Hip Fracture Emergency | Garden Classification | Fix vs Replace
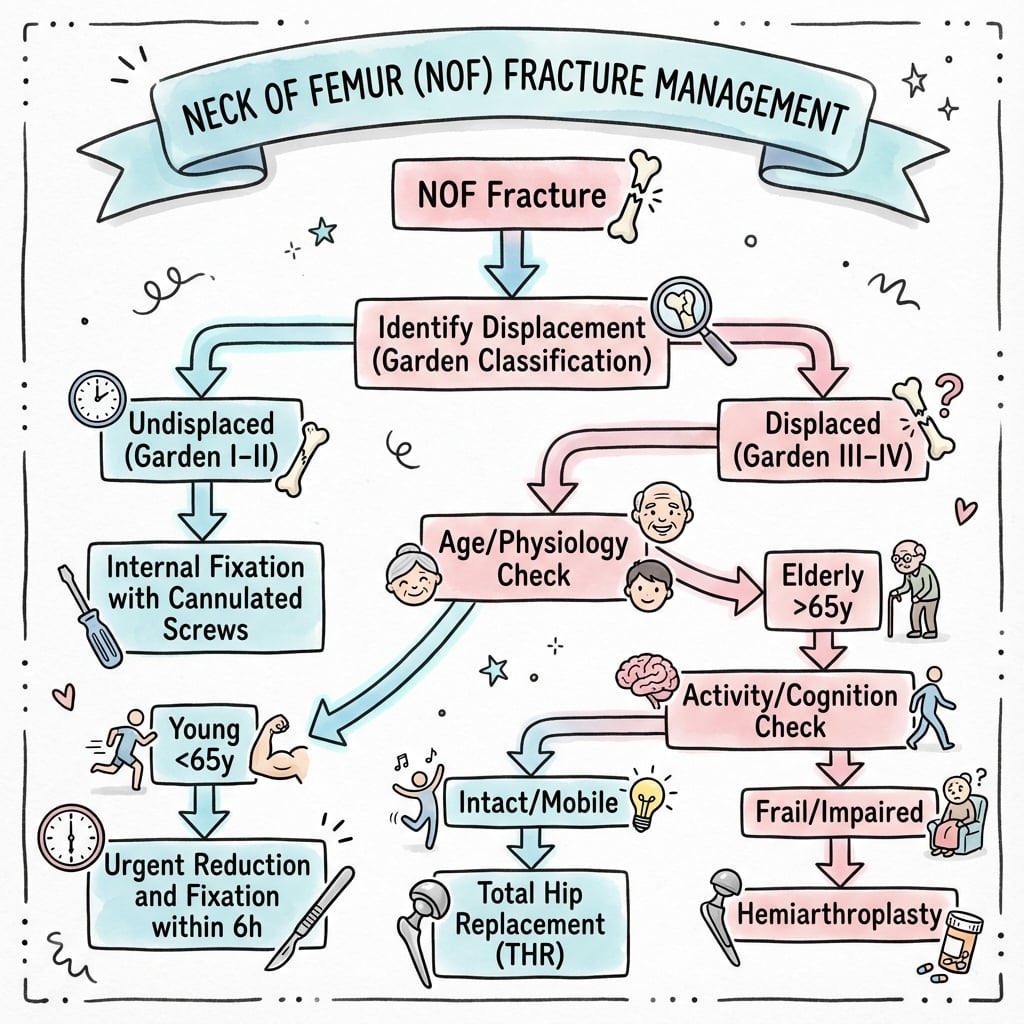
- Garden I/II = undisplaced (fix). Garden III/IV = displaced (replace in elderly)
- Intracapsular location = AVN risk (blood supply)
- Surgery within 48 hours improves outcomes
- Hemiarthroplasty vs THR: Depends on cognitive status, mobility, age
- Young patients with displaced fractures: attempt reduction and fixation
- “Blood supply: lateral epiphyseal vessels from MFCA
- “Displaced fractures in elderly: arthroplasty (hemi or THR)
- “Garden I may progress to displaced if not fixed
- “Cannulated screws in inverted triangle configuration


I/II = Undisplaced - screw fixation. III/IV = Displaced - arthroplasty in elderly (AVN risk too high). Simpler to remember: undisplaced = fix, displaced = replace.
Lateral epiphyseal vessels from medial femoral circumflex artery (MFCA) are main supply to femoral head. Displaced fractures disrupt these = AVN.
Surgery within 36-48 hours reduces mortality, pressure sores, complications. Delay increases mortality. This is a surgical emergency.
THR: Cognitively intact, independently mobile, expected survival greater than 4 years. Hemiarthroplasty: Cognitive impairment, limited mobility, frail elderly. THR has better function but higher dislocation risk.
Overview and Anatomy
Neck of femur (NOF) fractures are common in elderly with osteoporosis. They are a major cause of morbidity and mortality.
Anatomy
NOF fractures are intracapsular - within the hip joint capsule. This has two implications:
- Blood supply at risk: Lateral epiphyseal vessels (from MFCA) run along the neck and are disrupted by displacement → AVN.
- No periosteal healing: Intracapsular fractures rely on endosteal healing.
Blood Supply
Medial femoral circumflex artery (MFCA) gives rise to lateral epiphyseal vessels which are the main supply to the femoral head. Displaced fractures disrupt these.
The Calcar Femorale
The fixation and arthroplasty sections repeatedly invoke the calcar (the inferior "calcar screw", "loss of calcar continuity causing varus collapse", and "calcar-replacing stems"), so the structure itself is worth defining. The calcar femorale is a dense vertical plate of cortical bone arising from the posteromedial femoral shaft beneath the lesser trochanter and radiating upward and laterally into the femoral neck. It is not the same as the medial cortex (the visible medial "Adam's arch"): it is an internal weight-bearing buttress that reinforces the neck-shaft junction and transmits load from the neck to the shaft.
Why it matters clinically:
- Fixation: the inferior (calcar) screw or lag screw is placed along this dense buttress, where it gains the best purchase and provides the medial support that resists varus collapse. Loss of calcar/posteromedial continuity (comminution) removes this buttress and predicts fixation failure.
- Arthroplasty: when the medial calcar is deficient or resected too low, a standard stem can subside, which is why a calcar-replacing stem is used to restore medial support and leg length.
- Biomechanics: it lies in the path of the primary compressive trabeculae, completing the medial load-transfer column of the proximal femur.
The calcar femorale is the dense posteromedial bony strut of the proximal femur (distinct from the medial cortex). It is the key to medial support: the inferior fixation screw is aimed along it to resist varus collapse, its comminution predicts fixation failure, and its deficiency at arthroplasty is the indication for a calcar-replacing stem.
Pathophysiology
Mechanism of Injury
Neck of femur fractures occur through two main mechanisms:
- Low-energy falls in elderly osteoporotic patients (most common)
- High-energy trauma in younger patients (road traffic accidents, falls from height)
Blood Supply Disruption
The femoral head receives blood supply primarily from the medial femoral circumflex artery (MFCA), a branch of the profunda femoris. The MFCA gives rise to the lateral epiphyseal vessels which run along the posterior-superior aspect of the femoral neck within the capsule.
In displaced fractures, these vessels are disrupted, leading to:
- Avascular necrosis (AVN): 20-30% in young patients with displaced fractures
- Higher rates with delayed reduction (greater than 6 hours)
- Retrograde blood flow from ligamentum teres contributes minimally
Why Intracapsular Location Matters
- No periosteal sleeve: Intracapsular fractures lack periosteal contribution to healing
- Synovial fluid washout: Disrupts hematoma formation needed for healing
- Increased nonunion risk: 10-30% depending on fracture pattern
Capsular Tamponade: The Second Hit to the Blood Supply
Displacement tears the retinacular vessels directly, but there is a second, potentially modifiable vascular insult: an intracapsular fracture bleeds into a closed, non-distensible capsule, producing a tense haemarthrosis. The rising intracapsular pressure can exceed capillary perfusion pressure and tamponade the already-compromised retinacular vessels, adding a secondary ischaemic hit to the femoral head - the rationale offered for early decompression by capsulotomy or joint aspiration.
- Why it matters most in undisplaced (Garden I-II) fractures: here the retinacular vessels are often still intact, so a tense haemarthrosis is the main reversible threat to the head, and the theoretical case for decompression is strongest.
- The evidence: routine capsulotomy has not been shown to reduce AVN (the FAITH trial found no benefit), so it is not mandatory. Many surgeons still decompress in delayed presentations or aspirate/capsulotomise when fixing undisplaced fractures, accepting that the benefit is unproven.
The femoral head suffers two vascular insults: (1) mechanical disruption of the retinacular vessels by displacement (the dominant, irreversible hit in Garden III-IV), and (2) capsular tamponade from a tense intracapsular haemarthrosis raising the pressure around the surviving vessels (the potentially reversible hit, most relevant in undisplaced fractures). Capsular decompression targets the second hit, but the FAITH trial showed no clear AVN benefit, so it remains optional rather than standard.
Classification Systems
Neck of femur fractures can be classified by multiple systems, each providing different prognostic and treatment information.
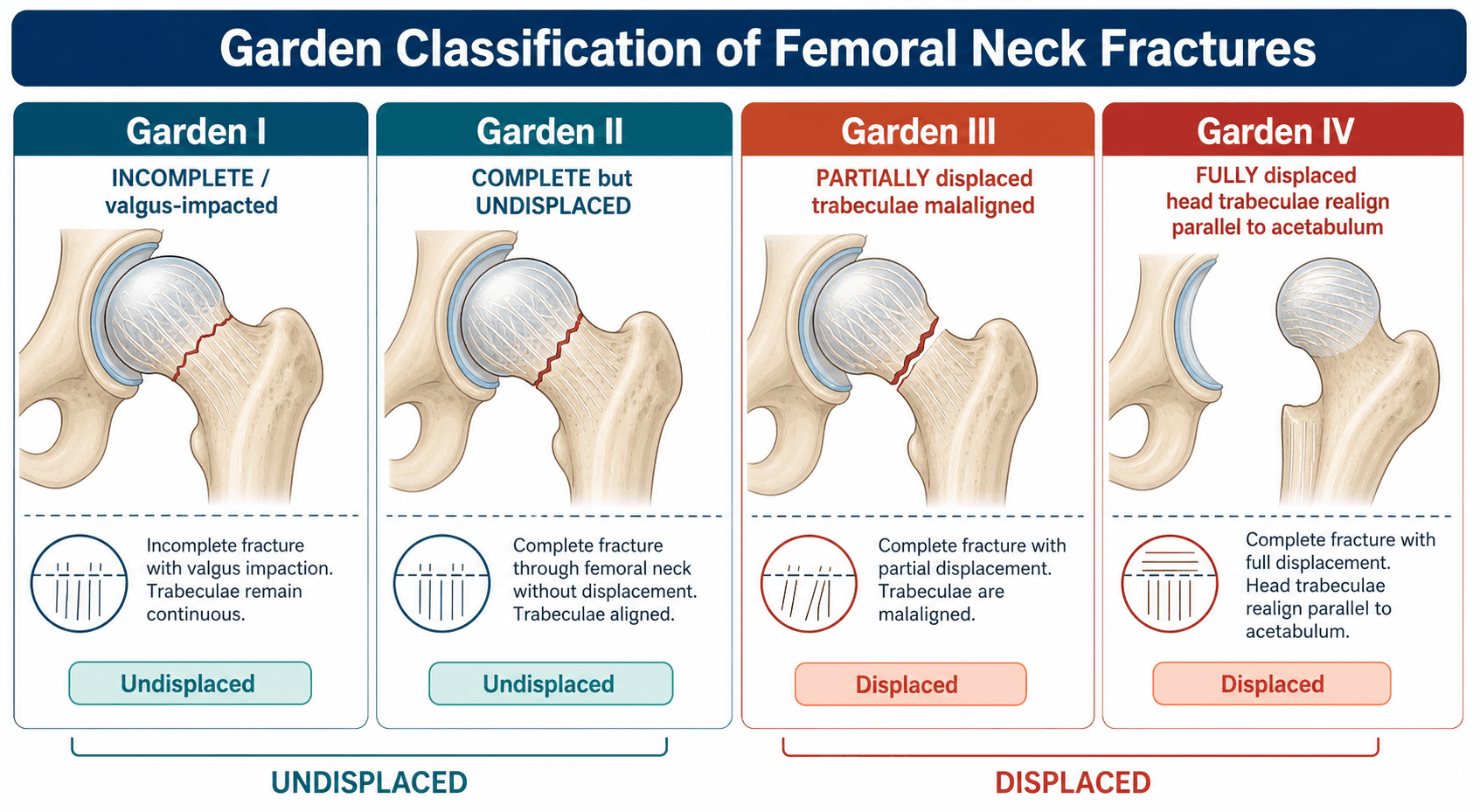
Garden Classification (1961)
Based on degree of displacement and alignment of trabecular lines on AP radiograph. Correlates with AVN risk and guides treatment.
Garden I - Incomplete/Impacted Valgus:
- Fracture line visible but incomplete
- Femoral head tilted into valgus (impacted position)
- Trabecular lines remain continuous across fracture
- AVN risk: 0-10%
- Treatment: Cannulated screw fixation
Garden II - Complete, Non-Displaced:
- Complete fracture line visible
- No displacement - trabecular lines of head align with acetabulum and neck
- Head remains in neutral position
- AVN risk: 10-20%
- Treatment: Cannulated screw fixation
Garden III - Complete, Partially Displaced:
- Complete fracture with partial displacement
- Trabecular lines of head misaligned with neck
- Head partially rotated but still some contact with neck
- AVN risk: 20-30%
- Treatment: Arthroplasty (elderly), urgent reduction and fixation (young)
Garden IV - Complete, Fully Displaced:
- Complete fracture with total displacement
- Trabecular lines of head align with acetabulum but not with neck
- Head fully dissociated from neck
- AVN risk: 30-100%
- Treatment: Arthroplasty (elderly), urgent reduction and fixation (young)
Clinical Simplification: Garden I-II (undisplaced) = FIX. Garden III-IV (displaced) = REPLACE (in elderly).
Reliability: Inter-observer agreement only moderate (kappa 0.4-0.6). Many surgeons simplify to just displaced vs undisplaced.
Clinical Presentation
History
Elderly Patient (Low-Energy Fall):
- Pain in groin, hip, or referred to knee
- Unable to weight-bear following fall from standing height
- Falls at home (bathroom, bedroom) or on street/stairs
- May report hearing/feeling "snap" or "pop" at time of injury
- Risk factors: Osteoporosis, age greater than 65 years, previous fragility fracture, low BMI, sedentary lifestyle
Young Patient (High-Energy Trauma):
- Road traffic accident, fall from height, sports injury
- Severe pain, inability to move leg
- May have polytrauma with other injuries
Examination
Inspection:
- Patient lying still, reluctant to move affected leg
- Classic posture: Leg shortened, externally rotated (typically 90 degrees), adducted
- Look for: swelling, bruising (may be minimal acutely), deformity
Palpation:
- Tenderness over groin/hip
- Pain on log-rolling leg (specific test - gentle internal/external rotation)
- Check peripheral pulses (dorsalis pedis, posterior tibial)
- Neurovascular exam: Sciatic nerve function (foot dorsiflexion/plantarflexion, sensation)
Movement:
- Active movement: Patient cannot straight leg raise or flex hip
- Passive movement: Painful with any attempt
- Do NOT stress fracture - risk displacement
Special Considerations
Impacted Fractures (Garden I):
- May be able to weight-bear partially (patient walked after fall)
- Less obvious deformity
- Diagnosis can be missed - have high index of suspicion
Occult Fractures:
- Pain but normal X-rays initially
- MRI or CT needed to confirm
- Treat as fracture until excluded
Differential Diagnosis
The painful, non-weight-bearing hip in an older patient has several mimics. The key discriminators are fracture location (intracapsular vs extracapsular) and whether plain films are diagnostic.
- Key Distinguishing Features
- Shortened, externally rotated, abducted leg; pain on log-roll; intracapsular = AVN risk
- Investigation / Action
- AP pelvis + cross-table lateral; classify (Garden/Pauwels)
- Key Distinguishing Features
- Extracapsular, lower AVN risk; often more shortening/bruising; cephalomedullary nail or DHS
- Investigation / Action
- AP/lateral hip; distinguishes implant choice
- Key Distinguishing Features
- Below lesser trochanter; high shear/deforming forces; consider atypical (bisphosphonate) fracture
- Investigation / Action
- Full-length femur films; review bisphosphonate history
- Key Distinguishing Features
- Hip pain, unable to weight-bear, NORMAL initial X-ray
- Investigation / Action
- MRI (gold standard) or CT; treat as fracture until excluded
- Key Distinguishing Features
- Prodromal pain weeks-months, minimal trauma, lytic/sclerotic lesion, constitutional symptoms
- Investigation / Action
- Staging CT, myeloma screen, bone scan/PET, biopsy
- Key Distinguishing Features
- Groin pain, may weight-bear partially, normal proximal femur
- Investigation / Action
- AP pelvis; CT if acetabulum suspected
- Key Distinguishing Features
- Lateral tenderness, able to straight-leg raise, no shortening/rotation
- Investigation / Action
- Clinical; X-ray to exclude fracture
Investigations
Imaging
Plain Radiographs (First-line):
- AP pelvis: Shows both hips for comparison, assess acetabulum
- Lateral hip: Cross-table lateral (avoid moving patient excessively)
- Look for: Fracture line, displacement, Garden classification, Shenton's line disruption
CT Scan:
- Indications: Occult fracture (suspected clinically but X-ray negative), complex fracture patterns, pre-operative planning for young patients
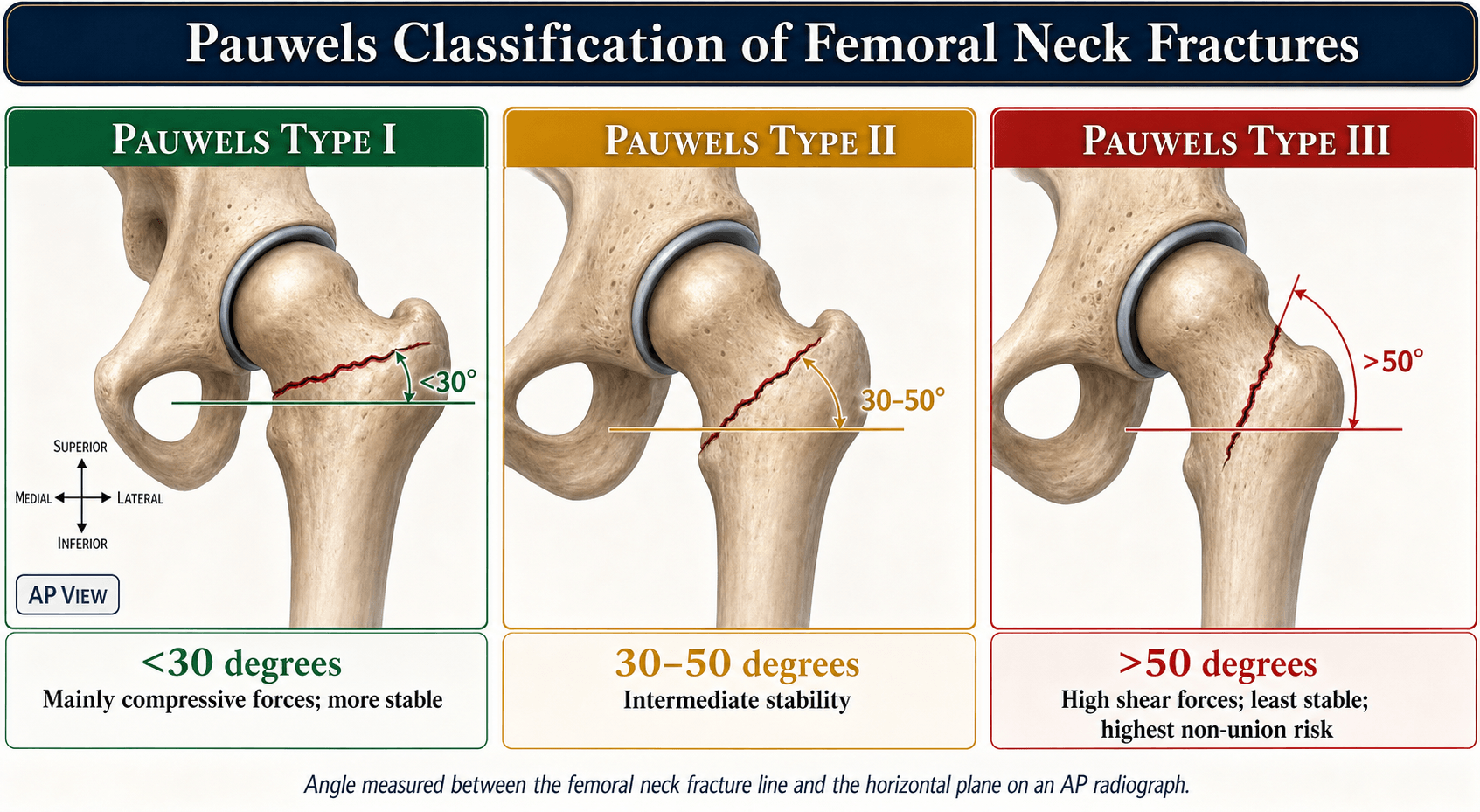
- Better delineation of fracture pattern, posterior comminution, vertical fracture angle (Pauwels classification)
MRI:
- Gold standard for occult fractures
- High sensitivity (99%) and specificity (95%)
- Shows bone marrow edema, undisplaced fracture lines not visible on X-ray
- Indicated when: clinical suspicion high but X-ray normal, patient unable to mobilize post-fall
Laboratory Tests
Pre-operative Bloods:
- FBC: Baseline hemoglobin (anemia common in elderly, may need transfusion)
- U&E: Renal function for anesthesia, contrast studies
- Coagulation: INR if on warfarin, platelet count if on antiplatelet agents
- Group and Save/Cross-match: For anticipated blood loss in arthroplasty
- CRP/ESR: Baseline (may be elevated due to fracture, useful if later infection suspected)
Cardiac Assessment:
- ECG: All patients (high-risk population for cardiac disease)
- Troponin: If chest pain or ECG changes (myocardial injury common post-fracture)
- Echocardiogram: If significant cardiac history or murmur detected
Bone Health Investigations (Post-acute):
- DEXA scan: Assess bone mineral density (osteoporosis)
- Vitamin D levels: Often deficient, correct post-operatively
- Calcium, phosphate, PTH: If secondary causes of osteoporosis suspected
- Thyroid function: Hyperthyroidism causes bone loss
Medical Optimization
Essential Pre-op Assessment:
- Cardiac clearance: Anesthesia review, optimization of cardiac medications
- Anticoagulation management: Reverse warfarin if needed (Vitamin K, PCC), hold DOACs appropriately
- Fluid resuscitation: Elderly often dehydrated, correct hypovolemia
- Pain control: Fascia iliaca block (regional anesthesia reduces opioid requirement)
Management
Treatment: Internal fixation with cannulated screws (typically 3 screws in inverted triangle configuration).
Rationale: Blood supply is preserved. Screw fixation stabilizes the fracture and allows healing.
Caution: Garden I (impacted valgus) can displace if not fixed. Most surgeons recommend fixation.
Post-op: Protected weight-bearing initially. Monitor for AVN and nonunion.
Hip fracture is a surgical emergency. Surgery within 36-48 hours is associated with lower mortality, fewer medical complications, shorter hospital stay. Delays significantly increase mortality.
Surgical Techniques
Internal Fixation for Undisplaced or Young Patients
Indications:
- Undisplaced fractures (Garden I-II) all ages
- Displaced fractures (Garden III-IV) in physiologically young patients (less than 60-65 years)
Patient Positioning:
- Supine on fracture table with gentle traction
- Image intensifier for AP and lateral views
Reduction Technique (if displaced):
- Leadbetter maneuver: Gentle longitudinal traction, flexion 15-30°, abduction 20-30°, internal rotation 15°
- Check fluoroscopy: aim for an acceptable Garden alignment index of 155-180 degrees on BOTH the AP and lateral views (the index is the angle of the medial compressive trabeculae of the head to the medial femoral cortex; do not confuse it with the Pauwels fracture-line angle)
- Acceptable criteria: Less than 20° angulation, less than 2mm displacement
- If closed reduction fails → Open reduction (Watson-Jones or Smith-Petersen approach)
Guidewire Placement:
- 3 wires in inverted triangle configuration
- Inferior wire along calcar (inferior neck)
- Two superior wires divergent
- Parallel in sagittal plane
- All within 5mm of subchondral bone
- Critical: Avoid joint penetration (check lateral view)
Screw Insertion:
- Partially threaded cannulated screws (6.5mm or 7.3mm diameter)
- Threads cross fracture site
- Compression by tightening screws
- Inferior screw provides calcar support (prevents varus collapse)
Biomechanics:
- Inverted triangle = best rotational stability
- Parallel configuration = compression
- Screws span fracture and engage far cortex
Post-operative:
- Touch weight-bearing initially, advance as tolerated
Capsulotomy:
- Controversial for AVN prevention
- FAITH trial: No benefit demonstrated
- Consider if delayed presentation (greater than 12 hours)
Biomechanics and Fixation Principles
Forces Acting on Femoral Neck
The femoral neck experiences complex loading during weight-bearing:
Compressive Forces (Primary):
- Body weight transmitted from acetabulum to femoral head
- Magnitude: 3-5x body weight (walking), up to 8x (running)
- Concentrated on superomedial femoral head (weight-bearing zone)
Tensile Forces:
- Along inferomedial cortex (calcar femorale)
- Generated by moment arm of body weight
- Resisted by thick cortical bone at calcar
Shear Forces:
- Parallel to fracture line
- Increase with fracture verticality (Pauwels angle)
- Pauwels III (greater than 50°): Predominantly shear → high failure risk
Rotational Forces:
- Torsion from muscle attachments (gluteus medius, iliopsoas)
- Cause rotation and displacement of fracture fragments
Trabecular Architecture
The femoral neck contains two main trabecular systems:
Primary Compressive Trabeculae (Vertical):
- Run from medial calcar to superior femoral head
- Resist compressive loads during weight-bearing
- Strongest trabecular system
Primary Tensile Trabeculae (Arcuate):
- Arc from lateral cortex to inferior femoral head
- Resist tensile forces along inferior neck
- Important for fracture stability
Secondary Compressive Trabeculae:
- From greater trochanter to femoral head
- Provide additional support
Ward's Triangle:
- Area of relative weakness (few trabeculae)
- Located in femoral neck between trabecular systems
- Common site of fracture initiation in osteoporotic bone
Orthogeriatric Co-Management - Systematic Review and Meta-Analysis
- 37 studies, 37,294 hip fracture patients across orthogeriatric care models
- 28% lower in-hospital mortality (RR 0.72, 95% CI 0.56 to 0.92)
- 14% lower 1-year mortality (RR 0.86, 95% CI 0.76 to 0.97)
- 19% lower risk of delirium and reduced length of stay (mean about minus 1.55 days)
- No single orthogeriatric model (consultant service, geriatric ward, integrated) proven superior
Peripheral Nerve Blocks for Analgesia - Cochrane Review
- 31 RCTs, 1760 participants (includes fascia iliaca and femoral nerve blocks)
- Reduced pain on movement within 30 minutes of block (SMD minus 1.41, high-quality evidence)
- Reduced risk of pneumonia (RR 0.41; NNT 7, moderate-quality evidence)
- Reduced time to first mobilisation after surgery (about 11 hours earlier)
- Lower analgesic drug cost with single-shot blocks
PAUWELS = Predict AVN Using Fracture AnglePauwels Classification
Hook:Pauwels III = VERTICAL = shear forces = needs stronger fixation (DHS not screws)!
PALNOF Arthroplasty Approaches
Hook:PAL approaches - Posterior most common but repair or dislocate!
Complications
Early Complications - First Days After Surgery
Mortality:
- 30-day mortality: 6-8%
- 1-year mortality: 25-30%
- Higher in elderly, frail, multiple comorbidities
- Delayed surgery (greater than 48 hours) increases mortality significantly
Medical Complications:
- Pressure sores: Prolonged immobility pre-operatively
- Pneumonia: Aspiration, reduced mobility, general anesthesia
- DVT/PE: High risk in elderly immobile patients
- UTI: Catheterization, dehydration
- Delirium: 20-50% of elderly post-op (pain, medications, unfamiliar environment)
- Myocardial infarction: Surgical stress, cardiac demand
Surgical Complications:
- Bleeding: Arthroplasty (300-500mL blood loss), may require transfusion
- Infection: Superficial (2-3%) or deep periprosthetic (less than 1%)
- Nerve injury: Sciatic (posterior approach, less than 1%), femoral (anterior, rare)
- Vascular injury: Femoral vessels (anterior approach - rare but catastrophic)
Rehabilitation and Outcomes
Post-operative Mobilization
Early Mobilization (Day 1 Post-op):
- Goal: Out of bed within 24 hours of surgery
- Strong evidence that early mobilization reduces:
- Pneumonia (40% reduction)
- Pressure sores (50% reduction)
- DVT/PE (30% reduction)
- Delirium (20% reduction)
Weight-Bearing Status:
After Arthroplasty (Hemiarthroplasty or THR):
- Weight-bearing as tolerated (WBAT) immediately
- No need for protected weight-bearing (implant is load-bearing)
- Encourage full weight-bearing as pain allows
- Walking aids (frame, crutches) for balance support initially
After Internal Fixation (Undisplaced Garden I-II):
- Touch weight-bearing for 6 weeks (some surgeons allow WBAT if stable fixation)
- Progress to partial weight-bearing (50%) at 6 weeks (if X-ray shows healing)
- Full weight-bearing at 12 weeks (if united)
- Risk of displacement if full weight-bearing too early
After Internal Fixation (Displaced Garden III-IV in Young):
- Strict non weight-bearing for 6-12 weeks
- High risk of fixation failure, AVN, nonunion
- Advance weight-bearing very cautiously based on serial X-rays
Hip Precautions (After Arthroplasty)
For Posterior Approach (Most Common):
- Avoid:
- Hip flexion greater than 90 degrees (no low chairs, toilet seats)
- Hip adduction across midline (no crossing legs)
- Internal rotation (avoid twisting inward)
- Duration: 6 weeks (some surgeons recommend 12 weeks)
- Risk: Posterior dislocation if precautions violated
- Note: If external rotators repaired well, some surgeons omit precautions (evidence mixed)
For Anterior/Anterolateral Approach:
- Avoid hip extension and external rotation
- Less restrictive than posterior approach precautions
- Lower dislocation risk overall
Guidelines, Registries & Global Practice
Global Burden and Projection of Hip Fracture
- Worldwide hip fractures estimated at 1.26 million in 1990 (338,000 men; 917,000 women)
- Projected to roughly double to 2.6 million by 2025 and 4.5 million by 2050 (age/sex-specific rates held constant)
- Proportional rise greater in men (about 310%) than women (about 240%)
- Asia's share of global hip fractures projected to rise from 26% (1990) to about 45% by 2050
Global Guideline Comparison
The fundamentals are consistent across major bodies; the main areas of genuine variation are the THA-vs-hemiarthroplasty threshold and the surgical-timing target.
- AAOS (USA)
- Within 24-48 h of admission (moderate evidence)
- NICE NG124 / BOAST (UK)
- On day of, or day after, admission (within 36 h)
- AO Foundation / EFORT (Europe)
- Early surgery, generally within 24-48 h
- AAOS (USA)
- Arthroplasty; THA an option for active patients
- NICE NG124 / BOAST (UK)
- THA if independently mobile, not cognitively impaired, medically fit
- AO Foundation / EFORT (Europe)
- Arthroplasty; THA for active, independent patients
- AAOS (USA)
- Cemented favoured (strong evidence)
- NICE NG124 / BOAST (UK)
- Cemented implant recommended
- AO Foundation / EFORT (Europe)
- Cemented favoured to reduce periprosthetic fracture
- AAOS (USA)
- Internal fixation
- NICE NG124 / BOAST (UK)
- Internal fixation; preserve head in younger patients
- AO Foundation / EFORT (Europe)
- Internal fixation; reduction quality emphasised
- AAOS (USA)
- Multimodal; regional/nerve blocks
- NICE NG124 / BOAST (UK)
- Offer nerve block (e.g. fascia iliaca) on presentation
- AO Foundation / EFORT (Europe)
- Multimodal incl. regional blocks
- AAOS (USA)
- Orthogeriatric co-management; treat osteoporosis
- NICE NG124 / BOAST (UK)
- Orthogeriatric/Hip Fracture Programme; FLS, bone protection
- AO Foundation / EFORT (Europe)
- Orthogeriatric pathways; secondary prevention
Registry Evidence (No PMID - Annual Registry Reports)
National Registry Evidence - Joint Replacement and Hip Fracture Registries
- AOANJRR (Australia): cemented stems and dual-mobility constructs reduce revision for fracture arthroplasty vs uncemented in older patients
- NJR (England, Wales, NI): large-volume data support cemented fixation and document dislocation as a leading early revision cause after THA for fracture
- ANZHFR / NHFD (UK): casemix-adjusted benchmarking links time-to-surgery and orthogeriatric input to lower mortality and length of stay
- Registries are observational; used for surveillance, benchmarking and implant performance rather than as randomised evidence
Epidemiology and Registry Snapshot (ANZHFR)
National and regional registries quantify the burden and benchmark outcomes. The ANZHFR (Australia and New Zealand) figures below are illustrative of the orders of magnitude seen across high-income settings:
Incidence and Burden (ANZHFR 2023):
- Approximately 20,000-22,000 hip fractures annually across the binational catchment
- Incidence rate: 150-200 per 100,000 population over age 65
- Female:male ratio approximately 3:1
- Projected to double by 2050 due to aging populations
- Annual economic burden: large by any measure — multi-billion-dollar costs in acute care, rehabilitation and long-term care in high-income health economies worldwide
Mortality (ANZHFR 2023):
- 30-day mortality: 6.2% (national average)
- 1-year mortality: 27.3%
- 5-year mortality: approximately 50%
- Casemix-adjusted variation between centres: top-quartile hospitals achieve 5-6% 30-day mortality, while rural/remote and under-resourced sites report 8-10%
Geographic and Equity Variation (global theme):
- Rural/remote vs urban: rural areas show slightly higher mortality and longer time to surgery (access and transfer logistics)
- Under-served and Indigenous populations: Registry data show hip fractures occur 10-15 years earlier in Indigenous populations, with higher mortality — a disparity mirrored in other under-served groups worldwide
- Remote communities: significant challenges with evacuation, surgical access and rehabilitation
Australian Hip Fracture Registry (ANZHFR)
The ANZHFR is a binational registry (Australia and New Zealand) established in 2015 to monitor and improve hip fracture care quality.
Key Performance Indicators (2023 National Report):
- Surgery within 48 hours: 82.4% nationally (target greater than 85%)
- Best performers: 90-95% (major metropolitan hospitals)
- Challenges: Rural hospitals, weekend admissions, medically complex patients
- Orthogeriatric assessment within 72 hours: 76.8% (target greater than 80%)
- Bone protection prescribed at discharge: 68.5% (target greater than 80%)
- Post-discharge fracture liaison service contact: 45.2% (target greater than 70% - needs improvement)
Registry Data Insights:
- Hospitals with dedicated hip fracture pathways have 30-40% lower mortality
- Orthogeriatric co-management associated with 2-day reduction in length of stay
- Weekend admissions have 15% longer time to surgery (resource constraints)
Special Populations
Mechanism: Usually high-energy trauma (RTA, fall from height)
Key Differences:
- Preserve femoral head at almost any cost - avoid arthroplasty if possible
- Even if AVN risk 30%, preferable to THR at age 40-50 (revision burden)
- Urgent surgery (ideally less than 6 hours) to minimize AVN
- Anatomic reduction mandatory - accept nothing less
- Strong fixation: Consider DHS for vertical fractures (Pauwels III)
- Prolonged follow-up: Monitor for AVN (can occur 2-5 years post-fixation)
If Fixation Fails:
- Salvage options: Valgus osteotomy (if nonunion), arthroplasty (if AVN)
- THR considerations in young: Uncemented implants, hard-on-hard bearings (ceramic-on-ceramic, highly cross-linked polyethylene), anticipate multiple revisions over lifetime
MCQ Practice Points
Q: What distinguishes Garden I from Garden II femoral neck fractures?
A: Garden I is an incomplete/impacted fracture with the head tilted into valgus. Garden II is complete but non-displaced with trabecular alignment preserved. Both are undisplaced and treated with screw fixation. Key difference: Garden I has visible trabecular lines crossing fracture; Garden II has complete fracture line but no displacement.
Q: Why do displaced femoral neck fractures have high AVN rates?
A: The medial femoral circumflex artery (MFCA) gives rise to lateral epiphyseal vessels which provide the main blood supply to the femoral head. These vessels run along the posterior-superior femoral neck. Displaced fractures disrupt this supply, causing AVN rates of 20-30% in young patients and even higher in delayed treatment. This is why displaced fractures in elderly warrant arthroplasty rather than fixation.
Q: What are the indications for THR over hemiarthroplasty in displaced NOF fractures?
A: THR is indicated for patients who are: cognitively intact, independently mobile (walking outdoors), and have life expectancy greater than 4 years. THR provides better function and lower reoperation rates. Hemiarthroplasty is preferred for: cognitive impairment, limited mobility, frail patients. NICE guidelines recommend THR for independently mobile patients.
Q: How do you manage a displaced NOF fracture in a 45-year-old?
A: Urgent reduction and internal fixation (ideally within 6 hours) to minimize AVN risk. Use closed or open reduction with 3 cannulated screws (inverted triangle) or sliding hip screw. Despite high complication rates (AVN 20-30%, nonunion 10-20%), preserving the native hip is preferred over arthroplasty in young patients. Counsel patient about potential need for future arthroplasty.
At a Glance
Neck of femur fractures are orthopaedic emergencies requiring surgery within 36-48 hours to reduce mortality and complications. The Garden classification guides treatment: Garden I-II (undisplaced) undergo cannulated screw fixation in inverted triangle configuration, while Garden III-IV (displaced) in elderly patients require arthroplasty. Blood supply via the medial femoral circumflex artery (MFCA) is disrupted in displaced fractures, leading to high AVN risk. THA is indicated for cognitively intact, independently mobile patients with expected survival greater than 4 years; hemiarthroplasty for frail, cognitively impaired, or limited mobility patients. Young patients (under 60 years) with displaced fractures receive urgent reduction and internal fixation to preserve the femoral head. 1-year mortality is approximately 30% in elderly populations.
FIX-REPLACEGarden Simplified
Hook:I/II = FIX with screws. III/IV = REPLACE (arthroplasty)!
MICTHR Indications
Hook:MIC check before THR - Mobile, Intact, Continued survival!
MFCA-LEVNOF Blood Supply
Hook:MFCA gives LEV - disrupt it and head dies!
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“An 80-year-old woman with osteoporosis falls at home and has a Garden IV neck of femur fracture. She was previously independently mobile and cognitively intact. How do you manage?”
“A 78-year-old woman presents to the emergency department at 10pm with a Garden III displaced neck of femur fracture following a fall at home. She takes warfarin for atrial fibrillation. Her INR is 3.2 (therapeutic range 2.0-3.0 for AF). She is otherwise stable with no other injuries. The anaesthetist asks whether you want to reverse her warfarin and operate tonight, or wait for the INR to normalize naturally over the next 48 hours. What factors do you consider and how do you proceed?”
“A 42-year-old man is brought to your trauma center following a high-speed motorcycle accident. He has multiple injuries including a closed head injury (GCS 14), liver laceration being managed conservatively, and a Garden IV displaced neck of femur fracture. It is now 8 hours since injury. He is hemodynamically stable. X-rays show the femoral neck fracture is very vertical (Pauwels Type III) with significant posterior comminution. What are your management options and what factors influence your decision?”
“A 68-year-old woman presents with a Garden III femoral neck fracture after a minor fall in the bathroom. On questioning, she mentions she has had worsening hip pain for the past 3 months that was present even before the fall. She attributes it to 'arthritis'. On examination, the fracture site is more tender than expected, and she appears cachectic. X-ray shows a displaced femoral neck fracture with some lytic changes in the intertrochanteric region. How do you approach this case?”
“A 72-year-old man with Parkinson's disease has a fall at home and is brought to the emergency department. X-ray pelvis shows displaced femoral neck fractures bilaterally (Garden IV both sides). He is medically stable but in significant pain. The emergency department physician asks you urgently whether this is possible or if there's been a mix-up with the X-rays. How do you approach this rare presentation and what are your management priorities?”
Garden Classification
- I/II: Undisplaced → SCREWS
- III/IV: Displaced → ARTHROPLASTY (elderly)
Arthroplasty Choice
- THR: Mobile, cognitively intact, good life expectancy
- Hemiarthroplasty: Frail, impaired cognition, limited mobility
Key Points
- Surgery within 36-48 hours
- MFCA supply disrupted → AVN risk
- Young displaced: Attempt fixation urgently
Post-Op Care
- DVT prophylaxis
- Early mobilization
- Bone protection (bisphosphonates)
- Falls assessment
Evidence Base
THR vs Hemiarthroplasty - HEALTH Trial
- 1495 independently ambulating patients, age 50+, displaced femoral neck fracture, 80 centres in 10 countries
- Secondary hip procedure within 24 months: 7.9% THA vs 8.3% hemiarthroplasty (HR 0.95, not significant)
- Hip instability or dislocation: 4.7% THA vs 2.4% hemiarthroplasty
- Mortality similar (14.3% THA vs 13.1% hemiarthroplasty); function/quality of life only modestly favoured THA
Timing of Surgery - HIP ATTACK Trial
- 2970 patients, 69 hospitals, 17 countries; accelerated surgery (median 6 h) vs standard care (median 24 h)
- No difference in 90-day mortality: 9% vs 10% (HR 0.91, 95% CI 0.72 to 1.14)
- No difference in composite of major complications: 22% vs 22% (HR 0.97)
- Accelerated surgery did not significantly lower mortality or major complications
Cemented vs Uncemented Hemiarthroplasty - WHiTE 5 Trial
- UK multicentre RCT of cemented vs hydroxyapatite-coated uncemented hemiarthroplasty for displaced intracapsular hip fracture
- Cemented implants were cost-saving (mean difference about minus 961 pounds)
- Cemented implants increased quality-adjusted life years (mean QALY difference 0.010)
- Cemented hemiarthroplasty 95 to 97% probability of being cost-effective
Internal Fixation Method - FAITH Trial
- 1108 patients age 50+ with low-energy hip fracture; sliding hip screw vs multiple cancellous screws
- 24-month reoperation: 20% (SHS) vs 22% (screws) - no significant difference (HR 0.83)
- Avascular necrosis MORE common with sliding hip screw: 9% vs 5% (HR 1.91)
- Subgroups (smokers, displaced or base-of-neck fractures) may do better with a sliding hip screw