Seddon and Sunderland Classifications | Wallerian Degeneration | Schwann Cell Bands of Büngner | 1mm/day Growth
- Wallerian degeneration occurs distal to injury site within 24-48 hours
- Chromatolysis is the proximal cell body response preparing for regeneration
- Schwann cells form bands of Büngner guiding axonal regrowth
- Growth cone at axon tip extends 1mm per day in peripheral nerves
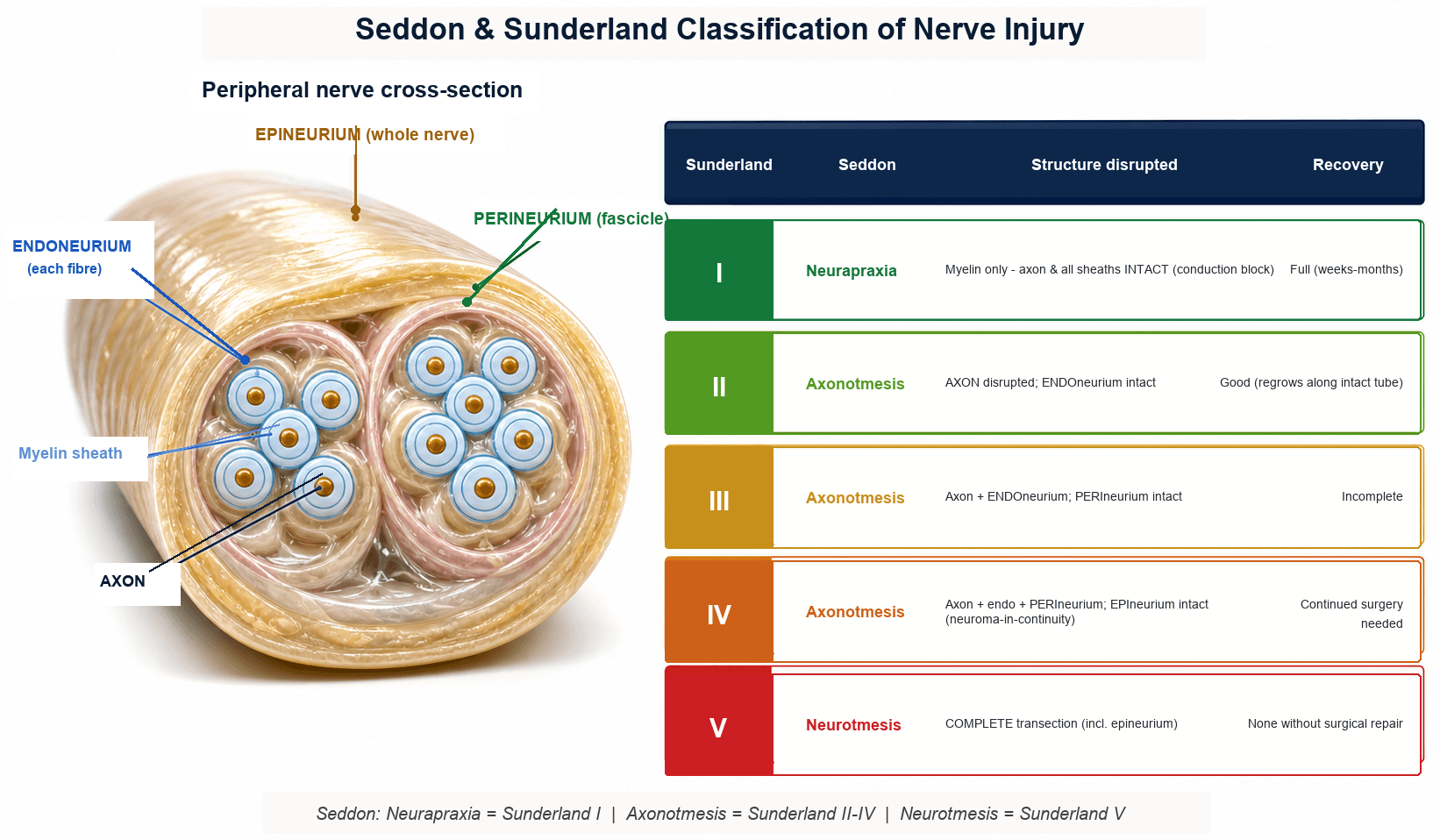
- Sunderland classification has 5 degrees based on which structures are injured
- “Seddon: neurapraxia, axonotmesis, neurotmesis (increasing severity)
- “Sunderland adds detail: degrees I-V (I = neurapraxia, V = neurotmesis)
- “Tinel sign progression indicates axonal regeneration front
- “Primary repair within 3 months has better outcomes than delayed repair
Axon and myelin distal to injury degenerate within 24-48 hours. Schwann cells phagocytose debris and proliferate to form bands of Büngner. This is essential to clear path for regenerating axon.
Cell body response to axonal injury. Nissl substance disperses, nucleus becomes eccentric, cell body swells. Peaks at 7-14 days. Cell shifts from neurotransmission to regeneration mode.
Schwann cells are critical for regeneration. They form bands of Büngner (tubular scaffolds), secrete growth factors (NGF, BDNF, GDNF), and guide axons to targets. Without endoneurial tubes, misdirection occurs.
Growth cone at axon tip extends filopodia sensing chemical gradients. Responds to neurotrophic factors and extracellular matrix cues. Rate of 1mm per day limits functional recovery in proximal injuries.
Overview and Classification
Peripheral nerve injury is common in trauma and surgical complications. Understanding the biological response to nerve injury is fundamental to predicting recovery and determining surgical indications. The nerve's capacity for regeneration depends on injury severity, timing of repair, and preservation of endoneurial architecture.
Why nerve injury biology matters clinically:
Seddon/Sunderland classification determines expected recovery. Neurapraxia recovers fully, axonotmesis recovers well if endoneurium intact, neurotmesis requires surgical repair. Electrodiagnostics differentiate types.
Primary repair within 3 months optimal. Delayed repair allows fibrosis of endoneurial tubes and target muscle atrophy. After 18-24 months motor recovery unlikely even with perfect repair.
Seddon (1943) has 3 types based on functional outcomes. Sunderland (1951) has 5 degrees based on anatomical structures injured. Seddon is simpler for clinical use. Sunderland adds detail: degree I equals neurapraxia, degrees II-IV are types of axonotmesis with increasing structural damage, degree V equals neurotmesis.
Concepts and Mechanisms
Peripheral nerve regeneration depends on three fundamental biological processes working in concert:
1. Wallerian Degeneration (Distal Stump)
The distal nerve segment undergoes active degeneration starting 24-48 hours after injury. This is not passive decay but a coordinated cellular response:
- Axon fragments into ellipsoids
- Myelin breaks down into lipid droplets
- Schwann cells phagocytose debris (40-50%)
- Macrophages recruited to clear remaining debris
- c-Jun activation drives Schwann cell transformation
Purpose: Clear inhibitory molecules (MAG, Nogo) and create permissive environment.
2. Chromatolysis (Proximal Cell Body)
The neuronal cell body in dorsal root ganglion (sensory) or anterior horn (motor) undergoes metabolic reprogramming:
- Nissl substance disperses (rough ER moves to periphery)
- Nucleus becomes eccentric
- Cell body swells 30-50%
- Gene expression shifts from neurotransmission to growth
- Upregulate GAP-43, tubulin, actin
Purpose: Prepare neuron for axonal regeneration by producing growth-associated proteins.
3. Axonal Regeneration (Growth Cone)
The proximal axon stump forms a growth cone that navigates toward the target:
- Multiple sprouts emerge (20-50 initially)
- Growth cone extends filopodia sensing chemical gradients
- Follows bands of Büngner in endoneurial tubes
- Advances 1-3mm per day
- Forms synapse when target contacted
Purpose: Re-establish neuronal connection to target organ (muscle, skin receptor).
All three processes must succeed for functional recovery. Wallerian degeneration without regeneration leaves denervated targets. Chromatolysis without successful reinnervation leads to neuronal death. Growth cone navigation without intact endoneurial tubes causes neuroma formation.
Key Biological Principles
Intact endoneurial tubes (axonotmesis) allow bands of Büngner to guide regenerating axons to correct targets. Disrupted tubes (neurotmesis) cause misdirection and poor outcomes even with surgical repair.
Schwann cell bands persist 3-4 months then deteriorate. Muscle endplates survive 18-24 months then degenerate. These biological clocks determine surgical timing windows.
1mm per day regeneration limits functional recovery in proximal injuries. A 30cm injury requires 300 days (10 months) for axons to reach distal muscles - often exceeding viable reinnervation window.
Schwann cells orchestrate regeneration by clearing debris, forming guidance tubes, secreting neurotrophins (NGF, BDNF, GDNF), and remyelinating. Without Schwann cell response, regeneration fails.
Anatomy
Peripheral Nerve Structure
- Surrounds
- Individual axons
- Function
- Collagen tubes for Schwann cells
- Clinical Significance
- Preservation critical for regeneration guidance
- Surrounds
- Fascicles (groups of axons)
- Function
- Blood-nerve barrier, tensile strength
- Clinical Significance
- Disruption causes axonal misdirection
- Surrounds
- Entire nerve trunk
- Function
- External protective layer, blood supply entry
- Clinical Significance
- Surgical plane for nerve repair
Myelinated fibers:
- One Schwann cell per internode (1-2mm)
- Nodes of Ranvier between internodes
- Saltatory conduction (fast)
Unmyelinated fibers:
- One Schwann cell wraps multiple axons
- Slower conduction velocity
Extrinsic supply:
- Segmental vessels from adjacent arteries
- Enter through epineurium
Intrinsic supply:
- Longitudinal network in epineurium
- Critical for survival during mobilization
The endoneurial tube is the key to successful regeneration.
- If endoneurium intact (axonotmesis): Regenerating axon follows the tube to its original target
- If endoneurium disrupted (neurotmesis): Axons enter wrong tubes → misdirection → poor functional recovery
Bands of Büngner form within endoneurial tubes, providing guidance scaffolds.
Classification Systems
Seddon Classification (1943)
Three types based on severity and prognosis:
- Neurapraxia
- Intact
- Axonotmesis
- Disrupted
- Neurotmesis
- Disrupted
- Neurapraxia
- Intact
- Axonotmesis
- Intact
- Neurotmesis
- Disrupted
- Neurapraxia
- No
- Axonotmesis
- Yes (distal)
- Neurotmesis
- Yes (distal)
- Neurapraxia
- Blocked locally
- Axonotmesis
- Lost distal
- Neurotmesis
- Lost distal
- Neurapraxia
- Excellent (weeks-months)
- Axonotmesis
- Good (months)
- Neurotmesis
- Poor without surgery
- Neurapraxia
- Demyelination recovery
- Axonotmesis
- 1mm per day regrowth
- Neurotmesis
- Depends on repair quality
Neurapraxia is a local conduction block from myelin injury (compression, traction, ischemia). The axon remains in continuity. No Wallerian degeneration occurs. Recovery is complete within weeks to months as myelin regenerates. Most common in Saturday night palsy (radial nerve compression), prolonged tourniquet use.
Axonotmesis involves axonal disruption but preservation of endoneurial tubes (and perineurium, epineurium). Wallerian degeneration occurs distal to injury. Proximal axon regenerates through intact endoneurial tubes at 1mm per day. Prognosis is good because bands of Büngner guide axons to original targets. May occur with severe traction, crush, or ischemia.
Neurotmesis is complete nerve transection with disruption of all structures including endoneurium. Wallerian degeneration occurs but regenerating axons have no guidance channels. Neuroma forms at injury site. Surgical repair is required for any recovery. Even with repair, outcomes are limited by misdirection and target muscle atrophy.
This classification is most useful clinically.
From inside out: endoneurium (surrounds individual axons), perineurium (surrounds fascicles), epineurium (surrounds entire nerve). Blood supply enters through epineurium. Injury to deeper layers causes more misdirection during regeneration.
Wallerian Degeneration
Wallerian degeneration is the process of axonal and myelin breakdown distal to a nerve injury site. Named after Augustus Waller (1850) who first described it. This is an active process, not passive decay, requiring Schwann cells and macrophages.
Wallerian Degeneration Timeline
Immediate response: Axon transport interrupted, distal axon swells due to calcium influx, cytoskeleton breaks down.
Axonal fragmentation: Distal axon breaks into fragments (ellipsoids). Myelin sheath begins to fragment. Schwann cells detect injury signals.
Schwann cell activation: Schwann cells dedifferentiate, proliferate, and begin phagocytosing myelin debris. Macrophages recruited from blood.
Debris clearance: Macrophages and Schwann cells clear myelin and axonal debris. Schwann cells form columns (bands of Büngner) within endoneurial tubes.
Ready for regeneration: Endoneurial tubes clear, bands of Büngner secreting neurotrophic factors (NGF, BDNF, GDNF), awaiting regenerating axon.
Key molecular events:
- Calcium influx triggers axonal breakdown via calpain-mediated cytoskeletal degradation
- Ubiquitin-proteasome system degrades axonal proteins
- Schwann cells express c-Jun transcription factor driving dedifferentiation and pro-regenerative phenotype
- Macrophages recruited by CCL2 and MCP-1 chemokines secreted by Schwann cells
- Endoneurial fibroblasts proliferate if denervation prolonged, causing fibrosis
Wallerian degeneration is essential for regeneration. Myelin debris contains inhibitory molecules (MAG - myelin-associated glycoprotein) that block axonal growth. Clearing debris and converting Schwann cells to pro-regenerative state creates permissive environment. Without this, regeneration fails.
Proximal (retrograde) degeneration also occurs but is limited. Extends 3-5mm proximal to injury site (one or two nodes of Ranvier). If severe injury causes cell body death (chromatolysis failure), entire neuron dies.
Chromatolysis - Cell Body Response
Chromatolysis is the morphological and metabolic response of the neuronal cell body to axonal injury. The neuron switches from neurotransmission mode to regeneration mode. Occurs in dorsal root ganglion (sensory) and anterior horn (motor) cell bodies.
- Nissl substance dispersal - ribosomes and rough endoplasmic reticulum move from center to periphery (chromatolysis means dissolution of color on Nissl stain)
- Nuclear eccentricity - nucleus moves to cell periphery
- Cell body swelling - volume increases 30-50%
- Nucleolar enlargement - increased protein synthesis
- Downregulation of neurotransmitter genes (acetylcholine, neurotransmitter receptors)
- Upregulation of growth-associated genes - GAP-43, tubulin, actin, cytoskeletal proteins
- Increased protein synthesis - ribosomal RNA production, rough ER expansion
- Activation of transcription factors - ATF3, c-Jun, STAT3 drive regeneration program
- Enhanced axonal transport - kinesin and dynein motors upregulated
- Normal Neuron
- Central distribution
- Chromatolysis
- Dispersed to periphery
- Failed Regeneration
- Absent (atrophy)
- Normal Neuron
- Central
- Chromatolysis
- Eccentric (peripheral)
- Failed Regeneration
- Pyknotic (condensed)
- Normal Neuron
- Baseline
- Chromatolysis
- Increased 30-50%
- Failed Regeneration
- Decreased (shrinkage)
- Normal Neuron
- Neurotransmission
- Chromatolysis
- Growth and regeneration
- Failed Regeneration
- Apoptotic markers
- Normal Neuron
- Normal function
- Chromatolysis
- Regeneration if successful
- Failed Regeneration
- Cell death
Critical concept: Chromatolysis is a positive response indicating cell survival and regeneration attempt. Absence of chromatolysis after nerve injury suggests cell death. Prolonged chromatolysis beyond 3-4 weeks without successful regeneration leads to neuronal atrophy and eventual apoptosis.
Muscle atrophy parallels chromatolysis. Motor neurons that fail to reinnervate muscle within 12-18 months undergo apoptosis. Muscle fibers denervated beyond 18-24 months undergo irreversible fibrofatty degeneration. This is why timing of nerve repair is critical - delay beyond 6-12 months severely compromises motor recovery.
Schwann Cell Biology in Regeneration
Schwann cells are the glial cells of the peripheral nervous system. In myelinated fibers, one Schwann cell wraps one internode of myelin. After nerve injury, Schwann cells undergo dramatic phenotypic transformation to support regeneration.
Schwann cell functions in nerve regeneration:
Phagocytose myelin and axonal debris with macrophages. Schwann cells express phagocytic receptors and clear 40-50% of debris themselves. Secrete chemokines (CCL2, MCP-1) recruiting macrophages for remaining debris.
Form tubular scaffolds by aligning in columns within endoneurial tubes. Create physical guidance channels directing regenerating axons toward original targets. Without endoneurial tubes (neurotmesis), bands collapse and neuroma forms.
Secrete growth factors: NGF (nerve growth factor), BDNF (brain-derived neurotrophic factor), GDNF (glial-derived neurotrophic factor), CNTF (ciliary neurotrophic factor), and FGF (fibroblast growth factor). Create chemical gradient guiding growth cone.
Remyelinate regenerated axons once contact re-established. Transition back to myelinating phenotype. Remyelinated internodes are shorter and myelin thinner than original, explaining slower conduction velocity after regeneration.
Molecular regulation of Schwann cell response:
The transcription factor c-Jun is master regulator of Schwann cell dedifferentiation and pro-regenerative phenotype. c-Jun knockout mice show failed Wallerian degeneration and poor nerve regeneration.
- c-Jun upregulation drives dedifferentiation, proliferation, and growth factor secretion
- Sox2 expression maintains dedifferentiated state
- Neuregulin-1 signaling from regenerating axon promotes remyelination
- Laminin and fibronectin in Schwann cell basal lamina provide extracellular matrix cues for axonal growth
Schwann Cell Response After Nerve Injury
Detection of injury: Loss of axonal contact signals detected. Schwann cells sense absence of neuregulin-1 and other axonal signals.
Dedifferentiation: Schwann cells downregulate myelin genes (P0, MBP, PMP22), upregulate c-Jun and growth factor genes. Begin to proliferate.
Proliferation and alignment: Schwann cells divide and align into columns (bands of Büngner) within endoneurial tubes. Begin secreting neurotrophic factors.
Pro-regenerative state: Schwann cells maintain bands, secrete growth factors, clear debris with macrophages. Create permissive environment for axonal regrowth.
Remyelination or atrophy: If regenerating axon arrives, Schwann cells remyelinate. If no axon contact by 3-4 months, bands gradually deteriorate and endoneurial tubes fibrose.
Schwann cells maintain bands of Büngner for 3-4 months awaiting regenerating axon. After this, bands gradually deteriorate, endoneurial tubes collapse and fibrose. This is why nerve repair beyond 6-12 months has poor outcomes - loss of Schwann cell guidance and endoneurial tube integrity.
Neurotrophins and Their Receptors
The growth factors that repair Schwann cells secrete (NGF, BDNF, GDNF, CNTF) are named above, but they act on the regenerating neuron only through specific cell-surface receptors - the ligand-receptor pairing is high-yield basic science:
- Trk (tropomyosin-receptor-kinase) receptors - high-affinity receptor tyrosine kinases, each matched to a neurotrophin:
- TrkA binds NGF (nerve growth factor) - small sensory and sympathetic neurons
- TrkB binds BDNF and NT-4/5 - motor and many sensory neurons
- TrkC binds NT-3 (neurotrophin-3) - large proprioceptive neurons
- On ligand binding the receptor dimerises and autophosphorylates, activating PI3K/Akt (survival), Ras/MAPK (growth and differentiation) and PLC-gamma signalling that drives neuronal survival, axonal elongation and growth-cone advance.
- GDNF signals through a distinct two-part receptor - the GFR-alpha-1 co-receptor together with the RET receptor tyrosine kinase - and is particularly important for motor and sensory neuron survival after axotomy.
- p75NTR - the low-affinity pan-neurotrophin receptor (a TNF-receptor-superfamily member) binds all the neurotrophins (and their immature pro-forms). It modulates Trk signalling - sharpening ligand specificity and enhancing high-affinity binding - but, when expressed without a partnering Trk, can instead trigger apoptosis. p75NTR is strongly re-expressed by injured neurons and by repair Schwann cells, so it contributes both to regeneration support and, in a neuron that fails to reconnect, to programmed cell death.
The neurotrophins secreted by repair Schwann cells act on the neuron through matched high-affinity receptors - NGF→TrkA, BDNF→TrkB, NT-3→TrkC (and GDNF→GFR-alpha-1/RET), driving survival and growth-cone advance via PI3K-Akt and Ras-MAPK. The low-affinity p75NTR binds all neurotrophins, tunes Trk specificity, and - uncoupled from Trk - can drive apoptosis of neurons that fail to reconnect.
Axonal Regeneration and Growth Cone
Axonal regeneration begins within days of injury. The proximal axon stump forms a growth cone at its tip, which extends processes (filopodia and lamellipodia) sensing the local environment and navigating toward the target.
Growth cone structure and function:
The growth cone is a specialized structure at the regenerating axon tip containing:
- Filopodia - thin finger-like projections extending 10-50 micrometers, sensing chemical and physical cues
- Lamellipodia - sheet-like membrane expansions between filopodia, providing surface for advancement
- Growth cone receptors - Trk receptors for neurotrophins (NGF, BDNF, GDNF), integrins for extracellular matrix, semaphorin receptors, ephrin receptors
- Cytoskeletal machinery - actin filaments in filopodia, microtubules in central domain, motor proteins (myosin, kinesin) for advancement
Guidance mechanisms:
- Molecules
- NGF, BDNF, GDNF, CNTF
- Effect
- Growth cone advances toward gradient
- Source
- Schwann cells, target organ
- Molecules
- Laminin, fibronectin, N-CAM
- Effect
- Growth cone adheres and advances
- Source
- Schwann cell basal lamina, ECM
- Molecules
- Semaphorins, Slits
- Effect
- Growth cone retracts from inappropriate paths
- Source
- Non-target tissue
- Molecules
- MAG, Nogo, OMgp (myelin proteins)
- Effect
- Growth cone stalls
- Source
- Myelin debris (if not cleared)
- Proximal stump sealing (0-24 hours) - calcium influx triggers membrane sealing at injury site
- Growth cone formation (24-72 hours) - multiple sprouts emerge from proximal stump (up to 20-50 initially)
- Endoneurial tube entry (3-7 days) - sprouts that successfully enter endoneurial tubes advance, others retract
- Elongation (weeks to months) - growth cone extends at 1-3mm per day along band of Büngner guidance
- Target contact (months) - growth cone reaches target (muscle, skin receptor), forms synapse
- Maturation (months to years) - axon diameter increases, Schwann cells remyelinate, conduction velocity improves
- Distance - proximal injuries (brachial plexus, sciatic nerve) require months-years for growth cone to reach distal targets
- Age - regeneration rate declines with age (1-3mm/day in youth, slower in elderly)
- Gap distance - gaps greater than 3-5mm require nerve grafting; tension-free repair critical
- Denervation time - muscle fibers and Schwann cells atrophy if denervation exceeds 12-18 months
Advancing Tinel sign indicates regeneration front. Percussion over the nerve produces tingling distal to percussion site. The point of maximal Tinel advances 1mm per day distally, indicating growth cone progression. Stationary Tinel suggests neuroma (failed regeneration).
GAP-43: The Axonal Growth Marker
GAP-43 is named repeatedly above as one of the growth-associated genes upregulated by the injured cell body, but it merits explanation as the prototypical molecular marker of axonal regeneration.
- What it is - GAP-43 (growth-associated protein 43, also called neuromodulin or B-50) is a membrane-associated phosphoprotein highly concentrated in the growth cone and the axonal plasma membrane. Its expression is low in mature, stable neurons and is strongly upregulated by the injured cell body as it switches from a transmission phenotype to a growth phenotype.
- Function - GAP-43 regulates the actin cytoskeleton and membrane dynamics at the growth cone. It binds calmodulin and is a major substrate of protein kinase C (PKC); its phosphorylation state modulates filopodial extension, growth-cone motility and the axon's capacity to advance and form new connections. It is therefore part of the structural machinery of regeneration, not merely a passive label.
- Clinical and experimental relevance - because GAP-43 rises specifically when an axon is actively elongating, it is used experimentally as a readout of genuine regeneration and helps distinguish a regenerating neuron from one destined to atrophy. It is, in effect, the molecular counterpart of the clinically advancing Tinel sign.
GAP-43 (growth-associated protein 43) is the prototypical growth-cone phosphoprotein and regeneration marker - low in stable neurons, strongly upregulated by the injured cell body, and a PKC and calmodulin substrate that drives actin remodelling and filopodial extension at the growth cone. Its rise is the molecular signature of an axon that is actively regenerating.
Factors Affecting Nerve Regeneration
Success of nerve regeneration depends on patient, injury, and surgical factors. Understanding these allows surgeons to optimize repair technique and set realistic expectations.
Patient Factors
- Effect on Regeneration
- Younger better than older
- Mechanism
- Decreased growth factor expression, slower Schwann cell response with age
- Effect on Regeneration
- Impaired regeneration
- Mechanism
- Microangiopathy, neuropathy, decreased neurotrophic support
- Effect on Regeneration
- Delayed regeneration
- Mechanism
- Vasoconstriction, tissue hypoxia, impaired Schwann cell function
- Effect on Regeneration
- Protein and B vitamins essential
- Mechanism
- Axonal protein synthesis requires amino acids, B vitamins for myelin
- Effect on Regeneration
- Cancer, renal failure, immunosuppression
- Mechanism
- Impaired cellular metabolism, healing, growth factor signaling
Age is the most important patient factor. Children regenerate faster and achieve better functional outcomes than adults. Elderly patients have slower regeneration and poorer outcomes even with optimal repair.
These patient factors are mostly non-modifiable, emphasizing importance of technique.
Critical surgical windows: Motor reinnervation must occur within 18-24 months or motor endplates degenerate. Sensory recovery can occur even after years but is less functional. This is why proximal nerve injuries in adults have poor prognosis - regeneration distance too great to reach muscle in time.
Investigations
Electrodiagnostic Studies
- Neurapraxia
- Normal
- Axonotmesis/Neurotmesis
- Reduced or absent
- Timing
- Wait 7-10 days for Wallerian degeneration
- Neurapraxia
- Normal
- Axonotmesis/Neurotmesis
- Reduced or absent
- Timing
- Wait 10-14 days for sensory axon degeneration
- Neurapraxia
- Present
- Axonotmesis/Neurotmesis
- May be present early
- Timing
- Perform across lesion stimulation
- Neurapraxia
- May be slowed at injury site
- Axonotmesis/Neurotmesis
- Cannot measure if absent response
- Timing
- Focal slowing suggests demyelination
Timing: Wait 3-4 weeks post-injury
Denervation potentials:
- Fibrillation potentials (spontaneous)
- Positive sharp waves
- Present in axonotmesis/neurotmesis
- Absent in neurapraxia
Motor unit changes:
- Reduced recruitment initially
- Large polyphasic units with reinnervation
Differentiate injury types:
- Neurapraxia: Normal NCS distal, conduction block at lesion
- Axonal injury: Absent/reduced distal responses
Prognosis and timing:
- Baseline at 3-4 weeks
- Follow-up at 3-month intervals
- Nascent units indicate reinnervation
Wallerian degeneration takes 7-14 days to complete.
- Before this, NCS may still show normal distal responses even with complete transection
- Denervation potentials (fibrillations) appear at 2-3 weeks as muscle becomes hypersensitive
- Early EMG may miss axonal injury and lead to incorrect neurapraxia diagnosis
- Exception: Intraoperative nerve action potential (NAP) testing during surgery

Management
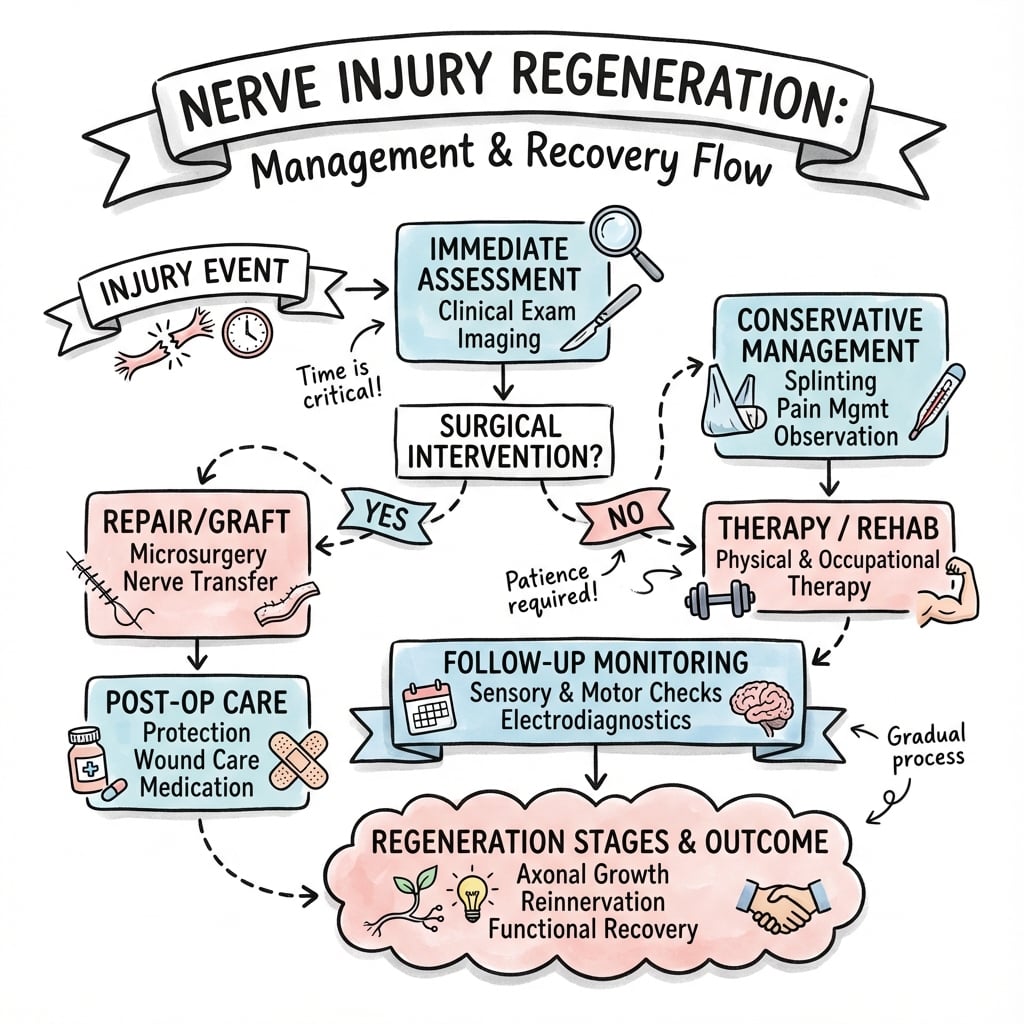
Management Overview
- Initial Management
- Observe, splinting, physiotherapy
- Surgical Indication
- None (spontaneous recovery)
- Expected Outcome
- Complete recovery in weeks to months
- Initial Management
- Observe 3 months, serial EMG
- Surgical Indication
- Surgery if no recovery by 3-4 months
- Expected Outcome
- Good recovery if endoneurium intact
- Initial Management
- Urgent exploration and primary repair
- Surgical Indication
- Immediate surgical repair
- Expected Outcome
- Variable, depends on level and timing
- Initial Management
- Delayed exploration after wound healing
- Surgical Indication
- Secondary repair 2-6 weeks
- Expected Outcome
- Worse than sharp injury
Neurapraxia and closed axonotmesis:
- Splinting to prevent contractures
- Physiotherapy for joint mobility
- Serial clinical examination (Tinel sign)
- EMG at 3-4 weeks baseline, 3 months follow-up
Observation period:
- Advancing Tinel sign indicates recovery
- Nascent motor unit potentials on EMG
- Clinical recovery appropriate for regeneration distance
Absolute indications:
- Open injury with nerve discontinuity
- Progressive neurological deficit
- Associated vascular injury requiring exploration
Relative indications:
- No clinical/EMG recovery by 3-4 months
- Stationary Tinel sign
- Neuroma-in-continuity on imaging
Why wait 3 months for closed nerve injuries?
- Allows time for neurapraxia to recover (demyelination resolves)
- Allows axonotmesis to show regeneration signs (advancing Tinel)
- EMG can document nascent units indicating reinnervation
- Beyond 3 months, delays compromise outcomes due to Schwann cell band deterioration
- Exception: Open injuries with known transection - repair immediately
Surgical Technique
Primary Nerve Repair (Neurorrhaphy)
- Description
- Sutures through epineurium only
- Indications
- Most common, mixed nerves
- Advantages
- Simple, minimal intraneural trauma
- Description
- Sutures through perineurium of fascicle groups
- Indications
- Large nerves with distinct groups
- Advantages
- Better alignment, more precise
- Description
- Individual fascicle coaptation
- Indications
- Pure motor/sensory nerves
- Advantages
- Most precise but most trauma
Key steps:
- Adequate exposure with proximal and distal mobilization
- Identify healthy nerve tissue (bulb resection)
- Align fascicular patterns (vessels, epineurial landmarks)
- Tension-free coaptation
- Minimal sutures (4-6 for digital, 8-12 for major nerve)
Instruments: Operating microscope or loupes, microsurgical instruments, 8-0 to 10-0 nylon
Ensure success:
- Rotate nerve to inspect entire circumference
- Match surface blood vessels for orientation
- Place sutures 1-2mm apart
- Avoid crushing nerve with forceps
- Fibrin glue can supplement suture repair
Positioning: 90 degrees coaptation, slight flexion of adjacent joints if needed
Epineurial repair is preferred for most injuries:
- Less intraneural dissection trauma
- Faster surgery
- Similar outcomes in mixed nerves
Fascicular repair reserved for:
- Pure motor nerves (anterior interosseous)
- Large nerves with distinct motor/sensory groups (median at wrist)
- Need to match specific fascicles
Complications
Complications of Nerve Injury
- Cause
- Misdirected axonal sprouting
- Prevention
- Tension-free repair, good fascicular alignment
- Treatment
- Neuroma resection and grafting
- Cause
- Late repair, poor technique, elderly
- Prevention
- Early repair, microsurgical technique
- Treatment
- Nerve transfer, tendon transfer
- Cause
- Motor axons entering sensory fascicles
- Prevention
- Fascicular matching, intraoperative NAP
- Treatment
- Often irreversible, consider tendon transfer
- Cause
- Prolonged immobilization, muscle imbalance
- Prevention
- Splinting, physiotherapy during recovery
- Treatment
- Tendon lengthening, capsular release
Painful neuroma:
- Disordered axonal sprouting at injury site
- Tapping causes severe lancinating pain
- Forms at amputation stumps, failed repairs
Prevention:
- Tension-free repair
- Cover nerve ends in vascularized tissue
- Buried relocation for amputation neuromas
Complex regional pain syndrome (CRPS):
- Can follow any nerve injury
- Burning pain, allodynia, autonomic changes
Management:
- Early mobilization and desensitization
- Mirror therapy, TENS
- Medications: gabapentin, pregabalin, duloxetine
- Multidisciplinary pain management
Key concept: A neuroma-in-continuity may conduct or not conduct.
- Conducting neuroma: Some axons passing through, NAP positive. External neurolysis only.
- Non-conducting neuroma: Complete block, NAP absent. Resect and graft.
Never resect a conducting neuroma - will worsen outcome by destroying regenerating axons.
Postoperative Care
Postoperative Protocol
Rehabilitation Timeline After Nerve Repair
Protection phase: Splint in position of repair (slight flexion to reduce tension). No active motion across repair. Wound care and edema control.
Gentle mobilization: Gradual increase in ROM. Wean from splint during day. Continue night splint. Begin scar management.
Progressive motion: Full ROM as tolerated. Strengthening begins when reinnervation evident. Sensory re-education starts when protective sensation returns.
Reinnervation and strengthening: Motor recovery progresses. Strengthening intensifies. Functional training for activities of daily living.
Purpose:
- Protect repair from tension
- Prevent joint contracture
- Position hand of function
Duration:
- Rigid splint: 3 weeks
- Removable splint: 3-6 weeks
- Night splint: Until reinnervation
Early phase (0-6 weeks):
- Edema control
- Scar management
- Passive ROM of uninvolved joints
- Desensitization if hypersensitive
Later phase (6+ weeks):
- Active ROM
- Strengthening when motor returns
- Sensory re-education
Why sensory re-education is necessary:
- Regenerating axons may reach different receptors than original
- Cortical representation must reorganize
- Begin when protective sensation returns (4.31 monofilament)
- Techniques: texture identification, localization training
Without re-education, sensory recovery is suboptimal even with good regeneration.
Outcomes
Motor Recovery Grading
- Description
- No contraction
- Clinical Significance
- Complete denervation
- Description
- Flicker of contraction
- Clinical Significance
- Early reinnervation beginning
- Description
- Contraction with gravity eliminated
- Clinical Significance
- Reinnervation progressing
- Description
- Contraction against gravity
- Clinical Significance
- Useful recovery achieved
- Description
- Contraction against resistance
- Clinical Significance
- Good recovery
- Description
- Normal power
- Clinical Significance
- Excellent recovery (uncommon after repair)
Sensory Recovery Grading
- Description
- No sensation
- Functional Implication
- Complete sensory loss
- Description
- Deep pain only
- Functional Implication
- Minimal protective sensation
- Description
- Some superficial pain and touch
- Functional Implication
- Protective sensation developing
- Description
- Touch and pain, no overreaction
- Functional Implication
- Functional protective sensation
- Description
- Good localization, some 2PD
- Functional Implication
- Useful discriminative function
- Description
- Normal two-point discrimination
- Functional Implication
- Rare after repair
Distal injuries (wrist, hand):
- Motor: M4-M5 achievable
- Sensory: S3+ common
Proximal injuries (arm, plexus):
- Motor: M3-M4 typical
- Sensory: S3 often best achieved
- Intrinsic muscle recovery rare
Better outcomes:
- Young age (children best)
- Distal injury level
- Sharp mechanism
- Early repair (under 3 months)
- Pure sensory or motor nerve
Worse outcomes:
- Elderly
- Proximal injury
- Crush/avulsion
- Delayed repair
- Mixed nerve (misdirection)
What to tell patients:
- Motor recovery: Expect M3-M4 (useful but not normal strength)
- Sensory recovery: Expect protective sensation, discriminative function limited
- Cold intolerance: Common and often permanent
- Time to recovery: 12-24 months depending on level
- Full normal function: Uncommon after nerve repair
Clinical Relevance
Understanding nerve injury biology directly informs clinical decision-making in diagnosis, prognosis, and treatment.
Diagnosis and Classification
- Neurapraxia
- Weakness without atrophy
- Axonotmesis
- Weakness with progressive atrophy
- Neurotmesis
- Complete paralysis with rapid atrophy
- Neurapraxia
- Patchy, incomplete
- Axonotmesis
- Complete in distribution
- Neurotmesis
- Complete in distribution
- Neurapraxia
- No denervation potentials
- Axonotmesis
- Denervation potentials
- Neurotmesis
- Denervation potentials
- Neurapraxia
- Conduction block at injury site
- Axonotmesis
- Absent distal to injury
- Neurotmesis
- Absent distal to injury
- Neurapraxia
- Stationary at injury site
- Axonotmesis
- Advancing 1mm per day
- Neurotmesis
- Stationary (neuroma) without repair
Electrodiagnostic testing at 3-4 weeks distinguishes neurapraxia (no denervation, conduction block) from axonotmesis/neurotmesis (denervation potentials, absent conduction). Serial testing shows recovery in neurapraxia, advancing Tinel in axonotmesis, or no recovery in neurotmesis.
Differential Diagnosis of Acute Focal Limb Weakness and Sensory Loss
- Distinguishing Features
- Deficit maps to a single peripheral nerve territory; history of trauma, laceration or fracture
- Key Investigation
- Nerve conduction studies / EMG at 3-4 weeks; ultrasound or MR neurography
- Discriminator
- Loss confined to one named nerve distribution
- Distinguishing Features
- Dermatomal/myotomal pattern crossing several peripheral nerves; neck or back pain, positive root tension signs
- Key Investigation
- MRI spine; EMG showing paraspinal denervation
- Discriminator
- Paraspinal muscle involvement and dermatomal (not peripheral-nerve) pattern
- Distinguishing Features
- Multi-nerve, multi-root deficit in one limb; possible Horner sign or pseudomeningocele in avulsion
- Key Investigation
- CT myelography / MRI; EMG mapping
- Discriminator
- Deficit too widespread for a single nerve but limited to one limb
- Distinguishing Features
- Pain out of proportion, tense compartment, pain on passive stretch; deficit not confined to one nerve
- Key Investigation
- Compartment pressures; urgent clinical diagnosis
- Discriminator
- Pain and tense swelling precede and exceed neurological signs
- Distinguishing Features
- Insidious onset, no acute trauma, positional symptoms (e.g. carpal/cubital tunnel)
- Key Investigation
- NCS localising focal slowing/conduction block
- Discriminator
- Chronic course and focal slowing without axonal transection
- Distinguishing Features
- Upper motor neuron signs (hyperreflexia, spasticity, Babinski); deficit not in a peripheral nerve pattern
- Key Investigation
- Brain/spine imaging
- Discriminator
- Upper motor neuron signs and non-peripheral distribution
- Distinguishing Features
- Inconsistent examination, give-way weakness, non-anatomical sensory loss
- Key Investigation
- Diagnosis of exclusion; normal NCS/EMG
- Discriminator
- Findings do not conform to any anatomical territory
Prognosis Estimation
Calculate expected recovery time based on injury level and regeneration rate:
Example: Median nerve laceration at wrist (12cm to thenar muscles):
- Time to reinnervation: 12cm ÷ 1mm/day equals 120 days (4 months)
- Add chromatolysis time (2-3 weeks) equals 5 months to first motor recovery
- Muscle strength improvement continues 12-18 months
Example: Brachial plexus injury at Erb point (35cm to hand intrinsics):
- Time to reinnervation: 35cm ÷ 1mm/day equals 350 days (11.5 months)
- Add chromatolysis time equals 12-13 months to first motor recovery
- Exceeds 18-24 month motor endplate viability - poor prognosis
Surgical Decision-Making
Surgical Timing Based on Biology
Immediate/delayed primary repair for clean sharp lacerations. Wound not contaminated, nerve ends fresh, minimal fibrosis. Best outcomes.
Secondary repair after wound healing in contaminated injuries. Nerve ends may need debridement. Schwann cell bands still intact and active.
Late repair still possible but outcomes declining. Schwann cell bands deteriorating. Muscle atrophy beginning. Consider nerve grafting if gap present.
Very late repair has poor motor outcomes. Schwann cells atrophied, endoneurial tubes fibrosed. Sensory recovery may still occur. Consider reconstruction (tendon transfers) instead.
Surgical technique modifications based on biology:
- Tension-free repair: Tension over 10% gap strain causes ischemia, fibrosis, failure - use nerve grafting
- Fascicular matching: Align motor and sensory fascicles to prevent misdirection in mixed nerves
- Minimal debridement: Preserve maximal endoneurial tubes for bands of Büngner guidance
- Primary neurorrhaphy vs grafting: Direct repair if gap under 3cm, grafting if larger (sural nerve donor)
Patient Counseling
Realistic expectations based on injury biology:
Good prognosis (likely functional recovery):
- Young patient (faster regeneration)
- Distal injury (short distance)
- Sharp laceration (minimal zone of injury)
- Early repair (within 3 months)
- Pure motor or sensory nerve (less misdirection)
Poor prognosis (limited functional recovery):
- Elderly patient (slower regeneration)
- Proximal injury (long distance, time exceeds endplate viability)
- Crush or avulsion (wide zone of injury)
- Late presentation (beyond 6 months)
- Mixed nerve (misdirection risk)
Set realistic expectations with patients. A brachial plexus injury in a 65-year-old at 9 months post-injury will not regain meaningful motor function even with perfect surgical repair. Offer reconstruction (tendon transfers, arthrodesis) instead of creating false hope.
Guidelines, Registries & Global Practice
Global Epidemiology
- Figure
- 2.8% of multiply-injured patients (200 nerve injuries in 162 of 5,777 patients)
- Source / Context
- Noble et al, Level 1 trauma centre, Canada (PMID 9680023)
- Figure
- Radial nerve
- Source / Context
- Noble et al (PMID 9680023)
- Figure
- Peroneal (common fibular) nerve
- Source / Context
- Noble et al (PMID 9680023)
- Figure
- Motor vehicle crashes (46%)
- Source / Context
- Noble et al (PMID 9680023)
- Figure
- Young, predominantly male (83%)
- Source / Context
- Noble et al (PMID 9680023)
Traumatic peripheral nerve injury is predominantly a disease of young men injured in high-energy mechanisms, with the upper limb (radial nerve) most often affected. Across health systems the dominant mechanisms vary with local injury epidemiology (road trauma, interpersonal violence with sharp lacerations, occupational injury and, in some regions, conflict-related wounds), but the biological principles of repair are universal.
Side-by-Side Guidance on Repair Principles
- Consensus Position
- Immediate/early primary repair (within days)
- Evidence Level
- Low (consistent observational data, expert consensus)
- Consensus Position
- Observe with serial clinical and electrodiagnostic review; explore if no recovery by 3-4 months
- Evidence Level
- Low-Moderate (cohort and IPD meta-analysis, PMID 16079678)
- Consensus Position
- Avoid; graft rather than repair under tension
- Evidence Level
- Low (basic-science and observational data)
- Consensus Position
- Direct repair for short gaps; autograft is the reference standard for larger gaps; conduits/allograft for short sensory gaps
- Evidence Level
- Moderate (RCTs for short-gap conduits/allograft, otherwise observational)
- Consensus Position
- Distal nerve transfer to shorten reinnervation distance
- Evidence Level
- Low-Moderate (consistent cohort outcomes)
No high-level (Grade A) guideline mandates a single timing protocol; international practice is built on consistent observational evidence and basic-science principles. The strongest quantitative evidence for timing comes from individual-patient-data meta-analysis showing recovery odds fall with each month of delay (PMID 16079678).
Basic Science Viva expectations:
- Define Seddon and Sunderland classifications
- Explain Wallerian degeneration timeline and purpose
- Describe chromatolysis and its significance
- Outline bands of Büngner formation
- State regeneration rate (1mm per day)
- Discuss factors affecting regeneration outcomes
MCQ Practice Points
Q: What is the Seddon classification of nerve injuries?
A: Three grades of increasing severity: (1) Neurapraxia: Conduction block without axonal damage, focal demyelination, complete recovery in weeks to months. (2) Axonotmesis: Axon disrupted but endoneurial tubes intact, Wallerian degeneration occurs, regeneration along intact tubes, good recovery. (3) Neurotmesis: Complete nerve transection including endoneurium, no spontaneous recovery, requires surgical repair.
Q: What is the Sunderland classification and how does it relate to Seddon?
A: Five grades: Grade I = Neurapraxia (conduction block). Grade II = Axonotmesis (axon damage, endoneurium intact). Grade III = Endoneurium damaged, perineurium intact. Grade IV = Only epineurium intact. Grade V = Neurotmesis (complete transection). Grades III-V require surgical intervention. Sunderland provides more granular prognosis than Seddon.
Q: What is the rate of nerve regeneration and what factors influence it?
A: Regeneration rate: approximately 1mm/day (or 1 inch/month). Factors affecting regeneration: (1) Age (younger = better). (2) Level of injury (proximal = worse due to longer regeneration distance). (3) Delay to repair (earlier = better). (4) Type of injury (sharp transection better than crush/avulsion). (5) Gap length (tension-free repair preferred).
Q: What is Wallerian degeneration?
A: Distal to injury, the axon and myelin sheath degenerate (occurs within 48-72 hours). Schwann cells proliferate, phagocytose debris, and form Bands of Büngner (tubes guiding regenerating axons). Macrophages clear myelin debris. The cell body undergoes chromatolysis (swelling, nucleus displacement). Wallerian degeneration is prerequisite for regeneration in axonotmesis/neurotmesis.
Q: What are the indications for surgical exploration of a peripheral nerve injury?
A: (1) Sharp transection injuries: Explore and repair within 72 hours (primary repair). (2) No clinical or EMG recovery by 3-4 months: Suggests Sunderland Grade III-V injury. (3) Open fracture with nerve deficit: Early exploration. (4) Closed injury with complete deficit: Observe initially, explore if no recovery by 3 months. (5) Advancing Tinel sign not present at expected time: Suggests failed regeneration.
At a Glance
Peripheral nerve injuries are classified by Seddon (neurapraxia/axonotmesis/neurotmesis) and Sunderland (Grades I-V). Wallerian degeneration begins within 24-48 hours distal to injury—axon and myelin fragment while Schwann cells phagocytose debris and proliferate to form bands of Büngner (tubular scaffolds). Chromatolysis is the proximal cell body response (Nissl dispersion, nuclear eccentricity) peaking at 7-14 days as the neuron shifts from transmission to regeneration mode. The growth cone at the axon tip extends filopodia sensing neurotrophic gradients (NGF, BDNF), regenerating at 1mm/day (1 inch/month). Neurapraxia (myelin only) recovers spontaneously; axonotmesis (axon disrupted, endoneurium intact) can regenerate; neurotmesis (complete transection) requires surgical repair within 3 months for optimal outcomes.
SEDDONSEDDON - Nerve Injury Classification
Hook:SEDDON classification goes from minor (neurapraxia) to severe (neurotmesis)
WALLERIANWALLERIAN - Degeneration Process
Hook:WALLERIAN degeneration clears the distal stump to allow regeneration
BUNGNERBÜNGNER - Schwann Cell Bands
Hook:BUNGNER bands are Schwann cell tubes that guide and support regenerating axons
Basic Science Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner asks: Describe the process of Wallerian degeneration. What is its purpose and what is the timeline?”
“The examiner shows you a diagram and asks: Compare the Seddon and Sunderland nerve injury classifications. Which do you prefer clinically and why?”
“A patient presents with a radial nerve laceration at the spiral groove from a humeral fracture 8 months ago. The nerve was not repaired. What are the chances of motor recovery if you repair it now? What biological factors limit recovery?”
Seddon Classification
- Neurapraxia: myelin injury only, axon intact, full recovery weeks-months, no Wallerian degeneration
- Axonotmesis: axon disrupted, endoneurium intact, Wallerian degeneration distal, regenerates 1mm/day, good prognosis
- Neurotmesis: complete transection all structures, requires surgical repair, poor outcomes even with repair
Sunderland Degrees
- Degree I: neurapraxia (myelin only)
- Degree II: axon disrupted, endoneurium intact (good regeneration)
- Degree III: endoneurium disrupted, perineurium intact (variable, may need surgery)
- Degree IV: perineurium disrupted, epineurium intact (poor without surgery)
- Degree V: complete transection (requires repair)
Wallerian Degeneration
- Distal axon and myelin breakdown starting 24-48 hours post-injury
- Schwann cells and macrophages phagocytose debris over 1-2 weeks
- Purpose: clear inhibitory myelin (MAG), create pro-regenerative Schwann cells
- Schwann cells form bands of Büngner (tubular scaffolds) secreting NGF, BDNF, GDNF
- c-Jun transcription factor is master regulator of Schwann cell dedifferentiation
Chromatolysis
- Cell body response to axonal injury, peaks 7-14 days
- Nissl substance disperses, nucleus eccentric, cell swells 30-50%
- Switch from neurotransmission to regeneration gene expression
- Upregulate GAP-43, tubulin, actin for growth cone extension
- Prolonged chromatolysis beyond 3-4 weeks without regeneration leads to neuronal apoptosis
Growth Cone and Regeneration
- Growth cone forms at proximal axon tip within 24-72 hours
- Filopodia and lamellipodia sense chemical gradients and ECM cues
- Regeneration rate: 1-3mm per day (average 1mm/day clinically)
- Guidance: chemoattraction (NGF, BDNF), contact attraction (laminin), chemorepulsion (semaphorins)
- Tinel sign advances 1mm/day indicating regeneration front
Schwann Cell Functions
- Debris clearance: phagocytose 40-50% of myelin debris, recruit macrophages
- Bands of Büngner: form tubular guidance channels for regenerating axons
- Neurotrophic support: secrete NGF, BDNF, GDNF creating chemical gradient
- Remyelination: wrap regenerated axons (shorter internodes, thinner myelin than original)
- Time limit: bands persist 3-4 months then deteriorate if no axon contact
Factors Affecting Regeneration
- Patient: younger better, diabetes/smoking impair regeneration
- Injury: distal better than proximal, sharp better than crush, shorter better
- Timing: primary repair within 3 months optimal, motor recovery unlikely after 18-24 months denervation
- Technique: tension-free repair critical (strain under 10%), fascicular alignment for mixed nerves
- Gap management: direct repair if gap under 3cm, nerve graft if larger
Critical Timelines
- 24-48 hours: Wallerian degeneration begins
- 7-14 days: Peak chromatolysis
- 1-2 weeks: Debris clearance complete, bands of Büngner formed
- 3-4 months: Schwann cell bands begin to deteriorate without axon
- 12-18 months: Muscle atrophy becomes irreversible
- 18-24 months: Motor endplate degeneration, no recovery possible
Evidence Base
Wallerian Degeneration Mechanisms (PNS vs CNS)
- Wallerian degeneration is an active, programmed clearance of degenerating axons and myelin, not passive decay
- Rapid macrophage recruitment and Schwann cell phagocytosis in the PNS create a permissive, pro-regenerative environment
- Slow debris clearance and persistent inhibitory myelin in the CNS help explain regenerative failure centrally
The Repair Schwann Cell and Bands of Büngner
- Nerve injury reprograms Schwann cells into a dedicated repair phenotype, not simple de-differentiation
- c-Jun is the master transcriptional regulator; its absence yields a dysfunctional repair cell, neuronal death and failed recovery
- Repair cells form Büngner's bands and supply trophic and spatial cues for axonal regrowth, but the phenotype is not indefinitely sustainable
Seddon Classification of Nerve Injury (Landmark)
- Three-tier classification based on functional prognosis rather than histological detail
- Neurapraxia recovers completely; axonotmesis regenerates well through intact endoneurial tubes
- Neurotmesis requires surgical repair, with outcomes limited even after repair
Predictors of Recovery After Median/Ulnar Nerve Repair
- Younger age strongly predicts recovery (motor OR 4.3, sensory OR 27.0 for under-16 vs over-40 years)
- Each month of delay between injury and repair reduces the odds of satisfactory motor (OR 0.94/month) and sensory (OR 0.92/month) recovery
- Ulnar nerve injuries have 71% lower odds of motor recovery than median nerve injuries (OR 0.29); proximal injuries fare worse than distal
Why Delayed Repair Diminishes Functional Recovery
- Numbers of motoneurons reinnervating muscle fell exponentially with each form of chronic delay
- Chronic denervation of the distal nerve stump is a key driver of reduced regeneration, with chronic muscle denervation an additional contributor
- Enlargement of surviving motor units could not compensate for severe loss of regenerating axons through chronically denervated stumps
c-Jun Reprograms Schwann Cells into Repair Cells
- c-Jun controls trophic factor expression, adhesion molecules, formation of regeneration tracks and myelin clearance
- Schwann-cell-specific c-Jun deletion produces a dysfunctional repair cell, with striking failure of functional recovery and neuronal death
- A single glial transcription factor is sufficient and necessary to direct transdifferentiation of Schwann cells into repair cells
Translational Barriers to Human Nerve Regeneration
- Human axons must traverse far greater distances than in rodent models, leaving distal stumps and targets denervated for prolonged periods
- Chronic denervation drives distal Schwann cell atrophy, falling neurotrophic factor expression and loss of basal lamina
- Strategies to accelerate axon growth and to keep Schwann cells and target tissues receptive are the key translational priorities
Epidemiology of Peripheral Nerve Injury in Major Trauma
- Peripheral nerve injury occurred in 2.8% of multiple-trauma patients (162 patients, 200 nerve injuries)
- Motor vehicle crashes were the leading mechanism (46%); the radial nerve was the most commonly injured upper-limb nerve and the peroneal nerve the most common in the lower limb
- Surgery was required in 54% of patients and head injury co-occurred in 60%, underscoring the polytrauma context
References
Key Research Articles
-
Waller A. Experiments on the section of the glossopharyngeal and hypoglossal nerves of the frog, and observations of the alterations produced thereby in the structure of their primitive fibres. Phil Trans R Soc Lond. 1850;140:423-429. doi:10.1098/rstl.1850.0021
-
Seddon HJ. Three types of nerve injury. Brain. 1943;66(4):237-288. doi:10.1093/brain/66.4.237
-
Sunderland S. A classification of peripheral nerve injuries producing loss of function. Brain. 1951;74(4):491-516. doi:10.1093/brain/74.4.491
-
Vargas ME, Barres BA. Why is Wallerian degeneration in the CNS so slow? Annu Rev Neurosci. 2007;30:153-179. doi:10.1146/annurev.neuro.30.051606.094354
-
Jessen KR, Mirsky R. The repair Schwann cell and its function in regenerating nerves. J Physiol. 2016;594(13):3521-3531. doi:10.1113/JP270874
-
Arthur-Farraj PJ, Latouche M, Wilton DK, et al. c-Jun reprograms Schwann cells of injured nerves to generate a repair cell essential for regeneration. Neuron. 2012;75(4):633-647. doi:10.1016/j.neuron.2012.06.021
-
Gordon T, Tyreman N, Raji MA. The basis for diminished functional recovery after delayed peripheral nerve repair. J Neurosci. 2011;31(14):5325-5334. doi:10.1523/JNEUROSCI.6156-10.2011
-
Fu SY, Gordon T. The cellular and molecular basis of peripheral nerve regeneration. Mol Neurobiol. 1997;14(1-2):67-116. doi:10.1007/BF02740621
-
Rosberg HE, Carlsson KS, Höjgård S, et al. Injury to the human median and ulnar nerves in the forearm - analysis of costs for treatment and rehabilitation of 69 patients in southern Sweden. J Hand Surg Br. 2005;30(1):35-39. doi:10.1016/j.jhsb.2004.09.003
-
Brushart TM. Nerve Repair. Oxford University Press. 2011. (Comprehensive textbook on peripheral nerve biology and repair)
-
Lundborg G. A 25-year perspective of peripheral nerve surgery: evolving neuroscientific concepts and clinical significance. J Hand Surg Am. 2000;25(3):391-414. doi:10.1053/jhsu.2000.4165
-
Lee SK, Wolfe SW. Peripheral nerve injury and repair. J Am Acad Orthop Surg. 2000;8(4):243-252. doi:10.5435/00124635-200007000-00005
-
Boyd JG, Gordon T. Neurotrophic factors and their receptors in axonal regeneration and functional recovery after peripheral nerve injury. Mol Neurobiol. 2003;27(3):277-324. doi:10.1385/MN:27:3:277
-
Griffin JW, Thompson WJ. Biology and pathology of nonmyelinating Schwann cells. Glia. 2008;56(14):1518-1531. doi:10.1002/glia.20778
-
Scheib J, Höke A. Advances in peripheral nerve regeneration. Nat Rev Neurol. 2013;9(12):668-676. doi:10.1038/nrneurol.2013.227
-
Jaquet JB, Luijsterburg AJ, Kalmijn S, et al. Median, ulnar, and combined median-ulnar nerve injuries: functional outcome and return to productivity. J Trauma. 2001;51(4):687-692. doi:10.1097/00005373-200110000-00011
-
Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR). Hip, Knee & Shoulder Arthroplasty: 2024 Annual Report. Adelaide: AOA; 2024. (For context on surgical outcomes research standards)
Suggested Reading
-
Mackinnon SE, Dellon AL. Surgery of the Peripheral Nerve. Thieme Medical Publishers. 1988. (Classic text on peripheral nerve surgery)
-
Spinner RJ, Kline DG. Surgery for peripheral nerve and brachial plexus injuries or other nerve lesions. Muscle Nerve. 2000;23(5):680-695. doi:10.1002/(SICI)1097-4598(200005)23:5
-
Terenghi G. Peripheral nerve regeneration and neurotrophic factors. J Anat. 1999;194(Pt 1):1-14. doi:10.1046/j.1469-7580.1999.19410001.x