Silencing the Scream
- A neuroma is a disorganized ball of axons attempting to regenerate.
- Painful neuromas have upregulated sodium channels.
- Treatment hierarchy: Conservative to SIMPLE Excision to ADVANCED Reconstruction (RPNI/TMR).
- Simply cutting the nerve usually leads to another neuroma.
- “RPNI uses a free muscle graft as a 'decoy' target.
- “TMR transfers the nerve to a nearby motor branch.
- “Neuroma-in-continuity with intact function should NOT be resected.
CRPS vs Neuroma CRPS is a regional pain syndrome with autonomic features. A neuroma causes localized pain with a specific trigger point (Tinel's). Operating on CRPS makes it worse. Operating on a Neuroma can cure it.
The Lidocaine Test A diagnostic nerve block proximal to the neuroma MUST relieve the pain temporarily. If pain persists despite a perfect block, the cause is central (Phantom) or alternative pathology.
- Terminal Neuroma
- Nerve End (Stump)
- Neuroma-in-Continuity
- Along Nerve Course
- Terminal Neuroma
- Zero (Distally)
- Neuroma-in-Continuity
- Variable (May be intact)
- Terminal Neuroma
- Transection
- Neuroma-in-Continuity
- Crush / Stretch / Partial Cut
- Terminal Neuroma
- Excision + Reconstruction
- Neuroma-in-Continuity
- Neurolysis vs Grafting
DSTNeuroma Prevention
Hook:Don't Suffer Tension.
MWMRPNI Steps
Hook:Muscle Wrap Monitor.
TPTSigns of Neuroma
Hook:The Painful Trigger.
Overview
Neuroma: A non-neoplastic proliferation of Schwann cells and axons at the site of a nerve injury. It represents a frustrated attempt at regeneration where axons fail to find a distal target.
Neuromas form after every nerve transection. However, only a minority become painful. Pain is due to mechanical irritation and ectopic firing.
Pathophysiology
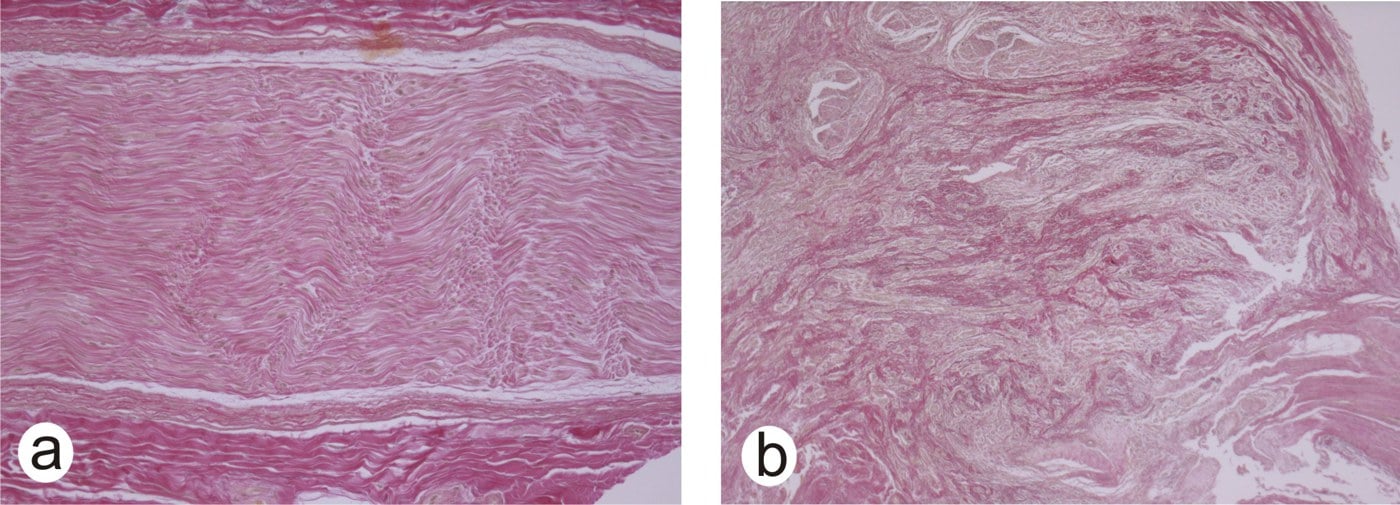
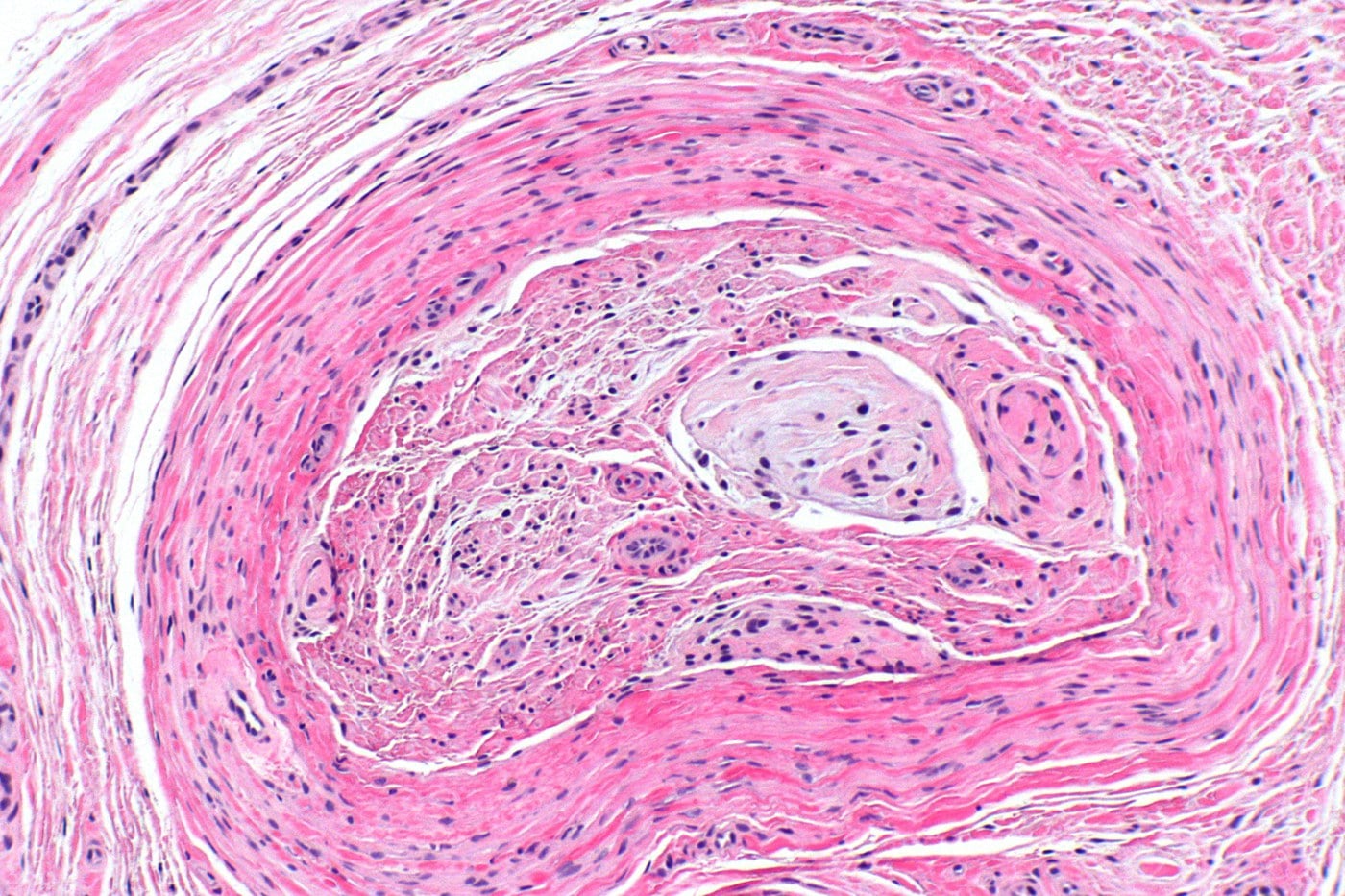
Microscopic Structure
- Axons: Disorganized, entangled sprouts (Zuckerandl's spirals).
- Stroma: Dense fibrosis and scar tissue.
- Schwann Cells: Proliferating without guidance.
The connective tissue barrier prevents axons from advancing, causing them to turn back on themselves.
The neuroma makes sense only against the normal regeneration sequence:
- After axonal disruption the distal segment undergoes Wallerian degeneration — the axon and myelin break down and are cleared by Schwann cells and macrophages over days, leaving the Schwann cells lined up as bands of Büngner that guide regrowth.
- The proximal stump sends out axonal sprouts (growth cones). If they enter a distal endoneurial tube they regenerate down it at roughly 1 mm per day (about an inch a month) — clinically tracked by an advancing Tinel's sign.
- A neuroma forms when this regeneration is "frustrated" — with no distal tube to enter (a transection or a gap), the sprouts grow chaotically into scar and produce the disorganised bulb. This is the precise rationale for RPNI and TMR: give the regenerating axons a target so they stop in an organised way rather than forming a neuroma.
- Timing matters: if denervated muscle is not reinnervated within roughly 12 to 18 months the motor end-plates degenerate irreversibly, which is why definitive nerve repair or transfer is not delayed indefinitely.
Classification
Terminal Neuroma
- End of a cut nerve. Classic "stump" neuroma.
- Pathophysiology: Unchecked sprout formation.
- Example: Amputation stump neuroma.
This is the most common type encountered in clinical practice.
A neuroma is the end result of a particular grade of nerve injury, so examiners expect the Seddon and Sunderland classifications as the substrate:
- Seddon (3 grades): neurapraxia (conduction block, axon intact, full recovery, NO Wallerian degeneration and no neuroma); axonotmesis (axon and myelin disrupted but the connective-tissue tubes intact — Wallerian degeneration then regrowth along the tubes, good recovery); neurotmesis (complete disruption including the connective tissue — no useful spontaneous recovery, the setting in which a terminal neuroma forms).
- Sunderland (5 degrees) refines this by which layer is breached: I = neurapraxia; II = axon only (endoneurium intact), recovers; III = axon + endoneurium (perineurium intact), variable recovery and can misroute into a neuroma-in-continuity; IV = axon + endoneurium + perineurium (epineurium intact), a neuroma-in-continuity with no useful recovery that needs surgery; V = complete transection (neurotmesis). (Mackinnon added a mixed grade VI.)
- This is exactly why the intra-operative nerve action potential decides a continuity lesion: a recovering Sunderland III conducts (a NAP is present → neurolysis), whereas a Sunderland IV does not (no NAP → resect and graft or transfer).
Clinical Assessment
History
- Pain: Electric shock, burning, shooting.
- Trigger: Tapping a specific spot.
- Phantom Pain: Pain felt in the missing limb (distinct from stump pain).
Examination
- Tinel's Sign: Pathognomonic. Tapping the localized spot reproduces the electric shock in the nerve distribution.
- Mobility: Is the skin tethered?
Investigations
Diagnostic Nerve Block
- Gold Standard.
- Inject Lidocaine proximal to the neuroma.
- Result: Complete relief of pain confirms peripheral generator.
- No Relief: Suggests central pain (Phantom) or wrong diagnosis.
Always use a control (saline) if psychogenic cause suspect (Placebo test).
Differential Diagnosis
The single most important examiner point is distinguishing a focal, block-responsive neuroma from diffuse or central pain that surgery will worsen. Use the response to a diagnostic block as the discriminator.
- Pain pattern
- Focal, Tinel-positive trigger point
- Block response
- Complete relief
- Key distinguishing feature
- Reproducible electric pain at one spot
- Pain pattern
- Regional, diffuse
- Block response
- Minimal / no relief
- Key distinguishing feature
- Autonomic and trophic changes, allodynia beyond one nerve
- Pain pattern
- Felt in the missing part
- Block response
- No relief of phantom component
- Key distinguishing feature
- Pain in absent limb, cortical reorganisation
- Pain pattern
- Positional, distribution of one nerve
- Block response
- Relief with proximal block
- Key distinguishing feature
- Provocative compression test, often reversible
- Pain pattern
- Mechanical, load-related
- Block response
- Variable
- Key distinguishing feature
- Linked to prosthetic fit, not a fixed trigger point
- Pain pattern
- Deep, bony, load-related
- Block response
- No relief
- Key distinguishing feature
- Visible on radiograph, palpable mass
Treatment
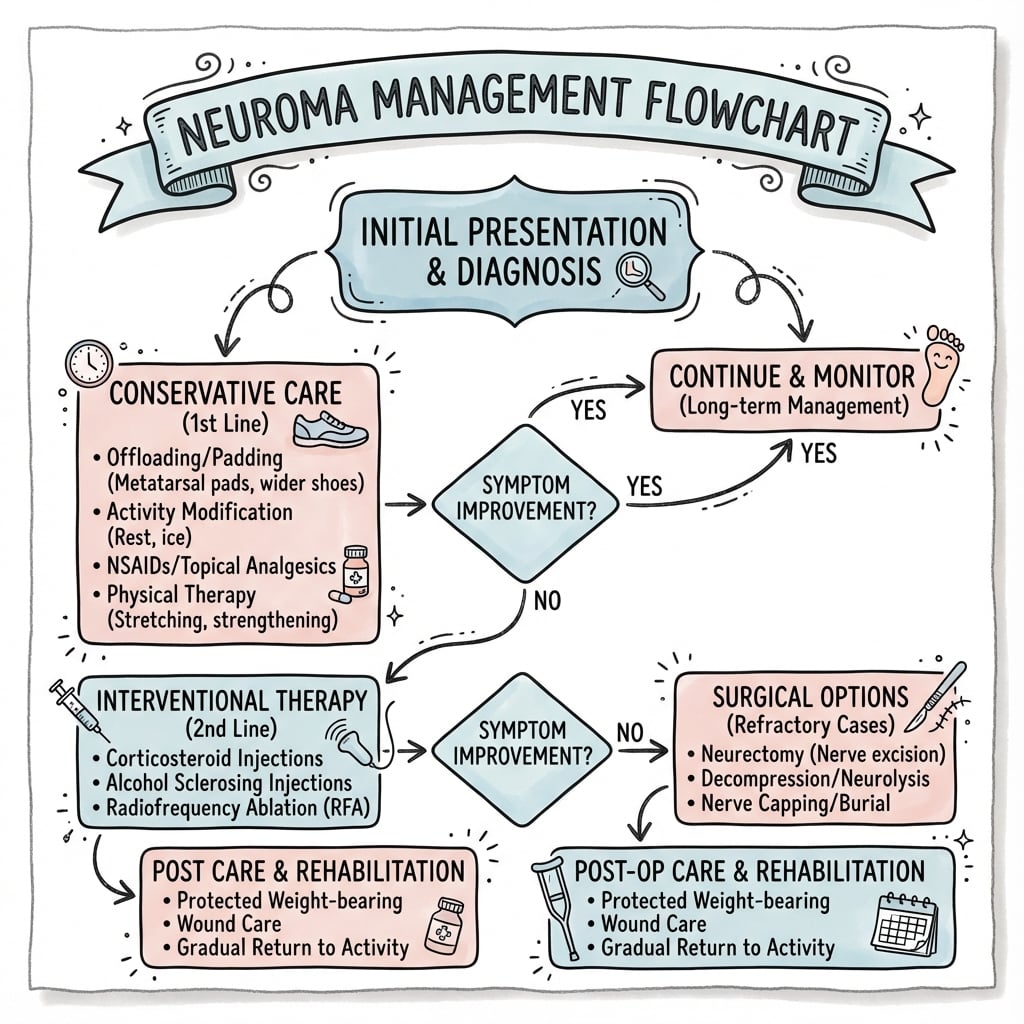
Level 1: Non-Surgical
- Desensitization: Massage, texture rubbing.
- Medication: Gabapentin, Pregabalin, Amitriptyline.
- Therapy: Mirror therapy (for Phantom pain).
Pharmacological management is the first line for neuropathic pain.
Surgical Technique
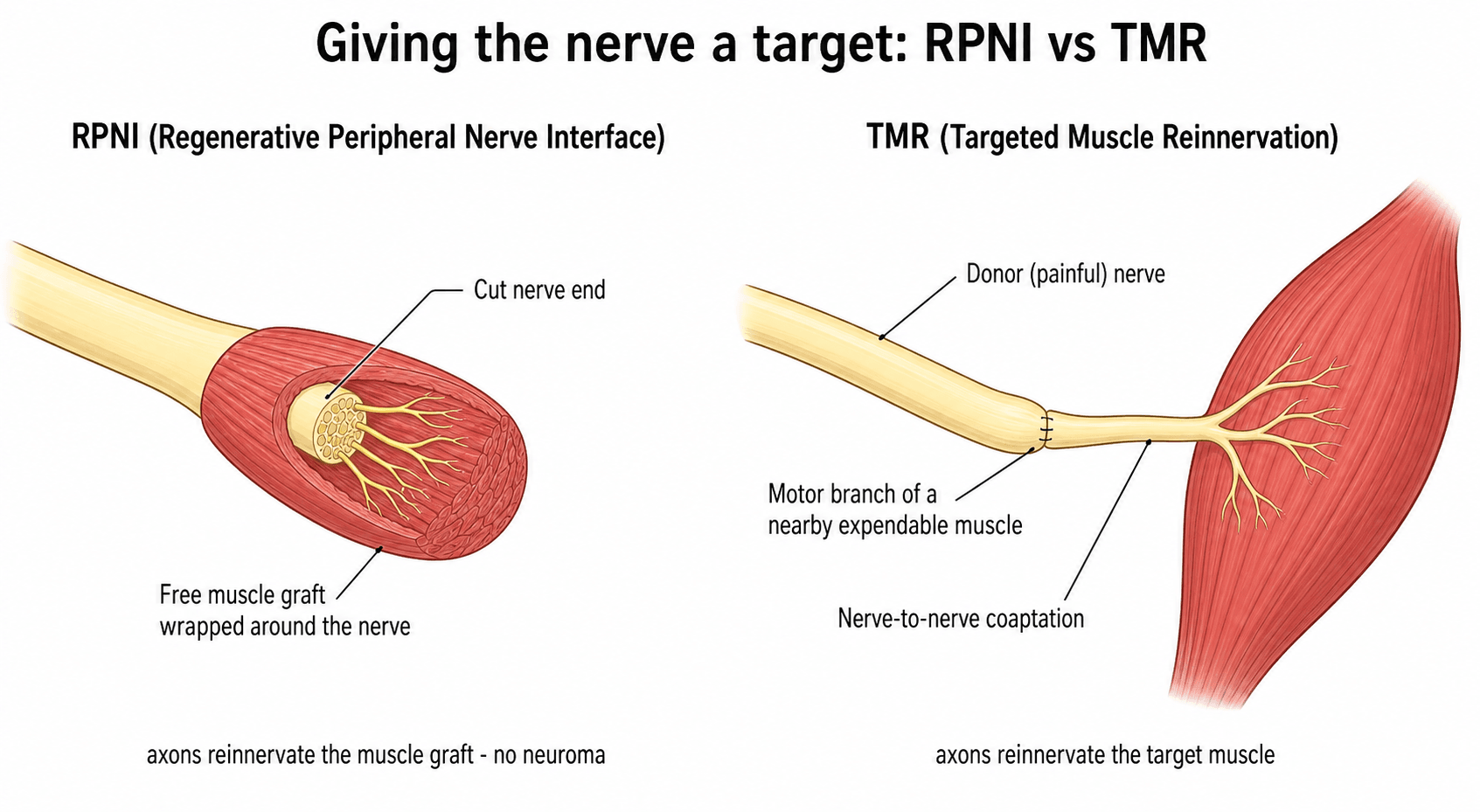
Regenerative Peripheral Nerve Interface (RPNI)
- Concept: Provide a physiologic target for the nerve end.
- Technique:
- Harvest a free muscle graft (e.g., Vastus Lateralis or local muscle). Size: 3x1.5cm.
- Neurolyse the nerve end.
- Wrap the muscle graft around the nerve end like a "Hot Dog in a Bun".
- Secure with sutures.
- Ensure the graft is well-vascularized by the recipient bed.
- Do not wrap too tightly (risk of ischemia).
- Outcome: Axons grow into the muscle graft and stop (Reinnervation).
The muscle acts as a "sponge" for regenerating axons. This prevents the formation of a chaotic neuroma bulb.
Specific Scenarios
- Very common after finger amputation or crush injury.
- Rx: Resect and bury in proximal phalanx medullary canal or into interosseous muscle.
- Care must be taken to avoid the digital artery.
- Centro-central union is an option if both digital nerves are injured.
- Dorsal branch neuromas are particularly bothersome due to thin skin.
- Notorious for painful neuromas (Wartenberg's area).
- Rx: Often requires resection and burying deep in brachioradialis or RPNI.
- Due to the thin subcutaneous tissue, superficial burial always fails.
- Consider transferring into the deep compartment of the forearm.
- "Cheiralgia Paresthetica" is the eponym for RSN compression/neuroma pain.
- Debilitating "sitting pain".
- Rx: Transgluteal approach. TMR to gluteal motor branches or burial deep in pelvis.
- Requires high exposure.
- Often mistaken for hamstring tendonitis or piriformis syndrome.
- Patient often unable to sit for more than a few minutes.
- Common after graft harvest or ankle surgery.
- Rx: Resect and bury into deep posterior compartment (Flexor Hallucis Longus).
- Avoid burying in superficial fat where shoes will rub.
Complications
Recurrence
- Rate: High with simple excision. Reduced to greater than 10 percent with RPNI/TMR.
- Cause: Nerve grows out of the burial site or forms a new neuroma at the cut end.
Recurrence is frustrating for both surgeon and patient.
Postoperative Care
- Rest: Protect the surgical repair with appropriate splinting.
- Elevation: Reduce swelling and optimize wound healing.
- Analgesia: Continue neuropathic pain medications (do not cease perioperatively).
- Start: Gentle percussion and texture stimulation once wound heals.
- Graded Motor Imagery: Especially important for phantom pain management.
- Hand Therapy: Weekly supervised sessions with home program.
- Return to function: Gradual load bearing on stump.
- Prosthetic fitting: Socket modifications may be needed post-surgery.
- Work rehabilitation: Liaise with occupational therapy for graded return-to-work planning.
Patient education is essential. Recovery from chronic neuroma pain takes months, not weeks.
Prognosis
Success Rates by Technique
- Simple Excision: Approximately 60-70% success rate. However, recurrence at the new transection site is common.
- Burial (Muscle/Bone): Approximately 70-80% success rate. Results depend heavily on the location and quality of the burial site.
- RPNI (Regenerative Peripheral Nerve Interface): Early data suggests over 90% success in reducing neuroma pain. The muscle graft provides a physiological target.
- TMR (Targeted Muscle Reinnervation): Over 90% success rate. Level II evidence from Dumanian trial supports its use.
Complete pain freedom is rare. The realistic goal is "manageable pain" allowing return to function.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Symptomatic neuromas affect an estimated 10 to 30 percent of patients after major limb amputation, and a smaller but significant proportion after digital and peripheral nerve injury.
- The dominant cause of major amputation worldwide is dysvascular disease (diabetes and peripheral arterial disease); trauma-related and combat amputations carry the highest rates of painful neuroma and phantom limb pain.
- Upper-limb and digital amputations tend to produce more functionally disabling neuromas than lower-limb levels, because of superficial nerve position and high sensory demand of the hand.
Side-by-side guideline and consensus positions:
- Position on neuroma / amputation nerve management
- Endorse active nerve handling at amputation; TMR and RPNI increasingly recommended as first-line for prevention and treatment of neuroma-related pain.
- Position on neuroma / amputation nerve management
- Emphasise multidisciplinary limb-loss pathways, diagnostic block before surgery, and targeted reconstruction over repeated simple neurectomy.
- Position on neuroma / amputation nerve management
- Teach sharp transection, tension-free handling and burial principles, with RPNI/TMR as modern target-based reconstruction.
- Position on neuroma / amputation nerve management
- Support TMR and RPNI as evidence-based options; stress patient selection and exclusion of central/CRPS pain.
There is broad agreement across societies that: (1) a diagnostic local anaesthetic block confirming a peripheral generator is mandatory, (2) simple repeated excision has unacceptable recurrence, and (3) target-based reconstruction (RPNI or TMR) is the preferred modern strategy where expertise allows.
- No dedicated international neuroma registry exists; evidence is built from single-centre and multi-institutional cohorts plus one small RCT (Dumanian 2019).
- Amputation and prosthetic registries (e.g. limb-loss and rehabilitation databases) capture amputation volume and prosthetic use but rarely code neuroma pain explicitly, which is a recognised data gap.
- Well-resourced centres: microsurgical expertise, intra-operative nerve action potential testing, RPNI/TMR, MR neurography, and multidisciplinary pain and prosthetic teams.
- Limited-resource settings: reliance on clinical Tinel and diagnostic block, sharp transection with deep muscle/bone burial, and gabapentinoid/tricyclic pharmacotherapy; advanced reconstruction may be unavailable, making meticulous primary nerve handling at amputation especially important.
- Early pain-medicine involvement, structured desensitisation and hand/limb therapy, and psychological support for chronic pain improve outcomes regardless of setting.
- Liaison with prosthetists ensures socket design accommodates surgical reconstruction and any myoelectric interface created by TMR.
Controversies & Areas of Uncertainty
Both give regenerating axons a target, but head-to-head randomised data are lacking. RPNI is technically simpler and uses a free muscle graft; TMR provides a larger motor target and intuitive myoelectric signals. Choice is currently driven by surgeon expertise, nerve calibre, and prosthetic goals rather than high-level comparative evidence.
Evidence (Valerio, Kubiak) supports treating nerves at the index amputation rather than waiting. The uncertainty is cost, added operative time, and whether every amputee benefits or only higher-risk levels.
The field rests on one small RCT and many single-centre cohorts. Heterogeneous outcome measures (NRS, PROMIS, neuroma size) limit pooling, and long-term durability beyond a few years is still being defined.
Peripheral surgery reduces afferent input and can ease phantom pain, but phantom pain is partly a central, cortical phenomenon. Surgery should never be promised as a cure for the phantom component.
MCQ Practice Points
Q: What is the defining histological feature of a neuroma? A: Disorganized proliferation of Schwann cells and axonal sprouts in a dense fibrous stroma.
Q: What clinical test best differentiates a neuroma from CRPS? A: A diagnostic nerve block provides complete relief for a neuroma but minimal/no relief for CRPS.
Q: Which muscle is commonly used for RPNI grafts? A: Vastus Lateralis (free graft) or local potentially expendable muscle.
Q: What surgical technique during amputation has been proven to reduce both phantom and residual limb pain? A: Targeted Muscle Reinnervation (TMR) - transfers nerves to motor branches, providing targets for regenerating axons.
Q: Why does simple neuroma excision often fail? A: The nerve simply grows another neuroma at the new cut end (~20-30% recurrence). Providing a physiological target (RPNI/TMR) reduces recurrence to less than 10%.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old carpenter had a amputation of the index finger at the PIPJ level 6 months ago. He complains of excruciating pain when he touches the tip. He cannot work.”
“You are performing a below-knee amputation for trauma. How do you manage the nerves to prevent pain?”
“A 35-year-old woman had a wrist fracture treated with plate fixation 8 months ago. She now has severe burning pain over the radial aspect of the wrist and thumb base. She cannot tolerate her watchband or any pressure. Tinel's is strongly positive over the radial styloid area.”
Principles
- Nerves need a target (or they form neuromas)
- Pain = Mechanical + Ectopic firing
- Diagnostic Block is mandatory before surgery
- Tinel's sign over neuroma = Positive diagnosis
- ALL stumps form neuromas, only some are painful
Techniques
- Simple: Resect and Bury (Muscle/Bone)
- RPNI: Wrap with free muscle graft
- TMR: Transfer to motor branch
- Centro-central: Connect two stumps
Outcomes
- Simple excision: High recurrence (30%)
- Reconstruction (RPNI/TMR): Low recurrence (under 10%)
- TMR now gold standard for major amputation
- RPNI: Newer, promising for minor neuromas
- Centro-central: Requires second nerve stump
Evidence Base
Every card below is anchored to a verified PubMed record. Read the DOI before quoting a figure: the literature is dominated by single-centre cohorts, with one small randomised trial (Dumanian) defining the modern standard.
TMR vs Standard Neurectomy (first surgical RCT)
- Prospective single-blind RCT, 28 major-limb amputees with chronic pain, TMR vs neuroma excision and intramuscular burial
- Longitudinal mixed-model change in phantom limb pain favoured TMR (mean difference 3.5 on NRS, P equals 0.03)
- Residual limb pain trended toward TMR (P equals 0.10); 3 crossover patients also improved after TMR
Preemptive TMR at the Time of Amputation
- Multi-institutional cohort, 51 immediate-TMR amputees vs 438 unselected amputee controls
- Median worst pain over 24 hours was 1 of 10 (TMR) vs 5 (phantom) and 4 (residual) of 10 in controls
- TMR carried roughly 3 to 4 times higher odds of reduced pain severity across all PROMIS domains
TMR Prospective Cohort (CORR)
- Prospective study of 33 major-limb amputees undergoing TMR for established pain
- Residual limb pain fell from 6.4 to 3.6 and phantom limb pain from 6.0 to 3.6 on NRS at 1 year (both P less than 0.001)
- OPUS and Neuro-QOL functional scores also improved significantly
RPNI for Postamputation Neuroma (pilot)
- First clinical series: 46 RPNIs implanted in 16 amputees for symptomatic neuromas
- Patients reported a 71 percent reduction in neuroma pain and a 53 percent reduction in phantom pain
- High satisfaction (94 percent would do it again); complications limited to delayed healing and one new-site neuroma
Prophylactic RPNI Prevents Neuroma
- Case-control study, 45 amputees with prophylactic RPNI vs 45 controls
- Symptomatic neuromas: 0 percent (RPNI) vs 13.3 percent (controls), P equals 0.026
- Phantom limb pain: 51.1 percent (RPNI) vs 91.1 percent (controls), P less than 0.0001
RPNI Biological Basis (mechanism)
- Rat model: divided peroneal nerve neurotised a non-vascularised free muscle transfer (extensor digitorum longus)
- Free muscle grafts revascularised and reinnervated, with axonal sprouting and synaptogenesis confirmed histologically
- Construct remained viable and transduced compound muscle action potentials over 7 months
Surgical Treatment of Painful Neuroma (principles)
- Diagnostic local anaesthetic block confirming a peripheral pain generator is mandatory before any neuroma surgery
- Simple traction neurectomy and re-burial have high recurrence; targeted reconstruction (RPNI/TMR) is preferred where feasible
- Centralised/CRPS pain and incomplete block relief predict surgical failure