Granulomatous Disease - Joints, Muscle, Bone
- Sarcoidosis is a multisystem NON-CASEATING GRANULOMATOUS disease whose musculoskeletal manifestations are widely variable in presentation and treatment response; the key MSK forms are an acute or chronic ARTHROPATHY, a granulomatous MYOPATHY, OSSEOUS sarcoidosis, and the INDIRECT skeletal effects of the disease.
- The classic ACUTE arthropathy is part of LOFGREN SYNDROME - the triad of (typically bilateral) ankle ARTHRITIS/PERIARTHRITIS, ERYTHEMA NODOSUM and BILATERAL HILAR LYMPHADENOPATHY - which is usually SELF-LIMITING with a GOOD prognosis and is a high-yield exam association; a CHRONIC arthritis is less common but can be oligo/polyarticular and, uncommonly, deforming or destructive.
- Granulomatous MYOPATHY is common pathologically but most often CLINICALLY SILENT; it may also present acutely, as a chronic proximal myopathy mimicking polymyositis, or as a nodular form - MRI is sensitive and these lesions are frequently missed clinically, so MRI should be considered for unexplained musculoskeletal complaints in sarcoidosis.
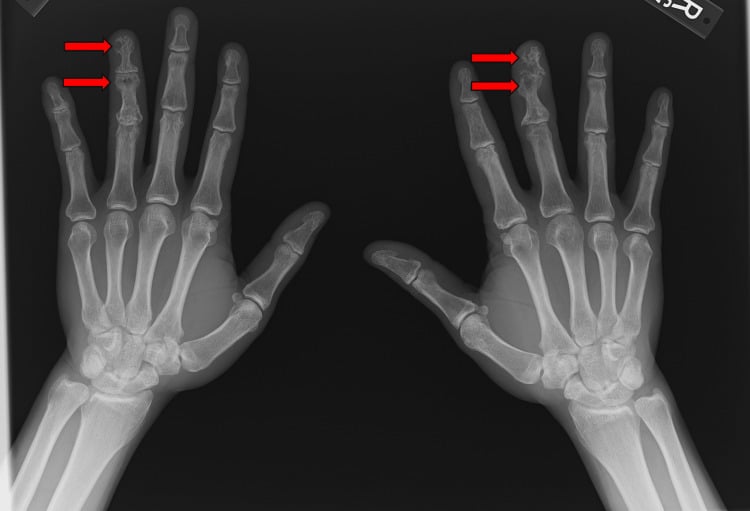
- OSSEOUS sarcoidosis classically produces LACE-LIKE (reticular) LYTIC/CYSTIC lesions in the PHALANGES of the hands and feet (often beneath cutaneous lesions and frequently asymptomatic), and can also affect the axial skeleton and large bones - the radiographic appearance is characteristic but the differential of lytic phalangeal lesions must be considered.
- INDIRECT skeletal effects are clinically important: activated macrophages in granulomas produce CALCITRIOL (1,25-dihydroxyvitamin D), causing HYPERCALCAEMIA and HYPERCALCIURIA (with nephrolithiasis/nephrocalcinosis), and patients are at increased risk of OSTEOPOROSIS and FRACTURES - so caution with vitamin D supplementation and attention to bone health are needed.
- MANAGEMENT of musculoskeletal sarcoidosis is generally part of treating the SYSTEMIC disease: the acute Lofgren arthropathy is usually managed symptomatically (NSAIDs, sometimes colchicine/short steroid course) and resolves, whereas chronic arthritis/myopathy and significant systemic disease are treated with CORTICOSTEROIDS and steroid-sparing agents (methotrexate; anti-TNF biologics in refractory cases) - and MRI should be used to evaluate unexplained osteoarticular complaints when standard radiographs are negative.
- DO NOT EXTEND LOFGREN'S GOOD PROGNOSIS TO SARCOIDOSIS AS A WHOLE. In 640 patients followed a mean of 112 months, 42.6% remitted spontaneously and 10.4% under treatment, but 28.1% became CHRONIC (8.5% with moderate-to-severe organ damage) and 18.9% were still active at closure; 43.4% needed corticosteroids. Just over half resolve.
- KNOW THE PROGNOSTIC FACTORS. Age over 40, pulmonary involvement on chest radiograph, splenic involvement and needing treatment predicted a CHRONIC course; LOFGREN SYNDROME and mediastinal lymphadenopathy predicted a GOOD outcome. In a second cohort Lofgren carried an adjusted odds ratio of 0.15 for chronicity, against 2.68 for extrapulmonary involvement.
- LOFGREN CAN RECUR LATE. Recurrence after complete remission is described up to more than 17 years later, usually again as Lofgren syndrome and usually with a good outcome - so arrange long-term follow-up rather than discharging, while recognising the evidence is a 17-patient series that gives no recurrence rate.
- “Sarcoid = non-caseating granulomatous multisystem disease. ACUTE arthropathy = LOFGREN syndrome (ankle periarthritis + erythema nodosum + bilateral hilar lymphadenopathy) - self-limiting, GOOD prognosis.
- “Osseous sarcoid = LACE-LIKE lytic/cystic phalangeal lesions (hands/feet, often asymptomatic). Granulomatous myopathy is usually clinically SILENT - MRI is sensitive.
- “Indirect effects: macrophage calcitriol -> HYPERCALCAEMIA/hypercalciuria (stones), osteoporosis, fracture risk (be cautious with vitamin D). Treat the systemic disease (steroids +/- methotrexate/anti-TNF).
- “OUTCOMES (n = 640, mean 112 months): 42.6% spontaneous remission + 10.4% on treatment, but 28.1% CHRONIC (8.5% severe organ damage); 43.4% needed steroids. Chronic predicted by age over 40, pulmonary involvement, splenic involvement, needing treatment; Lofgren protective (adjusted OR 0.15).
Bilateral ankle periarthritis + erythema nodosum + bilateral hilar lymphadenopathy = Lofgren syndrome - usually self-limiting (NSAIDs, sometimes a short steroid course), and the strongest protective factor against chronicity (adjusted OR 0.15). But sarcoidosis overall is less benign: 28.1% become chronic.
Lace-like lytic phalangeal lesions (osseous sarcoid, often asymptomatic); granulomatous myopathy is usually clinically silent - MRI is sensitive. Watch hypercalcaemia/osteoporosis.
The Musculoskeletal Manifestations
Sarcoidosis is a multisystem non-caseating granulomatous disease. Its MSK forms are: an acute arthropathy - classically bilateral ankle periarthritis as part of Lofgren syndrome (with erythema nodosum and bilateral hilar lymphadenopathy), usually self-limiting with a good prognosis - and a less common chronic arthritis that can be deforming; a granulomatous myopathy that is usually clinically silent (MRI sensitive); osseous sarcoidosis with characteristic lace-like lytic phalangeal lesions (often asymptomatic); and indirect effects - granuloma-derived calcitriol causing hypercalcaemia/hypercalciuria and an increased risk of osteoporosis and fractures.
Imaging, Differential & Management
- Imaging: radiographs for the lace-like phalangeal lesions; MRI is sensitive for the often-silent articular and muscular lesions and should be used for unexplained osteoarticular complaints when radiographs are negative.
- Differential: lytic phalangeal lesions (enchondroma, infection, metastasis); chronic arthritis (RA, spondyloarthropathy); myopathy (polymyositis); always correlate with the systemic picture and biopsy where needed.
- Acute (Lofgren): symptomatic - NSAIDs, sometimes colchicine or a short steroid course - usually resolves.
- Chronic arthritis/myopathy and systemic disease: corticosteroids and steroid-sparing agents (methotrexate; anti-TNF biologics in refractory disease).
- Bone health: treat hypercalcaemia, be cautious with vitamin D, and address osteoporosis/fracture risk.
Two balanced judgements define musculoskeletal sarcoidosis. On the one hand, the acute arthropathy of Lofgren syndrome - bilateral ankle periarthritis with erythema nodosum and bilateral hilar lymphadenopathy - has a good prognosis and is usually self-limiting, so it should generally be managed symptomatically rather than committed to prolonged immunosuppression. On the other hand, much MSK sarcoid is occult: granulomatous myopathy is frequently clinically silent, osseous lesions (the classic lace-like phalangeal lytic lesions) are often asymptomatic, and the chronic articular disease can be subtle - so MRI should be used to evaluate unexplained osteoarticular complaints when radiographs are negative. Finally, the indirect skeletal effects matter: granuloma-derived calcitriol can cause hypercalcaemia and hypercalciuria with stones, and patients are at increased risk of osteoporosis and fracture, so vitamin D supplementation must be used cautiously and bone health attended to. MSK sarcoid is managed as part of the systemic disease, with the rheumatology/respiratory team.
Osseous Sarcoidosis: The Jüngling Pattern and Its Differential
- The eponym and patterns. The lace-like/reticular phalangeal osseous sarcoid is osteitis multiplex cystoides of Jüngling (Perthes-Jüngling). Radiographic patterns are: a lace-like/reticular trabecular resorption (middle/distal phalanges, often with an intact cortex), cystic/"punched-out" lucencies, a permeative/destructive form (± acro-osteolysis, pathological fracture), and rarely a sclerotic form in the axial skeleton (which can mimic metastases). It often underlies lupus pernio skin and dactylitis; MRI/PET detect marrow lesions that radiographs miss.
- The phalangeal-lytic differential. A lytic phalangeal lesion may be an enchondroma (commonest - chondroid, expansile), infection (TB dactylitis / "spina ventosa"), a gout tophus, a glomus tumour, an epidermoid inclusion cyst, a brown tumour of hyperparathyroidism, or a metastasis - correlate with the systemic sarcoid picture.
Q: What is the eponym and radiographic spectrum of osseous sarcoidosis, and its phalangeal-lytic differential?
A: The lace-like/reticular phalangeal osseous sarcoid = osteitis multiplex cystoides of Jüngling (Perthes-Jüngling). Patterns: lace-like/reticular trabecular resorption (middle/distal phalanges, intact cortex), cystic/"punched-out" lucencies, permeative/destructive (± acro-osteolysis/fracture), rarely sclerotic (axial, mimics metastases); often under lupus pernio; MRI/PET catch marrow lesions radiographs miss. Differential of a lytic phalangeal lesion: enchondroma (commonest), TB dactylitis (spina ventosa), gout tophus, glomus, epidermoid cyst, brown tumour, metastasis.
What Actually Happens: Outcomes in 640 Patients Over 40 Years
"Sarcoidosis often resolves spontaneously" is true but incomplete, and the incomplete version is the one that gets candidates into trouble. In a 640-patient cohort followed at a single Spanish tertiary centre from 1976 to 2015, with follow-up in 587 patients over a mean of 112 months:
- 42.6% had spontaneous remission and a further 10.4% remitted under treatment - so a little over half resolve.
- 28.1% evolved to CHRONIC sarcoidosis - 19.6% with mild disease but 8.5% with moderate-to-severe organ damage. Another 18.9% still had active disease when the study closed.
- 43.4% required corticosteroids and 7.7% needed steroid-sparing agents. "Usually self-limiting" describes Löfgren syndrome, not sarcoidosis as a whole.
What predicts a chronic course. On multivariate analysis, age over 40 at diagnosis, pulmonary involvement on chest radiograph, splenic involvement, and needing treatment were associated with chronic disease. Löfgren syndrome and mediastinal lymphadenopathy were indicators of a GOOD outcome - so the page's optimism about Löfgren is well founded, and it is specifically Löfgren, not acute presentation in general, that carries the favourable prognosis. A separate Portuguese study comparing 110 chronic with 129 resolved patients put a number on it: Löfgren syndrome had an adjusted odds ratio of 0.15 for progressing to chronicity, against 2.68 for extrapulmonary involvement and 1.06 per year of age.
Löfgren syndrome genuinely carries a good prognosis, but it can recur years after complete remission. In a series of 17 patients with 24 recurrences collected over 28 years, the disease-free interval between resolution and the first recurrence ranged from 10 months to more than 17 years, and most recurrences again presented as Löfgren syndrome. Outcomes remained good - 14 of the 17 were in complete remission at last review and only one became chronic - but the authors recommend long-term follow-up even in patients whose disease is inactive. Note the striking sex distribution: all but one of those 17 patients were women. With only 17 patients this is a description of a rare phenomenon, not a recurrence rate, and it cannot tell you how often relapse occurs.
How Sarcoidosis Is Diagnosed
- A diagnosis of exclusion. There is no single diagnostic test: sarcoidosis requires a compatible clinical/radiological picture, histological non-caseating epithelioid granulomas on biopsy, and exclusion of other granulomatous causes - above all mycobacterial (TB) and fungal infection (stains/cultures negative), and also berylliosis, granulomatous drug reactions and lymphoma. The granulomas contain epithelioid histiocytes and multinucleate giant cells (sometimes with asteroid and Schaumann bodies - non-specific).
- When biopsy can be omitted. Löfgren syndrome is so characteristic that it is often diagnosed clinically without biopsy - the main exception to the biopsy rule.
- Supporting tests. Serum angiotensin-converting enzyme (ACE) is often raised (from the granuloma epithelioid cells) but is non-specific and non-sensitive - better for monitoring activity than for diagnosis; also look for hypercalcaemia/hypercalciuria, lymphopenia, raised inflammatory markers, and the chest findings (bilateral hilar lymphadenopathy).
Q: How is sarcoidosis diagnosed, and what is the role of serum ACE?
A: It is a diagnosis of exclusion - a compatible clinical/radiological picture + biopsy showing non-caseating epithelioid granulomas + exclusion of other granulomatous causes, above all TB and fungal infection (stains/cultures negative). Löfgren syndrome is characteristic enough to be diagnosed clinically without biopsy. Serum ACE (from the granuloma epithelioid cells) is often raised but non-specific/non-sensitive - better for monitoring activity than diagnosis; also hypercalcaemia, lymphopenia, bilateral hilar lymphadenopathy.
Mnemonics & Memory Aids
GRAIN
Hook:GRAIN: Granulomatous, lofgRen arthropathy, Asymptomatic bone/silent myopathy, Indirect hypercalcaemia/osteoporosis, Need systemic treatment.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A patient has bilateral ankle swelling, painful red shin nodules and bilateral hilar lymphadenopathy on chest radiograph. What is this, and what is the prognosis?”
Arthropathy
- Acute = Lofgren syndrome (ankle periarthritis + erythema nodosum + bilateral hilar lymphadenopathy)
- Lofgren is usually self-limiting with a good prognosis (adjusted OR 0.15 for chronicity)
- But it can recur after complete remission, up to more than 17 years later - follow up long term
- Chronic arthritis less common; occasionally deforming/destructive
Outcomes (n = 640, mean 112 months)
- 42.6% spontaneous remission + 10.4% remission on treatment - just over half resolve
- 28.1% evolve to chronic sarcoidosis; 8.5% with moderate-to-severe organ damage
- 18.9% still active at study closure; 43.4% required corticosteroids
- Chronic predicted by: age over 40, pulmonary involvement on CXR, splenic involvement, needing treatment
- Good outcome predicted by: Lofgren syndrome and mediastinal lymphadenopathy
- Cohort was 95.8% Caucasian at one tertiary centre - do not transfer the proportions unchanged
Muscle & bone
- Granulomatous myopathy - usually clinically silent (MRI sensitive)
- Osseous: lace-like lytic/cystic phalangeal lesions (hands/feet, often asymptomatic)
- Axial/large-bone lesions also occur
Indirect effects
- Calcitriol from granulomas -> hypercalcaemia + hypercalciuria (stones)
- Osteoporosis and increased fracture risk
- Be cautious with vitamin D supplementation
Management
- Acute Lofgren: symptomatic (NSAIDs +/- colchicine/short steroid course)
- Chronic/systemic: corticosteroids + methotrexate (anti-TNF if refractory)
- MRI for unexplained osteoarticular complaints; treat as part of systemic disease
Evidence & Key Studies
Multidisciplinary approach and long-term follow-up in 640 consecutive patients with sarcoidosis: a 40-year cohort at a tertiary centre in Barcelona
- 640 consecutive patients diagnosed 1976-2015 on a prospective protocol; 68.4% female, mean age 43.3 (SD 13.8), 95.8% Caucasian. Follow-up achieved in 587 (91.7%) over a mean of 112.4 months (SD 98.3, range 6.4-475) - genuinely long-term, which most sarcoidosis series are not.
- OUTCOMES: spontaneous remission in 250 (42.6%), remission under treatment in 61 (10.4%), still active at study closure in 111 (18.9%), and evolution to CHRONIC sarcoidosis in 165 (28.1%) - of whom 115 (19.6%) had mild disease and 50 (8.5%) moderate-to-severe organ damage. Corticosteroids were needed by 43.4% and steroid-sparing agents by 7.7%.
- Predictors of chronic disease on multivariate analysis: age over 40 at diagnosis, pulmonary involvement on chest radiograph, splenic involvement, and the need for treatment. LOFGREN SYNDROME and mediastinal lymphadenopathy were indicators of GOOD outcome.
- Erythema nodosum was the commonest extrapulmonary manifestation at 39.8%, with specific cutaneous lesions in 20.8%; 91.2% had intrathoracic involvement on chest radiograph at diagnosis and most had normal pulmonary function.
- Limitations: single tertiary referral centre and 95.8% Caucasian, so the proportions do not transfer to populations where sarcoidosis is more severe - notably African-ancestry patients, in whom the disease is well recognised to run a worse course. Referral bias inflates severe phenotypes; the 'still active' group is censored by the study end rather than truly resolved.
Pulmonary sarcoidosis: prognostic factors at diagnosis in patients from the north of Portugal
- Compared 110 patients with a chronic course against 129 whose disease resolved, seeking prognostic factors identifiable at diagnosis.
- In the final logistic regression, LOFGREN SYNDROME was strongly protective against chronicity with an adjusted odds ratio of 0.15, while EXTRAPULMONARY INVOLVEMENT carried an adjusted odds ratio of 2.68 and each year of age 1.06.
- Chronic disease was also positively associated with lung function impairment, radiologic stage II, a lower lymphocyte CD4/CD8 ratio and extrapulmonary disease. Asthenia, like Lofgren syndrome, was protective.
- Limitations: retrospective, single region, and the groups were defined by outcome rather than followed from a common starting point - so these are associations available at diagnosis, not a validated prediction rule. No confidence intervals are given in the abstract for the odds ratios.
Recurrent sarcoidosis: a study of 17 patients with 24 episodes of recurrence
- A SMALL DESCRIPTIVE SERIES, not a frequency study: 17 patients with 24 recurrences identified over 28 years at one hospital. It shows that late recurrence happens; it cannot say how often.
- Recurrence was defined strictly - reappearance after complete resolution of clinical, radiographic and other activity markers, maintained at least 3 years without therapy. The disease-free interval before first recurrence ranged from 10 months to more than 17 years.
- All but one of the 17 patients were women. All but one presented as Lofgren syndrome at onset, and 17 of the recurrences were again Lofgren syndrome.
- Outcome remained good: at last review 14 were in complete remission, 2 had recent activity and only 1 developed chronic sarcoidosis - supporting the teaching that acute sarcoid arthropathy does well even when it relapses, but justifying long-term follow-up rather than discharge.
Musculoskeletal manifestations of sarcoidosis
- A NARRATIVE REVIEW, not a study - it summarises the field and supplies no cohort, denominator or outcome data of its own.
- Sarcoidosis can involve the joints (acute arthritis - mostly self-resolving - and, less commonly, chronic arthritis that may deform/destroy the joint), the muscles (categorised by clinical presentation), and the bones (with around half of patients with bone lesions remaining asymptomatic).
- Indirect skeletal effects include osteoporosis, increased fracture risk, hypercalcaemia and hypercalciuria, contributed to by elevated calcitriol.
- Sarcoidosis can also be associated with small-, medium- and large-vessel vasculitis, and distinguishing sarcoid vasculitis from coexisting pure vasculitis can be difficult.
Radiologic manifestations of musculoskeletal sarcoidosis
- A NARRATIVE REVIEW of imaging findings - its recommendations reflect expert synthesis rather than a measured diagnostic yield, and no sensitivity or specificity figure for MRI in musculoskeletal sarcoidosis is supplied.
- Articular manifestations of sarcoidosis are difficult to distinguish from other inflammatory and degenerative arthropathies, and muscular lesions are generally clinically silent and therefore often missed.
- MRI shows these manifestations to be very common in active sarcoidosis and should be included in screening when musculoskeletal sarcoidosis is suspected.
- MRI should be considered for evaluating patients with sarcoidosis who have unexplained osteoarticular complaints if standard radiographs are negative.
The outcome proportions (42.6% spontaneous remission, 10.4% remission on treatment, 18.9% active, 28.1% chronic with 8.5% moderate-to-severe organ damage), the 43.4% corticosteroid requirement, the erythema nodosum frequency of 39.8%, and the predictors of chronic versus good outcome come from Mana's 640-patient Barcelona cohort (DOI). The adjusted odds ratios - 0.15 for Lofgren syndrome, 2.68 for extrapulmonary involvement, 1.06 per year of age - come from Silva (DOI), 110 chronic versus 129 resolved patients. The late-recurrence observations come from Mana's 17-patient series (PMID 14620164), which reports no recurrence rate. The MSK spectrum and indirect skeletal effects come from the El Hasbani review (DOI) and the imaging role from Brandao Guimaraes (DOI) - both NARRATIVE REVIEWS rather than studies. The Lofgren triad, the Jungling osseous pattern, the calcitriol mechanism of hypercalcaemia, and the biopsy/exclusion approach to diagnosis are standard, well-established teaching.
What is not established: no diagnostic accuracy figure (sensitivity or specificity) has been published for MRI in musculoskeletal sarcoidosis, so "MRI is sensitive" is expert recommendation rather than measured performance; there is no validated prognostic score, no agreed surveillance interval after remission, and no trial defining when to treat sarcoid arthropathy. The prevalence of MSK involvement is quoted variably and no reliable single figure exists. Both outcome cohorts are European and predominantly Caucasian, and sarcoidosis is recognised to run a more severe course in patients of African ancestry, so these proportions should not be applied universally.