Matrix Synthesis | Mineralization Control | Runx2 Master Regulator | Wnt and BMP Signaling
- Runx2 (Cbfa1) is the master transcription factor - essential for osteoblast differentiation
- Wnt/β-catenin signaling promotes osteoblast differentiation and bone formation
- Alkaline phosphatase hydrolyzes pyrophosphate (mineralization inhibitor) to enable mineralization
- Osteoblasts produce osteoid (unmineralized matrix) with 10-14 day lag before mineralization
- Mature osteoblasts become osteocytes (embedded), lining cells (quiescent), or undergo apoptosis
- “Osteoblast differentiation requires Runx2 and osterix transcription factors
- “BMP-2 and BMP-7 are potent osteoinductive growth factors
- “Sclerostin (from osteocytes) inhibits Wnt signaling to reduce bone formation
- “Parathyroid hormone has anabolic effect when given intermittently (stimulates osteoblasts)
Runx2 (Cbfa1) is the master transcription factor for osteoblast differentiation. Runx2 knockout mice have no osteoblasts and no bone formation. Cleidocranial dysplasia is caused by RUNX2 haploinsufficiency.
Wnt signaling promotes osteoblast differentiation and function. Sclerostin (SOST gene) inhibits Wnt by binding LRP5/6 co-receptors. Anti-sclerostin antibodies (romosozumab) are anabolic bone agents.
Alkaline phosphatase (ALP) is the osteoblast marker enzyme. It hydrolyzes pyrophosphate (mineralization inhibitor) allowing hydroxyapatite crystal formation. Hypophosphatasia (ALP deficiency) causes defective mineralization.
Osteoblasts synthesize type I collagen (90% of matrix) and non-collagenous proteins (osteocalcin, osteopontin, BSP). Osteoid is unmineralized matrix with 10-14 day mineralization lag time.
Overview and Introduction
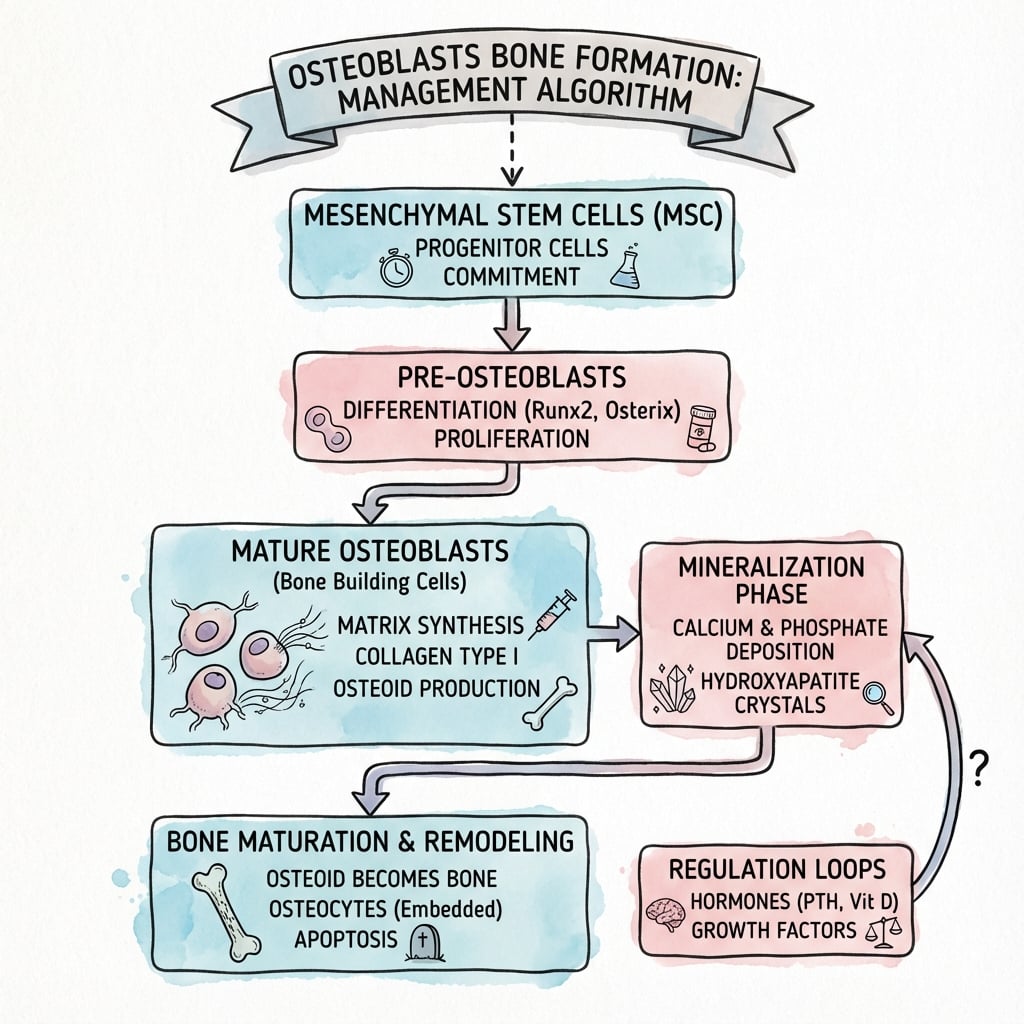
Osteoblasts are the bone-forming cells derived from mesenchymal stem cells. They synthesize and secrete the organic matrix (osteoid) and regulate its mineralization to form new bone.
Modes of Bone Formation: Intramembranous vs Endochondral
Osteoblasts build bone by two distinct mechanisms — a core "bone formation" concept and a common viva opener:
- Intramembranous ossification — mesenchymal cells condense and differentiate directly into osteoblasts that lay down bone within a fibrous membrane, with no cartilage intermediate. It forms the flat bones of the skull and face, much of the clavicle, and the periosteal (appositional) bone that increases the width/diameter of long bones.
- Endochondral ossification — a hyaline-cartilage model is formed first and then progressively replaced by bone through primary (diaphyseal) and secondary (epiphyseal) ossification centres. It forms most of the skeleton (long bones, vertebrae, pelvis) and drives longitudinal growth at the physis (and most fracture healing via callus).
Both routes first deposit disorganised woven bone, which is later remodelled into mature lamellar bone, and both require Runx2 (Runx2-null mice lack both — see the Komori evidence).
Concepts and Molecular Biology
Key Molecular Concepts
- Essential transcription factor for osteoblast differentiation
- Runx2 knockout = no osteoblasts and no bone
- Activates downstream genes: Col1a1, ALP, osteocalcin
- Primary anabolic signaling pathway for bone
- Wnt ligands stabilize β-catenin, promoting osteoblast genes
- Sclerostin (SOST) inhibits Wnt by blocking LRP5/6 receptors
- BMP-2 and BMP-7 are potent osteoinductive factors
- Used clinically for nonunion and spinal fusion
- Activate Smad signaling for osteoblast differentiation
- The osteoblast/osteocyte lineage is the master controller of osteoclast formation. Osteoblasts and osteocytes express RANKL (receptor activator of NF-κB ligand), which binds RANK on osteoclast precursors and — together with M-CSF — drives their differentiation and activation.
- The same cells secrete osteoprotegerin (OPG), a soluble decoy receptor that binds RANKL and prevents it engaging RANK. The RANKL : OPG ratio therefore sets the resorptive "tone": a high ratio favours resorption, a low ratio favours formation.
- Osteocytes are now recognised as a dominant source of RANKL in adult bone remodelling.
- This is the basis of coupling — resorption and formation are linked, partly via matrix-derived factors (TGF-β, IGF-1) released during resorption that recruit osteoblasts. It is also the target of denosumab (an anti-RANKL antibody), the antiresorptive mirror to the osteoblast-stimulating anabolic agents.
Differential Diagnosis: Disorders of Osteoblast and Mineralization Pathways
A favourite viva manoeuvre is to give a defect and ask which step of osteoblast biology is broken. Anchor your answer to the molecular lesion.
- Molecular Defect
- RUNX2 haploinsufficiency
- Osteoblast Step Affected
- Osteoblast differentiation (master TF)
- Discriminating Feature
- Absent/hypoplastic clavicles, delayed fontanelle closure, supernumerary teeth
- Molecular Defect
- COL1A1/COL1A2 (most), defective type I collagen
- Osteoblast Step Affected
- Matrix synthesis (collagen quality/quantity)
- Discriminating Feature
- Blue sclerae, recurrent low-energy fractures, dentinogenesis imperfecta
- Molecular Defect
- ALPL (tissue-nonspecific ALP) loss-of-function
- Osteoblast Step Affected
- Mineralization (PPi not hydrolyzed)
- Discriminating Feature
- LOW serum ALP, raised PLP and urinary phosphoethanolamine, premature tooth loss
- Molecular Defect
- Vitamin D or phosphate deficiency
- Osteoblast Step Affected
- Mineralization (substrate lack)
- Discriminating Feature
- Normal-to-high ALP, low calcium/phosphate, widened osteoid seams
- Molecular Defect
- LRP5 loss-of-function
- Osteoblast Step Affected
- Wnt signaling (low bone mass)
- Discriminating Feature
- Childhood low bone mass plus congenital blindness
- Molecular Defect
- SOST loss-of-function (no sclerostin)
- Osteoblast Step Affected
- Wnt disinhibition (high bone mass)
- Discriminating Feature
- Progressive bone overgrowth, cranial nerve entrapment, tall stature
- Molecular Defect
- OsteoCLAST failure (CA-II, CLCN7, TCIRG1)
- Osteoblast Step Affected
- NOT an osteoblast defect
- Discriminating Feature
- Dense brittle bone, marrow failure - the classic osteoblast-mimic trap
Osteopetrosis is a defect of osteoCLASTS, not osteoblasts. Bone formation proceeds normally but resorption fails, so dense, disorganised, fragile bone accumulates with marrow failure. Likewise, hypophosphatasia is the only one of these with a LOW serum ALP - every other mineralization disorder tends to raise ALP.
Management Algorithm
Clinical Relevance and Applications
Clinical importance:
- Anabolic therapy targets: Osteoblast stimulation is the goal of anabolic osteoporosis treatments (teriparatide, romosozumab)
- Fracture healing: Osteoblasts are responsible for callus formation and remodeling
- Bone tumors: Osteosarcoma arises from malignant osteoblasts
- Genetic disorders: Osteogenesis imperfecta (collagen synthesis defect), cleidocranial dysplasia (RUNX2 mutation)
Osteoblast function is the target of anabolic bone therapy. Understanding the Wnt/β-catenin pathway explains how anti-sclerostin antibodies (romosozumab) work. Understanding PTH receptors on osteoblasts explains why intermittent PTH is anabolic while continuous PTH (hyperparathyroidism) is catabolic.
Osteoblast Differentiation
From MSC to Osteoblast
Osteoblast Differentiation Stages
Multipotent progenitor that can differentiate into osteoblasts, chondrocytes, adipocytes, or myoblasts. Present in bone marrow and periosteum.
Committed to osteoblast lineage. Express Runx2 (master regulator). Can still proliferate. No alkaline phosphatase yet.
Express osterix (Sp7 transcription factor, downstream of Runx2). Begin expressing alkaline phosphatase. Proliferation slows.
Active matrix synthesis. High alkaline phosphatase activity. Secrete type I collagen and non-collagenous proteins (osteocalcin, osteopontin). Cuboidal morphology, located on bone surface.
Three possible outcomes: (1) Become osteocyte (embedded in matrix), (2) become bone lining cell (quiescent on surface), or (3) undergo apoptosis (50-70% of osteoblasts).

Understanding the differentiation sequence explains marker expression and therapeutic targets.
Osteoblast Function and Matrix Synthesis
Synthesis of Bone Matrix
Type I collagen synthesis (90% of organic matrix):
- Intracellular: Procollagen synthesis (pro-α1 and pro-α2 chains)
- Post-translational modification: Hydroxylation (requires Vitamin C), glycosylation
- Triple helix formation: Two α1(I) + one α2(I) chains
- Secretion: Procollagen secreted into osteoid
- Extracellular processing: N- and C-propeptides cleaved by proteases
- Fibril assembly: Tropocollagen self-assembles (67 nm periodicity)
- Crosslinking: Lysyl oxidase creates pyridinoline and deoxypyridinoline crosslinks
Non-collagenous proteins (10% of organic matrix):
- Osteocalcin: Vitamin K-dependent, binds calcium, regulates mineralization
- Osteopontin: Cell adhesion, regulates crystal growth
- Bone sialoprotein (BSP): Nucleates hydroxyapatite crystal formation
- Osteonectin (SPARC): Binds collagen and calcium, links organic and mineral phases
Osteoblasts secrete both collagen and non-collagenous proteins to form osteoid (unmineralized matrix).
Osteoblast Terminal Differentiation
After completing matrix synthesis, osteoblasts have three possible fates:
- Percentage
- 10-20%
- Characteristics
- Embedded in lacunae within bone matrix
- Function
- Mechanosensor, secretes sclerostin, regulates remodeling
- Percentage
- 30-40%
- Characteristics
- Flat, quiescent cells on bone surface
- Function
- Can reactivate to osteoblasts during remodeling
- Percentage
- 50-70%
- Characteristics
- Programmed cell death
- Function
- Removes excess osteoblasts after remodeling cycle
Osteocytes:
- Location: Embedded in lacunae, interconnected by canaliculi
- Morphology: Stellate (star-shaped) with long dendritic processes
- Number: 10 times more numerous than osteoblasts (90-95% of bone cells)
- Function: Mechanosensation (sense mechanical strain), secrete sclerostin (inhibits bone formation), regulate phosphate homeostasis (FGF23)
- Lifespan: Decades (as long as bone exists)
Bone lining cells:
- Location: Flat cells on quiescent bone surfaces
- Morphology: Squamous (flat), cover 80-90% of adult bone surfaces
- Function: Barrier between bone and marrow, can reactivate to osteoblasts when stimulated
- Clinical relevance: Reserve of osteoblast progenitors during remodeling
Osteocytes are mechanosensors that detect mechanical strain through fluid flow in canaliculi. Mechanical loading reduces sclerostin production by osteocytes, increasing Wnt signaling and bone formation. This is the cellular mechanism of Wolff's law (bone adapts to mechanical stress).

Regulation of Osteoblast Activity
Hormonal and Systemic Regulation
- Effect on Osteoblasts
- Anabolic (stimulates)
- Mechanism
- Activates Wnt pathway, reduces sclerostin
- Clinical Relevance
- Teriparatide for osteoporosis
- Effect on Osteoblasts
- Catabolic (via RANKL)
- Mechanism
- Increases RANKL, activates osteoclasts
- Clinical Relevance
- Hyperparathyroidism causes bone loss
- Effect on Osteoblasts
- Maturation, mineralization
- Mechanism
- Promotes osteocalcin synthesis
- Clinical Relevance
- Deficiency causes osteomalacia
- Effect on Osteoblasts
- Inhibits (high dose)
- Mechanism
- Reduces proliferation, increases apoptosis
- Clinical Relevance
- Steroid-induced osteoporosis
- Effect on Osteoblasts
- Maintains (indirect)
- Mechanism
- Reduces osteoblast apoptosis, decreases RANKL
- Clinical Relevance
- Loss at menopause increases remodeling
- Effect on Osteoblasts
- Stimulates
- Mechanism
- Promotes osteoblast differentiation and function
- Clinical Relevance
- Acromegaly increases bone formation
Intermittent PTH is anabolic (teriparatide given daily), while continuous PTH is catabolic (hyperparathyroidism causes bone loss). The difference: intermittent PTH stimulates osteoblasts without sustained RANKL-mediated osteoclast activation. Continuous PTH increases RANKL, driving net bone resorption.
Systemic factors coordinate bone formation with whole-body calcium and phosphate homeostasis.
Guidelines, Registries and Global Practice
Global Epidemiology
- Osteoporosis underlies the public-health burden that osteoblast-targeted drugs address: an estimated 1 in 3 women and 1 in 5 men over 50 worldwide will sustain a fragility fracture in their remaining lifetime.
- Hip-fracture incidence varies more than tenfold between countries, with the highest age-standardised rates historically reported in Northern Europe and the fastest absolute growth projected across Asia as populations age.
Side-by-Side Guideline Positions
- Anabolic agents covered
- Teriparatide, abaloparatide, romosozumab
- Positioning
- First-line for very-high-risk patients
- Notable caveat
- Follow with an antiresorptive to preserve gains
- Anabolic agents covered
- Teriparatide, romosozumab
- Positioning
- Recommended for high fracture risk; romosozumab up to 12 months
- Notable caveat
- Avoid romosozumab with recent MI/stroke
- Anabolic agents covered
- Teriparatide, romosozumab
- Positioning
- Reserved for very high risk / multiple vertebral fractures
- Notable caveat
- Cost-effectiveness thresholds gate access
- Anabolic agents covered
- Teriparatide, abaloparatide, romosozumab
- Positioning
- Anabolic-first for imminent/very-high risk
- Notable caveat
- Emphasise sequential therapy and adherence
Registry and Real-World Evidence
- Large pharmacovigilance and registry datasets confirm the rare class harms of antiresorptive follow-on therapy (osteonecrosis of the jaw, atypical femoral fracture) and have shaped the limited (12-month) treatment courses for romosozumab and teriparatide.
- Bone-turnover-marker registries (PINP for formation, CTX for resorption) are increasingly used internationally to monitor osteoblast response and adherence to therapy.
High- versus Limited-Resource Practice
- In well-resourced systems, fracture-liaison services, DXA, bone-turnover markers and the full anabolic armamentarium are available; sequencing decisions dominate.
- In limited-resource settings, calcium/vitamin D repletion and generic oral bisphosphonates remain the practical mainstays; high-cost biologics (romosozumab, denosumab) and routine bone-turnover-marker monitoring are often unavailable, so correcting nutritional osteomalacia and ensuring adherence carry the greatest yield.
Controversies and Areas of Uncertainty
Murine work proposed undercarboxylated osteocalcin as an endocrine regulator of insulin secretion, energy metabolism and fertility. Human data are inconsistent, and humans lacking the proposed receptor (GPRC6A) do not reliably reproduce the mouse phenotype. The "bone as an endocrine organ" story remains unproven in humans.
Recombinant BMP-2 reliably promotes fusion but carries real risks: retrograde ejaculation and life-threatening anterior cervical soft-tissue swelling (off-label), ectopic bone and seroma. An early cancer signal was not confirmed on pooled re-analysis. Use is now far more selective than after its launch.
ARCH and the VERO trial (teriparatide vs risedronate) suggest anabolic-first sequencing reduces fractures more than antiresorptive-first in high-risk patients, yet cost and the romosozumab cardiovascular signal keep antiresorptives as default first-line in most guidelines.
ARCH showed more serious cardiovascular events versus alendronate, but FRAME (versus placebo) did not. Whether this reflects a true hazard or alendronate cardioprotection is unresolved; regulators contraindicate romosozumab after recent myocardial infarction or stroke.
MCQ Practice Points
Q: What is the master transcription factor for osteoblast differentiation?
A: Runx2 (Cbfa1). It is essential for osteoblast differentiation - Runx2 knockout mice have no osteoblasts and no bone. Cleidocranial dysplasia is caused by RUNX2 haploinsufficiency (absent clavicles, delayed fontanelle closure, dental abnormalities).
Q: What is the role of the Wnt/β-catenin pathway in bone, and what inhibits it?
A: Wnt signaling promotes osteoblast differentiation and bone formation. It is inhibited by sclerostin (produced by osteocytes, encoded by SOST gene) which binds LRP5/6 co-receptors. This is the target for romosozumab - an anti-sclerostin antibody used as an anabolic bone agent.
Q: What is the primary role of alkaline phosphatase in bone mineralization?
A: Alkaline phosphatase (ALP) hydrolyzes pyrophosphate, which is an inhibitor of mineralization. By removing pyrophosphate, ALP allows hydroxyapatite crystal formation. Hypophosphatasia (ALP deficiency) causes defective bone mineralization resembling rickets.
Q: What are the possible fates of mature osteoblasts after completing bone formation?
A: Three possible fates:
- Osteocyte (most common) - embedded in matrix, become mechanosensors
- Bone lining cell - quiescent surface cells that can reactivate
- Apoptosis - programmed cell death (up to 60-80% undergo this fate)
At a Glance
Osteoblasts are the bone-forming cells derived from mesenchymal stem cells through a differentiation pathway controlled by the master transcription factor Runx2 (Cbfa1)—Runx2 knockout mice have no osteoblasts and no bone. Wnt/β-catenin signaling promotes osteoblast differentiation, while sclerostin (from osteocytes) inhibits this pathway. Osteoblasts synthesize Type I collagen (90% of organic matrix) and non-collagenous proteins (osteocalcin, osteopontin), producing osteoid that mineralizes after a 10-14 day lag. Alkaline phosphatase (the osteoblast marker enzyme) hydrolyzes pyrophosphate (a mineralization inhibitor) to enable hydroxyapatite crystal formation. Mature osteoblasts have three fates: become embedded as osteocytes, become quiescent bone lining cells, or undergo apoptosis.
RUNX2RUNX2 - Master Osteoblast Regulator
Hook:RUNX2 - if it doesn't RUN, no bone is formed (master regulator)
WNTWNT - Anabolic Bone Pathway
Hook:WNT = We Need This pathway for bone formation (sclerostin blocks it)
FATEFATE - Osteoblast Destinations
Hook:The FATE of every mature osteoblast: become a lining cell, die, or become an osteocyte
Basic Science Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Describe osteoblast differentiation from mesenchymal stem cells. What is the role of Runx2?”
“Explain how osteoblasts synthesize bone matrix and regulate its mineralization. What is the role of alkaline phosphatase?”
“How do osteoblasts and osteoclasts communicate, and how is this coupling exploited by anabolic osteoporosis drugs?”
Differentiation Pathway
- MSC → osteoprogenitor (Runx2+) → preosteoblast (osterix+) → mature osteoblast (ALP+) → terminal fate
- Runx2 is master regulator - knockout = no osteoblasts, no bone, death at birth
- Osterix (Sp7) required downstream of Runx2
- Three terminal fates: osteocyte (10-20%), lining cell (30-40%), apoptosis (50-70%)
Signaling Pathways
- Wnt/β-catenin: promotes differentiation and function (target of romosozumab)
- BMP-2/BMP-7: potent osteoinductive factors, activate Runx2 via Smad1/5/8
- Sclerostin (from osteocytes): inhibits Wnt by binding LRP5/6
- PTH: intermittent = anabolic (teriparatide), continuous = catabolic (hyperPTH)
Matrix Synthesis
- Type I collagen = 90% of organic matrix (triple helix, 67 nm periodicity)
- Non-collagenous proteins = 10% (osteocalcin, osteopontin, BSP, osteonectin)
- Osteoid deposition rate: 1-2 micrometers/day
- Mineralization lag time: 10-14 days (osteoid thickness 10-15 micrometers)
Alkaline Phosphatase
- Key osteoblast enzyme and marker (serum ALP reflects activity)
- Hydrolyzes pyrophosphate (PPi), a mineralization inhibitor
- Allows hydroxyapatite crystal formation by removing PPi
- Hypophosphatasia: ALP deficiency, defective mineralization, rickets/osteomalacia
Bone Formation Markers
- Alkaline phosphatase (ALP) - bone-specific ALP (BSAP) preferred
- Osteocalcin (OC) - vitamin K-dependent, late marker
- Procollagen I N-propeptide (PINP) - collagen synthesis, least variable
- Used to monitor osteoporosis treatment response
Key Clinical Correlations
- Cleidocranial dysplasia: RUNX2 haploinsufficiency (clavicle hypoplasia, delayed fontanelle closure)
- Teriparatide: intermittent PTH, anabolic therapy for osteoporosis
- Romosozumab: anti-sclerostin antibody, anabolic via Wnt pathway
- BMP-2: osteoinductive, used for spinal fusion (FDA-approved) and nonunions
Evidence Base
Cbfa1/Runx2 Disruption Causes Complete Lack of Bone Formation
- Homozygous Cbfa1 (Runx2) knockout mice died just after birth with a complete lack of ossification
- Both intramembranous and endochondral ossification were completely blocked
- Only immature osteoblasts formed (weak alkaline phosphatase, no osteopontin or osteocalcin) - a maturational arrest
- Establishes Runx2 as essential and non-redundant for osteoblast maturation and osteogenesis
Osterix (Sp7) Is Required Downstream of Runx2 for Osteoblast Differentiation
- Osterix (Osx) is a zinc-finger transcription factor expressed in all developing bones
- Osx-null mice show no bone formation despite normal Runx2 expression
- Osx is not expressed in Runx2-null mice, placing Osx genetically downstream of Runx2
- Osx-null preosteoblasts express chondrocyte markers, suggesting Runx2+ preosteoblasts remain bipotential
LRP5 (Wnt Co-receptor) Controls Bone Mass Accrual
- Loss-of-function LRP5 mutations cause osteoporosis-pseudoglioma syndrome (OPPG) with reduced bone mass
- OPPG carriers (heterozygotes) had reduced bone mass versus matched controls
- LRP5 is expressed by osteoblasts and transduces canonical Wnt signaling
- Wnt signaling via LRP5 determines peak bone mass during growth
Teriparatide (Intermittent PTH 1-34) Reduces Fractures
- 1637 postmenopausal women with prior vertebral fractures; daily subcutaneous PTH(1-34) versus placebo, median 21 months
- 20 mcg dose: new vertebral fractures fell from 14% (placebo) to 5% (relative risk 0.35) - about 65% reduction
- Nonvertebral fragility fractures reduced (relative risk 0.47) - about 53% reduction
- BMD rose roughly 9 percentage points at lumbar spine and 3 at femoral neck versus placebo
Romosozumab (Anti-Sclerostin) Reduces Vertebral Fracture - FRAME
- 7180 postmenopausal women with osteoporosis; monthly subcutaneous romosozumab 210 mg versus placebo for 12 months, then denosumab in both arms
- New vertebral fractures at 12 months: 0.5% romosozumab versus 1.8% placebo - a 73% lower risk (P less than 0.001)
- Clinical fractures reduced 36% at 12 months; nonvertebral fracture reduction did not reach significance
- Romosozumab simultaneously increased bone formation and decreased bone resorption - validating sclerostin as a target
Romosozumab Then Alendronate Beats Alendronate Alone - ARCH
- 4093 high-risk postmenopausal women; 12 months romosozumab then alendronate versus alendronate throughout
- New vertebral fractures at 24 months: 6.2% versus 11.9% - a 48% lower risk (P less than 0.001)
- Hip fracture risk lower by 38%; nonvertebral fracture risk lower by 19%
- More positively adjudicated serious cardiovascular events with romosozumab in year 1 (2.5% versus 1.9%)