Risk factors for revision: male sex, concomitant traumatic pathology, and a polymethylmethacrylate ulnar component surface finish
Primary Linked TEA for Acute Distal Humeral Fractures (Systematic Review)
- PRISMA systematic review of 10 studies (269 patients) of primary TEA for acute distal humeral fractures
- Coonrad-Morrey implant used in 83%; Bryan-Morrey approach commonest (33.7%), triceps-reflecting management in 42%
- Mean postoperative arc 102.3 degrees flexion-extension and 145.8 degrees pronation-supination
- Mean Mayo Elbow Performance Score 89.5; excellent scores when surgery performed within 7 days of injury
- Overall complication rate 21.5%
Complications of Total Elbow Replacement (Systematic Review)
- Systematic review of the published complications of total elbow replacement across implant designs and indications
- Confirms that TEA carries a substantially higher complication burden than hip or knee arthroplasty
- Major complication categories: aseptic loosening, deep infection, ulnar neuropathy, triceps insufficiency, periprosthetic fracture and bushing/polyethylene wear
- Ulnar nerve dysfunction is the most frequent neurological complication and aseptic loosening the leading mechanical failure mode
- Highlights wide variation in complication definitions and reporting across studies
Implant Survival and Risk Factors for Revision (Danish Registry, 324 TEAs)
- Registry-based cohort of 324 primary TEAs (234 patients) in eastern Denmark, 1980-2008, mean follow-up 8.7 years
- Overall implant survival 90% at 5 years and 81% at 10 years
- Unlinked designs had a relative risk of revision of 1.9 (95% CI 1.1-3.2) compared with linked designs
- Fracture sequelae carried a relative risk of revision of 1.9 (95% CI 1.05-3.45) versus other indications
- Confirms inferior survival for unlinked implants and for post-traumatic/fracture-sequelae indications at population level
Linked Semiconstrained vs Unlinked TER in Inflammatory Arthritis
- Case-comparison series of 21 total elbow replacements in 14 juvenile idiopathic arthritis patients (14 unlinked Kudo 5, 7 linked Coonrad-Morrey), mean 11.7-year follow-up
- Survivorship with revision as endpoint 95% at 5 years and 68% at 10 years overall
- Ten-year survival similar between designs: 70% unlinked vs 69% linked
- Radiographic aseptic loosening was high in the unlinked group (85.7%), though many remained asymptomatic
- Bilateral replacement was an independent risk factor for revision within 10 years