Mirels Score for Impending Pathological Fracture
A Mirels score of 9 or more is an indication for prophylactic internal fixation — the predicted fracture risk exceeds one in three. A score of 7 or less can be managed with radiotherapy and surveillance. A score of 8 sits in the grey zone: individualise, leaning toward fixation for a solitary metastasis, an unreliable patient, or a painful lower-limb lesion. If you fix, fix before radiotherapy (irradiated bone heals poorly).
The Mirels Scoring System
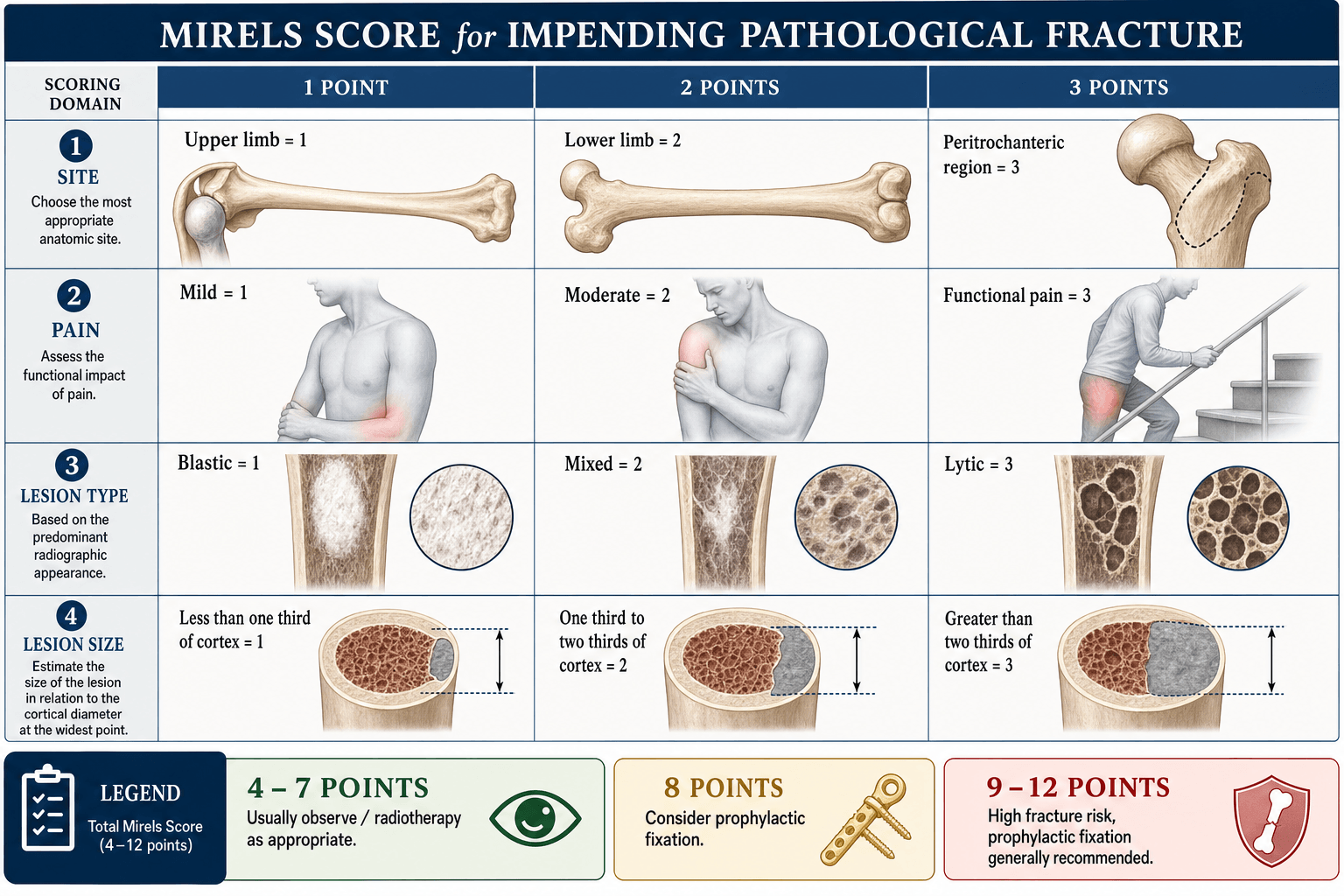

Each of the four variables is scored 1, 2, or 3. The total (4–12) stratifies fracture risk.
- 1 point
- Upper limb
- 2 points
- Lower limb
- 3 points
- Peritrochanteric
- 1 point
- Mild
- 2 points
- Moderate
- 3 points
- Functional (mechanical)
- 1 point
- Blastic
- 2 points
- Mixed
- 3 points
- Lytic
- 1 point
- Less than one-third
- 2 points
- One-third to two-thirds
- 3 points
- More than two-thirds
Site • Pain • Lesion • SizeThe four variables
Hook:Site, Pain, Lesion, Size — each scored 1 to 3, summed to 4–12. The 3-pointers (peritrochanteric, functional pain, lytic, over two-thirds cortex) are the danger values.
Functional (mechanical) pain means pain on weight-bearing or use that is reproducible and relieved by rest — it scores 3 and is the single most ominous symptom. Constant rest pain from the tumour itself is not the same thing.
Score Interpretation and Action
- Fracture Risk
- About 4 percent
- Recommended Action
- Radiotherapy and serial observation
- Key Consideration
- Reassess if pain increases or imaging changes
- Fracture Risk
- About 15 percent
- Recommended Action
- Individualised decision
- Key Consideration
- Lean to fixation if solitary metastasis, poor compliance, or lower-limb load
- Fracture Risk
- Over 33 percent
- Recommended Action
- Prophylactic internal fixation
- Key Consideration
- Fix first, then radiotherapy; allow immediate weight-bearing
Prophylactic fixation of an impending fracture is technically easier, carries lower morbidity, and allows earlier weight-bearing than fixation after a pathological fracture has occurred. The whole point of the score is to operate before the break.
Before You Score: Confirm It Really Is a Metastasis
The Mirels score answers "will this metastasis fracture?" — but it silently assumes the lesion is a metastasis. The single most important safety point an examiner will test is that a solitary bone lesion of unknown origin must never be internally fixed before it has been worked up and biopsied. Internally fixing (especially intramedullary nailing) a primary bone sarcoma that has been mistaken for a metastasis disseminates tumour along the entire bone and soft-tissue planes, converting a potentially limb-salvageable, curable tumour into one that costs the patient the limb or their life.
If a patient has no known primary cancer, or has a known cancer but a solitary bone lesion, treat the lesion as a possible primary bone sarcoma until proven otherwise. Complete the metastatic / tumour work-up first, refer to or discuss with a tumour unit, and obtain a biopsy (placed so the tract can be excised at definitive surgery, ideally by the team who will do the resection). Only once the diagnosis of metastasis is confirmed does the Mirels score become the right tool. In a patient with widespread known metastatic disease, a typical new lytic long-bone lesion can reasonably be treated as metastatic — but the threshold for biopsy should remain low.
Bone is one of the commonest sites of metastasis, and a focused work-up identifies the primary in the large majority of cases.
- What to do
- Ask about prior cancer, B-symptoms, breast/prostate/thyroid/renal/lung symptoms; examine breast, chest, abdomen, prostate, thyroid, lymph nodes
- Why
- Often reveals the likely primary and directs targeted imaging
- What to do
- FBC, ESR/CRP, U&E, calcium and bone profile, LFTs, PSA (men), serum/urine electrophoresis and free light chains (myeloma screen)
- Why
- Hypercalcaemia, a raised PSA or a paraprotein quickly narrow the diagnosis; myeloma is a key mimic that is treated very differently
- What to do
- Plain radiographs of the whole bone plus CT to quantify cortical destruction
- Why
- CT, not plain film, defines the true axial cortical involvement that drives the Mirels size points
- What to do
- CT chest/abdomen/pelvis; whole-body bone scan or PET; mammography/thyroid US as directed
- Why
- Finds the primary and other deposits; a solitary lesion changes the whole strategy
- What to do
- Image-guided needle (or open) biopsy through a planned, excisable tract after staging
- Why
- Confirms metastasis versus primary sarcoma versus myeloma BEFORE any fixation
BLT with a Kosher PickleCarcinomas that metastasise to bone
Hook:The five carcinomas that love bone: Breast, Lung, Thyroid, Kidney, Prostate — 'BLT with a Kosher Pickle'. Renal and thyroid are the hypervascular two that must be embolised pre-operatively.
Surgical Principles for Metastatic Bone Disease
When the Mirels score does indicate fixation, the operation follows principles that differ from fixing an ordinary fracture, because the construct must outlive a diseased, non-healing bone in a patient who may have limited time and physiological reserve.
- Protect the whole bone, not just the lesion. Metastatic disease is rarely confined to one spot, and a second deposit can fracture distal to a short implant. Use a device that spans the entire bone — a long cephalomedullary nail for femoral and most long-bone lesions — so the whole bone is protected at one operation.
- Build a durable construct that does not rely on bone healing. The bone is unlikely to unite, so achieve immediate mechanical stability with cement augmentation (PMMA) of defects and screws, allowing full weight-bearing immediately. The implant should be expected to last the patient's lifetime.
- Replace, do not fix, when destruction is too extensive. For a destroyed femoral head/neck or extensive peri-articular bone loss, an endoprosthetic (tumour) replacement or arthroplasty is more reliable than internal fixation — fixation into bone that crumbles will fail.
- Embolise hypervascular metastases pre-operatively. Renal cell and thyroid metastases can bleed catastrophically; angiographic embolisation 24–48 hours before surgery dramatically reduces intra-operative blood loss.
- Coordinate adjuvant therapy. Give post-operative radiotherapy to the whole operated bone to control local tumour and reduce implant loosening — but fix first, then irradiate. Add bone-targeted agents (bisphosphonates or denosumab) to reduce skeletal events, and manage the patient through a multidisciplinary team with the oncologists, factoring expected survival into how aggressive the reconstruction should be.
A renal cell carcinoma metastasis is the classic exam trap on the operative side: it is lytic, expansile and extremely vascular. Fail to embolise it 24–48 hours before nailing and you can lose litres of blood. Always ask "what is the primary?" before operating — the answer changes both the work-up (biopsy?) and the operation (embolise?).
The upper limb scores low on Mirels (site = 1) but still needs thought. Because the humerus is non-weight-bearing, a humeral metastasis rarely reaches a Mirels total of 9, yet it can still fracture and a humeral pathological fracture is very disabling (the patient loses the arm for transfers, toileting and crutch or frame use). So the decision to fix a humeral lesion leans less on the Mirels number and more on pain, functional demand and cortical destruction: prophylactic fixation is reasonable for a painful lytic lesion with significant cortical loss, especially in a patient who needs that arm to mobilise. Fixation options differ from the femur — an antegrade locked intramedullary nail (protecting the whole bone) for diaphyseal lesions, a cemented plate-and-screw construct where the canal is unsuitable, and a proximal humeral (tumour) endoprosthesis when the head and neck are destroyed. The structure most at risk during humeral surgery is the radial nerve (spiral groove), which must be identified and protected. The principle is the same as the femur — span the whole bone, augment with cement, allow immediate use, irradiate afterwards.
Not every metastasis is fixed palliatively — a SOLITARY metastasis with favourable biology may be RESECTED. The default for widespread metastatic disease is durable palliative fixation, but a patient with a solitary bone metastasis from a tumour with a good prognosis — classically renal cell carcinoma or thyroid (and sometimes a long-interval solitary breast deposit) — can have prolonged survival or even cure, so the lesion is treated more like a primary tumour: wide en-bloc excision with endoprosthetic (or other) reconstruction rather than simply nailing through it. This is an oncological resection, not a palliative implant — it both removes all disease and gives the most durable reconstruction. The decision turns on tumour biology, confirmed solitary status (on full staging) and life expectancy — which is exactly why survival-prediction tools (PATHFx) and MDT discussion matter. The contrast to hold in a viva: widespread mets → spanning fixation built to last the patient's lifetime; a solitary favourable met → resect it.
Limitations and Modern Context
- It over-predicts fixation. In Damron's multi-observer study the score was highly sensitive (about 91 percent) but poorly specific (about 35 percent), so many lesions are fixed that would never have fractured. A score of 8 in particular is unreliable in isolation.
- The original threshold was actually 8, not 9. Mirels' 1989 paper recommended prophylactic fixation for scores of 8 or higher and irradiation for 7 or lower. Because the score over-predicts fracture, modern practice has largely shifted the operative threshold to 9 or more, treating 8 as an individualised grey zone — a common examiner "gotcha," so be ready to state both the original and the contemporary cut-off.
- The pain variable is subjective and has the poorest inter-observer agreement (Damron et al.); size and site are more reproducible. Confirm cortical involvement on CT, not plain film, before finalising the size points.
- CT-based structural rigidity analysis (and finite-element estimates of bone strength) predicts fracture more accurately than Mirels in research settings, but is not yet routine.
- Modern systemic therapy lowers the fracture rate at any given Mirels score, so interpret the number alongside treatment response and life expectancy. A very short prognosis may favour radiotherapy or a non-operative approach even at a high score.
- Mirels is validated for long-bone (mainly femoral) lesions; it does not apply to the spine (use SINS) or flat bones.
- It is not the only system. The older Harrington criteria define an impending fracture qualitatively (over 50 percent cortical destruction, a lytic lesion over 2.5 cm, a painful lesion persisting after radiotherapy, or avulsion of the lesser trochanter) and are still quoted alongside Mirels. Newer prognostic and machine-learning tools (for example PATHFx) estimate patient survival to help decide whether — and how aggressively — to operate, since there is no point in a lifetime-durable reconstruction in a patient with weeks to live. Mirels tells you the bone risk; survival tools tell you whether surgery is worthwhile.
Exam Viva
Practise clinical reasoning and management decisions out loud
“A 64-year-old with known breast cancer has a painful right hip. Radiographs show a lytic lesion in the peritrochanteric femur involving about half the cortex; she has mechanical pain on weight-bearing. How would you assess and manage this?”
“A 58-year-old man with no known cancer presents with thigh pain and a solitary, expansile, lytic lesion of the proximal femoral diaphysis involving more than two-thirds of the cortex. The referring team has booked him for an intramedullary nail. Are you happy to proceed? How do you manage this?”
The four variables (each 1–3)
- Site: upper limb (1), lower limb (2), peritrochanteric (3)
- Pain: mild (1), moderate (2), functional/mechanical (3)
- Lesion: blastic (1), mixed (2), lytic (3)
- Size: under one-third (1), one-third to two-thirds (2), over two-thirds of cortex (3)
Act on the total
- 7 or less: radiotherapy plus observe (risk about 4 percent)
- 8: individualise (grey zone)
- 9 or more: prophylactic fixation (risk over 33 percent)
- When fixing: fix first, irradiate after; protect the whole bone
Before you operate
- Solitary lesion / unknown primary: work up and BIOPSY first — never nail a possible sarcoma
- Primaries that spread to bone (BLT + Kosher Pickle): Breast, Lung, Thyroid, Kidney, Prostate
- Embolise hypervascular mets (renal, thyroid) 24–48 h pre-op
- Fix the whole bone (long cephalomedullary nail), cement defects, immediate weight-bear, lifetime-durable construct; replace if destruction is extensive; RT after fixation
Caveats
- Pain scoring is subjective (poorest reliability) — confirm size on CT
- Over-predicts fixation; modern systemic therapy lowers risk
- For long bones only — the spine uses SINS, not Mirels
- Harrington criteria are the qualitative alternative; survival tools (PATHFx) decide if surgery is worthwhile
Evidence Base
The Mirels score rests on a single retrospective derivation (Mirels 1989) that was never prospectively validated against fracture outcomes in a large modern cohort — so treat the numbers as a useful guide, not a precise probability. The consistent message of the later work (Damron 2003, Howard 2018) is that the score's reproducibility is only fair-to-moderate, with the pain variable the weakest link — which is why you confirm cortical involvement on CT and apply judgement at the borderline. Van der Linden's data make the deeper point that cortical destruction (size), more than the other variables, drives fracture risk. None of this evidence addresses the prior question — is the lesion even a metastasis? — which is why the biopsy/work-up rule sits outside the score and is the more important safety principle.
Metastatic disease in long bones: a proposed scoring system for diagnosing impending pathologic fractures
- Original four-parameter scoring system derived from 78 irradiated metastatic long-bone lesions (27 fractured and 51 did not within 6 months)
- Mean score 10 in the lesions that fractured versus 7 in those that did not; risk rose steadily as the score increased above 7
- Mirels recommended prophylactic fixation for scores of 8 or higher and irradiation for 7 or lower (modern practice often shifts the operative cut-off to 9)
- By score band the fracture risk is about 4 percent at 7 or less and over 33 percent at 9 or more
Critical evaluation of Mirels' rating system for impending pathologic fractures
- 53 observers across 5 experience levels scored 12 femoral cases; significant agreement across all experience levels
- Overall sensitivity was 91 percent but specificity only 35 percent — the score over-predicts fracture
- Mirels scoring outperformed unstructured clinical judgement (higher pooled odds ratio) regardless of experience
- Validated as a screening tool, but the authors concluded more specific parameters are needed
Comparative analysis of risk factors for pathological fracture with femoral metastases
- Prospective follow-up of 110 femoral lesions in 102 patients within a radiotherapy RCT; 14 fractures occurred
- Only axial cortical involvement over 30 mm (p=0.01) and circumferential cortical involvement over 50 percent (p=0.03) independently predicted fracture
- The full Mirels score was insufficiently specific to predict fracture (p=0.36), and most conventional risk factors over-estimated the actual fracture rate
The validity of the Mirels score for predicting impending pathological fractures of the lower limb
- Reliability study of 62 lower-limb metastasis patients scored by four observers
- Interobserver agreement was only fair for the total score (kappa about 0.29); intra-observer agreement was moderate to substantial
- Concluded the Mirels score is subjective and lacks reproducibility for the total score, so it should not be used as a stand-alone rule