Cuboid Compression | Lisfranc Association | Lateral Column Shortening
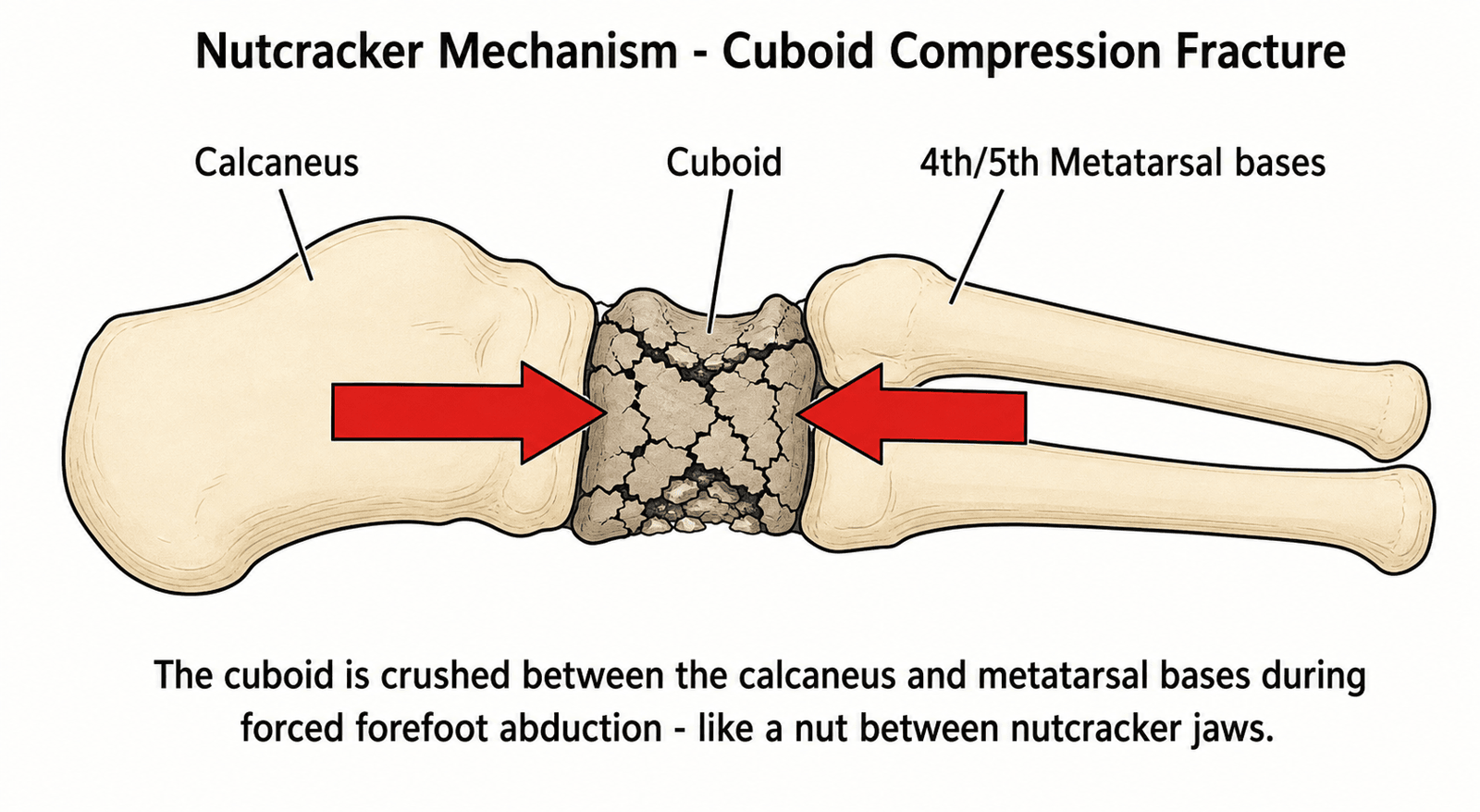
- Nutcracker fracture = cuboid compression between calcaneus and 4th/5th metatarsals during forced plantarflexion and abduction
- Often associated with Lisfranc injuries - Nutcracker fracture suggests midfoot instability, always check for Lisfranc injury
- Lateral column shortening - Compression causes impaction and bone loss, leading to lateral column shortening and midfoot collapse
- ORIF with bone graft required - Restore lateral column length with bone graft, prevent midfoot collapse
- Bone graft essential - Compression mechanism causes impaction, bone loss requires structural graft to restore length
- “Nutcracker = compression between calcaneus and metatarsals
- “Always check for Lisfranc injury
- “Bone graft essential for impaction
- “Restore lateral column length
Nutcracker fracture = cuboid compression - Compression between calcaneus and 4th/5th metatarsals during forced plantarflexion and abduction. Causes impaction and bone loss. Classic mechanism for cuboid fractures.
Nutcracker fracture suggests midfoot instability - Isolated cuboid fractures are rare; most arise within a Chopart (midtarsal) or Lisfranc injury complex. Always actively exclude associated midfoot injury — both components usually require ORIF.
Compression causes impaction and shortening - Bone loss leads to lateral column shortening and midfoot collapse. ORIF with bone graft required to restore length and prevent collapse.
Structural bone graft required - Compression mechanism causes impaction and bone loss. Autograft from calcaneus or iliac crest. Allograft acceptable. Essential to restore lateral column length.
- Impaction
- Isolated cuboid compression
- Treatment
- ORIF with bone graft
- Outcome
- 80-85% good results
- Impaction
- With Lisfranc injury
- Treatment
- ORIF both injuries
- Outcome
- 75-85% good results
- Impaction
- Severe impaction
- Treatment
- ORIF with structural graft
- Outcome
- 70-80% good results
NUTCRACKERNutcracker Fracture Features
Hook:NUTCRACKER: Nutcracker mechanism, Usually associated with Lisfranc, Tarsal cuboid compression, Compression injury, Restore lateral column, Abduction mechanism, Calcaneus compression, Keystone of lateral column, Examine for Lisfranc, Restore with ORIF and bone graft!
ALWAYSLisfranc Association
Hook:ALWAYS: Always check for Lisfranc, Lisfranc injury, With nutcracker fracture, commonly Associated, Yes check always, Surgery for both!
Overview and Epidemiology
Nutcracker fractures are compression injuries of the cuboid bone resulting from the nutcracker mechanism - compression between the calcaneus and 4th/5th metatarsals during forced plantarflexion and abduction. These fractures are often associated with Lisfranc injuries and require ORIF with bone graft to restore lateral column length.
Definition
Nutcracker fracture: Compression fracture of the cuboid bone, which:
- Mechanism: Nutcracker (compression between calcaneus and metatarsals)
- Location: Lateral midfoot (cuboid)
- Impaction: Causes bone loss and shortening
- Association: Often with Lisfranc injuries
Nutcracker mechanism:
- Compression: Between calcaneus and 4th/5th metatarsals
- Forced plantarflexion and abduction: Classic mechanism
- Impaction: Causes bone loss and lateral column shortening
- Lisfranc: Often associated with midfoot instability
Epidemiology
- Incidence: Rare — cuboid fractures account for under 1% of foot fractures, and the compression (nutcracker) subtype is rarer still
- Age: Predominantly adult trauma population; also described in children and adolescents (Fenton type 2 most common in children)
- Gender: No clear predominance
- Mechanism: Forced forefoot abduction with axial load; usually higher-energy, but low-energy and even classmate-collision injuries are reported in children
- Associated injuries: Isolated cuboid fractures are uncommon — most occur within a Chopart (midtarsal) or Lisfranc injury complex, so a high index of suspicion for associated midfoot injury is mandatory
Nutcracker fracture = cuboid compression - The cuboid is crushed between the calcaneus and the bases of the 4th/5th metatarsals when the forefoot is forced into abduction, causing impaction and lateral column shortening. Because isolated cuboid fractures are rare, always actively exclude an associated Chopart or Lisfranc injury.
Anatomy and Pathophysiology
Cuboid Anatomy
Cuboid bone:
- Location: Lateral midfoot
- Function: Keystone of lateral column
- Articulations: Calcaneus (proximal), 4th/5th metatarsals (distal), navicular (medial), lateral cuneiform (medial)
- Blood supply: Branches from dorsalis pedis and lateral plantar arteries
Lateral column:
- Components: Calcaneus, cuboid, 4th/5th metatarsals
- Function: Lateral foot stability and weight bearing
- Cuboid role: Keystone, maintains lateral column length
Nutcracker mechanism:
- Compression: Between calcaneus and 4th/5th metatarsals
- Forced plantarflexion and abduction: Classic mechanism
- Impaction: Causes bone loss and shortening
Pathophysiology
Injury mechanism:
- Forced plantarflexion and abduction: Classic mechanism
- Compression: Cuboid compressed between calcaneus and metatarsals
- Impaction: Causes bone loss and lateral column shortening
- Lisfranc association: Isolated cuboid fractures are rare — most occur within a Chopart or Lisfranc complex, so associated midfoot instability must be actively excluded
Why impaction matters:
- Bone loss: Compression causes impaction and bone loss
- Lateral column shortening: Loss of length causes midfoot collapse
- Arthritis risk: Shortening leads to lateral column arthritis
Why bone graft essential:
- Restore length: Bone graft restores lateral column length
- Prevent collapse: Prevents midfoot collapse
- Structural support: Provides structural support for articular surface
Peroneus Longus and the Peroneal Groove of the Cuboid
Every operative account of a nutcracker fracture stresses "protect the peroneal tendons," and the os peroneum appears in the differential — yet the relevant surgical anatomy is worth stating explicitly, because it is what makes the lateral approach and plantar-lateral hardware placement hazardous.
Course of the Peroneus Longus
- Retromalleolar to plantar: The peroneus (fibularis) longus tendon curves behind the lateral malleolus, passes plantar to the peroneal tubercle of the calcaneus, then turns sharply medially into a distinct groove — the peroneal sulcus — on the plantar-lateral surface of the cuboid.
- Fibro-osseous tunnel: At the cuboid the tendon runs in a fibro-osseous tunnel roofed by the long plantar ligament, before crossing the sole obliquely to insert on the base of the first metatarsal and the medial cuneiform.
- Function: It plantarflexes the first ray and everts the foot, and is an important dynamic stabiliser of the lateral column and transverse arch — the very column the nutcracker fracture shortens.
The Os Peroneum
- The os peroneum is a sesamoid within the peroneus longus tendon, lying at or just distal to the inferolateral cuboid; it is present (ossified) in a substantial minority of feet and is frequently bilateral.
- On radiographs it can be mistaken for an avulsion fracture of the cuboid — as flagged in the differential — so a smooth, corticated, often bilateral ossicle at the plantar-lateral cuboid should not be over-called as an acute fragment.
- Acute rupture of the peroneus longus can fracture or diastase the os peroneum (the "painful os peroneum syndrome"), a separate lateral-foot pathology.
Why It Matters in Nutcracker ORIF
- The lateral (longitudinal, Ollier-type) approach to the cuboid passes over or between the peroneal tendons; the peroneus longus, peroneus brevis and the sural nerve lie directly in the surgical field and must be identified, protected and retracted.
- Because the peroneal groove sits on the plantar-lateral cuboid, a plantar-lateral impaction fragment can involve the tendon's tunnel, and a prominent plantar-lateral screw or plate edge can impinge on or entrap the peroneus longus — so keep plantar-lateral hardware low-profile and screws out of the groove.
- Post-operative lateral or plantar-lateral foot pain after cuboid fixation should therefore prompt assessment of the peroneus longus, not just the healing fracture.
The peroneus longus runs in a groove on the plantar-lateral cuboid (with the os peroneum sesamoid nearby) before crossing to the first ray. In the lateral approach for cuboid ORIF, protect the peroneus longus, peroneus brevis and sural nerve; keep plantar-lateral hardware low-profile to avoid entrapping the tendon; and do not mistake a smooth, often bilateral os peroneum for an acute avulsion fracture.
Classification Systems
Pattern-Based Classification
Type I (Isolated cuboid compression):
- Isolated nutcracker fracture
- Impaction with bone loss
- Treatment: ORIF with bone graft
- Outcome: 80-85% good results
Type II (With Lisfranc injury):
- Nutcracker fracture with Lisfranc injury
- Treatment: ORIF both injuries
- Outcome: 75-85% good results
Type III (Severe impaction):
- Severe impaction with significant bone loss
- Treatment: ORIF with structural graft
- Outcome: 70-80% good results
Pattern guides treatment approach.
Clinical Assessment
History
Symptoms:
- Lateral foot pain: Pain on lateral side of foot
- Swelling: Localised to lateral midfoot
- Difficulty weight bearing: Pain with weight bearing
- Mechanism: Forced plantarflexion and abduction
Risk factors:
- High-energy trauma
- Lisfranc injury mechanism
- Midfoot instability
Physical Examination
Inspection:
- Swelling on lateral midfoot
- Ecchymosis (may be delayed)
- Deformity (lateral column shortening if displaced)
Palpation:
- Tenderness over cuboid
- Lisfranc joint tenderness (if associated)
- Lateral column instability
Range of Motion:
- Midfoot ROM limited and painful
- Inversion/eversion painful
- Plantarflexion/dorsiflexion painful
Special tests:
- Lisfranc stress test: Check for midfoot instability
- Lateral column stress: Pain with stress
- Midfoot alignment: Check for collapse
Always check for associated midfoot injury - Isolated cuboid fractures are rare, so any nutcracker fracture should prompt a careful search for an associated Chopart or Lisfranc injury. Perform a Lisfranc stress test, assess midfoot stability, and obtain CT to evaluate the whole midfoot. Routinely assess for compartment syndrome in higher-energy injuries.
Investigations
Standard X-ray Protocol
AP view:
- May show cuboid compression
- Check for Lisfranc injury
Lateral view:
- May show fracture
- Assess lateral column alignment
Oblique view:
- May show compression better
- Lisfranc joint view
Key point: CT is often needed for diagnosis and planning.
Differential Diagnosis
Lateral midfoot pain after a twisting or abduction injury has several causes. The nutcracker fracture is distinguished by cuboid impaction with lateral column shortening on imaging.
- Key Mechanism / Feature
- Forced forefoot abduction, axial load
- Discriminating Finding
- Cuboid compression with lateral column shortening on AP X-ray / CT
- Implication
- ORIF, restore length, graft impaction
- Key Mechanism / Feature
- Low-energy inversion (calcaneocuboid ligament)
- Discriminating Finding
- Small lateral fleck, no shortening, no articular step
- Implication
- Usually non-operative if under 1 mm
- Key Mechanism / Feature
- Axial load on plantarflexed foot
- Discriminating Finding
- Tarsometatarsal malalignment, fleck sign, C1-M2 diastasis
- Implication
- ORIF / fusion; commonly coexists with nutcracker
- Key Mechanism / Feature
- High-energy midtarsal force
- Discriminating Finding
- Talonavicular and/or calcaneocuboid disruption on CT
- Implication
- Urgent ORIF, restore both columns
- Key Mechanism / Feature
- Acute dorsiflexion-eversion
- Discriminating Finding
- Tenderness/clicking behind lateral malleolus, normal bone
- Implication
- Tendon-directed treatment
- Key Mechanism / Feature
- Chronic overload, painful os peroneum
- Discriminating Finding
- Sesamoid within peroneus longus, no acute trauma
- Implication
- Conservative, consider excision if refractory
Management Algorithm

Management Pathway
Nutcracker Fracture Management
CT is usually required for diagnosis - nutcracker fractures show impaction and bone loss. Assess impaction severity, associated Lisfranc injury, and lateral column shortening. Check for midfoot instability.
If isolated nutcracker fracture, ORIF with bone graft required. Restore lateral column length. Autograft from calcaneus or iliac crest. Allograft acceptable. Success rate 80-85%.
If associated with Lisfranc injury, address both injuries. Cuboid ORIF with bone graft as part of Lisfranc fixation. Restore lateral column length and midfoot stability. Success rate 75-85%.
If severe impaction with significant bone loss, structural bone graft required. Autograft from iliac crest preferred. Restore lateral column length and prevent collapse. Success rate 70-80%.
GRAFTTreatment Decision
Hook:GRAFT: Graft essential, Restore lateral column length, Anatomic reduction, Fixation with screws or plate, Treatment is ORIF!
Surgical Technique
ORIF with Bone Graft Technique
Indications:
- Nutcracker fractures with impaction
- Lateral column shortening
- Bone loss requiring restoration
Approach:
- Lateral approach to cuboid
- Expose cuboid
- Protect peroneal tendons
Technique:
- Exposure: Lateral approach to cuboid, expose fracture, protect peroneal tendons
- Debridement: Remove impacted bone fragments, assess bone loss
- Bone graft: Fill impaction defect with bone graft - autograft from calcaneus or iliac crest (preferred for structural support), allograft acceptable, structural graft if severe impaction
- Reduction: Restore lateral column length, reduce fracture anatomically
- Fixation: Screws (2.7-3.5mm) or mini-fragment plate (2.0-2.7mm)
- Verification: Confirm reduction and hardware position fluoroscopically, verify lateral column length restored (compare to contralateral)
Advantages:
- Restores lateral column length
- Prevents midfoot collapse
- Allows early motion
ORIF with bone graft restores lateral column length.
How Lateral Column Length Is Actually Restored: Disimpaction and Distraction
The whole topic turns on the instruction to "restore lateral column length," and the controversies section names "external or internal distraction" — but the mechanics of achieving that length deserve to be spelled out, because it is the step trainees most often get wrong. Impaction is a compression injury: the central articular fragment is driven inward and the column collapses. Simply lagging the fragments together reproduces the short, incongruent cuboid — length has to be actively regained and then held.
Regaining Length by Distraction (Ligamentotaxis)
- Distractor across the lateral column: A laminar spreader, a small femoral distractor, or a temporary external fixator / K-wire distractor spanning the calcaneocuboid joint (calcaneus to 4th–5th metatarsal bases) re-tensions the peripheral fragments and pulls them back out to length by ligamentotaxis.
- This restores the peripheral rim and column length, but the depressed central articular fragment usually does not follow — exactly as a depressed tibial plateau fragment will not reduce by traction alone.
Disimpaction and Elevation of the Depressed Surface
- The central impacted articular fragment is elevated en masse from below, typically through a cortical window in the lateral or dorsal cuboid, restoring articular congruity of the calcaneocuboid and cuboid–metatarsal surfaces.
- Elevating the surface leaves a subarticular metaphyseal void — the defect that mandates grafting.
Buttressing the Void and Definitive Fixation
- The void is filled with structural graft or a structural bone substitute (calcium phosphate / tricortical autograft) to physically support the elevated surface and maintain length — the graft acts as a strut, not merely a biological filler.
- Definitive fixation then holds the reconstruction: a mini-fragment plate used as a buttress, interfragmentary lag screws, or, for comminution too severe for stable internal fixation, a bridge plate spanning the calcaneocuboid joint (or retention of the spanning external fixator). Bridging constructs are removed after union.
- Distraction is maintained during fixation, and the final result is checked fluoroscopically against the contralateral foot, which is the practical reference standard for column length.
You cannot regain lateral column length with screws alone. The sequence is distract (laminar spreader / femoral distractor / calcaneocuboid-spanning fixator to pull out the periphery by ligamentotaxis), disimpact and elevate the depressed central articular fragment, buttress the void with structural graft or substitute, then fix (buttress plate, lag screws, or a CC bridge plate for severe comminution) while distraction is held — verifying length against the other foot.
Complications
- Incidence
- 15-20%
- Risk Factors
- Inadequate bone graft, severe impaction
- Prevention/Management
- Structural graft, restore length
- Incidence
- 15-20%
- Risk Factors
- Lateral column shortening
- Prevention/Management
- Restore length, adequate fixation
- Incidence
- Common
- Risk Factors
- Focus on cuboid only; injury often missed at first presentation
- Prevention/Management
- CT whole midfoot, exclude Chopart/Lisfranc
- Incidence
- 5-10%
- Risk Factors
- Inadequate fixation, bone loss
- Prevention/Management
- Rigid fixation, bone graft
Lateral Column Shortening
15-20% incidence (if untreated):
- Cause: Inadequate bone graft, severe impaction, bone loss
- Prevention: Structural bone graft, restore length, adequate fixation
- Management: Revision ORIF with structural graft if symptomatic
Midfoot Collapse
15-20% incidence (if untreated):
- Cause: Lateral column shortening, inadequate fixation
- Prevention: Restore length, adequate fixation
- Management: Revision ORIF or midfoot fusion if severe
Postoperative Care
Immediate Postoperative
- Immobilisation: Short leg cast or boot
- Weight bearing: Non-weight bearing (6-8 weeks)
- ROM: Ankle ROM after cast removal
- PT: Midfoot ROM and strengthening
Rehabilitation Protocol
Weeks 0-6:
- Short leg cast, non-weight bearing
- Elevation to reduce swelling
- Ankle ROM exercises (if stable)
Weeks 6-8:
- CT to confirm healing
- Cast removal if healing
- Transition to walking boot
- Progressive weight bearing
Weeks 8-12:
- Full weight bearing
- Progressive activity
- Return to sport (3-4 months)
Outcomes and Prognosis
Overall Outcomes
ORIF with bone graft (isolated):
- Success rate: 80-85% (union, pain relief)
- Functional outcomes: 75-80% return to pre-injury level
- Lateral column: 80-85% maintain length
ORIF with bone graft (part of Lisfranc):
- Success rate: 75-85% (union, pain relief)
- Functional outcomes: 70-75% return to pre-injury level
- Lateral column: 75-80% maintain length
ORIF with structural graft (severe impaction):
- Success rate: 70-80% (union, pain relief)
- Functional outcomes: 65-70% return to pre-injury level
- Lateral column: 70-75% maintain length
Long-Term Prognosis
Lateral column shortening progression:
- With proper treatment: 15-20% develop shortening
- Without treatment: 30-40% develop shortening
- Risk factors: Severe impaction, inadequate graft, delayed treatment
Guidelines, Registries & Global Practice
There is no dedicated arthroplasty/implant registry for cuboid fractures, and no randomised trial evidence — guidance is principle-based across societies and synthesised in critical-analysis and systematic reviews.
- Position on Cuboid / Nutcracker Fracture
- Cuboid is the keystone of the lateral column; goals are restoration of length, articular congruity and Chopart/Lisfranc stability. Disimpaction, bone-void filling and buttress fixation (lag screw, mini-fragment plate or temporary CC bridge plate) are described.
- Position on Cuboid / Nutcracker Fracture
- Non-operative care only for non-displaced articular fractures (under 1 mm) or low-energy avulsions; operate to restore congruity, length and stability. No classification validated for clinical use.
- Position on Cuboid / Nutcracker Fracture
- Apply general standards: timely senior assessment, CT for midfoot trauma, soft-tissue-led timing of fixation, compartment-syndrome vigilance in high-energy foot injuries.
- Position on Cuboid / Nutcracker Fracture
- Treat within the Chopart complex: routine CT, exclude compartment syndrome, urgent anatomic reduction maintaining column length gives best long-term outcomes.
- Cuboid fractures: under 1% of foot fractures worldwide; the compression (nutcracker) subtype is rarer still
- Reported across all regions and ages; paediatric cases described with Fenton type 2 predominating
- Evidence base is uniformly low level (case reports, small series) — no geographic registry data
- Well-resourced settings: CT and 3D planning routine; mini-fragment plating, structural graft/substitutes and staged soft-tissue care available
- Limited-resource settings: reliance on plain radiographs (risk of missed injury), K-wire fixation and provisional external fixation; bone substitutes may be unavailable, favouring autograft
- Across all settings the principle is identical: restore lateral column length and articular congruity
Nutcracker fractures are a common viva topic. Know the mechanism (cuboid crushed between calcaneus and metatarsal bases in forced forefoot abduction), that isolated fractures are rare so a Chopart/Lisfranc injury must always be excluded, that ORIF restores articular congruity and lateral column length, that bone graft fills impaction defects to prevent shortening, and that comminuted patterns may need bridge plating or external distraction. Be prepared to discuss the mechanism and why lateral column length restoration is central.
Controversies and Areas of Uncertainty
The 2020 critical analysis review (Engelmann/Rammelt/Schepers) concluded that no classification system is validated for clinical practice — none reliably guides management or predicts outcome. The Fenton system is descriptive (and was derived in part from paediatric cohorts). Treatment is principle-based (restore congruity, length, stability), not classification-driven.
Whether autograft, allograft, or synthetic/calcium-phosphate substitute best fills the impaction defect is unsettled — series report all three with acceptable results, and one paediatric series needed no graft at all. The principle (support the elevated articular surface and maintain length) matters more than the material.
Choice between lag screws, mini-fragment plates, temporary bridge plating across the calcaneocuboid joint, or external/internal distraction is individualised to comminution and soft tissues. Bridge constructs are typically removed after union; high-quality comparative data are lacking.
The widely quoted operative threshold (articular step or shortening greater than 1-2 mm) derives from small case series and expert opinion, not trials. The displacement at which non-operative care fails is not precisely defined.
Do not present fabricated percentages for "Lisfranc association" — the honest, defensible statement is that isolated cuboid fractures are rare and most occur within a Chopart or Lisfranc complex, so associated injury must be actively excluded. Evidence in this area is almost entirely Level IV/V (case reports and small series); there are no randomised trials.
MCQ Practice Points
Q: What is the nutcracker mechanism for cuboid fractures? A: Compression between calcaneus and 4th/5th metatarsals - During forced plantarflexion and abduction. Causes impaction and bone loss. Isolated cuboid fractures are rare, so a Chopart or Lisfranc injury must always be excluded.
Q: Why does a nutcracker fracture mandate a search for other midfoot injury? A: Isolated cuboid fractures are rare - The same forefoot-abduction force that crushes the cuboid commonly disrupts the Chopart (midtarsal) or Lisfranc (tarsometatarsal) joints. A nutcracker fracture therefore signals possible midfoot instability — obtain CT, exclude Chopart/Lisfranc injury, and fix all unstable components.
Q: Why is bone graft essential for nutcracker fractures? A: Compression mechanism causes impaction and bone loss - Structural bone graft required to restore lateral column length. Autograft from calcaneus or iliac crest (preferred). Prevents lateral column shortening and midfoot collapse.
Q: Why is lateral column length important in nutcracker fractures? A: Cuboid is keystone of lateral column - Loss of length causes lateral column shortening and midfoot collapse. ORIF with bone graft required to restore length. Success rate 80-85% if length restored.
Q: When is ORIF with bone graft required for nutcracker fractures? A: Impaction with bone loss or associated Lisfranc injury - Restores lateral column length and prevents midfoot collapse. Structural bone graft essential. Success rate 80-85% for isolated, 75-85% with Lisfranc.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old patient presents with lateral foot pain after forced plantarflexion and abduction injury. CT shows nutcracker fracture of cuboid with impaction and bone loss. No associated Lisfranc injury.”
“A 32-year-old patient has a nutcracker fracture as part of a Lisfranc injury. The examiner asks you to explain how you manage both injuries and why bone graft is essential.”
“A 40-year-old motorcyclist sustains a high-energy foot injury. CT shows a severely comminuted cuboid with marked articular impaction and lateral column shortening greater than 5 mm, plus a calcaneocuboid joint disruption. The skin over the lateral midfoot is swollen and blistered. The examiner asks how you would assess and manage this.”
Key Concepts
- Nutcracker mechanism = compression between calcaneus and 4th/5th metatarsals
- Isolated cuboid fractures are rare — always exclude a Chopart/Lisfranc injury
- Bone graft essential for impaction
- Restore lateral column length
Classification
- Type I: Isolated cuboid compression - ORIF with bone graft (80-85% good results)
- Type II: With Lisfranc injury - ORIF both injuries (75-85% good results)
- Type III: Severe impaction - ORIF with structural graft (70-80% good results)
- Key Factor: Impaction severity dictates graft requirement
Treatment
- Isolated: ORIF with bone graft (autograft from calcaneus or iliac crest, 80-85% good results)
- With Lisfranc: ORIF both injuries with bone graft (75-85% good results)
- Severe impaction: ORIF with structural graft (70-80% good results)
- Bone graft essential to restore lateral column length
Surgical Technique
- Lateral approach: Protect peroneal tendons
- Debride impacted bone, assess bone loss
- Bone graft: Fill impaction defect (autograft preferred, structural if severe)
- Fixation: Screws (2.7-3.5mm) or mini-fragment plate (2.0-2.7mm)
- Restore lateral column length
- Verify reduction fluoroscopically
Complications
- Lateral column shortening: 15-20% if untreated (prevent with bone graft, restore length)
- Midfoot collapse: 15-20% if untreated (prevent with adequate fixation)
- Missed associated injury: common, often missed at first presentation (prevent by CT of whole midfoot, exclude Chopart/Lisfranc)
- Nonunion: 5-10% (prevent with rigid fixation, bone graft)
Evidence Base
All evidence below has been verified against PubMed. Named reviews are cited at their stated level; primary case series carry their PubMed identifiers.
Original Description of the Nutcracker Fracture
- Coined the term 'nutcracker fracture' of the cuboid
- Mechanism: cuboid crushed between calcaneus and metatarsal bases
- Caused by indirect violence with forefoot abduction
- Foundational eponym still used in exams and practice
Cuboid Fractures: Critical Analysis Review
- Isolated cuboid fractures are rare — actively exclude Chopart/Lisfranc injury
- Cuboid is the cornerstone of the lateral column
- No validated clinical classification system exists
- Non-operative only for non-displaced (under 1 mm) or avulsion fractures
ORIF and Bone Grafting for Nutcracker Fractures
- All 6 fractures showed lateral column shortening
- Treated with ORIF plus allograft where bone loss present
- Operate if shortening or articular step greater than 1 mm
- Outcomes good in 2, fair in 4 — function often imperfect
Cuboid Nutcracker Fractures in Children: Management and Results
- Fenton classification applied; extra-articular type 2 most common (69%)
- Intra-articular involvement and midfoot disruption worsen AOFAS scores
- Paediatric remodelling means bone grafting often unnecessary
- Articular and associated injuries are the key prognostic drivers
Chopart Dislocations: Systematic Review
- 58 papers synthesised — historically poor outcomes for these injuries
- Routine CT and compartment syndrome assessment advised
- Urgent ORIF restoring column length gives best outcomes
- High rate of missed injury at first presentation
Chopart Joint Injuries — Contemporary Review
- Low incidence but high complication rate if missed or undertreated
- Combined bony and ligamentous injury requires column realignment
- Fixation construct tailored to pattern and soft-tissue envelope
- Prompt recognition and anatomic fixation predict good outcomes