Systematic Assessment of Muscles, Tendons, Ligaments, and Soft Tissue Masses
Size: Greater than 5cm
Location: Deep to fascia
Growth: Rapid enlargement
Signal: Heterogeneous, necrosis
Margins: Irregular, infiltrative
Key: Any deep soft tissue mass greater than 5cm requires urgent specialist referral
- Normal tendons and ligaments are dark on all sequences (low signal)
- Increased tendon signal suggests degeneration or tear
- Muscle oedema: high T2/STIR, normal T1
- Fatty infiltration: high T1 signal within muscle
- Soft tissue masses: size greater than 5cm and deep location are red flags
- “Magic angle artefact: 55° orientation causes false tendon signal
- “Complete tear: discontinuity with retraction and haematoma
- “Partial tear: intratendinous signal without complete disruption
- “Goutallier classification for rotator cuff fatty infiltration
- “Lipoma: follows fat signal on all sequences
Soft tissue MRI interpretation requires understanding normal signal characteristics. Tendons should be dark - any increased signal is abnormal. For soft tissue masses, know the red flags: size greater than 5cm, deep to fascia, heterogeneous signal, and rapid growth suggest malignancy.
SLIMEDescribing a Soft Tissue Mass
Hook:Any deep mass greater than 5cm, or any heterogeneous/enhancing lesion, should be referred to a sarcoma unit BEFORE biopsy or excision.
Overview
Soft tissue MRI interpretation rests on a single foundational principle: knowing what normal looks like on each sequence, so that any deviation can be recognised as pathology. The musculoskeletal soft tissues — muscle, tendon, ligament, nerve, fat and the fibrous capsular structures — each have a characteristic, predictable signal that reflects their water and collagen content. MRI is the dominant modality for these structures because of its unmatched soft tissue contrast, multiplanar capability and absence of ionising radiation.
Three questions answer most soft tissue MRI problems. First, is the lesion fluid, fat, fibrous tissue or something more complex (the four basic signal "building blocks")? Second, where does it sit relative to the deep fascia, and how large is it (the two strongest red flags for a sarcoma)? Third, is an apparent abnormality real, or an artefact such as the magic angle phenomenon that mimics tendon degeneration on short-echo sequences?
This topic builds the interpretation in layers: normal signal, a systematic reporting framework, then the four major pathological domains — tendon, muscle, soft tissue masses, and structure-specific assessment (rotator cuff, Achilles, meniscus). Throughout, the emphasis is on the findings that change management: the gap and retraction that determine reparability of a tendon, the Goutallier grade that predicts rotator cuff repair failure, and the depth/size combination that mandates referral to a sarcoma unit before any biopsy.
Fat, Blood, Protein, Melanin, ContrastWhat Is Bright on T1?
Hook:Most soft tissue pathology is LOW on T1; intrinsic high T1 signal narrows the differential sharply — fat suppression confirms fat, while a haematoma evolves over serial scans.
Normal Soft Tissue Signal
- T1 Signal
- Intermediate
- T2 Signal
- Intermediate to low
- Notes
- Pennate architecture visible
- T1 Signal
- Low (dark)
- T2 Signal
- Low (dark)
- Notes
- Organised collagen fibres
- T1 Signal
- Low (dark)
- T2 Signal
- Low (dark)
- Notes
- Similar to tendon
- T1 Signal
- High
- T2 Signal
- Intermediate to high
- Notes
- Suppresses on STIR/fat-sat
- T1 Signal
- Intermediate
- T2 Signal
- Intermediate to slightly high
- Notes
- Fascicular pattern visible
- T1 Signal
- Signal void
- T2 Signal
- Signal void
- Notes
- Flow-related signal loss
- T1 Signal
- Intermediate
- T2 Signal
- Intermediate
- Notes
- Articular surface assessment
Tendon Pathology
- MRI Finding
- Enlarged cross-sectional area
- Significance
- Chronic overload response
- MRI Finding
- Increased T1/T2 signal (not fluid bright)
- Significance
- Mucoid degeneration, disorganised collagen
- MRI Finding
- Fluid around tendon
- Significance
- Tenosynovitis or paratendinitis
- MRI Finding
- Signal void within tendon
- Significance
- Calcific tendinopathy
55° = False SignalMagic Angle Artefact
Hook:If increased tendon signal seen only on short TE sequences (T1/PD) but not on T2, suspect magic angle artefact
Muscle Pathology
- MRI Features
- Feathery oedema, no disruption
- Clinical Correlation
- Mild pain, minimal function loss
- MRI Features
- Partial fibre disruption, haematoma
- Clinical Correlation
- Moderate pain, weakness
- MRI Features
- Complete disruption, retraction, large haematoma
- Clinical Correlation
- Severe, may need surgery
Soft Tissue Masses
- Benign Indicators
- Less than 5cm
- Malignant Indicators
- Greater than 5cm
- Benign Indicators
- Superficial to fascia
- Malignant Indicators
- Deep to fascia
- Benign Indicators
- Well-defined, smooth
- Malignant Indicators
- Irregular, infiltrative
- Benign Indicators
- Homogeneous
- Malignant Indicators
- Heterogeneous
- Benign Indicators
- Uniform
- Malignant Indicators
- Necrosis, haemorrhage
- Benign Indicators
- None or uniform
- Malignant Indicators
- Peripheral, irregular
- Benign Indicators
- Stable
- Malignant Indicators
- Rapid enlargement
- T1 Signal
- High (fat)
- T2 Signal
- High (fat)
- Key Feature
- Follows fat on all sequences, thin septae OK
- T1 Signal
- Low
- T2 Signal
- Very high (fluid)
- Key Feature
- Well-defined, connects to joint
- T1 Signal
- Intermediate
- T2 Signal
- Very high
- Key Feature
- Serpiginous vessels, may have phleboliths
- T1 Signal
- Low to intermediate
- T2 Signal
- High
- Key Feature
- Target sign, fusiform, along nerve
- T1 Signal
- Low
- T2 Signal
- Very high
- Key Feature
- Intramuscular, well-defined, fluid-like signal
A subacute haematoma is a classic tumour mimic - it can be intrinsically bright on T1 (methaemoglobin) and may have an enhancing wall, so knowing how blood signal evolves over time is essential before calling such a lesion a tumour. The signal changes predictably with the oxidation state of haemoglobin:
- Haemoglobin form
- Oxyhaemoglobin (intracellular)
- T1 signal
- Iso/low
- T2 signal
- High
- Haemoglobin form
- Deoxyhaemoglobin (intracellular)
- T1 signal
- Iso/low
- T2 signal
- Low
- Haemoglobin form
- Methaemoglobin (intracellular)
- T1 signal
- High
- T2 signal
- Low
- Haemoglobin form
- Methaemoglobin (extracellular)
- T1 signal
- High
- T2 signal
- High
- Haemoglobin form
- Haemosiderin (rim)
- T1 signal
- Low rim
- T2 signal
- Low rim (blooms on gradient echo)
The discriminators between a resolving haematoma and a haemorrhagic tumour are: a haematoma should evolve and shrink on serial MRI, has no nodular internal enhancement (only a thin rim), and usually a fitting history of trauma/anticoagulation. Any solid enhancing nodule, lack of evolution, or growth means treat it as a tumour and refer - some sarcomas present with intratumoural haemorrhage that masquerades as a simple haematoma.
Functional Sequences: Diffusion-Weighted and Dynamic Contrast MRI
Beyond the conventional sequences, two functional techniques increasingly support soft-tissue mass characterisation, biopsy targeting and treatment-response assessment - and examiners now expect awareness of both.
- What it measures
- Restriction of water (Brownian) motion - a surrogate for cellularity
- Typical pattern and caveat
- Highly cellular tumours tend to restrict (low ADC), but overlap is large: myxoid tumours have HIGH ADC and can shine through, while some benign lesions (cellular schwannoma, fibromatosis) restrict. Best for response assessment (ADC rises with necrosis) and detecting recurrence.
- What it measures
- Rate and pattern of gadolinium uptake over time (the time-intensity curve)
- Typical pattern and caveat
- Malignant lesions tend to enhance early and rapidly (steep wash-in, washout-type curve); benign lesions enhance more slowly. Most useful to TARGET biopsy to the most enhancing (viable) region and to separate viable tumour from necrosis or post-treatment change.
Treat DWI and DCE as adjuncts, not arbiters. Neither reliably separates benign from malignant on its own because of major overlap, so they supplement - they do not replace - conventional multiplanar MRI and sarcoma-MDT review. Their highest-value uses are directing the biopsy to viable tissue and monitoring treatment response (a rising ADC and falling enhancement suggest necrosis/response).
Specific Structures
- Assessment
- Partial vs full thickness
- Reporting
- Articular, bursal, or interstitial
- Assessment
- AP dimension on coronal
- Reporting
- Small less than 1cm, medium 1-3cm, large 3-5cm, massive greater than 5cm
- Assessment
- Distance from footprint
- Reporting
- Affects repair tension
- Assessment
- Tangent sign (supraspinatus)
- Reporting
- Muscle below scapular spine line
- Assessment
- Goutallier grade
- Reporting
- Affects repair outcome
Peripheral Nerve Sheath Tumours and MR Neurography
A mass arising from a peripheral nerve has a characteristic constellation of signs, and recognising it both makes the diagnosis and warns against an ill-judged biopsy through a functioning nerve.
- What it is
- A nerve runs into and out of the fusiform lesion
- Meaning
- The lesion is neurogenic and follows a nerve course
- What it is
- A thin rim of fat surrounding the lesion
- Meaning
- It sits within the fat-containing neurovascular bundle (intermuscular)
- What it is
- Central low T2 (fibrocollagenous) with peripheral high T2 (myxoid)
- Meaning
- Classic of a benign nerve sheath tumour, especially neurofibroma
- What it is
- Multiple small ring-like fascicles within the lesion
- Meaning
- Reflects the internal nerve-fascicle architecture
- What it is
- Tapered ends continuous with the nerve
- Meaning
- Confirms the lesion lies along the nerve
A schwannoma typically sits eccentric to the nerve (so it can sometimes be shelled out), whereas a neurofibroma is fusiform with the nerve passing through it (harder to separate). The major concern is the malignant peripheral nerve sheath tumour (MPNST): suspect it when a nerve lesion is large (over about 5 cm), rapidly enlarging, heterogeneous with necrosis, ill-defined, or has peritumoral oedema, especially in a patient with neurofibromatosis type 1. Imaging cannot always separate an atypical neurofibroma from an MPNST, so FDG-PET and image-guided biopsy planned with the sarcoma team are used.
The combination of an entering/exiting nerve, split-fat sign, target sign and fascicular sign identifies a benign nerve sheath tumour. Loss of the target sign plus rapid growth, large size and heterogeneity in an NF1 patient should raise the alarm for malignant transformation (MPNST) and prompt sarcoma referral rather than local excision.
Systematic Approach to the Soft Tissue MRI
A reproducible search pattern prevents the two classic errors: satisfaction of search (stopping after the obvious finding) and over-calling artefact as disease. The framework below works for any soft tissue study and maps directly onto how examiners expect a candidate to present a film.
- Action
- Confirm region, side, sequences and planes
- Key question
- Do I have fluid-sensitive AND anatomical sequences?
- Action
- Identify muscle, tendon, ligament, fat, nerve, vessel
- Key question
- Is each structure the expected signal and calibre?
- Action
- Trace each from origin to insertion
- Key question
- Continuity, thickness, intrasubstance signal?
- Action
- Assess bulk, oedema (T2) and fat (T1)
- Key question
- Oedema, fatty infiltration, or both?
- Action
- Characterise any focal lesion
- Key question
- Fluid, fat, fibrous or solid? Depth and size?
- Action
- Re-examine suspicious signal
- Key question
- Magic angle, partial volume, failed fat-sat?
- Action
- State the finding that changes management
- Key question
- Reparable tear? Red-flag mass? Benign and dischargeable?
Differential Diagnosis by MRI Pattern
Soft tissue lesions are best approached by their dominant MRI signal pattern rather than by clinical suspicion alone. The table below groups the common differentials by the pattern that first catches the eye, with the discriminating feature that separates them.
- Differentials
- Lipoma; atypical lipomatous tumour / well-differentiated liposarcoma
- Discriminating feature
- Thick septae (over 2mm), nodular non-fat areas, size over 10cm, deep location favour ALT/WD-liposarcoma
- Differentials
- Ganglion/cyst; myxoma; myxoid sarcoma
- Discriminating feature
- True cyst is non-enhancing and joint-related; myxoid tumours show internal/septal enhancement
- Differentials
- Strain; denervation oedema; myositis; early infection
- Discriminating feature
- Distribution: focal at musculotendinous junction (strain) vs whole nerve territory (denervation) vs symmetric proximal (myositis)
- Differentials
- Chronic fatty infiltration; intramuscular lipoma; subacute haematoma (methaemoglobin)
- Discriminating feature
- Fatty infiltration follows muscle architecture; haematoma is focal with a fluid level and evolves over time
- Differentials
- Tendon/ligament; fibroma; PVNS/GCT-TS (haemosiderin); calcification
- Discriminating feature
- Blooming on gradient echo suggests haemosiderin (PVNS); CT confirms calcification
- Differentials
- Haemangioma / vascular malformation
- Discriminating feature
- Flow voids, fat overgrowth and rounded phleboliths are characteristic and reassuring
The most dangerous trap is calling a deep, large or heterogeneous mass "benign" on signal alone. Even a lesion that follows fat can be a well-differentiated liposarcoma, and some sarcomas (myxoid, synovial) mimic a cyst. When the pattern and the red flags disagree, the red flags win — refer before biopsy.
Guidelines, Registries & Global Practice
Soft tissue MRI interpretation is broadly consistent worldwide because it rests on physics-based signal characteristics, but referral pathways, access and protocol emphasis vary by health system and resource setting.
- Region
- UK
- Key recommendation
- Refer any unexplained lump deep to fascia, fixed, or larger than ~5cm urgently; MRI first-line; biopsy only within a sarcoma service
- Region
- Europe
- Key recommendation
- MRI for local staging of the whole compartment + chest CT for staging; planned biopsy by the sarcoma MDT before any excision
- Region
- US
- Key recommendation
- Image suspicious masses with MRI before any intervention; refer to an orthopaedic oncologist; avoid unplanned excision
- Region
- US
- Key recommendation
- MRI with and without contrast is the preferred study for a soft tissue mass of indeterminate nature
- Region
- Global
- Key recommendation
- MRI grading (e.g. BAMIC) to support return-to-play decisions in muscle injury, integrated with clinical assessment
Controversies & Areas of Uncertainty
Clinical Imaging
MRI is the workhorse for soft tissue assessment, but the protocol must be matched to the clinical question. A combination of fluid-sensitive and anatomical sequences in orthogonal planes is essential — a finding seen on only one plane or one sequence should always be scrutinised before it is called pathology.
- What it shows
- Anatomy, fat (bright), marrow
- Best for
- Fatty infiltration, fat in a mass, marrow assessment
- What it shows
- Fluid and oedema (bright), suppresses fat
- Best for
- Tendon tears, muscle oedema, cyst vs solid
- What it shows
- Robust fat suppression, oedema-sensitive
- Best for
- Marrow/muscle oedema, large field of view, off-isocentre
- What it shows
- Enhancing (vascular/solid) tissue
- Best for
- Solid vs cystic mass, abscess wall, tumour viability
- What it shows
- Susceptibility, cartilage
- Best for
- Calcification/haemosiderin (but prone to magic angle)
If an abnormality is visible on only one sequence or one plane, prove it before reporting it. Increased tendon signal on T1/PD but not on T2 is magic angle artefact, not a tear. A "lesion" seen on one slice only may be partial volume averaging or a normal structure (vessel, normal muscle slip).



Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old presents with chronic shoulder pain. MRI shows a full-thickness supraspinatus tear with the tendon stump retracted to the level of the glenoid. T1 sagittal shows high signal within the supraspinatus fossa.”
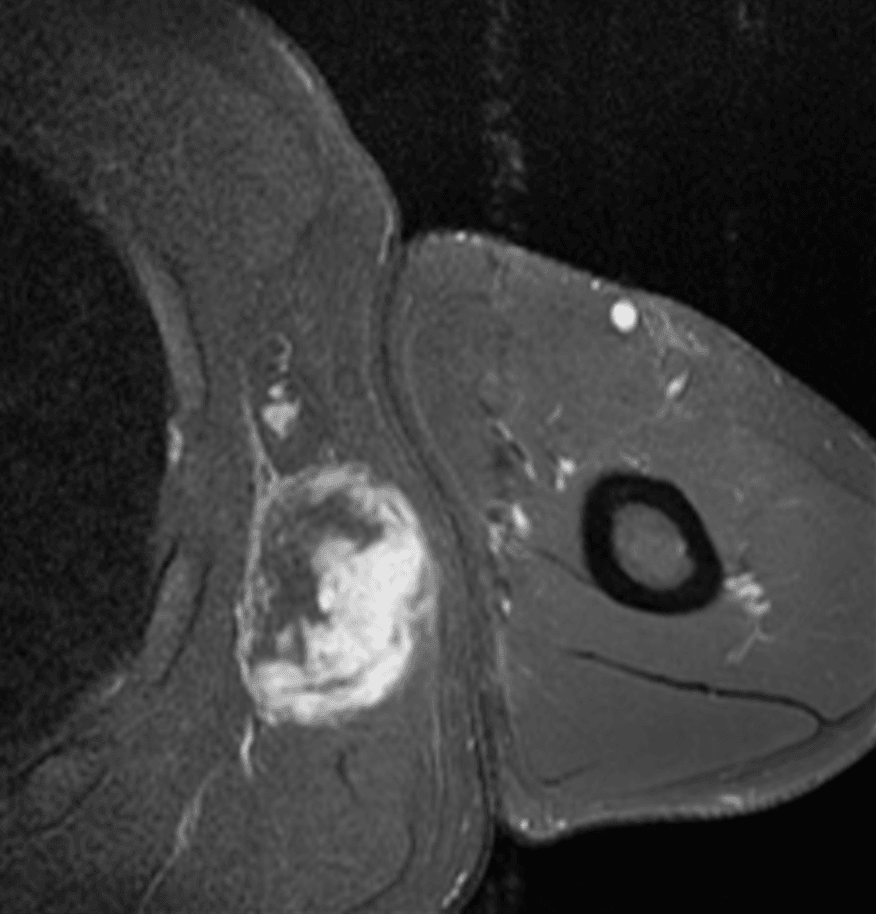
“A 45-year-old presents with a painless thigh mass that has slowly enlarged over 6 months. MRI shows a 12cm well-defined intramuscular mass that follows fat signal on all sequences but has thick internal septae measuring 3-4mm.”
“A 28-year-old runner presents with progressive calf pain. MRI shows diffuse high T2/STIR signal throughout the gastrocnemius and soleus muscles with no discrete mass. T1 signal is normal.”
Normal Signal
- Tendon/ligament: Dark on all sequences
- Muscle: Intermediate T1 and T2
- Fat: High T1, intermediate T2
- Nerve: Intermediate, fascicular pattern
Tendon Pathology
- Increased signal = degeneration or tear
- Magic angle at 55° (false signal on short TE)
- Full tear: discontinuity + fluid gap
- Measure gap and retraction for surgery
Muscle Assessment
- Oedema: High T2, normal T1
- Fatty infiltration: High T1 (Goutallier 0-4)
- Goutallier 3-4: Poor surgical outcome
- Denervation: Follows nerve territory
Soft Tissue Mass Red Flags
- Size greater than 5cm
- Deep to fascia
- Heterogeneous signal
- Rapid growth
- Irregular margins
Evidence Base
The interpretive frameworks used in soft tissue MRI are underpinned by classification and validation studies. According to PubMed, the following are the landmark and supporting references.
- Original five-stage (0-4) classification of rotator cuff muscle fatty degeneration on CT, derived from 63 patients undergoing cuff repair (57 re-evaluated at mean 17.7 months). Infraspinatus degeneration correlated with impaired active external rotation and had a strongly negative influence on the outcome of supraspinatus repairs; supraspinatus re-tear occurred in 25%. The authors concluded wide tears should be repaired before irreversible muscular damage occurs.
- Prospective comparison in 41 surgical shoulders. Interobserver reproducibility of fatty-degeneration grading was good-to-excellent for both CT and MRI, but the correlation between MRI and CT was only fair-to-moderate and remained unsatisfactory even when simplified to a 3-grade scale. The degree of fatty degeneration correlated significantly with muscle atrophy.
- Proposed an evidence-informed muscle injury grading system (BAMIC). Injuries are graded 0-4 on MRI features, with grades 1-4 carrying a suffix 'a' (myofascial), 'b' (musculotendinous) or 'c' (intratendinous) to capture the site of injury, which had been shown to influence prognosis. Designed to improve diagnostic accuracy and prognostication over the traditional three-grade system.
- Two radiologists classified 65 hamstring injuries in 45 elite athletes at two timepoints. Interrater agreement was substantial-to-almost perfect (kappa 0.80 then 0.88; 85-91% agreement) and intrarater agreement substantial (mean kappa 0.71). The system was judged straightforward and reproducible.