Intermetatarsal Nerve Entrapment
- 3rd Web Space: Most common location (65%), followed by 2nd web (30%).
- NOT a True Neuroma: Perineural fibrosis from compression, not nerve tumor.
- Mulder's Click: Pathognomonic - palpable/audible click with lateral metatarsal squeeze.
- Conservative First: Wide shoes, metatarsal pad, corticosteroid injection (30-40% response).
- Surgical Neurectomy: Dorsal (most common) or plantar approach; expect permanent numbness.
- “3rd web space most common (not 2nd)
- “Mulder's click is pathognomonic sign
- “Not a true neuroma - it's perineural fibrosis
- “Conservative fails in 60-70% - surgery indicated
- “Warn patient: numbness is EXPECTED after surgery
The 3rd web space is most common - NOT the 2nd.
- Mulder's Click: Compress metatarsal heads laterally while pressing web space plantarly. Positive = click + symptom reproduction.
- NOT a True Neuroma: Perineural fibrosis from compression, not neoplastic.
- Post-Op Numbness is EXPECTED: Warn patients they will have permanent numbness between affected toes after neurectomy.
- Stump Neuroma: Most common surgical complication (10-15%).
- Morton's Neuroma
- Web space (plantar)
- Metatarsalgia
- Under MT heads
- MTP Synovitis
- MTP joint
- Morton's Neuroma
- Burning, shooting
- Metatarsalgia
- Aching, pressure
- MTP Synovitis
- Aching, swelling
- Morton's Neuroma
- To adjacent toes
- Metatarsalgia
- Local
- MTP Synovitis
- Local
- Morton's Neuroma
- Mulder's click +ve
- Metatarsalgia
- Callus under MT
- MTP Synovitis
- Drawer test +ve
- Morton's Neuroma
- Removing shoes
- Metatarsalgia
- Rest
- MTP Synovitis
- Splinting
Overview and Epidemiology
Morton's Neuroma (interdigital neuroma, Morton's metatarsalgia) is a common cause of forefoot pain representing compression neuropathy of the common digital nerve.
Terminology
- Misnomer: Not a true neuroma (not neoplastic)
- Correct Term: Interdigital nerve compression or perineural fibrosis
- Historical: Named after Thomas Morton (1876), though Durlacher described it earlier (1845)
Epidemiology
- Prevalence: 30% of patients with forefoot pain
- Gender: Female predominance 8:1 (high heels, narrow shoes)
- Age: 4th-6th decade most common
- Bilateral: 15-20% bilateral involvement
Web Space Distribution
- 3rd Web: 65% (between 3rd and 4th metatarsals) - MOST COMMON
- 2nd Web: 30% (between 2nd and 3rd metatarsals)
- 4th Web: 3% (rare)
- 1st Web: 2% (very rare)
- Multiple: 2-3% have involvement of more than one web space
Why 3rd Web Most Common?
- Junction of medial and lateral plantar nerve branches
- Nerve thicker at this level
- More tethered → less mobile → more susceptible to compression
Pathophysiology and Anatomy
Relevant Anatomy
- Branches of medial and lateral plantar nerves
- Pass beneath transverse metatarsal ligament
- Divide into proper digital nerves to adjacent toes
- Receives branches from BOTH medial and lateral plantar nerves
- Results in thicker, less mobile nerve
- More susceptible to compression
Pathophysiology
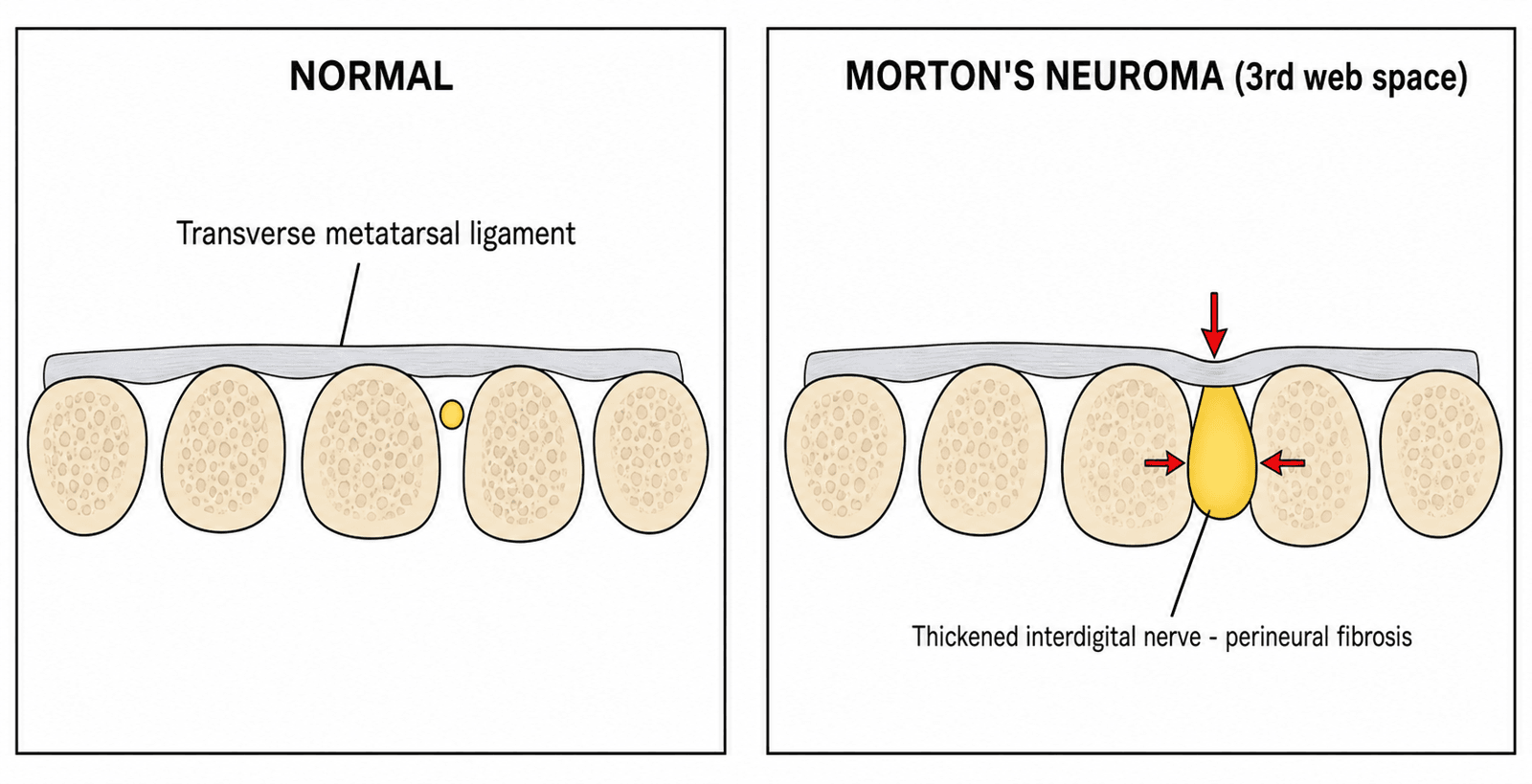
- Nerve passes between metatarsal heads
- Compressed against transverse metatarsal ligament (above)
- Metatarsal heads compress from sides
- Toe extension stretches nerve
- Perineural fibrosis (NOT neoplastic)
- Demyelination and axonal degeneration
- Renaut bodies (subperineurial fibrosis)
- Endoneurial and epineurial fibrosis
- Small vessel thrombosis and arteriolar thickening
Risk Factors
- Footwear: High heels (transfers weight forward), narrow toe box
- Foot Type: Pes planus, hypermobile first ray
- Activities: Running, ballet, activities with repetitive forefoot loading
- Anatomical: Long metatarsals, tight intermetatarsal space
Clinical Features
History
- Location: Web space (plantar aspect)
- Quality: Burning, shooting, electric shock-like
- Radiation: To adjacent toes (3rd and 4th in 3rd web neuroma)
- Numbness: Tingling or numbness in affected toes
- Aggravating: Tight shoes, high heels, walking, prolonged standing
- Relieving: Removing shoes, massaging forefoot, rest
- Night pain (consider tumor, infection)
- Swelling (synovitis, gout)
- Constitutional symptoms
- Multiple toe involvement (peripheral neuropathy)
Physical Examination
Mulder's Test (Key Examination)
- Hold foot with one hand around metatarsal heads
- Apply lateral compression (squeeze metatarsals together)
- With other hand, press affected web space from plantar to dorsal
- Positive = palpable/audible CLICK + symptom reproduction
- Sensitivity: 62-98%
- Specificity: 95%
- Highly specific but variable sensitivity
Web Space Compression Test
- Direct pressure on affected web space (plantar and dorsal)
- Reproduces symptoms
- Less specific than Mulder's
Sensory Examination
- May have decreased sensation in adjacent toes
- Two-point discrimination may be abnormal
- Often normal early in disease
Investigations
Clinical Diagnosis
- Diagnosis is primarily CLINICAL
- Imaging not always required if classic presentation
- Used to confirm diagnosis or exclude other pathology
Ultrasound
- Hypoechoic, ovoid mass in web space
- Often at level of metatarsal heads
- Dynamic compression may demonstrate lesion
- Widely available, low cost
- No radiation
- Dynamic assessment
- Operator-dependent
- Lesions more than 5mm are significant
- Correlation with symptoms improves with size
MRI
- Atypical presentation
- Failed treatment (exclude other pathology)
- Preoperative planning for large or recurrent neuromas
- T1: Low to intermediate signal mass
- T2: Low signal (fibrosis)
- Located between metatarsal heads
Diagnostic Injection
- Local anaesthetic injection into web space
- Relief confirms diagnosis
- Can be combined with corticosteroid for treatment
Morton's neuroma is a CLINICAL diagnosis. Imaging confirms but a positive Mulder's click with classic symptoms is often sufficient for diagnosis and conservative treatment initiation.
Management
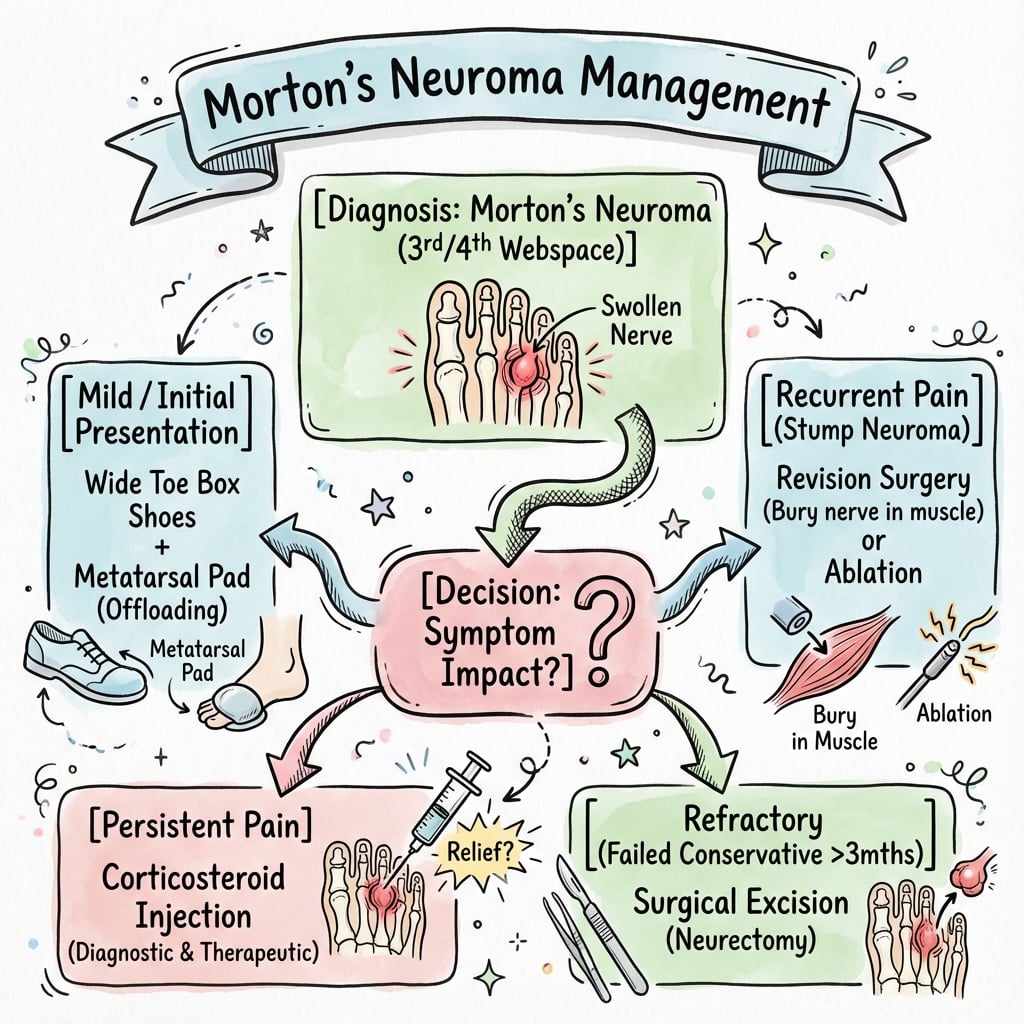
Non-Operative Management
- Wide toe box (MOST IMPORTANT)
- Low heel (under 2.5cm)
- Soft, cushioned sole
- Avoid pointed shoes
- Placed PROXIMAL to metatarsal heads
- Spreads metatarsals apart
- Reduces nerve compression
- 50-60% improvement with shoe mods + pad
- Short-term symptom relief
- Not disease-modifying
- 30-40% long-term relief
- Temporary response common
- Technique: Inject into web space from dorsal
- Multiple injections increase risk of fat pad atrophy
- Maximum 3 injections recommended
- Alcohol sclerosing injections (30% ethanol)
- Multiple sessions required
- Variable results (60-80% in some studies)
- 30-40% achieve adequate relief
- 60-70% eventually require surgery
- Conservative trial 3-6 months before surgery
Neurectomy involves excising the nerve, so permanent numbness between the affected toes is an EXPECTED outcome, not a complication. Patients MUST be counselled about this preoperatively to avoid dissatisfaction.
Complications
Surgical Complications
- Incidence
- 10-15%
- Risk Factors
- Insufficient proximal resection, traction
- Prevention/Management
- Adequate proximal cut, avoid tension
- Incidence
- 100%
- Risk Factors
- Expected outcome (not complication)
- Prevention/Management
- Warn all patients preoperatively
- Incidence
- 5-10%
- Risk Factors
- Incomplete excision, adjacent web neuroma
- Prevention/Management
- Confirm diagnosis, adequate resection
- Incidence
- 5-8%
- Risk Factors
- Plantar approach, hypertrophic scar
- Prevention/Management
- Prefer dorsal approach when possible
- Incidence
- 2-3%
- Risk Factors
- Diabetes, poor sterility
- Prevention/Management
- Standard perioperative antibiotics
- Incidence
- 3-5%
- Risk Factors
- Altered gait mechanics
- Prevention/Management
- Address forefoot mechanics, orthotics
Occurs in 10-15% of cases. The cut nerve end forms a painful neuroma at the stump. Prevention includes adequate proximal resection without excessive traction. Management includes revision surgery with more proximal resection into the plantar fat pad.
Neurectomy involves excising the nerve, so permanent numbness between the affected toes is an EXPECTED outcome. Patients MUST be counselled about this preoperatively to avoid dissatisfaction. This is not a complication but a predictable consequence of the procedure.
Guidelines, Registries & Global Practice
Global Epidemiology
- One of the commonest causes of forefoot neuralgia worldwide; strongly associated with constrictive footwear and elevated heels
- Marked female predominance (commonly quoted around 8:1) across populations; peak in the 4th-6th decades
- 3rd web space dominates, followed by the 2nd; multiple/bilateral involvement in a minority
- Lower reported prevalence in habitually barefoot or wide-footwear populations, supporting a footwear-driven mechanical aetiology
Guidelines & Society Positions (Side by Side)
- AAOS / AOFAS (US)
- Clinical first; Mulder's sign
- BOFAS / NICE (UK)
- Clinical; ultrasound as first imaging
- EFORT / European consensus
- Clinical with imaging confirmation
- AAOS / AOFAS (US)
- Ultrasound (cost-effective)
- BOFAS / NICE (UK)
- Ultrasound preferred; MRI if atypical
- EFORT / European consensus
- Ultrasound or MRI (equivalent sensitivity)
- AAOS / AOFAS (US)
- Footwear/orthoses, then injection
- BOFAS / NICE (UK)
- Footwear/metatarsal dome, then injection
- EFORT / European consensus
- Footwear, padding, injection trial
- AAOS / AOFAS (US)
- After failed conservative trial
- BOFAS / NICE (UK)
- After failed conservative trial
- EFORT / European consensus
- After failed conservative trial
- AAOS / AOFAS (US)
- Expected numbness, stump neuroma
- BOFAS / NICE (UK)
- Expected numbness, recurrence
- EFORT / European consensus
- Expected numbness, scar/recurrence
Registry & Evidence Notes
- No dedicated implant registry applies (no implant is used); evidence is driven by RCTs (steroid injection) and surgical case series rather than arthroplasty-style registries
- Imaging meta-analysis confirms ultrasound is equivalent to MRI for detection and is the more cost-effective first-line test
- Economic modelling supports an injection-first pathway (steroid then alcohol) before surgery when conservative measures fail
High- vs Limited-Resource Practice Variation
- Well-resourced settings: ultrasound-guided diagnosis and injection, day-case dorsal neurectomy, MRI for atypical/recurrent cases
- Limited-resource settings: clinical diagnosis with Mulder's sign and footwear/padding emphasised; diagnostic local-anaesthetic injection substitutes for advanced imaging; surgery reserved for refractory disease
- Workforce: depending on jurisdiction, surgery is performed by orthopaedic foot-and-ankle surgeons or, where licensed, podiatric surgeons; complex/revision cases are typically referred to specialist foot-and-ankle units
Special Considerations
Multiple Neuromas
- 2-3% have multiple web space involvement
- MRI helpful for preoperative planning
- May require staged surgery
- Higher risk of complications
Recurrent Morton's Neuroma
- Stump neuroma (most common)
- Incomplete excision
- Adjacent web space neuroma (missed)
- Confirm diagnosis (MRI, diagnostic injection)
- Conservative measures first
- Revision surgery with proximal resection
- Consider plantar approach for better visualization
Differential Diagnosis
- Metatarsalgia: Pain under metatarsal heads, no radiation
- Stress Fracture: Point tenderness over bone, swelling
- MTP Synovitis: Joint swelling, positive Drawer test
- Freiberg's Disease: 2nd MT head AVN, adolescent female
- Plantar Plate Injury: MTP instability, Drawer positive
- Peripheral Neuropathy: Multiple toes, bilateral
Alcohol Sclerosing Injection & Minimally Invasive Ablation
The topic repeatedly names alcohol sclerosing injection, radiofrequency ablation and cryoneurolysis as non-operative alternatives without developing them. These are targeted nerve-ablation techniques positioned between corticosteroid injection and open neurectomy — for patients who have failed footwear and steroid but wish to avoid surgery and its expected numbness.
Alcohol (Ethanol) Sclerosing Injection
- Principle: Dilute ethanol is neurotoxic — it produces chemical (Wallerian) degeneration of the common digital nerve, effectively a "chemical neurectomy" without an incision.
- Technique: Ultrasound-guided injection of dilute ethanol (commonly around 20-30% ethanol mixed with local anaesthetic) into the web space around the neuroma, repeated as a series (often several injections at one-to-two-week intervals).
- Evidence: Case series report widely varying success (roughly 60-90% symptom relief), but the systematic review by Matthews et al judged sclerosing-injection studies to be of limited methodological quality, and durable high-level RCT evidence is lacking.
- Cautions: Extravasation of alcohol can cause skin necrosis, plantar fat-pad injury or local reactions; incomplete response and symptom recurrence are common.
Radiofrequency Ablation & Cryoneurolysis
- Radiofrequency ablation: Thermal lesioning of the nerve under image guidance; reported in small case series with promising short-term relief.
- Cryoneurolysis: Freezing (cryoablation) of the nerve to interrupt conduction; also limited to case-series evidence.
- Status: Both are minimally invasive, sensation-preserving in intent and repeatable, but neither has robust randomised support — they remain second-line options where surgery is declined or high-risk.
Where They Fit
- A reasonable trial after failed footwear/pad and steroid, before open surgery — supported by cost-effectiveness modelling (Ross et al) showing a sequential steroid-then-alcohol injection pathway can be the dominant strategy.
- Not a substitute for accurate diagnosis: confirm the lesion on ultrasound and exclude adjacent-space or alternative pathology first.
Alcohol sclerosing injection is a "chemical neurectomy" — dilute ethanol causes Wallerian degeneration of the digital nerve. It can spare an operation, but the evidence is case-series level, results vary widely, and skin/fat-pad injury from extravasation is the key hazard.
Nerve-Preserving Surgery: Intermetatarsal Ligament Decompression
The Controversies section raises "neurectomy versus nerve-preserving surgery" but never explains the decompression option. Decompression (neurolysis) treats Morton's neuroma as an entrapment rather than a mass — the deep transverse intermetatarsal ligament is divided to relieve compression while the nerve is left in continuity, preserving sensation and avoiding a stump neuroma.
Rationale
- Morton's neuroma is fundamentally a compressive neuropathy beneath the transverse metatarsal ligament, so releasing that ligament addresses the cause without sacrificing the nerve.
- Gauthier popularised isolated division of the transverse intermetatarsal ligament (decompression) as a nerve-sparing alternative to excision.
Techniques
- Open decompression / neurolysis: Dorsal incision, division of the transverse intermetatarsal ligament and external neurolysis of the common digital nerve; the nerve is preserved.
- Endoscopic decompression of the intermetatarsal nerve (EDIN): A minimally invasive endoscopic release of the ligament, aiming for quicker recovery and a smaller scar.
Trade-offs vs Neurectomy
- Advantages: Preserves toe sensation (no expected numbness), avoids stump neuroma, and if it fails, neurectomy remains available as a salvage.
- Disadvantages: Higher risk of incomplete relief and recurrence because the pathological nerve is left in situ; best suited to earlier disease or smaller lesions where fibrosis is limited.
- Selection: Larger, chronically fibrotic neuromas and clear mass lesions are generally better served by excision; decompression is attractive when sensation preservation is the priority.
Decompression divides the transverse intermetatarsal ligament and preserves the nerve — no expected numbness and no stump neuroma, but a higher recurrence rate than excision. It reframes Morton's neuroma as an entrapment, with neurectomy kept as the fallback if symptoms persist.
Controversies & Areas of Uncertainty
- Does corticosteroid add anything over local anaesthetic? The 2013 Edinburgh RCT (Thomson) showed benefit over placebo, but the 2017 double-blind RCT (Lizano-Diez) found steroid no better than anaesthetic alone — the durable advantage of the steroid component remains contested.
- Neurectomy vs nerve-preserving surgery. Decompression (transverse intermetatarsal ligament release) avoids permanent numbness and stump neuroma but carries a higher recurrence risk; excision sacrifices sensation but is more definitive. The optimal choice is unsettled and patient-specific.
- Dorsal vs plantar incision. The dorsal approach avoids a weight-bearing scar and allows earlier mobilisation; the plantar approach gives superior exposure and, when correctly placed, a low scar-problem rate. High-level comparative evidence is lacking — largely surgeon preference.
- Size threshold for significance. A commonly cited cut-off is greater than 5mm, but symptoms correlate imperfectly with size and asymptomatic lesions are seen on imaging — imaging should confirm, not drive, the diagnosis.
- Minimally invasive alternatives. Alcohol sclerosing injection, radiofrequency ablation and cryoneurolysis show promise in case series but lack robust RCT support; reported success rates vary widely and reflect heterogeneous protocols.
- Bursa vs nerve. Whether the dominant pain generator is perineural fibrosis or an associated intermetatarsal bursitis is debated, which partly explains variable response to injection placement.
MCQ Practice Points
Q: Which intermetatarsal space is MOST commonly affected by Morton's neuroma?
A: 3rd web space (65%) - NOT the 2nd. This is a common exam trap. The 3rd common digital nerve receives branches from both medial and lateral plantar nerves, creating a larger and more susceptible nerve.
Q: What is the histological nature of Morton's neuroma?
A: Perineural fibrosis - NOT a true neuroma. The pathology shows fibrosis around the digital nerve, not proliferation of nerve tissue. This is why it's more accurately called "interdigital neuritis" or "intermetatarsal bursal swelling."
Q: What is Mulder's test and how is it performed?
A: Squeeze the metatarsal heads together with one hand while applying pressure in the interspace from plantar aspect. Positive test: Painful click (Mulder's click) as the neuroma subluxes between metatarsal heads. Sensitivity 60-80%.
Q: What is the advantage of the dorsal approach over the plantar approach for neurectomy?
A: Dorsal approach avoids a plantar scar (weight-bearing surface) and allows immediate weight-bearing. The plantar approach has better direct visualization but requires non-weight-bearing for 3 weeks and risks painful plantar scarring.
Self-Assessment Quiz
At a Glance
Morton's neuroma is a compressive neuropathy of the common digital nerve, most commonly affecting the 3rd web space (65%), not the 2nd. It is NOT a true neuroma but rather perineural fibrosis from repetitive compression beneath the transverse metatarsal ligament, with an 8:1 female predominance. Patients report burning, shooting pain radiating to adjacent toes, often relieved by removing shoes. Mulder's click (palpable click with lateral metatarsal squeeze while pressing the web space) is pathognomonic. Conservative management (wide shoes, metatarsal pad, corticosteroid injection 30-40% response rate) is first-line. Surgical neurectomy (dorsal or plantar approach) achieves 80-85% good outcomes; permanent numbness between affected toes is expected and must be counseled. Stump neuroma (10-15%) is the most common surgical complication.
3MBMorton's Neuroma - 3MB
Hook:3MB - 3rd web, Mulder's click, Burning pain. The three key features of Morton's neuroma.
CLICKMulder's Test - CLICK
Hook:CLICK - perform Mulder's test to get the diagnostic click.
SWIMTreatment Ladder - SWIM
Hook:SWIM through treatment - Shoes, Wedge pad, Injection, then (neuro)Mectomy.
SNPComplications - SNaP
Hook:SNaP - Stump neuroma, Numbness (expected), Plantar scar. Key complications to discuss.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 48-year-old woman presents with burning pain in the forefoot radiating to the 3rd and 4th toes. The pain is worse with high heels and relieved by removing her shoes. Mulder's click is positive.”
“A 52-year-old woman has had Morton's neuroma symptoms for 9 months despite shoe modifications, metatarsal pad, and two corticosteroid injections. She wants to discuss surgical options.”
“A patient returns 6 months after Morton's neuroma excision with recurrent burning pain in the same web space. They are unhappy with the result.”
KEY FACTS
- 3rd web space MOST COMMON (65%) - not 2nd!
- NOT a true neuroma - perineural fibrosis
- Female 8:1, 4th-6th decade
- Burning pain radiating to adjacent toes
MULDER'S TEST
- Squeeze metatarsals laterally
- Press affected web space plantar to dorsal
- Positive = CLICK + symptom reproduction
- PATHOGNOMONIC (95% specificity)
CONSERVATIVE
- Wide toe box shoes (MOST IMPORTANT)
- Metatarsal pad PROXIMAL to MT heads
- Corticosteroid injection (30-40% relief)
- Trial 3-6 months before surgery
SURGERY
- Neurectomy - dorsal approach (most common)
- Divide transverse MT ligament, excise nerve
- 80-85% good results
- Plantar approach: better view but scar risk
COMPLICATIONS
- NUMBNESS is EXPECTED - warn patient
- Stump neuroma 10-15% (most common complication)
- Plantar scar pain if plantar approach
- Recurrence 10-20%
EXAM TIPS
- Always say '3rd web most common'
- Call it 'perineural fibrosis' not 'neuroma'
- Emphasize post-op numbness is EXPECTED
- Know Mulder's technique
Evidence Base
- 131 patients (85% female, mean age 53), ultrasound-guided injection
- Corticosteroid + anaesthetic vs anaesthetic alone (placebo)
- Global foot-health 14.1 VAS points better at 3 months (p=0.002)
- Neuroma size on ultrasound did not influence treatment effect
- 41 patients, double-blind, 3 injections each arm
- Corticosteroid + anaesthetic NOT superior to anaesthetic alone at 3 and 6 months
- 48.5% requested surgical excision by study end (44% vs 53%, p=1.0)
- Tempers expectations of durable benefit from steroid
- 25 studies (7 RCTs, 18 case series); 8 interventions
- Corticosteroid injection reduced VAS pain vs control (WMD -5.3, 95% CI -7.5 to -3.2)
- Steroid superior to footwear/padding (OR 6.0, 95% CI 1.9 to 19.2)
- No single gold-standard non-surgical intervention identified
- 14 studies, surgery as reference standard
- Ultrasound sensitivity 0.91 vs MRI 0.90 (no significant difference, p=0.88)
- MRI pooled specificity 1.00; ultrasound 0.85
- Ultrasound is the most cost-effective first-line imaging
- 13 feet, mean 10.5-year follow-up after interdigital neurectomy
- VAS improved 8.6 to 2.4; good satisfaction in 61%
- 11/13 reported plantar numbness; 2 found it disabling
- Long-term results modestly worse than short/mid-term
- 51 feet / 56 neuromas, mean 54-month follow-up
- VAS pain fell from 8 to 0.4 after plantar excision
- Complications 7.1%, scar problems 5.2%
- Plantar scar not bothersome if correctly positioned
- 25 feet, recurrent interdigital neuroma, mean 75-month follow-up
- Primary excision success quoted at ~74% in literature
- Revision via dorsal approach: 78% excellent/good (SEFAS)
- All re-excised masses confirmed neuroma histologically
- Decision-analytic model after failed conservative care
- Sequential steroid then alcohol injection was the dominant strategy
- ICER $4402/QALY vs no treatment; favoured in 74% of simulations
- If alcohol success fell under 40%, steroid-only became most cost-effective
- Diagnosis is primarily clinical (web-space pain, Mulder's sign)
- Imaging (ultrasound first-line) to confirm or exclude alternatives
- Stepwise care: footwear/orthoses then injection then surgery
- Counsel expected post-neurectomy numbness and stump-neuroma risk