Energy transfer | Neurovascular status | Joint involvement | Debridement strategy
- Do not judge severity by skin wound size. A small entry wound can hide fracture comminution, vascular injury or compartment syndrome.
- Energy transfer is the key concept. Velocity, yaw, fragmentation, tissue resistance and bone strike determine tissue damage.
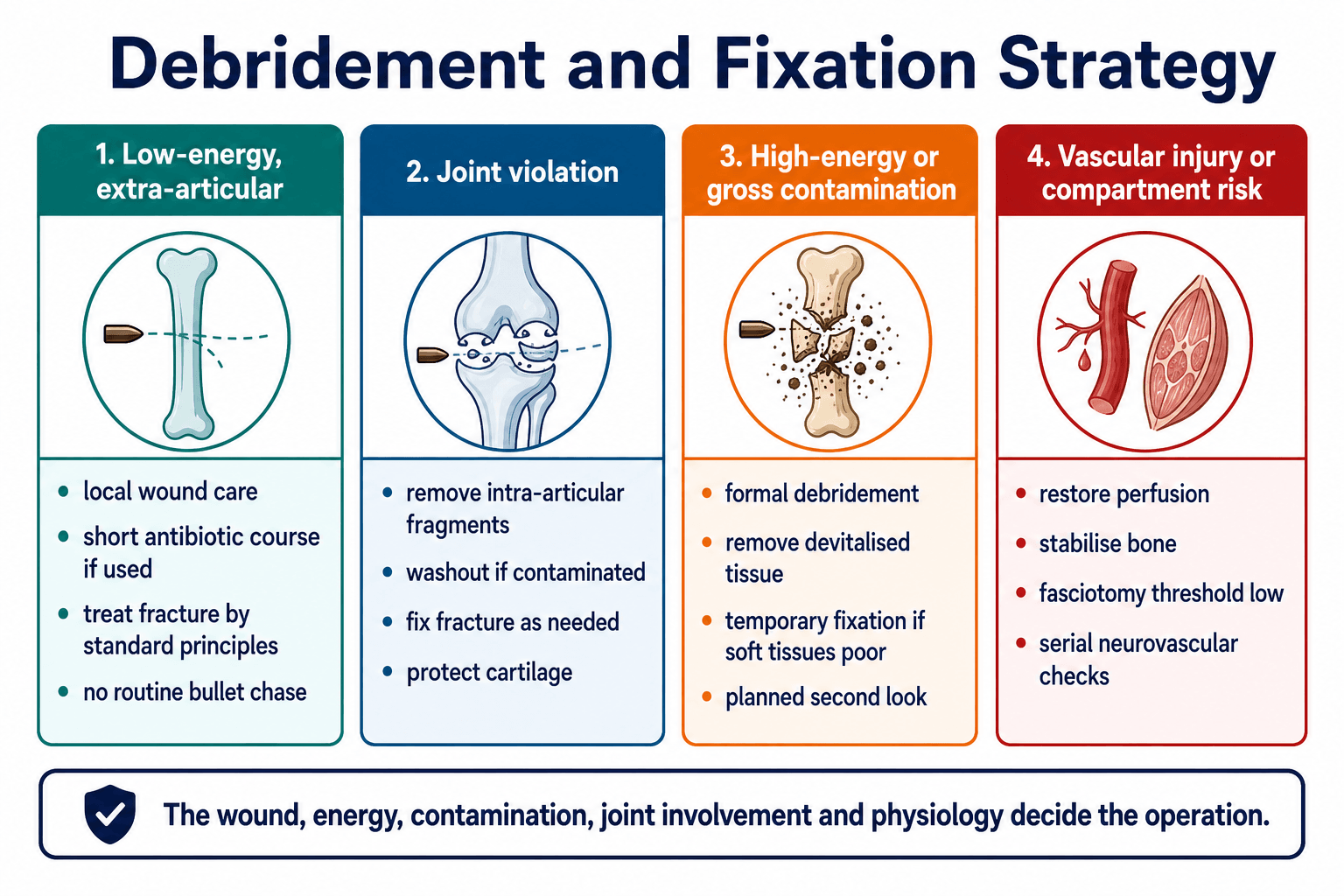
- Low-energy extra-articular fractures are not automatically massive open-fracture operations. They are often managed like the equivalent closed fracture with appropriate wound care.
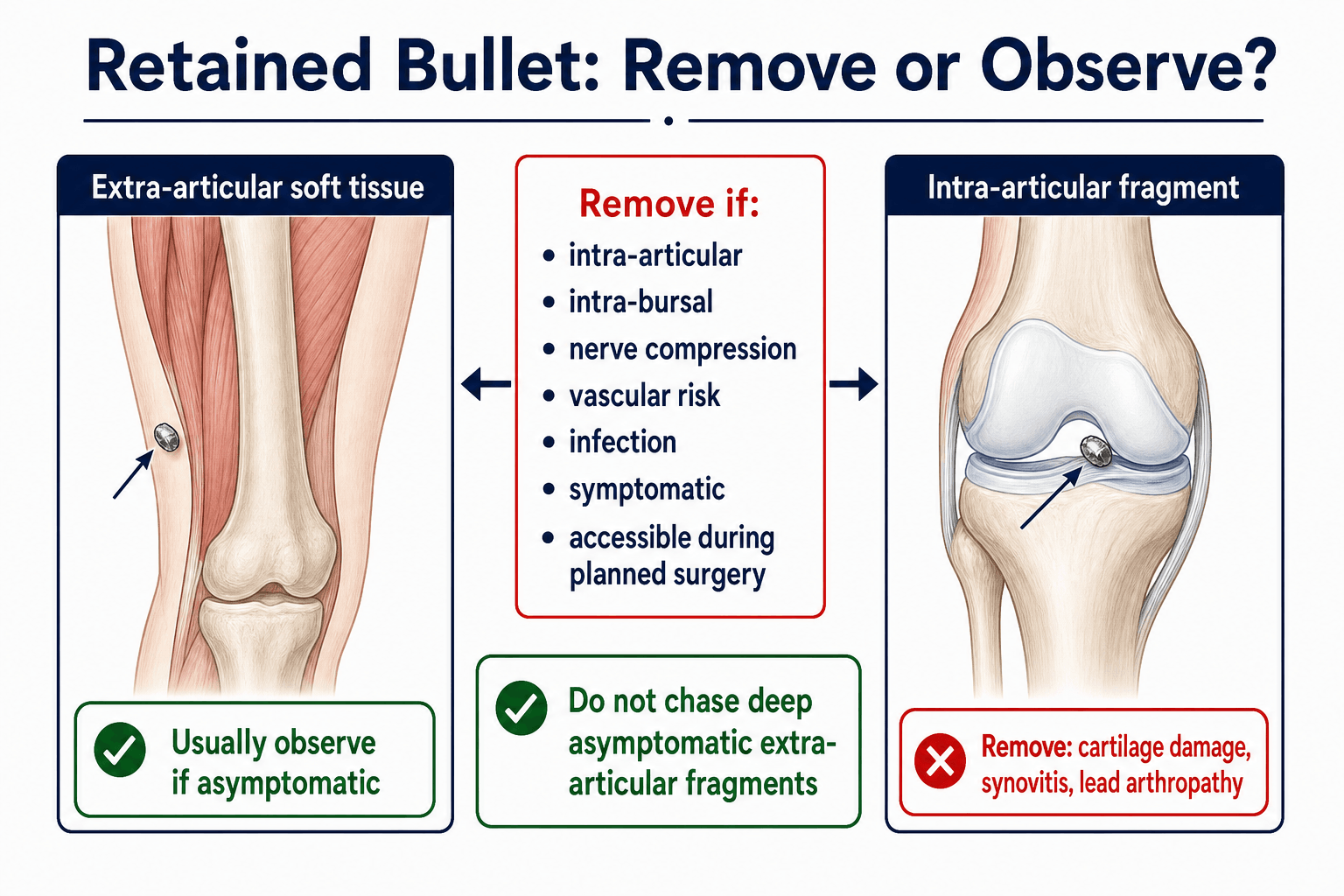
- Intra-articular bullets should be removed. Synovial fluid exposes lead and cartilage to ongoing chemical and mechanical injury.
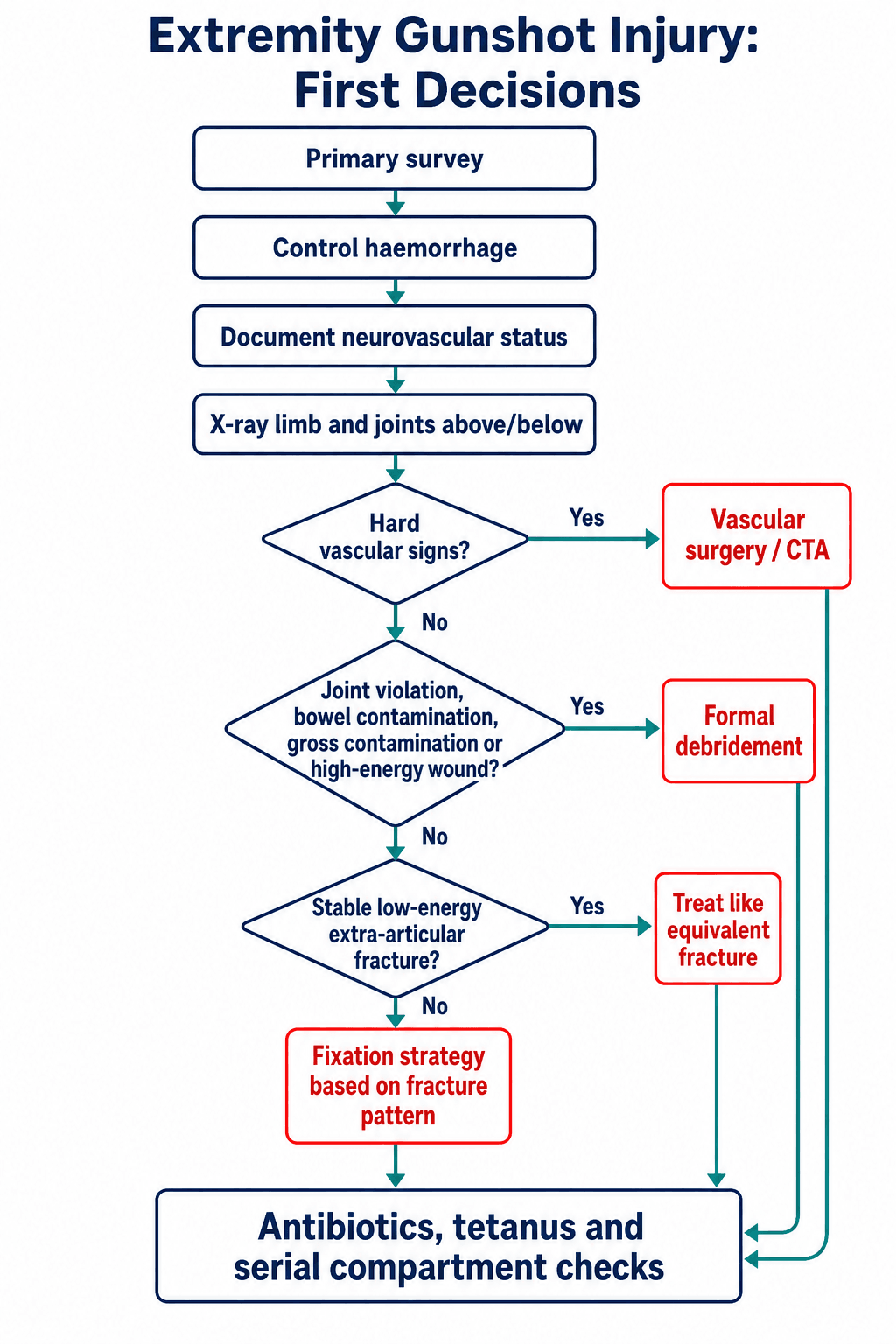
- Hard vascular signs change the sequence. Perfusion and haemorrhage control take priority over definitive fracture fixation.
- High-energy or contaminated wounds need formal debridement and staged reconstruction. Do not close them primarily when tissue viability is uncertain.
- “The safe first sentence is: assess the patient, limb perfusion, neurological status, wound energy, contamination, joint involvement and fracture stability.
- “The orthopaedic decision is not 'bullet equals open fracture protocol for everything'; it is energy, contamination, joint violation and stability.
- “Routine removal of deep asymptomatic extra-articular fragments can cause more damage than observation.
- “A fracture with vascular repair has a low threshold for prophylactic fasciotomy, especially after ischaemia or reperfusion.
Do not be reassured by palpable pulses alone. Document motor, sensory, capillary refill, Doppler signals and ankle-brachial index when appropriate; obtain vascular imaging or direct vascular surgery input when hard signs or abnormal perfusion are present.
- Finding That Matters
- Major haemorrhage, shock, airway or chest/abdominal injury.
- Action
- Primary survey, haemorrhage control and trauma resuscitation before fracture detail.
- Finding That Matters
- Absent pulses, expanding haematoma, bruit, thrill, active bleeding or ischaemic limb.
- Action
- Vascular surgery, CTA when appropriate, temporary shunt or repair with bone stabilisation.
- Finding That Matters
- Trajectory through a joint, intra-articular gas or fragments, haemarthrosis or synovial wound.
- Action
- Remove intra-articular fragments and wash out contaminated joints.
- Finding That Matters
- Small wound, limited contamination, stable patient, fracture behaves like standard pattern.
- Action
- Treat fracture by standard principles; do not chase deep asymptomatic bullet fragments.
- Finding That Matters
- Large tissue defect, fragmentation, devitalised muscle, delayed presentation, bowel/farm/water contamination.
- Action
- Formal debridement, staged fixation, second look and soft tissue planning.
SHOTInitial Assessment | BALLWhat Changes Treatment | FIREOperative Priorities |
|---|---|---|
S Survey Primary survey and haemorrhage control first. | B Bone stability Fix the fracture by standard mechanical principles. | F Fixation Temporary or definitive, depending physiology and soft tissues. |
H Haemorrhage Control bleeding and identify vascular hard signs. | A Artery Perfusion sequence overrides definitive fixation. | I Irrigation Formal washout when joint, contamination or high-energy injury exists. |
O Open joint Joint violation changes washout and fragment removal. | L Lead in joint Intra-articular fragments should be removed. | R Remove dead tissue Debride devitalised muscle, bone and foreign material that matters. |
T Tissues Energy and devitalisation decide debridement. | L Local contamination Bowel, farm, water or delayed contamination escalates debridement. | E Expect swelling Low threshold for fasciotomy when vascular or crush risk exists. |
Do not start by chasing the bullet. | The projectile matters less than what it did. | Match the operation to the wound. |
Overview
Gunshot wounds produce orthopaedic problems through penetrating soft tissue injury, fracture, contamination, vascular injury, nerve injury, compartment syndrome and retained foreign material. The visible wound is only the entry point. The injury that matters is the tissue damage along the projectile path and the zone of energy transfer around it.
Treat the patient and limb first, then the projectile. The operation is decided by physiology, perfusion, tissue viability, contamination, joint involvement and fracture stability.
Why this topic matters
Civilian gunshot wounds range from low-energy soft tissue wounds to comminuted open fractures with vascular injury.
Over-treatment causes unnecessary tissue damage; under-treatment misses joints, vessels, compartments and contamination.
Missed infection, nonunion, nerve injury, vascular compromise and intra-articular lead can produce major disability.
Practical language
Avoid describing a wound simply as "a gunshot fracture." Use a more useful description:
- Low-energy or high-energy mechanism.
- Extra-articular or intra-articular path.
- Clean, contaminated or delayed presentation.
- Stable or unstable fracture.
- Normal or abnormal neurovascular status.
- Isolated limb injury or polytrauma.
- Retained fragment location and whether it matters.
Anatomy and Biomechanics
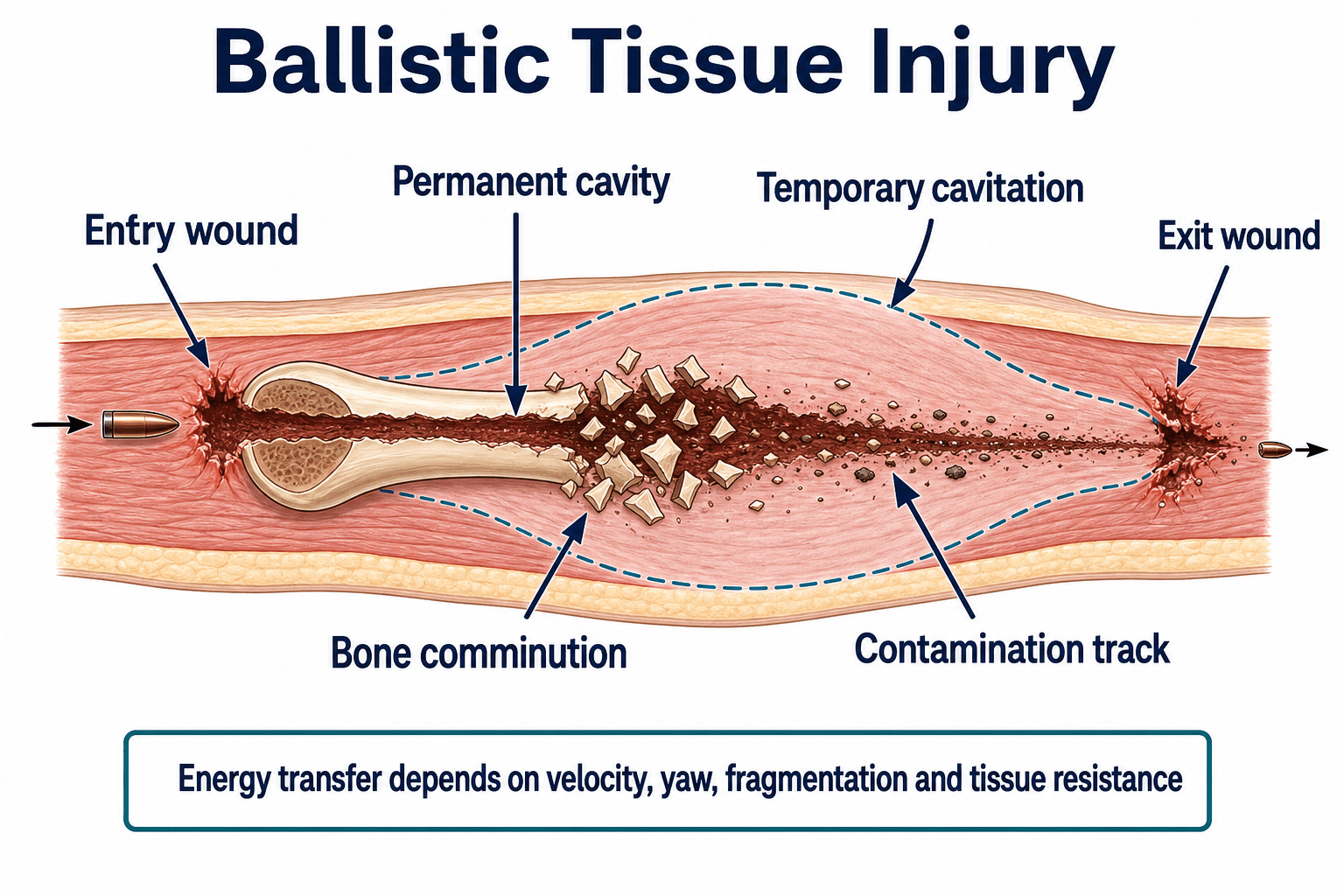
Permanent cavity
The permanent cavity is the direct tissue track made by the projectile and fragments. It is produced by crushing, cutting and shearing. It determines the true contaminated track and the structures that may be disrupted.
Temporary cavitation
Temporary cavitation is radial tissue stretch around the projectile path. It is more important in high-energy wounds, fragmenting projectiles and tissues that do not tolerate stretch well. Muscle may recover if viable; vessels, nerves and inelastic compartments may not.
Bone strike
When a projectile hits bone:
- Energy transfer rises abruptly.
- Bone becomes secondary missiles.
- Comminution and segmental defects may occur.
- The wound may behave more like a high-energy open fracture even if the skin wounds look small.
- Compartment syndrome and vascular injury risk increase.
Low-energy versus high-energy
- Low-Energy Civilian Pattern
- Handgun-type, lower velocity, often limited cavitation.
- High-Energy / Military / Blast Pattern
- Rifle, fragmentation, blast, shotgun at close range or high-energy transfer.
- Low-Energy Civilian Pattern
- Often narrow wound track with limited devitalisation.
- High-Energy / Military / Blast Pattern
- Wide zone of devitalised and contaminated tissue.
- Low-Energy Civilian Pattern
- May be treated like the equivalent non-gunshot fracture if extra-articular and clean.
- High-Energy / Military / Blast Pattern
- Often needs formal debridement, staged fixation and soft tissue reconstruction.
- Low-Energy Civilian Pattern
- Selective; no routine deep bullet chase.
- High-Energy / Military / Blast Pattern
- Formal; remove non-viable tissue and plan second look.
- Low-Energy Civilian Pattern
- Depends on wound and contamination.
- High-Energy / Military / Blast Pattern
- Avoid primary closure when viability is uncertain.
Velocity is important because kinetic energy rises with the square of velocity, but tissue damage is determined by the energy actually transferred into the limb. Yaw, fragmentation, bone strike and tissue resistance all matter.
Classification
Classify the injury in a way that changes treatment. Weapon labels alone are less helpful than tissue behaviour.
- Features
- Limited soft tissue injury, small wound track, often handgun-type civilian injury.
- Treatment Meaning
- May be managed like equivalent fracture if extra-articular and clean.
- Features
- Large temporary cavity, devitalised tissue, bone fragmentation, blast or rifle-type transfer.
- Treatment Meaning
- Formal debridement, staged care and soft tissue planning.
- Features
- Variable; close-range injuries can be devastating with pellets, wad and broad contamination.
- Treatment Meaning
- Treat by tissue destruction and contamination, not by the word shotgun alone.
- Features
- Penetrating fragments plus crush, burns, contamination and systemic trauma.
- Treatment Meaning
- Damage-control principles and repeated debridement are common.
Clinical Assessment
History
The history should clarify:
- Time of injury and time to antibiotics.
- Weapon type if known, distance, number of shots and whether shotgun or blast was involved.
- Environment: street, farm, water, soil, clothing, shoe or bowel contamination.
- Immediate bleeding, tourniquet use, transient limb ischaemia or prehospital reduction.
- Numbness, weakness, severe pain, progressive swelling or increasing analgesia requirement.
- Tetanus status, allergies, anticoagulation, diabetes, smoking and immunosuppression.
Do not rely on the patient's description of calibre or velocity to decide treatment. Use the clinical wound, imaging and tissue findings.
Examination
- What to Document
- Entry and exit wounds, soft tissue loss, contamination, swelling, deformity, expanding haematoma.
- Why It Matters
- Defines wound energy and urgent vascular concern.
- What to Document
- Compartments, bony tenderness, crepitus, temperature and capillary refill.
- Why It Matters
- Tense compartments and cool limb change urgency.
- What to Document
- Active motor function before reduction or anaesthesia.
- Why It Matters
- Baseline nerve function may be lost later if not recorded.
- What to Document
- Named motor and sensory testing relevant to the region.
- Why It Matters
- Ballistic nerve injuries can be neuropraxia, partial laceration or complete transection.
- What to Document
- Pulses, Doppler signals, ABI/API, capillary refill and hard signs.
- Why It Matters
- Determines CTA, exploration, shunt or repair.
- What to Document
- Trajectory across joint, haemarthrosis, intra-articular air or fragment.
- Why It Matters
- Changes removal and washout decisions.
Hard vascular signs
Hard signs include pulsatile bleeding, expanding haematoma, bruit or thrill, absent distal perfusion, ischaemic limb and rapidly progressive neurological deficit from ischaemia. These findings require immediate vascular decision-making rather than delayed outpatient fracture review.
Compartment syndrome risk
Gunshot wounds can cause compartment syndrome through fracture bleeding, vascular injury, reperfusion, swelling, crush, tight dressings or delayed presentation. Pain with passive stretch, tense compartments and increasing analgesic requirement remain important, but obtunded or intubated patients need pressure measurement and proactive monitoring.
Normal pulses do not exclude compartment syndrome, and a normal pulse can coexist with a major venous injury, intimal arterial injury or evolving swelling.
Differential diagnosis of the painful, swollen gunshot limb
A small skin wound can hide several time-critical diagnoses. The differential is really a question of which limb-threatening process is driving the pain and swelling.
- Discriminating Features
- Hard signs: pulsatile bleeding, expanding haematoma, bruit, thrill, absent distal pulses, cool pale ischaemic limb.
- Key Test
- Examination plus ABI; CTA if signs equivocal.
- First Action
- Vascular surgery, haemorrhage control, shunt or repair with bone stabilisation.
- Discriminating Features
- Pain out of proportion, pain on passive stretch, tense compartments, escalating analgesia; pulses often present.
- Key Test
- Serial examination; compartment pressures if obtunded.
- First Action
- Urgent fasciotomy; do not wait for pulselessness.
- Discriminating Features
- Trajectory across a joint, effusion, intra-articular gas or fragment, especially after a bowel-traversing path.
- Key Test
- Imaging for joint violation; treat as septic arthritis if missile crossed large bowel.
- First Action
- Washout, fragment removal and joint-appropriate antibiotics.
- Discriminating Features
- Delayed presentation, fever, spreading erythema, purulent or malodorous drainage.
- Key Test
- Deep operative cultures (superficial swabs are inferior).
- First Action
- Debridement and targeted antibiotics.
- Discriminating Features
- Low-energy, extra-articular, normal perfusion, soft compartments, no contamination.
- Key Test
- Clinical assessment and orthogonal radiographs.
- First Action
- Local wound care, tetanus and selective antibiotics; observe deep asymptomatic fragments.
Imaging and Investigations
Plain radiographs
Order orthogonal X-rays of:
- The injured bone or region.
- The joint above and below when a long bone is involved.
- Adjacent joints when the trajectory is near a joint.
- The pelvis or abdomen when the bullet path may be transpelvic.
On X-ray, assess:
- Fracture pattern, comminution, segmental bone loss and cortical violation.
- Retained fragment location: intra-articular, intra-bursal, extra-articular soft tissue, within bone or near a neurovascular bundle.
- Intra-articular gas or haemarthrosis clues.
- Bullet fragmentation, which suggests higher energy transfer.
- Foreign material and clothing debris when visible.
CT
CT is useful for:
- Intra-articular fracture extension.
- Pelvis, acetabulum, foot, ankle, hand or complex periarticular injuries.
- Retained fragment localisation when removal is planned.
- Bone loss and fixation planning.
- Transpelvic trajectory and associated visceral concern.
CTA and vascular studies
CTA is indicated when perfusion is abnormal, ABI/API is abnormal, hard or soft vascular signs exist, or the projectile path is close to a major vessel with concerning findings. Do not delay direct vascular surgery for a clearly ischaemic limb when the diagnosis is clinically obvious.
Laboratory tests
Blood tests depend on severity. Consider:
- Full blood count and group/crossmatch in major trauma.
- Creatine kinase, renal function and urine myoglobin if crush, ischaemia or compartment risk.
- Inflammatory markers are not useful for the acute decision but may help delayed infection follow-up.
- Baseline blood lead level when a retained fragment is intra-articular, intra-bursal, multiple, symptomatic or long-standing.
Management Algorithm
Immediate measures
Initial measures should be done in parallel with trauma resuscitation:
- Control external haemorrhage with direct pressure, haemostatic dressing or tourniquet when needed.
- Photograph wounds before theatre when practical, then cover with sterile dressing.
- Splint the limb in a position that protects soft tissue and neurovascular structures.
- Give analgesia.
- Give tetanus prophylaxis according to immunisation status and wound risk.
- Give antibiotics according to wound severity, contamination, joint involvement and local protocol.
- Do not probe the wound blindly in the emergency department.
Surgical Technique
This section describes operative principles rather than one universal operation. The correct operation depends on the limb region, wound, fracture and associated injuries.
Formal debridement
- Confirm patient identity, limb, imaging, antibiotics, tetanus status and vascular plan.
- Position to allow access to entry wound, exit wound, fracture and potential vascular repair.
- Prep widely; include adjacent joints if the trajectory may involve them.
- Extend wounds only as needed for safe exposure and debridement.
- Identify the projectile track, but do not tunnel blindly through healthy tissue.
- Excise non-viable skin and subcutaneous tissue.
- Assess muscle using colour, consistency, contractility and capacity to bleed.
- Remove loose dead bone, gross debris, clothing fragments and heavily contaminated foreign material.
- Preserve bone and soft tissue required for reconstruction when viable.
- Irrigate with low-pressure fluid; avoid tissue-destructive high-pressure lavage.
- Obtain deep cultures if infection is suspected or delayed presentation is infected.
- Stabilise the fracture in a way that protects soft tissue access.
- Leave wounds open or use temporary coverage when viability is uncertain.
- Plan second look and reconstruction early.
Retained Bullet Fragments
Remove
Remove or strongly consider removal when the fragment is:
- Intra-articular.
- Intra-bursal or in a synovial sheath.
- Causing nerve compression.
- Threatening a vessel or repair.
- Infected or associated with abscess.
- Symptomatic and safely accessible.
- Encountered during planned exposure without added morbidity.
- In the palm, sole or other pressure-bearing region where it causes functional symptoms.
Observe
Observation is reasonable when:
- The fragment is deep, extra-articular and asymptomatic.
- Removal would require extensive dissection through healthy tissue.
- There is no infection, nerve compression, vascular risk or joint communication.
- The fragment is within soft tissue and not causing mechanical symptoms.
Lead arthropathy
Lead dissolves more readily in synovial fluid than in inert soft tissue. Retained intra-articular fragments can cause synovitis, cartilage damage, radiographic lead deposition, systemic lead toxicity and secondary arthritis. Symptoms may appear years later.
Follow-up considerations:
- Ask about pain, swelling, stiffness, fatigue, abdominal symptoms, neuropathy and cognitive symptoms when retained intra-articular fragments are known.
- Check blood lead level for intra-articular, intra-bursal, multiple or symptomatic retained fragments.
- Coordinate medical toxicology or physician input for elevated levels or systemic symptoms.
The removal list above names an "intravascular" fragment, but the entity behind it - bullet embolism - is a classic trap worth holding explicitly:
- When to suspect it: an entry wound with no exit wound and no projectile where the trajectory predicts, or a bullet that has moved between serial films. The missile has entered a vessel and embolised.
- Venous bullet embolism: the fragment travels with venous return toward the right heart and pulmonary circulation - it can lodge in the right ventricle or a pulmonary artery and cause arrhythmia, valvular injury or pulmonary infarction; paradoxical (arterial) embolism is possible with a septal defect.
- Arterial bullet embolism: the fragment lodges distally and causes limb (or organ) ischaemia - pulse deficit distal to a proximal wound is the clue.
- Action: if the bullet is "lost", image to find it (radiographs of chest/abdomen/limb, CT/CTA, echo) before assuming it is simply retained in soft tissue. Retrieve embolised bullets that cause ischaemia, are intracardiac/intravascular with embolic risk, or are symptomatic (endovascular retrieval or open) - do not leave a migratory intravascular missile.
Exam point: a gunshot with an entry wound but no exit and no bullet on the expected film is bullet embolism until proven otherwise - search the heart/lungs (venous) or the distal limb (arterial), and retrieve a migratory intravascular fragment.
The topic correctly says to monitor blood lead, but the clinical syndrome of lead toxicity (plumbism) and its treatment are never stated - and that is what the surveillance is for:
- Clinical features: abdominal colic and constipation, anaemia (microcytic/normocytic) with basophilic stippling of red cells, peripheral motor neuropathy (classically wrist/foot drop), fatigue, a gingival "lead line", nephropathy, and at high levels encephalopathy (especially in children).
- The orthopaedic link: retained fragments in synovial fluid (intra-articular/intra-bursal) dissolve and raise blood lead far more than inert soft-tissue fragments; multiple fragments and an associated fracture also raise risk - hence the surveillance thresholds.
- Management - the source matters: confirm with blood lead level; for symptomatic toxicity or high levels use chelation (oral DMSA/succimer, or IV calcium-EDTA, with dimercaprol/BAL added in encephalopathy) - but the decisive orthopaedic point is that chelation gives only temporary control while the lead source remains, so the retained fragment (especially intra-articular) must be removed to achieve definitive cure.
Exam point: know plumbism (colic, anaemia with basophilic stippling, wrist drop, lead line, encephalopathy) as the consequence of retained lead; chelate symptomatic/high levels (DMSA or EDTA, BAL in encephalopathy) but remove the fragment source because chelation alone does not cure an ongoing intra-articular lead depot.
Region-Specific Traps
- Do Not Miss
- Intra-articular fragments, nerve injury, vascular proximity.
- Practical Point
- CT helps locate fragments; arthroscopy may remove selected joint fragments.
- Do Not Miss
- Compartment syndrome, nerve injury, unstable both-bone mechanics.
- Practical Point
- Assess median, ulnar, radial and AIN/PIN function before anaesthesia.
- Do Not Miss
- Tendon, nerve, vessel, joint and contamination in a small volume.
- Practical Point
- Low-calibre does not mean low-risk in the hand.
- Do Not Miss
- Bowel, rectal, bladder, urethral, vascular and intra-articular contamination.
- Practical Point
- Trajectory and visceral injury decide antibiotics and debridement.
- Do Not Miss
- Vascular injury, compartment syndrome, comminution, nonunion.
- Practical Point
- Treat fracture mechanically, but respect soft tissues and perfusion.
- Do Not Miss
- Contamination from shoe, small compartments, joint violation, retained fragments in sole.
- Practical Point
- Do not underestimate infection and compartment risk.
Complications and Follow-Up
Haemorrhage, vascular thrombosis, compartment syndrome, missed nerve injury, wound contamination and acute infection.
Deep infection, fixation failure, delayed union, nonunion, stiffness, neuropathic pain and soft tissue breakdown.
Lead arthropathy, systemic lead toxicity, chronic osteomyelitis, post-traumatic arthritis, malunion and complex regional pain.
Follow-up priorities
- Recheck wound within the timeframe appropriate for contamination and surgery.
- Repeat neurovascular examination.
- Continue compartment vigilance while swelling evolves.
- Monitor fracture alignment and union.
- Review cultures and adjust antibiotics when infection is present.
- Start early motion when fixation and soft tissues permit.
- Counsel on smoking cessation, diabetes optimisation and return precautions.
- Monitor retained intra-articular or symptomatic fragments.
Red flags after discharge
Patients should return urgently for:
- Increasing pain out of proportion.
- Increasing swelling or tight compartments.
- Numbness, weakness or cold limb.
- Fever, spreading redness, pus or foul odour.
- New drainage after an initially dry wound.
- Worsening joint pain when a fragment may be intra-articular.
Postoperative Care
Postoperative care depends on the wound and fixation, but the same priorities recur.
- What to Do
- Document pulses, Doppler signals, capillary refill, motor and sensory function after surgery.
- Why
- Detects vascular thrombosis, nerve deterioration and compartment syndrome.
- What to Do
- Repeat examinations and measure pressures when examination is unreliable.
- Why
- Gunshot fractures with vascular injury or reperfusion remain high risk.
- What to Do
- Schedule dressing review, second look, delayed closure, graft or flap timing.
- Why
- Soft tissue failure is a major driver of infection and nonunion.
- What to Do
- Stop prophylaxis when appropriate; continue targeted therapy only for established infection or high-risk contamination.
- Why
- Prevents unnecessary prolonged antibiotics while treating real infection.
- What to Do
- Begin joint motion when fixation and soft tissues allow.
- Why
- Stiffness is common after periarticular and upper-limb gunshot injuries.
Follow-up schedule
- Early wound review for high-risk, contaminated or surgically treated wounds.
- Radiographs to confirm alignment and progression to union.
- Review cultures and histology when debridement was performed.
- Lead monitoring for retained intra-articular, intra-bursal, multiple or symptomatic fragments.
- Hand therapy, splinting or physiotherapy when tendons, joints or nerves are involved.
Outcomes and Prognosis
Outcome depends more on tissue injury and associated structures than on the bullet itself.
Low-energy, extra-articular, clean wound, stable fracture, normal neurovascular status and reliable follow-up.
High-energy transfer, vascular injury, compartment syndrome, bone loss, joint injury, infection, smoking and poor soft tissue cover.
Nerve injury, stiffness, chronic infection, nonunion and post-traumatic arthritis may dominate function even after fracture union.
Prognostic factors to state clearly
- Energy and tissue devitalisation.
- Time to antibiotics and debridement when contamination is significant.
- Vascular injury and ischaemia duration.
- Need for fasciotomy.
- Joint surface injury.
- Bone defect size and fixation stability.
- Patient factors: smoking, diabetes, immunosuppression, nutrition and adherence.
Common Pitfalls
Chasing a deep asymptomatic extra-articular bullet can injure nerves, vessels and soft tissue without benefit.
Missing joint violation, bowel contamination, vascular injury or compartment syndrome can be limb-threatening.
Low-energy evidence does not justify ignoring contamination, operative fixation, delayed infection or high-energy tissue loss.
Closing high-energy or contaminated wounds before tissue viability is clear increases infection risk.
Guidelines, Registries & Global Practice
Global epidemiology and practice variation
The burden of ballistic limb trauma is extremely unevenly distributed. Civilian gunshot violence is concentrated in specific high-incidence regions — parts of the Americas and southern Africa carry a disproportionate share of orthopaedic ballistic workload, and centres such as the OrthoBallistics group in Cape Town manage volumes rarely seen elsewhere. By contrast, in the United Kingdom, much of Europe and Australasia, civilian gunshot injury is comparatively uncommon, so the largest published high-energy experience is military and is reported through defence trauma systems. This drives a real practice gap: a low-energy handgun fracture is the everyday lesion in high-incidence civilian settings, whereas blast and high-velocity rifle wounds dominate the military literature and shape much of the published surgical doctrine.
A recurring methodological problem, emphasised by the Cape Town group (according to PubMed, Maqungo et al., Injury 2020, DOI), is that the field is scientifically under-represented: high loss to follow-up and poor compliance in affected populations make high-quality prospective evidence scarce, so most guidance rests on Level III to V data and expert consensus.
Side-by-side guideline and doctrine comparison
There is no single international gunshot-fracture guideline; instead, principles are drawn from open-fracture and trauma-system standards applied to the ballistic wound.
- Position Relevant to Gunshot Wounds
- High-energy or contaminated ballistic wounds follow open-fracture standards: early antibiotics, senior orthoplastic assessment, debridement of devitalised tissue and combined skeletal-soft-tissue reconstruction; avoid premature closure.
- Evidence Basis
- National standard / consensus.
- Position Relevant to Gunshot Wounds
- Stratify by energy: low-velocity extra-articular fractures may be treated like equivalent closed fractures; remove intra-articular bullets; reserve extensive debridement for high-energy or contaminated wounds.
- Evidence Basis
- Review-level, mostly Level III-IV.
- Position Relevant to Gunshot Wounds
- Apply standard fracture-fixation mechanics once contamination and soft tissues are controlled; favour temporary external fixation and staged care for severe contamination or poor soft-tissue envelope.
- Evidence Basis
- Educational consensus.
- Position Relevant to Gunshot Wounds
- High-velocity and blast wounds: haemorrhage control first, never close primarily, repeated debridement and planned reconstruction; liberal damage-control and shunting.
- Evidence Basis
- Combat-casualty series.
- Position Relevant to Gunshot Wounds
- Wound excision, delayed primary closure and tetanus prophylaxis form the backbone where staged reconstruction and imaging may be limited.
- Evidence Basis
- Field experience / guidance.
Registry and surveillance evidence
There is no dedicated international gunshot-fracture implant registry. Relevant population-level data instead come from national trauma registries and injury surveillance systems — for example the Australian and New Zealand trauma registries, the UK Trauma Audit and Research Network (TARN), and the US National Trauma Data Bank — which capture mechanism, injury severity and outcome but not bullet-specific decisions. Vascular-imaging practice has been validated in this registry-style way: an Australian major trauma centre series confirmed that CTA is the accurate first-line vascular study yet rarely changes management when no clinical signs are present (according to PubMed, Joseph et al., Injury 2021, DOI).
Applying this locally (Australia)
- Use a major trauma pathway for unstable patients and high-energy wounds, with early multidisciplinary involvement (orthopaedics, vascular surgery, plastic surgery, emergency medicine, intensive care, infectious diseases and rehabilitation).
- Antibiotic choice should follow eTG antimicrobial guidance and the hospital open-fracture policy rather than a fixed international recipe; tetanus assessment is part of every penetrating wound plan.
- Document neurovascular status, wound appearance, antibiotics, tetanus decision, splinting, imaging and serial compartment checks clearly.
- For retained intra-articular, multiple or symptomatic fragments, or any lead-toxicity concern, coordinate blood lead surveillance with physicians, toxicology or infectious diseases according to local service availability.
Clinical management should be based on injury severity, patient physiology, local trauma pathways and available specialist services, recognising that civilian and military ballistic patterns differ markedly between regions.
MCQ Practice Points
Q: Does every low-energy extra-articular gunshot fracture need wide operative debridement? A: No. Many can be treated like the equivalent fracture with local wound care and appropriate antibiotic/tetanus decisions.
Q: Which retained bullet fragments should be removed? A: Intra-articular, intra-bursal, infected, symptomatic, neurovascularly threatening or accessible fragments during planned surgery.
Q: What is the key determinant of tissue destruction? A: Energy transferred into the tissue, influenced by velocity, yaw, fragmentation, bone strike and tissue resistance.
Q: Why is fasciotomy considered after vascular repair? A: Ischaemia and reperfusion increase compartment syndrome risk, especially with fracture, swelling and prolonged ischaemia.
Applied Scenarios
Practise clinical reasoning and management decisions out loud
“A stable adult has a small entry and exit wound, normal neurovascular examination and an extra-articular tibial shaft fracture after a handgun injury.”
“A patient has a gunshot wound crossing the knee with a retained metallic fragment visible inside the joint.”
“A patient has a comminuted femoral fracture with a large soft tissue defect, devitalised muscle and gross contamination after a high-energy projectile injury.”
“A patient with a gunshot fracture around the distal femur has an ischaemic foot and expanding popliteal fossa haematoma.”
Start with
- Primary survey and haemorrhage control.
- Neurovascular status before anaesthesia.
- Entry, exit, contamination, joint path and fracture stability.
Image
- Orthogonal X-rays of limb and adjacent joints.
- CT for joint, pelvis, complex fracture or fragment localisation.
- CTA for hard or soft vascular signs, abnormal ABI/API or concerning trajectory.
Operate for
- High-energy devitalised tissue.
- Gross contamination, delayed infected wounds or bowel contamination.
- Joint violation with retained intra-articular fragments.
- Unstable fractures needing standard fixation.
- Vascular injury or compartment syndrome.
Do not
- Judge severity by skin wound size alone.
- Chase deep asymptomatic extra-articular fragments.
- Close high-energy contaminated wounds primarily.
- Ignore compartment syndrome because pulses are present.
Evidence Base
Management of Civilian Low-Velocity Gunshot Injuries to an Extremity
- Most low-velocity gunshot-induced extremity fractures can be managed similarly to equivalent non-gunshot fractures, with goals of restoring function and minimising complications.
- Intra-articular retained bullets should be removed; routine prophylactic irrigation and debridement of a transarticular bullet track is not warranted purely for infection prevention.
- Evidence supporting prophylactic antibiotics in non-operatively treated wounds is limited; most literature is Level III or IV.
Gunshot Injuries to the Lower Extremities: Issues, Controversies and Algorithm of Management
- Proposes conservative management of soft-tissue-only wounds and of incomplete (non-displaced) tibial or femoral shaft fractures, with fixation of all complete fractures and prophylactic fixation of incomplete peritrochanteric fractures.
- All intra-articular projectiles should be removed.
- A joint should be treated as septic arthritis only when the missile traverses large bowel (not small bowel) before entering the joint capsule.
- Evidence remains scarce and limited by high loss to follow-up in this population.
Reference Links
- Jabara JT, Gannon NP, Vallier HA, Nguyen MP. Management of civilian low-velocity gunshot injuries to an extremity. PubMed
- Maqungo S, Kauta N, Held M, et al. Gunshot injuries to the lower extremities: issues, controversies and algorithm of management. PubMed
- Sathiyakumar V, Thakore RV, Stinner DJ, et al. Gunshot-induced fractures of the extremities: a review of antibiotic and debridement practices. PubMed
- Papasoulis E, Patzakis MJ, Zalavras CG. Antibiotics in the treatment of low-velocity gunshot-induced fractures: a systematic literature review. PubMed
- Penn-Barwell JG, Brown KV, Fries CA. High velocity gunshot injuries to the extremities: management on and off the battlefield. PubMed
- Omid R, Stone MA, Zalavras CG, Marecek GS. Gunshot wounds to the upper extremity. PubMed
- Sclafani SJ, Vuletin JC, Twersky J. Lead arthropathy: arthritis caused by retained intra-articular bullets. PubMed
- deSouza IS, Benabbas R, McKee S, et al. Accuracy of physical examination, ankle-brachial index and ultrasonography in the diagnosis of arterial injury in penetrating extremity trauma: a systematic review and meta-analysis. PubMed
- Joseph TI, Ratnakanthan PJ, Paul E, Clements W. Utility of computed tomography angiography in traumatic lower limb injury: review of clinical impact in a level 1 trauma centre. PubMed
- Nickel WN, Steelman TJ, Sabath ZR, Potter BK. Extra-articular retained missiles: is surveillance of lead levels needed? PubMed