External rotation symphysis diastasis - the classic pelvic emergency
Open Book Classification
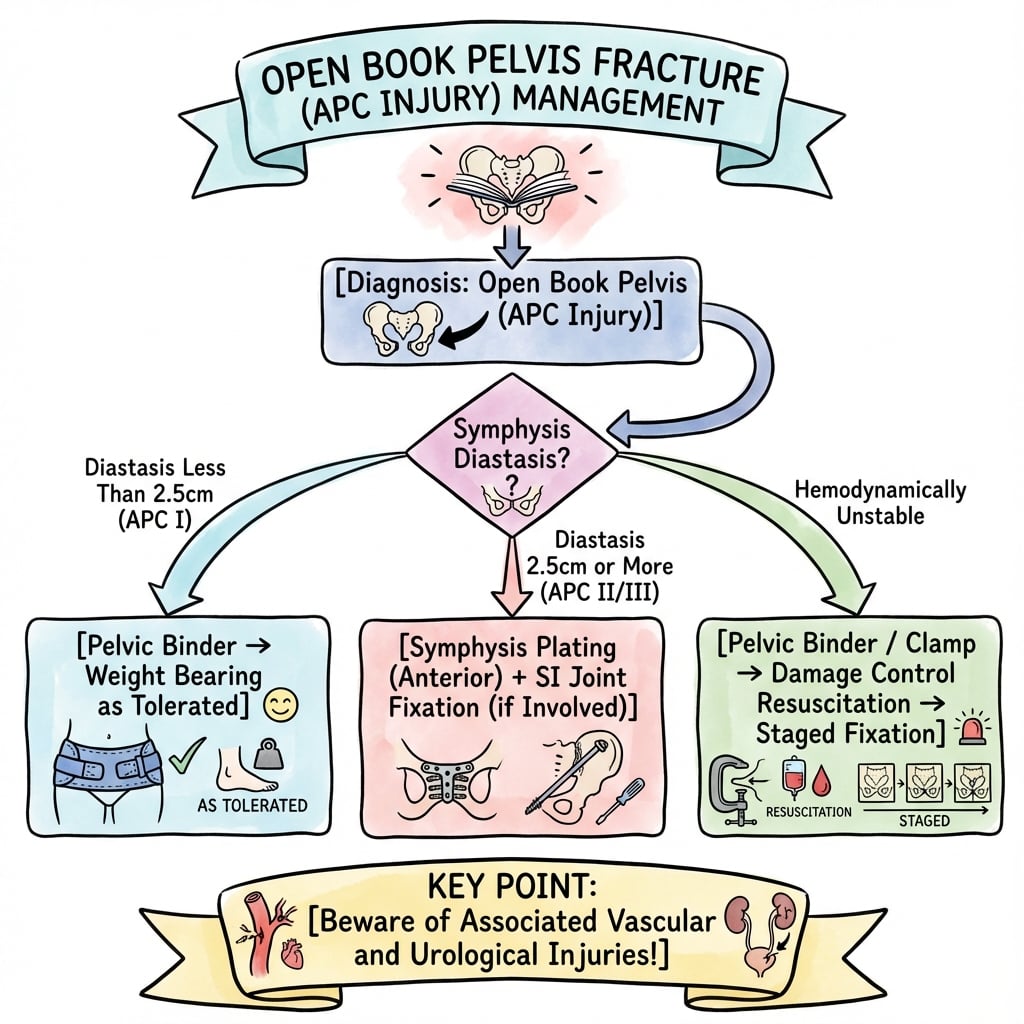
Critical Must-Knows
- PELVIC BINDER immediately - do NOT wait for imaging
- 2.5cm symphysis widening is the surgical threshold
- External rotation OPENS the book - binder CLOSES it
- 80% of bleeding is VENOUS - mechanical closure helps most
- Symphysis fixation alone if posterior ligaments intact (APC-II)
Clinical Pearls
- "Open book = pelvis opens like a book (symphysis = spine of book)
- "Normal symphysis width approximately 5mm, pathological greater than 10mm
- "Greater than 2.5cm widening = anterior SI ligament disruption
- "Assess posterior stability - determines if anterior fixation alone sufficient
- "Urological injury common - check for blood at meatus
Exam Warning
Open book injuries are a PELVIC EMERGENCY. The external rotation mechanism opens the pelvic ring, massively increasing pelvic volume and allowing uncontrolled hemorrhage. The pelvic binder CLOSES the book and restores tamponade - apply it IMMEDIATELY in any suspected case. Do NOT wait for imaging to confirm the injury. The 2.5cm symphysis widening threshold distinguishes stable (conservative) from unstable (surgical) injuries.
At a Glance
Open book pelvic injuries (APC injuries) result from external rotation forces that "open" the pelvis like a book at the symphysis pubis. Symphysis widening greater than 2.5cm is the surgical threshold, indicating anterior SI ligament disruption (APC-II). Critical emergency: the open book increases pelvic volume by up to 4L, causing life-threatening hemorrhage. Apply pelvic binder IMMEDIATELY - do not wait for imaging. 80% of bleeding is venous and responds to mechanical closure. Definitive treatment depends on posterior stability: symphysis plating alone if posterior ligaments intact (APC-II), or combined anterior and posterior fixation for APC-III.
Open Book Injury Quick Reference
BOOKBOOK - Open Book Key Features
| B | Binder immediately don't wait for imaging |
| O | Opens pelvic ring volume expands dramatically |
| O | Originates from external rotation force AP compression |
| K | Key threshold is 2.5cm symphysis widening |
| B | Binder immediately don't wait for imaging | O | Originates from external rotation force AP compression |
| O | Opens pelvic ring volume expands dramatically | K | Key threshold is 2.5cm symphysis widening |
Hook:Open BOOK injuries need immediate BINDER to close the book
VOLUMEVOLUME - Why Open Book Bleeds
| V | Volume expands as ring opens 1.5L to greater than 4L |
| O | Opens retroperitoneal space Opens retroperitoneal space |
| L | Lost tamponade effect from ring disruption |
| U | Uncontrolled venous plexus bleeding 80% |
| M | Massive transfusion often required |
| E | Early binder is lifesaving |
| V | Volume expands as ring opens 1.5L to greater than 4L | L | Lost tamponade effect from ring disruption | M | Massive transfusion often required |
| O | Opens retroperitoneal space Opens retroperitoneal space | U | Uncontrolled venous plexus bleeding 80% | E | Early binder is lifesaving |
Hook:VOLUME expansion causes hemorrhage - close the book to restore tamponade
CLOSECLOSE - Pelvic Binder Protocol
| C | Circumferential application Circumferential application |
| L | Level of greater trochanters NOT iliac crests |
| O | Opens becomes closed internal rotation force |
| S | Snug but not too tight check skin |
| E | Early apply before imaging confirmation |
| C | Circumferential application Circumferential application | S | Snug but not too tight check skin |
| L | Level of greater trochanters NOT iliac crests | E | Early apply before imaging confirmation |
| O | Opens becomes closed internal rotation force |
Hook:CLOSE the book with correct binder placement at trochanters
Overview
Introduction
"Open book" is the colloquial term for anteroposterior compression (APC) pelvic injuries, specifically APC-II pattern. The name derives from the appearance of the pelvis on AP radiograph - the two hemipelves externally rotate and separate anteriorly at the symphysis, like opening a book where the symphysis represents the spine.
This injury pattern is critical because it produces the highest hemorrhage risk of all pelvic fracture patterns. The external rotation mechanism dramatically increases pelvic volume, eliminating the tamponade effect of the intact ring and allowing massive retroperitoneal bleeding.
The Book Analogy
Understanding the "book" concept:
- Spine of book: Pubic symphysis
- Pages: The two hemipelves
- Opening the book: External rotation force
- Closing the book: Pelvic binder (internal rotation)
Clinical Significance
Why Open Book Injuries Matter:
- Hemorrhage: Volume expansion allows liters of blood loss
- Instability: Rotational instability affects function
- Associated injuries: Urological, vascular, neurological
- Time-critical: Hemorrhage control is lifesaving
- Recognizable pattern: Classic radiographic appearance
Epidemiology
Incidence:
- Most recognized pelvic injury pattern
- Classic presentation of APC mechanism
- Common in motorcycle accidents
Mechanism:
- Motorcycle collision (handlebar impact to pelvis)
- Pedestrian struck anteriorly
- Frontal MVA with AP compression
- Crush injuries
Demographics:
- Young males predominate
- High-energy mechanism
- Associated polytrauma common
Anatomy and Pathophysiology
Pelvic Ring Biomechanics
Normal Anatomy
Pubic Symphysis:
- Fibrocartilaginous joint
- Normal width approximately 5mm (range 3-8mm)
- Increases physiologically in pregnancy
- Limited mobility normally
Stability Hierarchy:
- Posterior structures provide 60% of stability
- Anterior structures provide 40% of stability
- Symphysis disruption alone does NOT cause complete instability
Open Book Pathoanatomy
The external rotation force causes sequential failure:
Stage 1 (less than 2.5cm diastasis - APC-I):
- Symphysis stretched/partially disrupted
- Anterior SI ligaments intact
- Mechanically stable
- Conservative management usually appropriate
Stage 2 (greater than 2.5cm diastasis - APC-II/Open Book):
- Complete symphysis disruption
- Anterior SI ligaments disrupted
- Sacrospinous ligament torn
- Posterior SI ligaments INTACT (KEY)
- Rotationally unstable, vertically stable
Stage 3 (Complete disruption - APC-III):
- All anterior structures disrupted
- All posterior structures disrupted
- Complete hemipelvic instability
Hemorrhage Mechanism
Volume Expansion:
- Normal pelvic volume approximately 1.5 liters
- Open book can expand to greater than 4 liters
- No tamponade from intact ring
- Retroperitoneal space fills with blood
Bleeding Sources:
- Venous (80%): Presacral plexus, internal iliac veins
- Arterial (20%): Superior gluteal (most common), internal iliac branches
- Bone surfaces: Cancellous bleeding
Associated Soft Tissue Injuries
Urological (Common):
- Bladder injury (15-25%)
- Urethral injury (males)
- Mechanism: Symphysis disruption tears attached structures
Vascular:
- Presacral venous plexus
- Internal iliac branches
- Corona mortis (variant vessels)
Neurological (Less Common):
- L5 nerve root
- Lumbosacral plexus
- Less common than VS injuries
Classification Systems
Young-Burgess APC Classification
The Anteroposterior Compression (APC) classification system is essential for understanding open book injuries and guiding treatment.
Injury Pattern
- Symphysis widening UNDER 2.5cm
- Pubic rami may have vertical fractures
- Anterior SI ligaments INTACT
- Posterior SI ligaments INTACT
- Sacrospinous and sacrotuberous ligaments INTACT
Stability
- Mechanically STABLE
- No rotational instability
- No vertical instability
Clinical Features
- Minimal hemorrhage risk
- Usually stable hemodynamically
- Low energy mechanism possible
Treatment
- CONSERVATIVE management
- Symptom-based mobilization
- Protected weight bearing as tolerated
- Usually does NOT require surgery
- Binder may provide symptomatic relief
Prognosis
- Excellent functional outcome
- Early return to activity
- Low complication rate
Overall, APC-I injuries have excellent prognosis with conservative management.
Key Radiographic Measurements
Symphysis Width:
- Normal: approximately 5mm (3-8mm range)
- Suspicious: greater than 10mm
- APC-I: under 2.5cm
- APC-II/III: greater than 2.5cm
SI Joint Widening:
- Anterior SI widening suggests ligament disruption
- Posterior SI widening indicates APC-III
- CT imaging essential for accurate assessment
Inlet View Assessment:
- Best view for assessing symphysis diastasis
- Shows rotational deformity
- Evaluates anterior SI joint
Clinical Assessment
Primary Survey
Open book injuries present in major trauma context. Assessment follows ATLS principles.
Mechanism History
Classic Mechanisms:
- Motorcycle vs car (handlebar impact)
- Pedestrian struck from front
- Frontal vehicle collision
- Direct AP compression
Physical Examination
Apply pelvic binder BEFORE completing examination if open book injury suspected. Do NOT repeatedly compress or distract the pelvis - this can dislodge clot and restart hemorrhage. A single gentle assessment is acceptable.
Inspection:
- Leg external rotation (both limbs)
- Perineal swelling/ecchymosis
- Scrotal/labial hematoma
- Blood at urethral meatus (urological injury)
- Obvious widening of pubic area
Palpation (Once Only):
- Palpable symphysis gap
- Tenderness over symphysis
- SI joint tenderness
- Avoid repeated manipulation
Signs of Hemorrhage:
- Tachycardia (early sign)
- Hypotension
- Reduced consciousness
- Poor capillary refill
- Ongoing transfusion requirements
Urological Assessment
CRITICAL Before Catheterization:
- Blood at urethral meatus
- Perineal hematoma
- High-riding prostate (DRE in males)
- Scrotal hematoma
If Urethral Injury Suspected:
- Do NOT attempt urethral catheterization
- Retrograde urethrogram first
- Suprapubic catheter if complete rupture
Stability Assessment
Clinical Signs of Instability:
- Bilateral leg external rotation
- Palpable symphysis gap greater than 2 finger widths
- Hemodynamic instability
- Ongoing resuscitation requirements
Radiographic Correlation:
- greater than 2.5cm symphysis widening
- Anterior SI widening
- Assess posterior integrity on CT
Differential Diagnosis
The widened or painful symphysis on an AP pelvis has several mimics. The key discriminators are the mechanism, the degree and symmetry of widening, and the posterior ring on CT.
Differential Diagnosis of Symphyseal Widening / Anterior Pelvic Pain
Differential Pearl
A widened symphysis is NOT always traumatic. Peripartum symphysis pubis dysfunction can exceed 10mm, and osteitis pubis or septic arthritis of the symphysis causes pain with erosive (not separated) changes. In trauma, the discriminator from lateral compression is direction: open book OPENS the ring (external rotation), whereas lateral compression CLOSES it (internal rotation) - which is why a binder helps the former and may overcompress the latter.
Investigations
Imaging Protocol
Plain Radiography
AP Pelvis (First-Line):
- Immediate in trauma bay
- Can be done with binder in place
- Measure symphysis width
Measurement Technique:
- Measure at superior aspect of symphysis
- Normal: approximately 5mm
- greater than 10mm: Suspicious
- greater than 25mm (2.5cm): Surgical threshold
Associated Findings:
- External rotation of hemipelves
- Pubic rami fractures
- SI joint widening
- Sacral fracture
Inlet View:
- Best demonstrates AP displacement
- Shows symphysis widening clearly
- Evaluates SI joint anteriorly
Outlet View:
- Evaluates vertical displacement
- Distinguishes from VS component
- Sacral fracture visualization
CT Imaging
Indications:
- All hemodynamically stable patients
- Surgical planning
- Assess posterior injury
Key Findings:
- Symphysis diastasis measurement
- Anterior SI ligament status
- Posterior SI ligament integrity (CRITICAL)
- Associated fractures
- Hematoma extent
CT Angiography:
- Active arterial bleeding
- Guides angioembolization
- Contrast extravasation
Retrograde Urethrogram
Indications:
- Blood at urethral meatus
- High-riding prostate
- Perineal hematoma
- Before urethral catheterization if suspicious
Technique:
- 20-30mL water-soluble contrast
- Gentle injection
- Look for extravasation
Cystogram
Indications:
- Gross hematuria with pelvic fracture
- After urethral integrity confirmed
Findings:
- Extraperitoneal rupture: Flame-shaped extravasation
- Intraperitoneal rupture: Contrast around bowel
Management
Treatment Algorithm
PELVIC BINDER is FIRST-LINE treatment. Apply IMMEDIATELY for ANY suspected open book injury. Do NOT wait for X-ray confirmation. The binder CLOSES the book, reduces pelvic volume, and restores tamponade. This is TIME-CRITICAL hemorrhage control.
Pelvic Binder Application
Mechanism of Action:
- Applies internal rotation force
- Closes the "open book"
- Reduces pelvic volume
- Restores tamponade effect
- Compresses bleeding surfaces
Correct Position:
- At level of GREATER TROCHANTERS
- NOT at iliac crests (too high - ineffective)
- Circumferential compression
- Not too tight (skin necrosis risk)
Options:
- Commercial pelvic binder (preferred)
- Sheet wrap (acceptable alternative)
- T-POD, SAM Pelvic Sling, etc.
Damage Control Resuscitation
Principles:
- Massive Transfusion Protocol (MTP)
- 1:1:1 ratio (RBC:FFP:Platelets)
- Permissive hypotension (SBP 80-90mmHg)
- Avoid crystalloid overload
- TXA within 3 hours (1g bolus then 1g over 8 hours)
- Correct hypothermia
- Correct acidosis
- Correct coagulopathy
Critical first steps are binder and resuscitation while identifying bleeding sources.
Surgical Technique
Symphysis Plating - Step by Step
Patient Assessment
- Confirm APC-II pattern on CT (posterior SI ligaments intact)
- Check for urological injuries (cystogram/urethrogram if indicated)
- Rule out bladder injury requiring concurrent repair
- Identify Morel-Lavallee lesion (may delay surgery)
- Hemodynamic stability confirmed
Surgical Timing
- Acute: Within 24-48 hours if stable
- May need damage control first (external fixation)
- Definitive fixation when medically optimized
- Soft tissue condition permitting
Equipment Needed
- 3.5mm reconstruction plate or symphysis-specific plate
- 3.5mm cortical screws (6-8 screws)
- Large pointed reduction forceps
- Fluoroscopy (inlet, outlet, AP views)
- Pelvic retractors
- Bladder catheter in situ
Careful preoperative planning ensures optimal surgical outcome.
Posterior SI Screw Fixation (APC-III)
Indications
- APC-III with posterior SI disruption
- Posterior SI widening on CT
- Vertical instability
Technique Overview
- Percutaneous iliosacral screw preferred
- Patient prone or lateral
- Entry point: Posterior iliac crest
- Trajectory: Across SI joint into S1 body
- Guide with AP, inlet, outlet views
- 6.5mm or 7.3mm cannulated screws
- One or two screws depending on stability
Key Safety Points
- L5 nerve root at risk (stays superior)
- S1 foramen must be avoided
- Stay in "safe zone" of S1 body
- Outlet view ensures screw below L5
Complications
Early Complications
Hemorrhagic Shock:
- Primary cause of early mortality
- Requires aggressive resuscitation
- Binder is lifesaving intervention
Urological Injury:
- Bladder rupture (15-25% incidence with open book)
- Extraperitoneal more common (symphysis tears bladder)
- Intraperitoneal rupture with full bladder at impact
- Urethral injury (male predominance, longer urethra)
- Membranous urethra at risk
- Blood at meatus is cardinal sign
Management:
- Bladder extraperitoneal: Catheter drainage 10-14 days
- Bladder intraperitoneal: Surgical repair required
- Urethral: Retrograde urethrogram before catheterization
- Suprapubic catheter if complete urethral rupture
- Delayed primary repair vs immediate realignment
Vascular Injury:
- Superior gluteal artery most common arterial source (exits greater sciatic notch)
- Corona mortis (aberrant obturator vessels, present in 30%)
- Can cause significant bleeding during anterior approaches
- Angioembolization effective for arterial injuries
Morel-Lavallee Lesion:
- Closed degloving injury
- Subcutaneous fat separates from fascia creating fluid-filled cavity
- Typically over greater trochanter or iliac crest
- Delays surgical fixation
- Infection risk if not addressed
- May need debridement before surgery
Thromboembolic Events:
- Very high DVT risk
- Early prophylaxis when safe
- May need IVC filter
Infection:
- Especially with open injuries
- Morel-Lavallee lesion increases risk
- Surgical site infection
Late Complications
Malunion:
- Residual diastasis
- Gait abnormality
- Chronic pubic symphysis pain
Hardware Failure:
- Plate loosening
- Screw pullout
- May indicate unrecognized posterior instability
Sexual Dysfunction:
- Erectile dysfunction (vascular or neurological)
- Dyspareunia
- Counseling important
Chronic Pain:
- Symphysis pain
- SI joint pain (if posterior injury)
- May need plate removal
Postoperative Care
Immediate Postoperative Period
Initial Management:
- ICU or HDU monitoring if major resuscitation
- Continue DVT prophylaxis (mechanical and chemical when safe)
- Adequate analgesia (epidural or PCA)
- Monitor for ongoing bleeding
- Bladder catheter initially
- Regular neurovascular observations
Wound Care:
- Inspect daily for hematoma
- Watch for Morel-Lavallee complications
- Remove drain when output under 30mL/24hr
- Suture/staple removal at 14 days
Weight Bearing Protocol
APC-II (Symphysis Plate Alone)
Weeks 0-6:
- Touchdown weight bearing (TDWB) both legs
- Mobilize with walking frame/crutches
- No single leg stance
- Pelvic tilt exercises in bed
- Gentle range of motion
Weeks 6-12:
- Progress to partial weight bearing (50%)
- X-rays at 6 weeks to check healing
- If union progressing, increase weight bearing
- May transition to single crutch
Weeks 12+:
- Full weight bearing as tolerated
- X-ray confirmation of symphysis union
- Gradual return to activities
- Formal physiotherapy
APC-III (Anterior + Posterior Fixation)
Weeks 0-8:
- Touchdown weight bearing (stricter than APC-II)
- Higher instability requires longer protection
- Active hip and knee exercises
Weeks 8-12:
- X-rays to assess posterior healing
- Begin partial weight bearing if healing well
- Continue protection longer than APC-II
Weeks 12-16:
- Progress to full weight bearing
- May need 16 weeks for complete posterior healing
- Gradual activity progression
Physiotherapy Protocol
Phase 1 (Weeks 0-6): Protection
- Pelvic floor exercises
- Gluteal isometrics
- Ankle pumps
- Knee extension in bed
- Avoid hip abduction/adduction against resistance
Phase 2 (Weeks 6-12): Progressive Loading
- Hydrotherapy (excellent for early mobilization)
- Stationary bike (no resistance)
- Gentle core strengthening
- Balance exercises
Phase 3 (Weeks 12+): Functional Restoration
- Progressive resistance exercises
- Gait retraining
- Return to work assessment
- Sport-specific training if appropriate
DVT Prophylaxis
Critical Consideration:
- VERY HIGH risk (immobility + pelvic trauma + surgery)
- Mechanical: TED stockings, intermittent pneumatic compression
- Chemical: LMWH or alternative (when bleeding controlled)
- Duration: Minimum 6 weeks, often 12 weeks
- Consider IVC filter if bleeding prohibits anticoagulation
Follow-Up Schedule
2 weeks: Wound check, remove sutures/staples
6 weeks: X-rays (AP, inlet, outlet), assess healing, progress weight bearing
12 weeks: X-rays, consider full weight bearing if union evident
6 months: Final X-rays, functional assessment
1 year: Long-term outcome assessment, consider plate removal if symptomatic
Plate Removal
Indications:
- Symptomatic hardware (pain with activity)
- Usually NOT needed
- Wait minimum 12 months for solid union
- More common in young, active patients
Timing:
- Not before 18-24 months
- Ensure complete symphysis healing
- May improve pain in select patients
Outcomes and Prognosis
Functional Outcomes
APC-II (Open Book) - Good Prognosis
Expected Outcomes:
- 70-80% return to pre-injury function
- Most patients ambulate independently by 6 months
- Return to work: 4-6 months for sedentary, 6-12 months for physical
- Sports: 9-12 months for high-impact activities
Factors Predicting Better Outcome:
- Younger age
- Anatomic reduction achieved
- No posterior injury
- Early appropriate fixation
- No major associated injuries
APC-III - More Guarded Prognosis
Expected Outcomes:
- 50-60% return to pre-injury level
- Longer recovery (12-18 months)
- Higher residual pain rates
- More likely to have permanent limitations
Complications More Common:
- Chronic SI pain
- Residual instability
- Gait abnormalities
- Need for revision surgery
Mortality and Morbidity
Mortality:
- APC-II: 5-8% (mostly from hemorrhage if uncontrolled)
- APC-III: 15-20%
- Early deaths: Hemorrhagic shock
- Late deaths: Multi-organ failure, PE
Major Morbidity:
- DVT/PE: 20-30% without prophylaxis
- Sexual dysfunction: 10-15%
- Chronic pain: 20-30%
- Gait abnormality: 10-20%
Long-Term Issues
Pelvic Pain:
- Symphysis pain common initially
- Usually improves by 12 months
- Persistent pain in 15-20%
- May benefit from plate removal
Sexual Function:
- Males: Erectile dysfunction (vascular or neurological)
- Females: Dyspareunia, altered sensation
- Counseling important
- May improve with time
Pregnancy Considerations:
- Future pregnancy generally possible
- May have pelvic pain during pregnancy
- Consider elective caesarean section
- Discuss with patient before fixation
Arthritis:
- SI joint arthritis long-term risk if APC-III
- Symphysis arthritis rare with good reduction
- Monitor for late degenerative changes
Return to Activity
Desk Work: 3-4 months
Light Manual Work: 6 months
Heavy Manual Work: 9-12 months
Running: 9-12 months
Contact Sports: 12+ months (if ever)
Driving: When off narcotics and can perform emergency stop (usually 8-12 weeks)
Evidence and Guidelines
Young-Burgess Classification (Defining Landmark)
- Prospective series of 210 high-energy pelvic ring disruptions established the force-vector classification (lateral compression, anteroposterior compression, vertical shear, combined). Anteroposterior compression (open book) injuries had the highest transfusion requirement (mean 14.8 units vs 3.6 units for lateral compression) and the highest mortality (20%), confirming the open book pattern as the most haemorrhagic mechanism.
Stability Determined by Posterior Lesion (Tile)
- The anterior structures (symphysis and pubic rami) contribute approximately 40% of pelvic stiffness, but the posterior sacroiliac complex is more important to ring stability. Classification is therefore based on the posterior lesion: type A stable, type B (open book, bucket-handle) rotationally unstable, type C completely unstable. Type A and B account for 70-80% of injuries.
Circumferential Compression Reduces the Open Book
- Prospective clinical trial of a force-controlled pelvic circumferential compression device in 16 patients. In external rotation (open book) patterns the device reduced pelvic width by 9.9% +/- 6.0%, closely approximating the 10.0% +/- 4.1% reduction achieved by definitive fixation, without overcompressing lateral compression injuries. No complications occurred.
Predominantly Venous Hemorrhage Source
- Postmortem angiographic and dissection study of the hypogastric (internal iliac) system in fatal pelvic fractures demonstrated that the majority of pelvic haemorrhage arises from low-pressure venous and cancellous bone sources rather than from major arterial injury, which is comparatively uncommon.
Tranexamic Acid in Bleeding Trauma (CRASH-2)
- Randomised, placebo-controlled trial of 20,211 bleeding trauma patients across 40 countries. Tranexamic acid (1g over 10 min, then 1g over 8 h) reduced all-cause mortality (14.5% vs 16.0%; RR 0.91, 95% CI 0.85-0.97) and death due to bleeding (4.9% vs 5.7%; RR 0.85, 95% CI 0.76-0.96), with greatest benefit when given early.
Concurrent Bladder Injury with Urethral Trauma
- In 98 patients with blunt urethral trauma, 28 had concurrent bladder injury. Injury Severity Score correlated strongly with bladder injury (OR 2.2 per 10-unit ISS rise). Patients with ISS greater than or equal to 34 had a 54% probability of bladder injury versus 13% with lower ISS.
Viva Scenarios
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
"A 28-year-old motorcyclist is brought in after colliding with a car. He is tachycardic (HR 130), hypotensive (BP 75/50), with both legs externally rotated. The AP pelvis shows 4cm symphysis diastasis. Describe your immediate management."
Immediate Recognition: This is an OPEN BOOK pelvic injury with hemorrhagic shock - a pelvic emergency.
Immediate Actions (Simultaneous):
- PELVIC BINDER at greater trochanter level - CLOSE THE BOOK
- Massive Transfusion Protocol activation
- Large bore IV access (x2), blood samples including crossmatch
- TXA 1g IV bolus
- Permissive hypotension (target SBP 80-90mmHg)
- Avoid excessive crystalloid
Concurrent Assessment:
- ATLS primary survey completion
- Exclude other hemorrhage sources (chest, abdomen)
- Blood at urethral meatus? - If yes, do NOT catheterize blindly
- Brief neurological assessment
If Responding to Resuscitation:
- CT pelvis with angiography when stable
- Define posterior injury pattern
- Angioembolization if arterial extravasation
- Definitive symphysis plating when optimized
If NOT Responding:
- Emergency external fixation
- Consider preperitoneal packing
- Angioembolization if available
- REBOA as bridge if trained personnel available
Definitive Management:
- Greater than 4cm diastasis = surgical fixation required
- CT to assess posterior SI ligaments
- If posterior intact (APC-II): Symphysis plating alone
- If posterior disrupted (APC-III): Add SI fixation
"Describe your surgical technique for symphysis plating in an open book pelvic injury. What are the key steps and potential complications?"
Preoperative Planning:
- Confirm this is APC-II (posterior SI ligaments intact on CT)
- Review for associated urological injuries
- Ensure hemodynamic stability
- Prophylactic antibiotics
Positioning:
- Supine on radiolucent table
- Fluoroscopy available (inlet, outlet, AP views)
- Prep widely including iliac crests
Approach (Pfannenstiel):
- Transverse incision 2cm above symphysis
- Incise rectus sheath transversely
- Separate rectus muscles in midline (DO NOT detach from pubis)
- Identify bladder - it is often contused, protect carefully
- Expose superior pubic ramus bilaterally
Reduction:
- Large pointed reduction forceps across symphysis
- Apply internal rotation force to close diastasis
- Confirm reduction on inlet view (should see symmetric ring)
- Accept less than 1cm residual diastasis
Fixation:
- 3.5mm reconstruction plate or symphysis-specific plate
- Position on superior surface of pubis
- 2-hole plate for simple diastasis
- 4-hole plate if additional rotational control needed
- Bicortical screws, avoid bladder
Potential Complications:
- Bladder injury (retract and protect)
- Corona mortis bleeding (ligate if encountered)
- Infection (especially with Morel-Lavallee lesion)
- Hardware failure (underestimated posterior injury)
- Loss of reduction (inadequate fixation)
"How do you differentiate between an APC-II (open book) injury and an APC-III injury? Why is this distinction clinically important?"
Key Distinction: Posterior SI ligament integrity
APC-II (Classic Open Book):
- Symphysis widening greater than 2.5cm
- Anterior SI ligaments disrupted
- Sacrospinous ligament torn
- Posterior SI ligaments INTACT (KEY DIFFERENCE)
- Rotationally unstable but vertically stable
APC-III:
- All above plus complete posterior disruption
- Posterior SI ligaments disrupted
- Sacrotuberous ligament torn
- Both rotationally AND vertically unstable
- Higher hemorrhage risk
- Higher mortality
How to Differentiate:
- CT imaging is essential
- Evaluate SI joint on axial and coronal CT
- Posterior SI widening suggests APC-III
- Sacral fracture may indicate posterior involvement
- Vertical displacement suggests complete disruption
Clinical Importance:
- APC-II: Symphysis fixation ALONE is sufficient
- APC-III: Requires BOTH anterior AND posterior fixation
- Underestimating leads to inadequate fixation and failure
- APC-III has higher hemorrhage risk requiring more aggressive resuscitation
Surgical Implications:
- APC-II: Pfannenstiel approach, symphysis plate, done
- APC-III: Add SI screws or posterior fixation
- Getting this wrong leads to hardware failure and malunion
MCQ Practice Points
Classification
Q: What symphysis width indicates surgical fixation in open book pelvic injury?
A: Greater than 2.5cm. This threshold distinguishes APC-I (partial disruption, conservative management) from APC-II (complete anterior disruption, requires fixation).
Key Distinction
Q: What structure differentiates APC-II (open book) from APC-III injury?
A: Posterior sacroiliac ligaments. APC-II has intact posterior SI ligaments (vertically stable, rotationally unstable). APC-III has complete posterior disruption (vertically AND rotationally unstable).
Hemorrhage
Q: What percentage of bleeding in pelvic fractures is venous vs arterial?
A: 80% venous, 20% arterial. This is why pelvic binders work - they reduce pelvic volume and restore venous tamponade. Superior gluteal artery is the most common arterial bleeding source.
Pelvic Binder
Q: What is the correct anatomical landmark for pelvic binder placement?
A: Greater trochanters (NOT iliac crests). Binder at trochanter level closes the open book and reduces pelvic volume from greater than 4L back toward normal 1.5L, restoring tamponade.
Surgical Planning
Q: An APC-II injury is confirmed on CT with intact posterior SI ligaments. What fixation is required?
A: Symphysis plating alone is sufficient for APC-II. Use 3.5mm reconstruction plate via Pfannenstiel approach. APC-III requires both anterior AND posterior (SI screw) fixation.
Guidelines, Registries & Global Practice
Global Epidemiology
According to PubMed (Balogh et al., J Trauma 2007, DOI), a population-based study of an inclusive trauma system found the overall incidence of pelvic ring fractures was 23 per 100,000 persons per year, split evenly between high-energy (10 per 100,000) and low-energy (10 per 100,000) mechanisms, with 3 per 100,000 dying pre-hospital. High-energy fractures occurred predominantly in younger men, and pelvic-fracture-related mortality was always attributable to bleeding. Demonstrated arterial bleeding was rare (1.3 per 100,000 per year), reinforcing that most haemorrhage is venous and amenable to mechanical control.
In the original Young-Burgess series (Burgess et al., J Trauma 1990, PMID 2381002), anteroposterior compression (open book) injuries had the highest transfusion requirement (mean 14.8 units) and the highest mortality (20%) of all force-vector patterns. Type A (stable) and type B (rotationally unstable, including open book) patterns together account for 70-80% of all pelvic ring injuries (Tile, JAAOS 1996, DOI).
Guideline Comparison (Side-by-Side)
International Guidance on the Hemodynamically Unstable Open Book Pelvis
There is broad international concordance: all major bodies (WSES, NICE NG37, BOA/BOAST, AAOS/OTA, AO Foundation, EFORT) endorse immediate circumferential compression, early tranexamic acid, and posterior-ring-led decision making for definitive fixation. The principal practice variation is in the haemorrhage-control adjunct - North American and Northern European centres with hybrid theatres favour early angioembolisation, whereas systems without immediate interventional radiology (and most military doctrine) favour preperitoneal packing first. The WSES classification and guidelines (Coccolini et al., World J Emerg Surg 2017, DOI) integrate haemodynamic status with anatomical pattern and are the most widely adopted contemporary algorithm.
Registry Evidence
National and regional registries (German Pelvic Trauma Registry / TraumaRegister DGU, UK Trauma Audit and Research Network [TARN], and the Victorian Orthopaedic Trauma Outcomes Registry [VOTOR] in Australia) consistently report that bleeding remains the dominant early cause of death in unstable pelvic ring injury, and that mortality is driven more by associated injuries and haemodynamic status than by the anterior diastasis itself. TARN data have been used to quantify the small subset of exsanguinating pelvic patients potentially amenable to REBOA in England and Wales (Barnard et al., Emerg Med J 2015, DOI).
Pharmacological and System Considerations
| Agent / measure | Principle | Notes |
|---|---|---|
| Tranexamic acid | 1 g IV over 10 min, then 1 g over 8 h, within 3 h of injury | Level I evidence (CRASH-2); concordant across all guidelines |
| VTE prophylaxis | Mechanical immediately; pharmacological (LMWH) once haemorrhage controlled | Very high VTE risk; continue 6-12 weeks; consider IVC filter only if anticoagulation contraindicated |
| Surgical antibiotic prophylaxis | First-generation cephalosporin at induction | Add Gram-negative cover for open injury per local antimicrobial guidance (e.g. eTG in Australia) |
Practice variation: pharmacological VTE prophylaxis timing also differs - earlier initiation in some European protocols versus more conservative North American thresholds - reflecting the tension between bleeding and thrombosis risk in the polytrauma pelvis. Drug availability, reimbursement and trauma-network maturity differ by jurisdiction and should be checked against local formularies and guidelines.
Exam Focus Points
High-Yield Concepts
Clinical Pearl
REMEMBER: Open book = APC-II = symphysis widening greater than 2.5cm with INTACT posterior SI ligaments. If posterior ligaments are disrupted, it becomes APC-III and requires BOTH anterior and posterior fixation. The posterior injury determines treatment, not the anterior widening.
Critical Numbers
- 5mm: Normal symphysis width
- 10mm: Suspicious for injury
- 25mm (2.5cm): Surgical threshold (APC-I vs APC-II)
- 80%: Proportion of bleeding that is venous
- 1.5L to 4L: Pelvic volume increase with open book
Surgical Decision-Making
Symphysis Fixation Alone (APC-II):
- Posterior SI ligaments intact on CT
- Symphysis widening is the primary pathology
- Single anterior approach, symphysis plate
Add Posterior Fixation (APC-III):
- Posterior SI widening on CT
- SI ligament disruption
- Complete hemipelvic instability
- Need anterior AND posterior fixation
Binder Positioning
Correct: Greater trochanters Incorrect: Iliac crests (too high, doesn't close book effectively)
OPEN BOOK PELVIC INJURIES
Clinical summary
Key Definitions
- •Open book = symphysis widening greater than 2.5cm (APC-II)
- •Mechanism: external rotation force (AP compression)
- •Normal symphysis = approximately 5mm
- •Surgical threshold = greater than 2.5cm (25mm)
- •Key distinction: posterior SI ligament status determines treatment
Critical Numbers
- •Volume expansion: 1.5L to greater than 4L
- •Bleeding source: 80% venous, 20% arterial
- •Binder position: greater TROCHANTERS (NOT iliac crests)
- •2.5cm = surgical threshold to remember
Critical Actions
- •Hemodynamic instability: immediate pelvic binder at trochanters - do NOT wait for X-ray
- •Blood at urethral meatus: do NOT catheterize - retrograde urethrogram first
- •APC-II confirmed: symphysis plating alone sufficient (posterior intact)
- •APC-III confirmed: both anterior (plate) AND posterior (SI screws) fixation
Exam Mnemonics
- •BOOK: Binder immediately, Opens ring, Opens from external rotation, Key threshold 2.5cm
- •VOLUME: Volume expands, Opens retroperitoneum, Lost tamponade, Uncontrolled venous bleeding, Massive transfusion, Early binder saves lives
- •CLOSE: Circumferential application, Level of trochanters, Opens becomes closed, Snug not tight, Early application
- •APC: Anterior opens, Posterior determines stability, CT to classify
Common Pitfalls
- •Waiting for X-ray before applying binder
- •Applying binder at iliac crests (too high - ineffective)
- •Blind urethral catheterization with blood at meatus
- •Treating APC-III with anterior fixation alone
- •Not assessing posterior ligament status on CT
Exam Day Tips
- •Open book = APC-II = external rotation = HIGHEST hemorrhage risk
- •2.5cm (25mm) symphysis widening is THE threshold to remember
- •Binder at TROCHANTERS closes the book (NOT iliac crests)
- •Posterior ligaments determine if anterior fixation alone is enough
- •80% venous bleeding - binder helps most; 20% arterial needs angio