The 'Grey Zone' Deformity
Severity Classification
Critical Must-Knows
- Reducibility: TN joint reduces on max plantarflexion (unlike CVT)
- Radiographic Sign: Talar axis passes plantar to 1st MT on lateral view (Meary's broken)
- Talonavicular Relationship: Dorsolateral subluxation
- Differentiation: Distinguish from Rigid CVT and Flexible Flatfoot
- Treatment: Often requires treatment if painful or progressing
Clinical Pearls
- "In the exam, demonstrate REDUCTION of the deformity on plantarflexion lateral X-ray
- "Always screen the hips and spine (neuromuscular check)
- "If it doesn't reduce, it is a Vertical Talus
- "Look for the 'sliding' navicular
The Critical Differentiator
The single most important feature to distinguish Oblique Talus from Congenital Vertical Talus (CVT) is the reducibility of the talonavicular joint. In Oblique Talus, the navicular slides back onto the talar head when the foot is plantarflexed. In CVT, the navicular is dislocated dorsally and rigidly locked, and will NOT reduce. This must be demonstrated on a forced plantarflexion lateral radiograph.
The Spectrum of Valgus Foot
| Feature | Flexible Flatfoot | Oblique Talus | Vertical Talus |
|---|---|---|---|
| Congruent | Subluxed Dorsally | Dislocated Dorsally | |
| Fully Reducible | Reduces with PF | Irreducible ( Rigid) | |
| Normal (NWB) / Sag (WB) | Broken (Extension) | Severely Broken | |
| Parallel to 1st MT | Plantar to 1st MT | Vertical orientation | |
| Valgus (Corrects with toe rise) | Fixed Valgus | Fixed Valgus (Equinus) |
SLIDEOblique Features
| S | Subluxed TN joint subluxed (not dislocated) |
| L | Laxity Associated with hypermobility |
| I | Improves Reduces on plantarflexion |
| D | Dorsal Navicular is dorsal to talus |
| E | Equinus Often present (Achilles contracture) |
| S | Subluxed TN joint subluxed (not dislocated) | D | Dorsal Navicular is dorsal to talus |
| L | Laxity Associated with hypermobility | E | Equinus Often present (Achilles contracture) |
| I | Improves Reduces on plantarflexion |
Hook:The navicular SLIDES back into place in Oblique talus.
WPDRadiographic Views
| W | Weight-bearing AP/Lat Shows deformity |
| P | Plantarflexion Lat Proves reducibility (Oblique) |
| D | Dorsiflexion Lat Shows fixed equinus (CVT) |
| W | Weight-bearing AP/Lat Shows deformity |
| P | Plantarflexion Lat Proves reducibility (Oblique) |
| D | Dorsiflexion Lat Shows fixed equinus (CVT) |
Hook:The Dynamic Stress Views are mandatory.
REDDifferentiation: RED
| R | Reducible Navicular reduces on plantarflexion (Oblique) |
| E | Equinus Less severe than CVT |
| D | Dorsal Navicular is dorsal but not dislocated |
| R | Reducible Navicular reduces on plantarflexion (Oblique) |
| E | Equinus Less severe than CVT |
| D | Dorsal Navicular is dorsal but not dislocated |
Hook:Oblique Talus is REDucible.
Overview/Epidemiology
Oblique Talus (also known as Supranavicular Subluxation) occupies the middle ground in the spectrum of congenital flatfoot deformities. It is more severe than a flexible flatfoot but less rigid than a Congenital Vertical Talus (CVT).
Definition: A condition where the talus is plantarflexed and the navicular is subluxed dorsally upon it. The key definition is that the relationship is reducible; the navicular can be brought back into alignment with the talus, usually by plantarflexion.
Associations:
- Neuromuscular Disorders:
- Cerebral Palsy: Especially spastic diplegia. The muscle imbalance (spastic peroneals/gastroc) pulls the foot into valgus.
- Spina Bifida: Muscle weakness leading to instability.
- Genetic Syndromes (Ligamentous Laxity):
- Ehlers-Danlos Syndrome: Collagen defect causing hypermobility. The spring ligament fails.
- Marfan Syndrome: Similar mechanism. arachnodactyly may be noted.
- Down Syndrome (Trisomy 21): Hypotonia and ligamentous laxity are hallmark features.
- Larsen Syndrome: Multiple joint dislocations.
- Developmental Delay: Hypotonia contributes to the "flat" appearance.
Clinical Course: Many are asymptomatic in childhood. However, because the joint is subluxed (incongruent), it is prone to progressive deformity and degenerative changes. Pain typically develops in adolescence along the medial border (talar head prominence) or sinus tarsi (impingement).
Long Term Sequelae (Untreated):
- Medial Column Collapse: Complete loss of the medial arch.
- Spring Ligament Failure: Irreversible elongation.
- Talonavicular Arthritis: Due to the incongruent joint surfaces wearing unevenly.
- Forefoot Abduction: Leading to hallux valgus (bunions).
- Functional Impairment: Inability to run or play sports without pain.
Anatomy/Biomechanics
Pathoanatomy:
- Talus: Plantarflexed attitude (more vertical than normal).
- Navicular: Subluxed dorsally and laterally. It articulates with the dorsal aspect of the talar head.
- Calcaneus: In valgus and eversion.
- Spring Ligament: Attenuated (stretched), failing to support the talar head.
- Triceps Surae: Often tight (Achilles contracture), which forces the midfoot to breach/break dorsally to achieve clearance during gait.
Biomechanics: The medial longitudinal arch is obliterated. During weight-bearing, the ground reaction force pushes the talar head further plantarward and the navicular further dorsal. Unlike a flexible flatfoot where the locking mechanism of the midfoot is intact during push-off, the Oblique Talus foot remains unlocked and unstable, leading to an inefficient gait and fatigue.
Pathophysiology
The oblique talus is a dynamic failure of the medial column in which the talonavicular (TN) joint is the weak link of the medial longitudinal arch.
Deforming sequence:
- Lax or imbalanced TN joint — generalised ligamentous laxity (hypotonia, syndromic collagen disease) or a neuromuscular muscle imbalance (spastic peroneals/gastrocnemius overpowering tibialis posterior) destabilises the joint.
- Repetitive stance-phase loading drives the talar head plantar-medially while ground reaction force pushes the navicular dorsally and laterally — a progressive dorsal subluxation rather than a fixed dislocation.
- Spring (plantar calcaneonavicular) ligament attenuation removes the static sling that supports the talar head, deepening the sag.
- Dorsal soft-tissue contracture (extensor tendons, dorsal TN capsule) plus a tight triceps surae forces the midfoot to "break" dorsally for ground clearance, perpetuating the deformity.
- Conversion along the spectrum — if the dorsal contractures become fixed, the reducible oblique talus migrates towards the rigid, irreducible congenital vertical talus.
The crucial distinction (Harris, Clin Podiatr Med Surg 2000) is that in oblique talus the TN joint is pushed to, or just past, its end range but is not truly dislocated — which is why it remains reducible and why prognosis is better than in CVT.
Classification Systems
Hamanishi Classification (1984)
This system classifies congenital vertical talus and its variants based on the reducibility of the talonavicular joint.
- Group 1 (Flexible Flatfoot):
- Resting position: Normal or Valgus.
- TN Joint: Congruent/Reduced.
- Stress Views: Stable.
- Group 2 (Oblique Talus):
- Resting position: Valgus/Plantarflexed Talus.
- TN Joint: Subluxed Dorsally.
- Stress Views: Reduces on Plantarflexion.
- Group 3 (Vertical Talus):
- Resting position: Rocker Bottom.
- TN Joint: Dislocated Dorsally.
- Stress Views: Irreducible.
- Subgroups: 3a (Less than 3 months), 3b (Older than 3 months).
Clinical Assessment
History:
- "Fail to thrive" of foot posture.
- Parents report "ankles rolling in".
- Pain/Fatigue with sport (older child).
- Shoe wear issues (medial wear).
Physical Examination:
- Standing: Severe planovalgus foot. The medial malleolus is prominent. The talar head bulges on the medial border ("double malleolus" sign).
- Tiptoe Test: The heel may go into some varus (indicating some power), but the arch often does not reconstitute fully.
- Jack's Test: Extending the big toe fails to elevate the arch (Windlass failure).
- Reduction Test: With the child seated, plantarflex the ankle and foot. Palpate the TN joint. The "hollow" dorsal to the talus disappears as the navicular slides back into place.
- Neurological Exam: Essential. Check tone, reflexes, and gait for mild CP or spina bifida. Assess Beighton score for hyperlaxity.
Gait Analysis:
- Stance Phase: Increased medial foot contact. The "arch" is absent.
- Heel Rise: Watch for the calcaneus to invert (varus). In Oblique Talus/Flexible Flatfoot, the heel should invert due to the windlass mechanism (though often delayed or weak). In Vertical Talus, the heel remains in valgus.
- Propulsion: Disorganized. Push-off occurs from the midfoot rather than the metatarsal heads due to the midfoot break (sag).
- Fatigue: Use of accessory muscles to stabilize the foot leads to early tiring ("carry me" sign).
Investigations
Radiographs (Standard + Stress Views):
- Weight-Bearing AP:
- Kite's Angle (Talocalcaneal): Increased (greater than 35-40 degrees). Hindfoot Valgus.
- Talar Head Coverage: The navicular is shifted laterally, uncovering the talar head.
- Weight-Bearing Lateral:
- Meary's Angle: The talus axis points plantar to the 1st MT axis (Angle greater than 20 degrees).
- Calcaneal Pitch: Decreased.
- Forced Plantarflexion Lateral: The Money View.
- Oblique Talus: The axis of the talus lines up with the 1st metatarsal. The deformity reduces.
- Vertical Talus: The axis remains broken. The deformity is rigid.
- Forced Dorsiflexion Lateral:
- Assesses ankle vs midfoot stiffness.
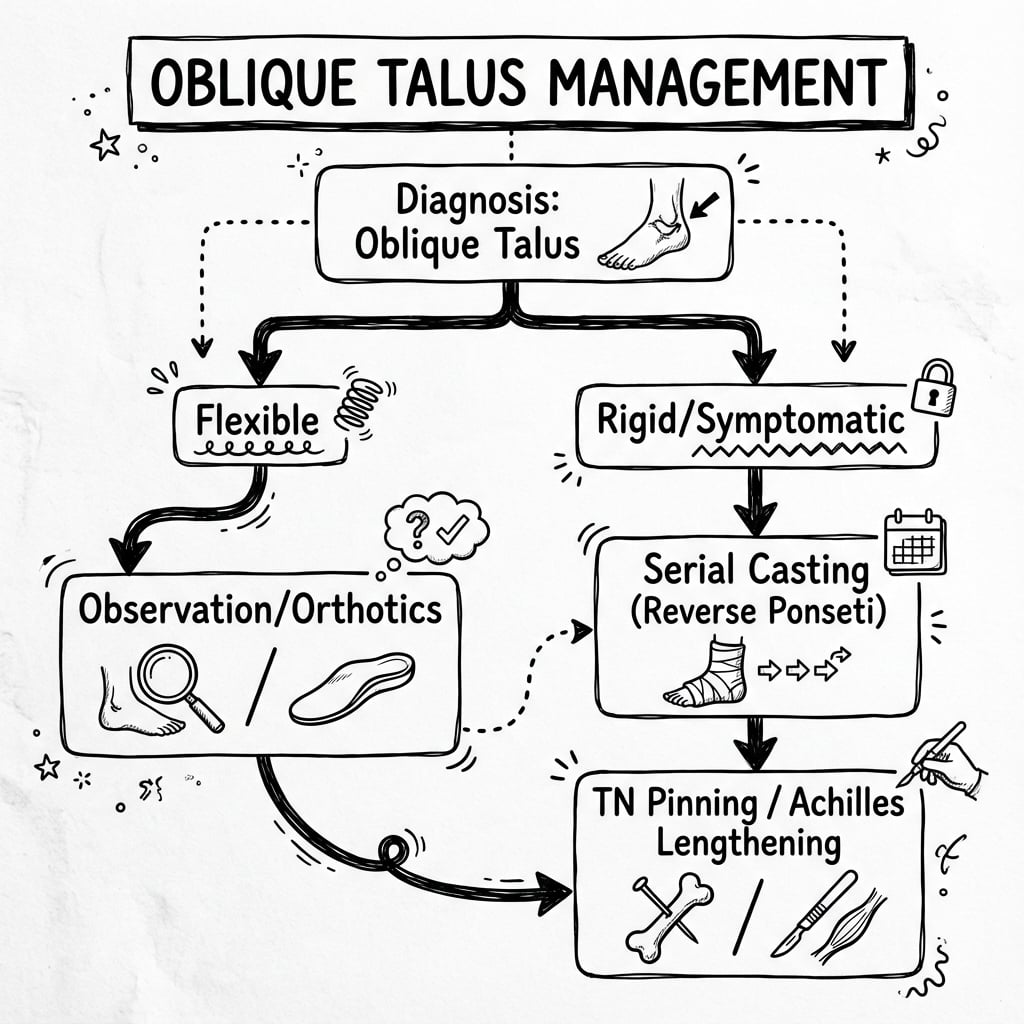
Management Algorithm
Surgical Technique
Minimal Invasive Pinning (Dobbs Technique modified)
Indication: After successful serial casting where stability is uncertain.
Technique:
- Percutaneous stabilization.
- Hold the foot in the corrected position (plantarflexion and inversion).
- Drive a K-wire retrograde from the dorsum of the 1st MT, through the navicular, into the Talus.
- Confirm on image intensifier.
- Cast for 6-8 weeks.
(Note: Ensure list items are not directly before closing tag)
Complications
| Complication | Risk Factors | Prevention/Management |
|---|---|---|
| Progression to CVT | Failure of treatment, severe laxity. | Prevention: Close monitoring. If becoming rigid, treat as CVT. |
| Painful Flatfoot | Subluxation causing arthritis. | Management: Orthotics first, then realignment surgery (osteotomies), finally triple arthrodesis (salvage). |
| Recurrence | Undercorrection of Equinus. | Prevention: Aggressive Achilles lengthening. Management: Repeat casting or surgery. |
| AVN of Talus | Excessive dissection during open reduction. | Prevention: Use Dobbs (minimally invasive) technique where possible. Avoid stripping dorsal neck. |
| Overcorrection | Varus deformity. | Prevention: Careful molding. Don't over-lengthen lateral column. |
Postoperative Care
- Casting: Long leg cast (knee flexed) is essential to control the gastrocnemius pull and prevent the pin from migrating.
- Duration: 6-8 weeks non-weight bearing.
- Pin Removal: At 6-8 weeks.
- Orthotics: Use of AFO (Ankle Foot Orthosis) or UCBL for 6-12 months post-correction to prevent recurrence.
- Monitoring: Radiographs every 6 months to check for recurrence of the "sag".
Outcomes/Prognosis
- Natural History: Some debate exists. Some authors believe Oblique Talus is simply a severe flatfoot and benign. Others believe it leads to inevitable degenerative changes. The truth is likely in the middle – symptomatic cases do poorly without treatment.
- Conservative: Orthotics provide symptom relief but do not change the radiographic angles.
- Surgical: Joint-sparing reconstructive surgery (osteotomies + soft tissue) yields good results in children. Arthrodesis is reserved for salvage in adults.
- Neuromuscular Cases: Have a higher recurrence rate and may require bony stabilization (arthrodesis) earlier.
Evidence Base
- Establishes oblique talus as a distinct entity between severe flexible pes planus and congenital convex pes valgus (CVT)
- Key feature is ABSENCE of a fixed talonavicular dislocation; the TN joint is often only pushed to maximum range, not even truly subluxed
- Describes two subsets based on whether the calcaneal inclination angle is maintained or reversed
- Classified 69 cases of congenital vertical talus into 5 aetiological groups (neural tube, neuromuscular, syndromic, chromosomal, idiopathic)
- Introduced the talar-axis and calcaneal-axis to first-metatarsal-base angles (TAMBA / CAMBA) to quantify deformity
- Defined the transition from flexible oblique talus to rigid CVT at a TAMBA of approximately 60 degrees and CAMBA of approximately 20 degrees
- 11 patients (19 feet) treated with serial reverse-Ponseti casts (mean 5 casts), percutaneous Achilles tenotomy and talonavicular pin fixation, minimum 2-year follow-up
- All radiographic parameters improved significantly (p less than 0.0001) and reached normal age-matched values without extensive soft-tissue release
- Dorsal navicular subluxation recurred in 3 patients, ALL of whom had NOT undergone talonavicular pin fixation
- 31 severe symptomatic valgus feet (flatfoot and skewfoot) in 20 children corrected by a modified Evans calcaneal lengthening osteotomy
- Satisfactory correction of all hindfoot components in all but the 2 most severe feet, with subtalar motion preserved (joint-sparing)
- 26 of 31 deformities were neuromuscular in origin, supporting use in lax/spastic feet while avoiding arthrodesis
- Most paediatric flatfoot is flexible, painless and resolves by adolescence; observation is safe and appropriate for the asymptomatic child
- Orthotics are generally unproven to alter the natural course of flexible flatfoot but may relieve pain when present
- No large prospective trials compare natural history versus treatment, so surgery is reserved for the painful or rigid foot
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
The Rocker Bottom Foot
"A newborn presents with a rocker bottom foot. How do you distinguish between CVT and Oblique Talus?"
The key differentiator is rigidity. I would perform a physical exam focusing on the midfoot. I would attempt to reduce the navicular onto the talus by plantarflexing and inverting the foot. If it reduces (slides back), it is an Oblique Talus. If it is rigid and irreducible, it is a Congenital Vertical Talus. I would confirm this with a forced plantarflexion lateral radiograph.
The Painful Teenager
"14-year-old with painful bilateral planovalgus feet. Meary's angle is 25 degrees. Navicular subluxed. Treatment?"
This represents a symptomatic Oblique Talus or severe Flexible Flatfoot. Since conservative measures (orthotics) have likely failed given the severity, I would consider surgical reconstruction. My aim is joint-preserving. I would propose a Lateral Column Lengthening (Evans) to correct the hindfoot valgus and reduce the TN joint, possibly combined with a Medial Cuneiform Osteotomy (Cotton) to restore the arch. I would also assess for Achilles tightness.
The Neuromuscular Foot
"Child with Cerebral Palsy and Oblique Talus. Does this change your management?"
Yes. In neuromuscular conditions, the deforming forces (spasticity, muscle imbalance) are persistent. Soft tissue procedures alone invariably fail. Recurrence is high. I would be more aggressive with stabilization. While I would still attempt reconstruction (osteotomies + tendon balancing), I would have a lower threshold for bony stabilization (e.g., Grice arthrodesis or subtalar fusion) if the deformity is severe/unstable, although definitive fusion is best delayed until maturity.
MCQ Practice Points
Radiology MCQ
Q: Which view best differentiates Oblique Talus from Vertical Talus? A: Forced Plantarflexion Lateral. Oblique Talus reduces (axis restores); CVT does not.
Natural History
Q: What is the natural history of untreated oblique talus? A: Most cases remain asymptomatic or have mild flatfoot symptoms. Unlike CVT, it does not cause severe disability.
Radiographic Key
Q: What is the key radiographic view to distinguish Oblique Talus from CVT? A: Forced Plantarflexion Lateral View. In Oblique Talus, the TN joint reduces (lines up). In CVT, it remains dislocated.
Anatomy MCQ
Q: Where does the navicular articulate in Oblique Talus? A: Dorsal aspect of the Talar Head. It is subluxed, not dislocated (dislocation = CVT).
Association MCQ
Q: What is a strong risk factor for Oblique Talus? A: Generalised Ligamentous Laxity (or Neuromuscular conditions).
Treatment MCQ
Q: Why is serial casting successful in Oblique Talus but not rigid CVT? A: Because the TN joint is capable of reduction. Casting stretches the dorsal tissues to allow the navicular to remain reduced. In rigid CVT, the dislocation is fixed.
Controversies & Areas of Uncertainty
- Is oblique talus a real entity or just severe flatfoot? Some authors regard it as the severe end of flexible flatfoot rather than a true diagnosis. Harris (Clin Podiatr Med Surg 2000) argues for keeping it distinct because it carries a better prognosis than CVT and prevents over-diagnosis of CVT.
- Definition of "subluxation": Harris notes that in many feet the TN joint is merely pushed to its maximum range and does not even meet a strict definition of subluxation, blurring the boundary with flexible flatfoot.
- Natural history is unknown: There are no large prospective trials defining which children progress to symptomatic disease, so the threshold for any intervention is judgement-based (Carr, Pediatrics 2016).
- Orthotics: Widely prescribed, but there is no high-level evidence that they alter bony architecture or natural history — their role is symptom relief only.
- Subtalar arthroereisis: Remains controversial — variable evidence, high hardware-removal and sinus-tarsi pain rates; not a substitute for correcting fixed valgus or equinus.
- Timing and choice of surgery: When casting is attempted versus straight to reconstruction, and joint-sparing osteotomy versus arthrodesis in neuromuscular feet, are not standardised.
Guidelines, Registries & Global Practice
Global epidemiology
- Flexible flatfoot is near-universal in toddlers and falls to roughly 15-25 percent prevalence by adolescence as the arch develops; oblique talus is a rare subset within this and is over-represented in children with hypotonia, ligamentous laxity syndromes and neuromuscular disease.
- There is no dedicated registry for oblique talus; evidence is drawn from single-centre paediatric series across North America, Europe and Asia.
Side-by-side guidance
| Body / Source | Position on the asymptomatic flexible / oblique foot | Surgery |
|---|---|---|
| AAOS / POSNA (US) | Observe; reserve treatment for pain or rigidity | Joint-sparing osteotomy (Evans/Cotton) before fusion |
| BOA / BSCOS (UK) | Reassure and observe; orthotics for symptom relief only | Reconstruction for persistent pain; arthrodesis as salvage |
| EFORT / European consensus | Distinguish flexible from rigid; image only if painful/rigid | Address hindfoot valgus and equinus together |
| Carr 2016 / AAP (Pediatrics) | Observation is safe for the asymptomatic child | Escalate only for painful or rigid foot |
The consistent global message: treat the symptomatic or rigid foot, not the radiograph; investigation and intervention are triggered by pain, rigidity or documented progression, not by appearance alone.
High- versus limited-resource practice
- Well-resourced settings: stress radiographs, gait analysis, custom UCBL/AFO orthoses, and image-guided minimally invasive casting/pinning are routinely available.
- Limited-resource settings: diagnosis rests on clinical reducibility and a single lateral radiograph; serial casting (reverse Ponseti) is favoured as a low-cost, effective first line, with reconstructive surgery reserved for the disabling or rigid foot.
OBLIQUE TALUS
Clinical summary
Key Features
- •Flexible Deformity
- •Reducible TN Joint
- •Talar Head Prominence
- •Painless in Child
X-ray Findings
- •Plantarflexed Talus
- •Normal Calcaneal Pitch
- •Reduces on PF View
- •Meary's Angle Broken
Differentiation
- •CVT is Rigid
- •Oblique is Flexible
- •Flatfoot is variant
- •Neuromuscular (Exclude)
Management
- •Observation (Most)
- •Orthotics (Symptomatic)
- •Stretching (Achilles)
- •Surgery (Rare)