IMWG Criteria | MRI Patterns | Bone Disease | Orthopaedic Management
- IMWG 2014 criteria: 2 or more focal lesions on MRI (5mm+) = symptomatic myeloma
- Pure lytic lesions - myeloma NEVER produces blastic/sclerotic response
- Radiosensitive tumor - radiation highly effective for local control
- Pathological fracture risk - vertebroplasty/kyphoplasty effective for pain
- Spinal cord compression - emergency requiring urgent decompression
- “CRAB criteria: Calcium elevated, Renal insufficiency, Anemia, Bone lesions
- “MRI more sensitive than CT for detecting bone marrow infiltration
- “Whole-body low-dose CT has replaced skeletal survey
- “Myeloma is radiosensitive - responds well to radiation therapy
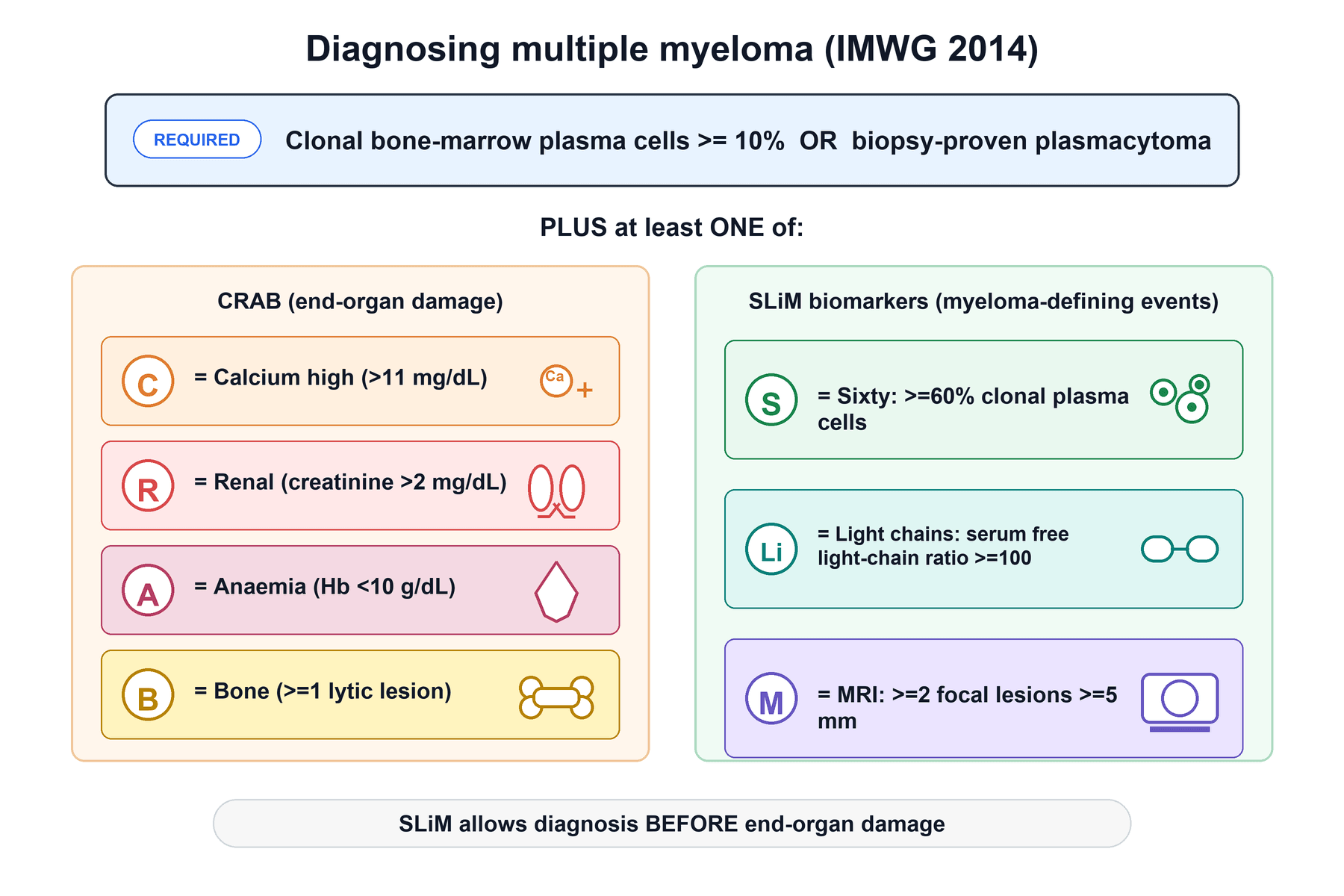
Symptomatic myeloma definition: C=Calcium elevated (over 11 mg/dL), R=Renal insufficiency (creatinine over 2), A=Anemia (Hb under 10), B=Bone lesions. Any one of these with clonal plasma cells = requires treatment.
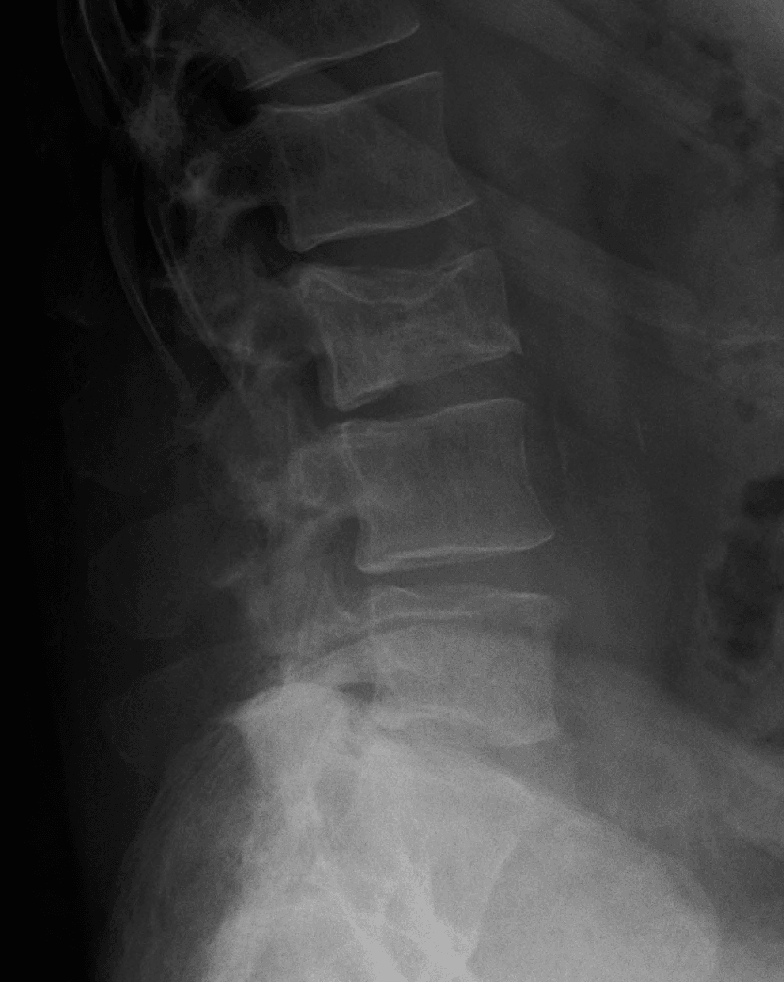
2014 IMWG criteria include MRI: 2 or more focal lesions (5mm or greater) on MRI OR one or more osteolytic lesions on CT = symptomatic myeloma. Single MRI lesion is NOT diagnostic but warrants investigation.
Myeloma produces ONLY lytic lesions - never blastic. If you see sclerotic response, consider POEMS syndrome (rare) or other diagnosis. The "punched out" lytic lesions are pathognomonic.
Myeloma is radiosensitive - unlike many solid tumor metastases. Radiation provides excellent local control. Surgery reserved for mechanical instability or decompression needs.
- Multiple Myeloma
- PURE LYTIC only
- Metastatic Carcinoma
- Lytic, blastic, or mixed
- Multiple Myeloma
- Bone marrow (plasma cells)
- Metastatic Carcinoma
- Breast, prostate, lung, kidney, thyroid
- Multiple Myeloma
- Often NEGATIVE (no osteoblastic)
- Metastatic Carcinoma
- Usually positive
- Multiple Myeloma
- Very high (marrow infiltration)
- Metastatic Carcinoma
- High for lytic lesions
- Multiple Myeloma
- Highly radiosensitive
- Metastatic Carcinoma
- Variable by histology
- Multiple Myeloma
- M-protein, free light chains
- Metastatic Carcinoma
- Tumor markers (PSA, CEA, etc)
Overview and Epidemiology
Multiple myeloma is a plasma cell neoplasm characterized by clonal proliferation of malignant plasma cells in the bone marrow, monoclonal protein in blood/urine, and end-organ damage including bone disease.
Epidemiology:
- Second most common hematologic malignancy (after NHL)
- Approximately 10% of all hematologic cancers
- Median age at diagnosis: 65-70 years
- Male to female ratio: 1.4:1
- Higher incidence in African Americans (2-3x)
Bone Disease Distribution:
- Frequency
- 49%
- Clinical Significance
- Most common - compression fractures
- Frequency
- 35%
- Clinical Significance
- "Pepper pot" appearance
- Frequency
- 34%
- Clinical Significance
- May cause pathological fractures
- Frequency
- 33%
- Clinical Significance
- Pain, fracture risk
- Frequency
- 20%
- Clinical Significance
- Impending fracture concern
Pathogenesis of Bone Disease:
Myeloma cells activate osteoclasts and suppress osteoblasts through:
- RANKL upregulation
- DKK1 (Dickkopf-1) inhibits Wnt signaling
- MIP-1alpha (macrophage inflammatory protein)
- IL-6, IL-1beta, TNF-alpha secretion
Myeloma causes ONLY lytic lesions because it suppresses osteoblast activity through DKK1. Without osteoblastic response, bone scans are often negative (no radioisotope uptake). This is why MRI and CT are preferred over bone scan for myeloma.
Pathophysiology
Disease Spectrum
Monoclonal Gammopathy of Undetermined Significance
Precursor condition with low risk of progression:
- M-protein under 3 g/dL
- Clonal plasma cells under 10% in marrow
- No CRAB features or myeloma-defining events
- 1% per year progression to myeloma
- No treatment required - observation only
MRI typically normal or minimal abnormality in MGUS.
Bone Marrow Infiltration
The pattern of bone marrow infiltration on MRI correlates with prognosis:
- Description
- No signal abnormality
- Prognosis
- Best
- Treatment Response
- N/A (MGUS/early)
- Description
- Discrete lesions, normal background
- Prognosis
- Good
- Treatment Response
- Generally favorable
- Description
- Homogeneous marrow replacement
- Prognosis
- Worst
- Treatment Response
- Higher tumor burden
- Description
- Focal + diffuse changes
- Prognosis
- Intermediate
- Treatment Response
- Variable
- Description
- Salt-and-pepper heterogeneous
- Prognosis
- Variable
- Treatment Response
- Depends on extent
Diffuse bone marrow infiltration on MRI indicates high tumor burden and correlates with worse prognosis and higher ISS stage. These patients often have more severe cytopenias and higher beta-2 microglobulin levels.
Classification and Staging
International Staging System (ISS)
- Criteria
- Beta-2 microglobulin under 3.5 mg/L AND Albumin 3.5 g/dL or more
- Median Survival
- 62 months
- Criteria
- Neither I nor III
- Median Survival
- 44 months
- Criteria
- Beta-2 microglobulin 5.5 mg/L or more
- Median Survival
- 29 months
ISS is based on two readily available serum markers. Beta-2 microglobulin reflects tumor burden while albumin reflects performance status.
A single focal lesion on MRI does NOT meet IMWG criteria for myeloma diagnosis. However, it should prompt further investigation with CT (one lytic lesion on CT IS diagnostic) or biopsy.
POEMS Syndrome (Osteosclerotic Myeloma)
The exam warning above flags that a sclerotic - rather than lytic - plasma-cell bone lesion should prompt thought of POEMS syndrome. POEMS (Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal protein, Skin changes), also called osteosclerotic myeloma or Crow-Fukase syndrome, is a rare paraneoplastic syndrome driven by an underlying plasma-cell disorder, and it is the classic exception to the "myeloma is always lytic" rule.
- POEMS Syndrome
- OSTEOSCLEROTIC or mixed sclerotic-lytic
- Multiple Myeloma
- Pure lytic ('punched out'), never blastic
- POEMS Syndrome
- Chronic progressive peripheral polyneuropathy
- Multiple Myeloma
- Bone pain and CRAB end-organ damage
- POEMS Syndrome
- Almost always lambda-restricted
- Multiple Myeloma
- Kappa or lambda
- POEMS Syndrome
- Usually low (often under 10%)
- Multiple Myeloma
- 10% or more, or biopsy-proven plasmacytoma
- POEMS Syndrome
- Elevated VEGF
- Multiple Myeloma
- M-protein, serum free light chains, beta-2 microglobulin
- POEMS Syndrome
- Organomegaly, endocrinopathy, skin changes, Castleman disease
- Multiple Myeloma
- Hypercalcaemia, renal failure, anaemia
When the bone lesions are SCLEROTIC, think POEMS rather than myeloma. Diagnosis requires the two mandatory criteria - a peripheral neuropathy plus a monoclonal plasma-cell disorder - together with at least one major criterion (osteosclerotic bone lesions, Castleman disease, or an elevated VEGF). A solitary or limited osteosclerotic lesion is treated with radiotherapy, whereas disseminated disease needs systemic anti-plasma-cell therapy. The neuropathy, not the bone disease, usually dominates the clinical picture.
Clinical Presentation
Presenting Features
- Most common symptom
- Often back pain from vertebral involvement
- Worse with movement, may improve at rest
- Pathological fractures common
- Fatigue (anemia)
- Weight loss
- Recurrent infections (immunoparesis)
- Hyperviscosity symptoms (rare)
Spinal Manifestations
- Present in 55-70% at diagnosis
- May be presenting feature
- Multiple levels common
- Thoracolumbar junction most common
- Emergency presentation
- From vertebral collapse or extraosseous extension
- Requires urgent assessment and treatment
- Good prognosis if treated promptly (radiosensitive)
- Neural foraminal narrowing
- Extraosseous tumor extension
- May present before diagnosis
Red Flags
- Age over 50 with new back pain
- Pathological fracture (minimal trauma)
- Anemia, renal insufficiency
- Hypercalcemia
- Elevated ESR/plasma viscosity
- Recurrent infections
Differential Diagnosis of a Lytic/Destructive Vertebral Lesion
- Discriminating features
- Pure lytic, often bone scan negative, M-protein, CRAB
- Key investigation
- SPEP/UPEP, serum free light chains, marrow biopsy
- Discriminating features
- Lytic, blastic or mixed; bone scan usually positive; known primary
- Key investigation
- CT chest/abdo/pelvis, tumour markers, biopsy
- Discriminating features
- Single lesion, less than 10% marrow plasma cells, no CRAB
- Key investigation
- Whole-body MRI/PET, marrow biopsy
- Discriminating features
- Permeative pattern, large soft-tissue mass relative to bone destruction
- Key investigation
- Biopsy with immunohistochemistry
- Discriminating features
- No marrow replacement on MRI, benign fluid sign, retropulsion uncommon
- Key investigation
- MRI (fat-suppressed), DEXA
- Discriminating features
- Disc involvement and endplate destruction, raised CRP, systemic sepsis
- Key investigation
- MRI with contrast, CT-guided biopsy and culture
A pivotal exam discriminator: myeloma and metastasis characteristically spare the intervertebral disc, whereas infection crosses the disc space and destroys adjacent endplates. Marrow replacement on T1 MRI distinguishes a malignant collapse from a benign osteoporotic fracture.
Investigations
Laboratory Studies
- FBC (anemia, rouleaux formation)
- Renal function, electrolytes
- Calcium (hypercalcemia)
- Total protein, albumin (AG ratio)
- LDH, beta-2 microglobulin
- Serum protein electrophoresis (SPEP) - M-spike
- Urine protein electrophoresis (UPEP) - Bence-Jones protein
- Serum free light chains (kappa/lambda ratio)
- Immunofixation (identifies M-protein type)
- Aspirate and trephine biopsy
- Plasma cell percentage
- Cytogenetics/FISH for prognostic markers
Imaging
Whole-Body Low-Dose CT (WBLDCT)
Now preferred first-line imaging (replaced skeletal survey):
- Higher sensitivity than conventional skeletal survey for osteolytic disease (IMWG 2019 consensus)
- One lytic lesion (5mm or larger) on CT = diagnostic criterion
- Better detection of rib/pelvic lesions
- Can assess fracture risk
Findings:
- Punched-out lytic lesions
- NO sclerotic rim (unlike metastases)
- Pathological fractures
- Osteopenia
WBLDCT is first-line imaging for initial staging per IMWG.
Management

Systemic Treatment
First-Line Therapy (Haematology):
Orthopaedic surgeons should understand systemic treatment:
- Triplet therapy: VRd (Bortezomib, Lenalidomide, Dexamethasone)
- Quadruplet therapy: Adding daratumumab for fit patients
- Autologous stem cell transplant: For eligible patients under 70
Bone-Targeted Therapy:
- Bisphosphonates: Zoledronic acid monthly
- Denosumab: Alternative if renal impairment
- Reduces skeletal events by 40%
Orthopaedic Management
Conservative Measures
Most patients managed non-operatively:
- Analgesia (WHO ladder)
- Bracing for vertebral fractures
- Activity modification
- Physiotherapy
Vertebral Augmentation:
- Kyphoplasty/Vertebroplasty highly effective
- 80-90% pain relief
- Can be done under local anesthesia
- Multiple levels in single session
- Good option for pathological compression fractures
Vertebral augmentation is first-line for painful compression fractures.
Spinal Cord Compression
Oncological Emergency in Myeloma:
Unlike metastatic carcinoma, myeloma cord compression has excellent prognosis if treated promptly:
- Dexamethasone 10mg IV bolus then 4mg q6h
- MRI whole spine (skip lesions common)
- Assessment for surgery:
- If mechanically unstable = surgery + radiation
- If stable = radiation alone effective
- Radiation highly effective (radiosensitive)
- Ambulatory patients: 90%+ maintain ambulation
- Non-ambulatory: 50-70% recover ambulation (better than carcinoma)
Unlike metastatic carcinoma, myeloma is highly radiosensitive. If the spine is mechanically stable (SINS under 7), radiation alone is often sufficient for cord compression. Surgery is not automatically required as in radioresistant tumors.
Complications
Skeletal Complications
- Vertebral compression fractures (55-70%)
- Long bone fractures (less common)
- Rib fractures
- 5-10% of myeloma patients
- Usually from vertebral collapse
- Extraosseous extension less common
- Present in 25-30% at diagnosis
- From osteoclast activation
- Medical emergency if severe
Treatment-Related Complications
- Osteonecrosis of jaw (ONJ) - 1-10%
- Renal toxicity (especially zoledronic acid)
- Atypical femoral fractures (rare)
- Wound healing issues (immunosuppression)
- Hardware failure (poor bone quality)
- Infection risk (hypogammaglobulinemia)
Disease Progression
Extramedullary Disease:
- Occurs in 10-20% during disease course
- More aggressive biology
- Requires modified treatment approach
AL (Light-Chain) Amyloidosis
Amyloidosis is listed among the events that define active disease and trigger treatment, but it is worth developing because the orthopaedic surgeon may be the first to encounter it. AL (primary, light-chain) amyloidosis is a plasma-cell dyscrasia in which misfolded monoclonal immunoglobulin light chains form amyloid fibrils that deposit in tissues; it can occur alone or alongside multiple myeloma.
- Detail
- Misfolded monoclonal light chains (usually lambda) form beta-pleated-sheet amyloid fibrils depositing in organs
- Exam Relevance
- A plasma-cell dyscrasia; a minority of myeloma patients (around 10-15%) have concurrent AL
- Detail
- Cardiac (restrictive cardiomyopathy), renal (nephrotic-range proteinuria), hepatic, autonomic and peripheral neuropathy, GI
- Exam Relevance
- Cardiac involvement dominates prognosis
- Detail
- Bilateral carpal tunnel syndrome (often the presenting feature), 'shoulder pad sign', amyloid arthropathy, soft-tissue and periarticular deposits, macroglossia
- Exam Relevance
- The orthopaedic/hand surgeon may see it first
- Detail
- Tissue biopsy with Congo red stain showing apple-green birefringence under polarised light; abdominal fat-pad aspirate; fibril typing by mass spectrometry
- Exam Relevance
- Congo red plus apple-green birefringence is the classic answer
- Detail
- AL = light-chain amyloid in a plasma-cell dyscrasia; dialysis-related amyloid = beta-2 microglobulin in long-term dialysis
- Exam Relevance
- Different protein and different clinical setting
In a patient with a plasma-cell disorder, bilateral carpal tunnel syndrome, unexplained restrictive cardiomyopathy or nephrotic-range proteinuria, macroglossia or a 'shoulder pad sign' should raise AL amyloidosis. Confirm with a Congo red stain demonstrating apple-green birefringence under polarised light and type the fibril by mass spectrometry. Treatment targets the underlying clone (bortezomib- or daratumumab-based) to switch off light-chain production, plus organ-supportive care. Distinguish it from dialysis-related beta-2 microglobulin amyloid, which is a different protein in a different setting.
Guidelines, Registries & Global Practice
Global Epidemiology
Multiple myeloma accounts for roughly 1% of all cancers and about 10% of haematological malignancies, with an age-standardised incidence of approximately 2 per 100,000 worldwide and a marked rise in absolute case numbers driven by ageing populations. Incidence is two- to threefold higher in people of African ancestry than in white populations and lower in East Asian populations, a disparity that persists after adjustment for access to care. The spine is the most common site of skeletal involvement, so the orthopaedic and spinal surgeon is frequently the first clinician to encounter undiagnosed disease through a pathological vertebral fracture.
Major Guidelines, Side by Side
- Position
- SLiM-CRAB diagnostic criteria; WBLDCT first-line imaging, whole-body MRI most sensitive; bone-targeted agent for all patients on therapy
- Evidence basis
- Consensus statements (Rajkumar 2014; Hillengass 2019; Terpos 2021)
- Position
- Offer whole-body MRI first-line for suspected myeloma (CT if MRI unsuitable); zoledronic acid as preferred bone-protective agent; consider cement augmentation for non-responsive pain
- Evidence basis
- Guideline, GRADE-appraised
- Position
- Treat suspected MSCC as an emergency; MRI whole spine within 24 hours; definitive treatment within 24 hours of diagnosis
- Evidence basis
- Guideline / national standard
- Position
- R-ISS staging; triplet/quadruplet induction; bisphosphonate or denosumab for bone disease; radiotherapy for cord compression or uncontrolled pain
- Evidence basis
- Category 1-2A consensus
- Position
- SINS for instability assessment; separation surgery plus radiotherapy for radioresistant compression; myeloma usually radiosensitive so radiotherapy alone often sufficient if stable
- Evidence basis
- Expert consensus
A key cross-guideline point of agreement, and a frequent exam discriminator, is that myeloma is radiosensitive: unlike most solid-tumour metastatic spinal cord compression (where decompressive surgery before radiotherapy improves ambulation, per Patchell), a mechanically stable myeloma cord compression can often be treated with radiotherapy alone.
Registry and Real-World Evidence
Myeloma bone disease is tracked less by arthroplasty-style implant registries than by national cancer and trials networks. Examples include the SEER programme (US), the Haematological Malignancy Research Network (UK), and the Myeloma and Related Diseases Registry (MRDR), which includes Australian and New Zealand cohorts. These provide population-level survival and practice-pattern data, consistently showing improving median survival (now exceeding 5-6 years in transplant-eligible patients) following the introduction of proteasome inhibitors, immunomodulatory drugs and anti-CD38 antibodies, while also documenting persistent under-use of bone-protective therapy and variation in time-to-diagnosis.
Practice Variation
In high-resource settings whole-body MRI or PET/CT and quadruplet induction with autologous transplant are standard. In limited-resource settings skeletal survey and plain radiography remain in use, and access to novel agents, denosumab and timely radiotherapy is restricted, so vertebral augmentation and conventional fractionated radiotherapy carry proportionally greater importance. The orthopaedic priorities, structural stabilisation, pain control and preservation of neurological function, are universal even where systemic options differ.
MCQ Practice Points
Q: What is the SINS score and its role in myeloma spine management?
A: Spinal Instability Neoplastic Score (SINS): Evaluates tumor-related spinal instability. Components: Location, pain, bone quality, radiographic alignment, vertebral body collapse, posterolateral involvement. Score 0-6: Stable. 7-12: Potentially unstable (surgical consultation). 13-18: Unstable (surgical stabilization indicated).
Q: What are the indications for surgical intervention in spinal myeloma?
A: Neurological deficit from cord compression, spinal instability (SINS greater than 12), intractable pain unresponsive to radiation/chemotherapy, pathological fracture with deformity, need for tissue diagnosis when uncertain. Surgery typically combined with radiation and systemic chemotherapy. Goal is palliation and function preservation.
Q: What is the role of vertebroplasty/kyphoplasty in spinal myeloma?
A: Percutaneous cement augmentation provides pain relief and mechanical stability for compression fractures without cord compression. Can be performed under local anesthesia in frail patients. Contraindicated if: posterior wall breach with epidural extension, neurological deficit, coagulopathy. May be combined with radiation.
Q: Why do myeloma lesions not appear on bone scan?
A: Myeloma cells secrete osteoclast-activating factors (RANKL, IL-6) causing pure bone resorption while suppressing osteoblast activity (via DKK1). Bone scan relies on osteoblastic activity for tracer uptake. No osteoblast response = no bone scan uptake. Use skeletal survey, whole-body low-dose CT, or MRI for myeloma staging.
Q: What is the typical surgical approach for myeloma cord compression?
A: Posterior decompression and stabilization most common - allows access to most vertebral levels, provides immediate stability. Circumferential approach (anterior + posterior) for significant anterior compression or vertebral body destruction. Separation surgery concept: Decompression to create space, then radiation for tumor control.
At a Glance
Multiple myeloma is a plasma cell malignancy with 80% having bone disease at diagnosis, with the spine being the most common site (49%). It produces only pure lytic lesions (never blastic) - the classic "punched out" appearance. Symptomatic disease is defined by CRAB criteria (Calcium elevation, Renal insufficiency, Anaemia, Bone lesions). The 2014 IMWG criteria include imaging: ≥2 focal lesions (≥5mm) on MRI is diagnostic. Myeloma is highly radiosensitive, so radiation provides excellent local control. Surgery is reserved for mechanical instability (SINS score) or spinal cord decompression; vertebroplasty/kyphoplasty effectively manages painful vertebral lesions.
CRABCRAB Criteria for Symptomatic Myeloma
Hook:CRAB criteria define end-organ damage requiring treatment
IMWGSLiM Criteria - New IMWG Biomarkers
Hook:SLiM criteria added in 2014 - can diagnose myeloma WITHOUT CRAB symptoms
MRIMRI Infiltration Patterns
Hook:FDMVN patterns - Diffuse pattern has worst prognosis
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old man presents with 3 months of progressive thoracic back pain. Blood tests show Hb 9.5, creatinine 1.8, calcium 2.8 mmol/L. SPEP shows M-protein 45 g/L. MRI shows multiple T1-hypointense vertebral lesions.”
“A 72-year-old woman with known myeloma presents with 48-hour history of progressive leg weakness. Examination shows 3/5 bilateral LE power. MRI shows T8 vertebral collapse with Bilsky grade 2 epidural compression.”
“A 65-year-old woman with myeloma in remission presents with severe L1 and L3 compression fractures (50% and 40% collapse). SINS 7. She has severe mechanical pain limiting mobility.”
“A 55-year-old man presents with a single T12 lytic lesion. Biopsy confirms plasmacytoma. Bone marrow shows 5% plasma cells. SPEP shows small M-protein 8 g/L. No CRAB features. Whole-body imaging shows no other lesions.”
CRAB Criteria
- C: Calcium over 11 mg/dL
- R: Renal - Creatinine over 2 mg/dL
- A: Anemia - Hb under 10 g/dL
- B: Bone - 1 or more lytic lesions
- Any CRAB + clonal plasma cells = symptomatic myeloma
SLiM Biomarkers (IMWG 2014)
- S: Sixty percent or more plasma cells in marrow
- Li: Light chain ratio 100 or more
- M: MRI - 2 or more focal lesions (5mm+)
- Any SLiM = myeloma WITHOUT needing CRAB
Key Imaging Points
- WBLDCT replaced skeletal survey (first-line)
- MRI most sensitive for marrow infiltration
- 2 or more MRI lesions = diagnostic criterion
- Bone scan often NEGATIVE (no blastic response)
- Pure LYTIC - never blastic in myeloma
MRI Patterns
- Focal: Best prognosis, discrete lesions
- Diffuse: Worst prognosis, homogeneous replacement
- Mixed: Focal + diffuse
- Variegated: Salt-and-pepper heterogeneous
- Normal: MGUS or early disease
Treatment Pearls
- Myeloma is RADIOSENSITIVE - radiation very effective
- Vertebroplasty/kyphoplasty for painful fractures
- Surgery only if unstable (SINS 13+) or failed RT
- Cord compression: If stable = RT alone effective
- Bisphosphonates reduce skeletal events by 40%
vs Metastatic Carcinoma
- Myeloma: Pure lytic, radiosensitive, bone scan negative
- Carcinoma: May be blastic/mixed, variable sensitivity
- Myeloma cord compression: RT alone often sufficient
- Carcinoma cord compression: Usually needs surgery
Evidence Base
IMWG 2014 Updated Diagnostic Criteria (SLiM-CRAB)
- Added validated SLiM biomarkers to the existing CRAB definition
- 2 or more focal lesions on MRI (each 5mm+) = myeloma-defining event
- Clonal bone marrow plasma cells 60% or more = myeloma-defining
- Involved/uninvolved serum free light chain ratio 100 or more = myeloma-defining
Revised International Staging System (R-ISS)
- Pooled analysis of 4,445 newly diagnosed patients from 11 international trials
- Combines ISS with high-risk cytogenetics (del(17p), t(4;14), t(14;16)) and LDH
- 5-year overall survival: R-ISS I 82%, R-ISS II 62%, R-ISS III 40%
- 5-year progression-free survival: 55%, 36% and 24% respectively
IMWG Consensus on Imaging in Plasma Cell Disorders
- Low-dose whole-body CT has higher sensitivity than conventional skeletal survey for bone disease
- WBLDCT recommended as the standard first-line imaging for newly diagnosed disease
- Whole-body MRI is the most sensitive modality for marrow infiltration and cord compression
- PET/CT preferred for treatment response and minimal residual disease assessment
Vertebroplasty/Augmentation in Spinal Malignancy
- Systematic review of 30 studies and 987 patients with metastases or myeloma
- Pain reduction ranged from 47% to 87%, comparable with osteoporotic augmentation
- Serious procedure-related complication rate approximately 2%
- No correlation between pain reduction and cement volume
MRI Marrow Infiltration Pattern and Prognosis
- 228 newly diagnosed symptomatic patients (41% diffuse, 41% focal, 15% normal pattern)
- Diffuse MRI pattern associated with high-risk cytogenetics (50% vs 31%) and poorer survival
- Diffuse pattern + ISS-3 + high-risk cytogenetics defined a very poor group (median OS 21 months)
- Diffuse-pattern patients benefited more from novel agents than conventional chemotherapy
IMWG Bone Working Group: Bone Disease Management
- Bisphosphonates (zoledronic acid) or denosumab recommended for all patients requiring anti-myeloma therapy
- Denosumab preferred over zoledronic acid in renal impairment (not renally cleared)
- Low-dose radiotherapy (8 Gy single fraction up to 30 Gy) for uncontrolled pain, impending fracture or cord compression
- Vertebral augmentation recommended for symptomatic vertebral compression fractures; surgery for instability or neurological compromise
References
- Rajkumar SV, Dimopoulos MA, Palumbo A, et al. International Myeloma Working Group updated criteria for the diagnosis of multiple myeloma. Lancet Oncol. 2014;15(12):e538-48. PMID: 25439696. doi:10.1016/S1470-2045(14)70442-5
- Hillengass J, Usmani S, Rajkumar SV, et al. International Myeloma Working Group consensus recommendations on imaging in monoclonal plasma cell disorders. Lancet Oncol. 2019;20(6):e302-e312. PMID: 31162104. doi:10.1016/S1470-2045(19)30309-2
- Palumbo A, Avet-Loiseau H, Oliva S, et al. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. J Clin Oncol. 2015;33(26):2863-9. PMID: 26240224. doi:10.1200/JCO.2015.61.2267
- Moulopoulos LA, Dimopoulos MA, Kastritis E, et al. Diffuse pattern of bone marrow involvement on magnetic resonance imaging is associated with high risk cytogenetics and poor outcome in newly diagnosed, symptomatic patients with multiple myeloma. Am J Hematol. 2012;87(9):861-4. PMID: 22641455. doi:10.1002/ajh.23258
- Chew C, Craig L, Edwards R, et al. Safety and efficacy of percutaneous vertebroplasty in malignancy: a systematic review. Clin Radiol. 2010;66(1):63-72. PMID: 21147301. doi:10.1016/j.crad.2010.09.011
- Terpos E, Zamagni E, Lentzsch S, et al. Treatment of multiple myeloma-related bone disease: recommendations from the Bone Working Group of the International Myeloma Working Group. Lancet Oncol. 2021;22(3):e119-e130. PMID: 33545067. doi:10.1016/S1470-2045(20)30559-3