Protecting the Most Vulnerable
- Non-Mobile Infants: Any fracture in a non-mobile infant warrants investigation.
- Metaphyseal Corner Fractures: Highly specific (bucket-handle/corner fractures).
- Multiple Fractures: Different healing stages = repeated trauma.
- Rib Fractures: Posterior rib fractures are highly suspicious.
- Mandatory Reporting: Legal obligation to report suspected NAI.
- “Know the high-specificity fracture patterns
- “Any fracture in non-mobile infant = suspect NAI
- “Skeletal survey is essential
- “Document meticulously
In most jurisdictions worldwide, clinicians have a legal duty (mandatory reporting) or a strong professional duty to report suspected child abuse.
- You do not need to prove abuse - a reasonable suspicion is the threshold for referral.
- Refer to the local child protection / safeguarding service or social work team and the child protection paediatric lead; involve police where there is risk of immediate harm.
- Failure to act on a reasonable suspicion can carry professional and (where mandatory reporting applies) legal consequences.
- Document all findings meticulously and contemporaneously - your notes may be used in court.
- Fracture Patterns
- Metaphyseal corner (bucket-handle), Posterior rib, Scapula, Spinous process, Sternum
- Clinical Context
- Pathognomonic for abuse
- Fracture Patterns
- Multiple fractures at different stages, Bilateral fractures, Complex skull
- Clinical Context
- Raise strong suspicion
- Fracture Patterns
- Clavicle, Long bone shaft, Linear skull, Subperiosteal
- Clinical Context
- Common in accidental trauma too
NAIRed Flags for NAI
Hook:DIME - Delay, Inconsistent, Multiple, Explanation absent.
Overview/Epidemiology
Non-Accidental Injury (NAI) is physical abuse of a child, often by a caregiver.
- Epidemiology:
- Peak age: under 2 years (especially under 1 year).
- Boys slightly more affected.
- Mortality: 10-30% in severe cases (shaken baby syndrome).
- Risk Factors:
- Young, single parents.
- Substance abuse, mental health issues.
- Previous history of NAI in family.
- Colicky or difficult child.
- Low socioeconomic status (although occurs in all groups).
- Importance for Orthopaedic Surgeons:
- Fractures are the second most common manifestation of NAI (after bruising).
- Early recognition can save lives.
Pathophysiology & Pathomechanics
Mechanisms of Injury in NAI
- Shaking: Causes subdural hematoma, retinal hemorrhages. In infants, the head is large and the neck muscles are weak.
- Gripping/Squeezing: Causes posterior rib fractures (thumbs on spine, fingers on ribs).
- Twisting/Pulling: Causes metaphyseal corner fractures (avulsion at the chondro-osseous junction).
- Direct Blows: Long bone shaft fractures, skull fractures.
Why Metaphyseal Corner Fractures are Specific
- The metaphysis is weaker than the shaft.
- Twisting or pulling forces cause avulsion at the periosteal-bone junction.
- This mechanism rarely occurs in accidental falls.

Classification Systems
Fracture Specificity Classification
HIGH SPECIFICITY (Pathognomonic for NAI):
- Metaphyseal corner fractures (bucket-handle)
- Posterior rib fractures
- Scapula fractures
- Spinous process fractures
- Sternum fractures
These fractures are virtually never seen in accidental trauma.
Clinical Assessment
- Delayed Presentation: Caregivers wait before seeking help.
- Inconsistent History: Explanation doesn't match injury severity or pattern.
- Changing Story: Different versions from different caregivers.
- No History: "I don't know how it happened."
- Inappropriate Affect: Caregiver not appropriately concerned.
- Full Body Inspection: Look for bruises (especially non-accidental patterns like grip marks, loop marks, bite marks).
- Bruises in Non-Mobile Infants: Any bruise in a non-mobile infant is suspicious.
- Skeletal Tenderness: Palpate all limbs and axial skeleton.
- Head Circumference: Increasing head size may indicate subdural hematoma.
- Fontanelle: Bulging fontanelle is concerning.
Recognising the Abusive Bruise: Sentinel Injuries & TEN-4-FACESp
A fracture is rarely the first abusive injury - it is often the one that finally reaches an orthopaedic surgeon. The topic notes that any bruise in a non-mobile infant is suspicious; this section develops why, and gives the two clinical rules that turn that instinct into a defensible referral.
The sentinel injury. A sentinel injury is a minor but unexplained injury - most often a bruise, but also an intra-oral injury or a frenulum tear - in a young, pre-mobile infant, noticed by a caregiver or clinician before a later, more serious abusive event. These are the missed early warnings: in a case-control study, a prior sentinel injury was reported in a substantial minority of infants with definite abuse but in none of the non-abused controls, the lesion was a bruise in the large majority, most occurred before three months of age, and a medical provider had often been aware of the injury at the time without acting on it. The lesson is that a "trivial" bruise in a very young infant is a chance to intervene before the fracture or the head injury - not a finding to dismiss.
"Those who don't cruise rarely bruise." Accidental bruising tracks motor development. Independently mobile (cruising/walking) toddlers bruise over bony prominences - shins, knees, forehead - from everyday falls. Bruising in an infant who cannot yet cruise has no innocent mechanical explanation and must be explained or referred. Bruises over soft, protected, non-bony sites (the trunk, ear, neck, cheeks, eyelids, genitalia) are the abusive pattern at any age.
The TEN-4-FACESp clinical decision rule operationalises this for bruising in children under four years and infants. It flags bruising as high-concern when it involves any of these regions or features:
- Region / feature
- Chest, abdomen, back, flank, buttocks, genitourinary region
- Why it matters
- Soft protected sites do not bruise from ordinary falls
- Region / feature
- Pinna and around the ear
- Why it matters
- Almost never injured accidentally; a 'boxing' or pinch site
- Region / feature
- Anterior or posterior neck
- Why it matters
- Implies grabbing, choking or smothering
- Region / feature
- Bruising anywhere in a child under 4 years; ANY bruise in an infant under ~4-5 months
- Why it matters
- The pre-mobile infant who should not have bruises at all
- Region / feature
- Torn frenulum (forced feeding), jaw angle, fleshy cheeks, eyelids, subconjunctival haemorrhage
- Why it matters
- Facial soft tissues that are not struck in everyday play
- Region / feature
- Hand/slap marks, loop or linear ligature marks, bite marks, grip/pinch marks
- Why it matters
- The shape itself encodes the mechanism
Applied to bruising in young children the rule is highly sensitive and reasonably specific for abusive injury, which makes it a screening prompt to escalate - not a diagnosis. A positive TEN-4-FACESp bruise, like a sentinel injury, mandates the full safeguarding pathway and a skeletal survey; it does not on its own prove abuse, and a negative rule does not exclude it.
If asked "what would have prevented this child's femoral fracture?", the answer the examiner wants is recognition of the earlier sentinel injury. Say it explicitly: a pre-mobile infant should not have unexplained bruises ("those who don't cruise rarely bruise"), and any TEN-4-FACESp-positive bruise - Torso, Ear, Neck, under-4, Frenulum, Angle of jaw, Cheeks, Eyelids, Subconjunctivae, or patterned - triggers the same admit-protect-investigate-report pathway as a suspicious fracture.
Fracture Patterns in NAI
HIGH SPECIFICITY (When present, NAI is highly likely):
- Metaphyseal Corner Fractures (Bucket-Handle): Classic. Caused by twisting/pulling.
- Posterior Rib Fractures: Caused by squeezing (thumbs on back).
- Scapula Fractures: Very unusual in children (requires significant force).
- Spinous Process Fractures: Direct blow or hyperflexion.
- Sternum Fractures: Direct blow.
MODERATE SPECIFICITY:
- Multiple Fractures at Different Healing Stages: Indicates repeated trauma.
- Bilateral Fractures: Statistically unlikely from single accident.
- Complex Skull Fractures: Multiple fracture lines, depressed.
LOW SPECIFICITY (Common in accidental trauma):
- Clavicle Fractures: Common in birth and falls.
- Long Bone Shaft Fractures: Can be accidental or non-accidental.
- Linear Skull Fractures: Common in falls.
- Toddler's Fractures: Common accidental injury.
Investigations
- Full body X-rays (AP and lateral of all limbs, chest, abdomen, skull, spine).
- Repeat at 10-14 days if initial is negative (allows healing fractures to become visible).
- CT Head: Urgent if any neurological signs.
- MRI Brain: More sensitive for subtle injury.
- Dilated Fundoscopy: Retinal hemorrhages (especially multilayer) are highly specific for shaken baby syndrome.
- Bleeding studies (PT, APTT, platelet count) to rule out bleeding disorders.
- Metabolic bone disease screen (calcium, phosphate, ALP, vitamin D) to rule out rickets, OI.
- Meticulous notes, diagrams, photographs.
- Your documentation may be used in court.
SHEDInvestigation Checklist
Hook:SHED - Survey, Head, Eyes, Document.
Parent's Guide: Understanding Child Injury Investigations
Why is my child being investigated? When a child has an injury that doctors cannot easily explain, they have a legal and ethical duty to make sure the child is safe. This does not mean they are accusing you of anything - it means they are being thorough.
What investigations will be done?
- X-rays of the whole body (skeletal survey) to check for other injuries.
- A scan of the brain if there is any concern.
- An eye examination to look for signs of bleeding.
- Blood tests to rule out medical conditions.
What happens next? A team of doctors, social workers, and sometimes police will review the findings. Their goal is to ensure your child is safe.
What are your rights? You have the right to legal representation. Cooperating with the investigation is in your child's best interest.
Dating Fractures Radiologically in NAI
The whole reason a skeletal survey is repeated, and the reason "multiple fractures at different healing stages" is a moderate-specificity flag, is that healing fractures can be approximately aged on radiographs. The orthopaedic surgeon is repeatedly asked - in clinic, in MDT, and in court - "how old is this fracture?" The honest, defensible answer is a range, never a precise day. (The underlying biology of callus formation is developed in the fracture-healing topic; here the focus is the radiological timeline and its medico-legal limits.)
The radiographic features of healing appear in a predictable sequence, but with wide and overlapping windows that depend on the bone, the fracture type and the child's age:
- Typical window
- From the time of injury, resolving over the first 1-2 weeks
- Note
- Non-specific; the earliest and least reliable sign
- Typical window
- Earliest from about 4-7 days, usually well seen by 10-14 days
- Note
- The single most useful early dating sign; absence early is why the survey is repeated at 10-14 days
- Typical window
- Soft callus over roughly 2-3 weeks, hard callus from a few weeks
- Note
- Becomes denser and better defined as it matures
- Typical window
- From several weeks to many months
- Note
- A remodelled, well-corticated callus indicates an old injury
Key NAI-specific caveats:
- A fresh fracture has no periosteal reaction. The absence of healing means the injury is recent (broadly within the last week or so) - which is exactly why a negative initial survey is repeated at 10-14 days, when occult rib and metaphyseal fractures declare themselves with periosteal new bone.
- Classic metaphyseal lesions and rib fractures date poorly. Corner/bucket-handle metaphyseal fractures show little or no periosteal reaction and are notoriously hard to age; rib fractures are frequently invisible acutely and only become apparent as callus forms - reinforcing the value of the repeat survey and oblique rib views.
- Fractures of clearly different ages = repeated episodes. A non-healing fracture alongside a remodelling one cannot have occurred in a single event, which is the radiological basis of the "different healing stages" red flag.
- Bruises cannot be dated by colour. Despite courtroom tradition, the colour of a bruise does not reliably indicate its age; only the presence of yellow has any (weak) discriminating value, and multiple bruises of "different ages" by colour should not be presented as proof of repeated assault.
- Avoid over-precision in reports. State a defensible range and acknowledge the uncertainty; over-precise dating ("this fracture is exactly 12 days old") is a frequent and successful target for medico-legal challenge.
Never give a single number. The defensible structure is: no periosteal reaction = recent (days); periosteal new bone = roughly 1-3 weeks; mature, dense, remodelling callus = weeks to months. Then add the two caveats that win marks: metaphyseal corner fractures and rib fractures date poorly, and bruise colour does not date a bruise. This honesty about uncertainty is itself the examined competency.
MRSHigh Specificity Fractures
Hook:MRS - Metaphyseal, Ribs, Scapula/Spinous/Sternum.
Differential Diagnosis
- Discriminating Features
- Blue sclerae, dentinogenesis imperfecta, wormian bones, positive family history, low-trauma fractures, normal/osteopenic bone density
- Key Investigation
- Genetic testing (COL1A1/COL1A2); does NOT exclude coexisting abuse
- Discriminating Features
- Cupped, frayed, splayed metaphyses (not corner fractures), generalised osteopenia, risk factors for vitamin D deficiency
- Key Investigation
- Calcium, phosphate, ALP, vitamin D, PTH; wrist/knee radiographs
- Discriminating Features
- Clavicle or humeral fracture in a neonate, consistent perinatal history, healing already present at first presentation
- Key Investigation
- Birth records; timeline correlation
- Discriminating Features
- Explains bruising and intracranial haemorrhage but NOT fractures; may coexist with abuse
- Key Investigation
- FBC, PT, APTT, fibrinogen, von Willebrand screen, factor levels
- Discriminating Features
- Pathological fractures, metaphyseal lucent bands, systemic features, cytopenias
- Key Investigation
- FBC and film, blood film, marrow if indicated
- Discriminating Features
- Metaphyseal changes in malnourished/preterm or malabsorptive infants; rare
- Key Investigation
- Serum copper and caeruloplasmin
Clinical tip: Investigate mimics thoroughly, but a negative medical workup does not exclude abuse - and a confirmed medical condition (e.g. OI) does not exclude coexisting inflicted injury. Report if the clinical picture is suspicious.
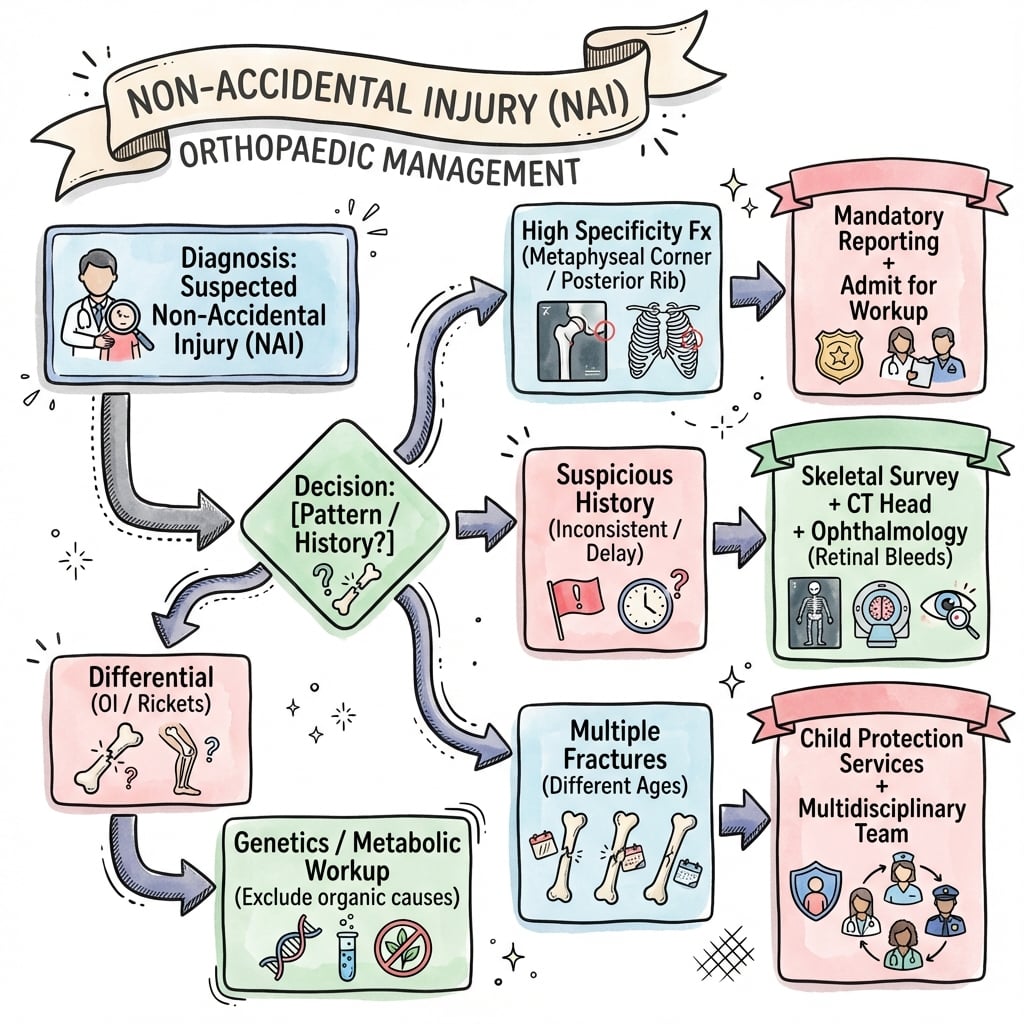
Management Algorithm
Immediate Management
- Ensure Child Safety: Do not discharge to unsafe environment.
- Admit to Hospital: For protection and investigation.
- Multidisciplinary Team (MDT): Involve pediatrician, child protection, social services.
The child's safety is the absolute priority.
Surgical Technique
Fracture Management in NAI Context:
- Priority is Child Safety: Fracture treatment is secondary to ensuring the child is protected.
- Conservative Treatment Preferred: Most NAI fractures can be treated non-operatively.
Lower Limb Fractures
- Infants (under 6 months): Pavlik harness
- Older infants/toddlers: Spica cast (immediate or delayed)
- K-wire fixation rarely needed
- Above-knee cast for most
- Conservative treatment preferred
Spica cast application is the standard treatment.
- Open fractures (rare in NAI)
- Unstable fractures requiring fixation
- Neurosurgical intervention for intracranial hemorrhage
- Always document pre-operative findings with photographs.
- Ensure child protection clearance before discharge.
- Post-operative follow-up must be coordinated with social services.
Complications
- Fracture Malunion/Nonunion: Rare with appropriate treatment.
- Growth Disturbance: Physeal injuries may cause limb length discrepancy.
- Neurological Sequelae: Brain injury from shaking can cause permanent disability.
- Visual Impairment: Retinal hemorrhages may lead to visual problems.
- Post-Traumatic Stress Disorder (PTSD): Common in abused children.
- Attachment Disorders: Difficulty forming healthy relationships.
- Developmental Delay: Physical and cognitive delays.
- Behavioral Problems: Aggression, anxiety, depression.
- Without intervention, abuse typically escalates.
- Early recognition and intervention can be life-saving.
- Children who remain in abusive environments have high mortality rates.
Postoperative Care
- Standard fracture aftercare applies (cast care, weight-bearing status).
- Follow-up imaging to confirm healing.
- Physiotherapy if indicated for stiffness or weakness.
- Do Not Discharge Without Clearance: Social services must approve discharge plan.
- Safe Placement: If home is unsafe, alternative placement must be arranged.
- Follow-Up: Coordinated between orthopaedics, pediatrics, and social services.
- Sibling Assessment: Other children in the household must also be assessed.
- Complete discharge summary with all findings.
- Clear follow-up plan documented.
- Communication with GP and community health services.
Outcomes/Prognosis
- Most fractures heal well with appropriate treatment.
- Growth disturbance is possible with physeal injuries.
- Functional outcomes are generally good if recognized early.
- With Intervention: Children removed from abusive environments have better long-term outcomes.
- Without Intervention: Mortality rate is 10-30% in severe cases; morbidity approaches 100%.
- Age at recognition (younger children more vulnerable)
- Severity of injuries (especially neurological)
- Quality of intervention and follow-up
- Availability of safe alternative placement
Early recognition by the orthopaedic surgeon can save lives. Even if uncertain, report suspected NAI - you are protected from liability when acting in good faith.
Medico-Legal Considerations
- Mandatory Reporting: Legal obligation. You are protected from liability if acting in good faith.
- Documentation: Your notes may be subpoenaed. Be factual, objective, and comprehensive.
- Avoid Speculation: Document what you observe, not your opinion on who caused it.
- Chain of Custody: If specimens or photographs are taken, maintain proper procedures.
- Expert Witness: You may be called as a witness. Be prepared to explain findings objectively.
Role of the Orthopaedic Surgeon
- Recognition: Identify suspicious fracture patterns.
- Reporting: Notify appropriate authorities.
- Documentation: Meticulous records.
- Treatment: Treat fractures appropriately (usually conservative).
- Court Attendance: May be required as a factual or expert witness.
- Ongoing Monitoring: If child returns with new injuries, re-escalate.
Guidelines, Registries & Global Practice
Global epidemiology
- Child maltreatment is reported worldwide; physical abuse disproportionately affects infants, with the highest fracture and fatal-head-injury rates in the first year of life.
- Fractures are a common manifestation of physical abuse and are second only to bruising; up to a third of physically abused children have a fracture, and the proportion is highest in non-ambulant infants.
- Risk is increased by young/sole caregivers, parental substance misuse and mental illness, intimate-partner violence, social isolation and prematurity/disability of the child - but abuse occurs across all socioeconomic groups and no profile is diagnostic.
Side-by-side guideline comparison
- Core position on suspected physical abuse
- Skeletal survey mandatory under 2 years; standardised 2-view survey with follow-up survey at ~2 weeks; neuroimaging for occult head injury in young infants
- Core position on suspected physical abuse
- Joint imaging standards: full survey under 2 years (consider 2-5 years selectively); oblique rib views; repeat survey at 11-14 days; CT then MRI for suspected abusive head trauma
- Core position on suspected physical abuse
- "Suspect" vs "consider" framework for physical abuse; act on unexplained injury in a non-mobile child; multi-agency safeguarding referral
- Core position on suspected physical abuse
- Treat the fracture on standard paediatric principles, but recognition and safeguarding referral take precedence over operative planning
- Core position on suspected physical abuse
- Population-level prevention and a multi-sectoral response; clinical recognition feeds into child-protection systems
Practice variation: high- vs limited-resource settings
- High-resource: dedicated child-protection paediatric teams, on-site paediatric radiology, ophthalmology and forensic input, statutory multi-agency pathways.
- Limited-resource: skeletal survey may be substituted by targeted/limited radiography; ophthalmology and CT/MRI may be unavailable; reporting frameworks and social-care infrastructure vary widely. The clinical threshold for suspicion and the duty to protect the child remain the same regardless of available investigations.
- Reporting is mandatory by law in many countries (e.g. across the US, Australia, parts of Europe and Asia) and professionally expected elsewhere; clinicians must know the local pathway, but the duty to act on reasonable suspicion is universal.
Controversies & Areas of Uncertainty
- Vitamin D deficiency as a cause of fractures: A recurring courtroom argument. Subclinical vitamin D insufficiency is common and does not, by itself, produce the fracture patterns of abuse; radiographic rickets is required before metabolic bone disease can plausibly explain fractures. This remains a contested medico-legal area.
- "Temporary brittle bone disease": A proposed entity used in some defences to explain multiple infant fractures. It is not accepted as a validated diagnosis in mainstream paediatric and radiological practice and lacks a reproducible evidence base.
- The biomechanics of abusive head trauma: The relative contribution of shaking versus impact, and the specificity of the "triad" (subdural haemorrhage, retinal haemorrhage, encephalopathy), remain debated. Current consensus is that the triad raises strong suspicion but is interpreted alongside the whole clinical and radiological picture rather than as standalone proof.
- Dating of fractures and bruises: Radiological fracture dating is broad (ranges, not precise days) and bruise colour does not reliably date injury; over-precise dating in reports is a frequent source of challenge.
- Whole-skeleton imaging in older children: The yield of routine skeletal survey falls sharply after 2 years, so imaging in the 2-5 year group is selective and guideline-dependent rather than uniform.
MCQ Practice Points
Q: Which fracture pattern is MOST specific for NAI? A: Metaphyseal corner (bucket-handle) fractures.
Q: Which location of rib fracture is most specific for NAI? A: Posterior rib fractures (from squeezing).
Q: What is the single most important investigation for suspected NAI? A: Skeletal survey (full body X-rays).
Q: What is the legal obligation when NAI is suspected? A: Mandatory reporting to child protection services.
Q: What condition is most commonly confused with NAI? A: Osteogenesis Imperfecta (OI) - but NAI-specific patterns differ.
Q: What is the mechanism of metaphyseal corner fractures? A: Twisting/pulling forces cause avulsion at the chondro-osseous junction.
Self-Assessment Quiz
Additional Self-Assessment Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“6-month-old brought to ED with a swollen thigh. X-ray shows a mid-shaft femoral fracture. Parents say the baby rolled off the couch.”
“Same infant. Skeletal survey shows healing rib fractures (posterior), a healing radius fracture, and a fresh femur fracture.”
“Parents of the infant claim their child has 'brittle bone disease' (OI). How do you approach this?”
HIGH SPECIFICITY
- Metaphyseal Corner (bucket-handle)
- Posterior Ribs
- Scapula
- Spinous Process
- Sternum
RED FLAGS
- Non-Mobile Infant with fracture
- Delayed Presentation
- Inconsistent History
- Multiple Injuries different stages
INVESTIGATIONS
- Skeletal Survey (repeat at 10-14 days)
- Head CT/MRI
- Dilated Fundoscopy
- Bleeding Studies
DIFFERENTIALS
- Osteogenesis Imperfecta
- Rickets
- Birth Trauma
- Bleeding Disorders
MANAGEMENT
- Admit for Safety
- MDT Involvement
- Mandatory Report
- Meticulous Documentation
LEGAL
- Mandatory Reporting required
- Good faith = liability protection
- Notes may be subpoenaed
- Avoid speculation
Evidence Base
- 32 comparative studies; once major trauma excluded, rib fractures carried the highest probability of abuse (0.71, 95% CI 0.42-0.91)
- Probability of abuse for a humeral fracture 0.48-0.54, femoral fracture 0.28-0.43 (developmental stage a key discriminator)
- Skull fracture probability 0.30; linear fractures were the commonest skull pattern in both abuse and non-abuse
- No single fracture, in isolation, distinguishes abusive from non-abusive injury
- Histological study of 40 metaphyseal lesions from 10 abused infants at autopsy
- Fracture runs through the primary spongiosa adjacent to the chondro-osseous junction, undercutting a peripheral fragment
- Inclusion of the subperiosteal bone collar explains the radiographic corner and bucket-handle appearances described by Caffey
- 34 studies: diagnostic yield of occult fractures is significant in children under 2 years
- A repeat skeletal survey at ~2 weeks provides significant additional information on number and age of fractures
- Skeletal survey commonly misses rib fractures unless oblique rib views are added
- Of 200 definitely abused infants, 27.5% had a prior sentinel injury versus 0% of 101 non-abused controls (P less than 0.001)
- Most sentinel injuries were bruises (80%); 66% occurred before 3 months of age
- A medical provider was aware of the sentinel injury in 42% of cases yet abuse was not recognised
- Prospective study of 2,123 children under 4 years presenting with bruising across 5 children's hospitals
- Refined bruising clinical decision rule was 95.6% sensitive and 87.1% specific for abusive trauma
- High-risk regions: Torso, Ear, Neck, Frenulum, Angle of jaw, Cheeks, Eyelids, Subconjunctivae; any bruise in an infant under 5 months; or patterned bruising
- 20 studies: intraocular haemorrhage had 75% sensitivity and 94% specificity for abusive head trauma
- Bilateral, extensive, multilayered retinal haemorrhages are the most specific pattern
- Traumatic retinoschisis and perimacular folds are seen in a minority of cases but are rarely present in other conditions
- 14 studies, 1,655 children with intracranial injury (779 inflicted)
- Apnoea (PPV 93%, OR 17.1) and retinal haemorrhage (PPV 71%, OR 3.5) were most predictive of inflicted brain injury
- Gender, seizures and long-bone fractures were not discriminatory; isolated skull fracture was more associated with non-inflicted injury
- Skeletal survey is mandatory in all children under 2 years with suspected physical abuse
- Standardised survey: dedicated coned views, oblique rib views; follow-up survey at ~2 weeks
- CT/MRI head indicated in infants with neurological signs or in those under 6-12 months with suspected abuse