Recurrent Dislocation of the Patellofemoral Joint | MPFL and Bony Anatomy
RISK FACTORS (Principal Anatomic Factors)
Critical Must-Knows
- MPFL Anatomy: Runs from Schottle's point (femur) to superomedial patella. Primary restraint in 0-30 degrees of flexion.
- Bony Anatomy: Once past 30 degrees, the patella enters the trochlea and bony constraint takes over.
- J-Sign: Lateral deviation of the patella in full extension as it exits the trochlea.
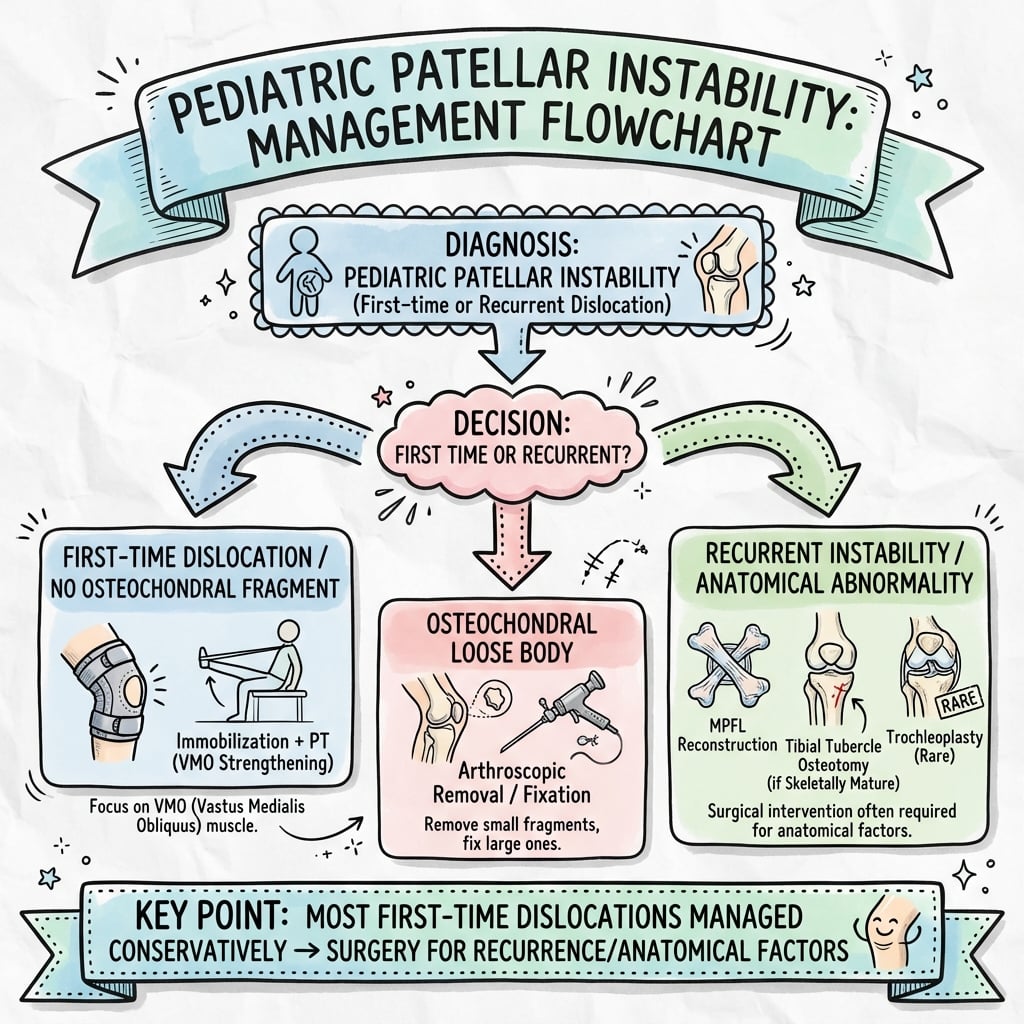
- Treatment Philosophy: First time dislocation = Non-op (Physical Therapy). Recurrent = Surgery (Address the specific pathology).
Clinical Pearls
- "Schottle's Point is between the posterior cortex line and medial condyle posterior line, just proximal to posterior condylar line.
- "Always assess for generalized ligamentous laxity (Beighton Score).
- "Don't forget rotational profile (Femoral Anteversion / Tibial External Rotation) which increases the Q-angle.
Don't Miss the Malalignment
Miserable Malalignment
Rotational Deformity: Addressing the MPFL alone in a patient with excessive femoral anteversion or tibial external rotation will fail. You must assess the rotational profile (Gait, prone internal rotation) and consider derotational osteotomy if severe.
Open Physis
Surgical Hazard: Standard MPFL reconstruction involves drilling through the distal femur. In skeletally immature patients, respect the physis. Use fluoroscopy and avoid crossing the growth plate, or use soft-tissue only fixation.
Acute vs Recurrent Instability
| Feature | Acute Dislocation | Recurrent Instability |
|---|---|---|
| Pathology | Traumatic MPFL rupture | Bony dysplasia + MPFL incompetence |
| History | Clear trauma, hemarthrosis | Low energy, 'giving way', apprehension |
| Findings | Gross effusion, tenderness medial epicondyle | Positive J-sign, Apprehension test |
| Imaging | Bone bruise (LFC/Medial Patella) | Trochlear Dysplasia, Alta |
| Treatment | Non-operative (Brace + PT) | Surgical Reconstruction (MPFL +/- TTO) |
4 H'sRisk Factors for Instability
| H | High Patella Alta (Caton-Deschamps greater than 1.2) |
| H | Horizontal Trochlear Dysplasia (Flat/Shallow groove) |
| H | Huge TT-TG Distance greater than 20mm (Lateral vector) |
| H | Hyperlaxity Generalized ligamentous laxity / Ehlers-Danlos |
| H | High Patella Alta (Caton-Deschamps greater than 1.2) | H | Huge TT-TG Distance greater than 20mm (Lateral vector) |
| H | Horizontal Trochlear Dysplasia (Flat/Shallow groove) | H | Hyperlaxity Generalized ligamentous laxity / Ehlers-Danlos |
Hook:The 4 H's determine if the patella stays in or goes out.
Overview and Epidemiology
Anatomic Restraints
Stability is biphasic:
- 0-30 degrees Flexion: Soft tissue dependent. The MPFL is the primary restraint to lateral translation.
- Greater than 30 degrees Flexion: Bony dependent. The patella engages the Trochlea.
Epidemiology:
- Acute Dislocation: 43 per 100,000 children.
- Recurrence Rate:
- Overall approx 30-50%.
- Increases to 70-80% if immature skeleton + dysplasia.
- Demographics: Highest in adolescent females (10-17 years).
Pathophysiology:
- Dislocation is almost always LATERAL.
- Results in tearing of the MPFL (Medial Patellofemoral Ligament).
- "Kissing Contusion": Bone bruise on the Lateral Femoral Condyle and Medial Patellar Facet.
- Osteochondral fractures (loose bodies) occur in 10-20% of acute dislocations.
Pathophysiology and Mechanisms
Medial Patellofemoral Ligament (MPFL)
- Origin: Schottle's Point (Femur).
- Saddle between medial epicondyle and adductor tubercle.
- Radiographic landmark: Between posterior cortical line and posterior condylar line.
- Insertion: Upper 2/3 of medial patellar border.
- Function: Provides 50-60% of restraint to lateral translation in early flexion (0-30 degrees).
- Biomechanics: Isometric behavior (length changes minimal during flexion).
Classification Systems
Trochlear Dysplasia (Dejour Classification)
| Type | Description |
|---|---|
| Type A | Shallow Trochlea |
| Type B | Flat Trochlea |
| Type C | Convex Lateral Facet |
| Type D | Cliff Pattern |
Patellar Height (Caton-Deschamps)
| Parameter | Ratio (A/B) |
|---|---|
| Patella Baja | less than 0.6 |
| Normal | 0.8 - 1.2 |
| Patella Alta | greater than 1.2 |
MPFL Injury Location
Based on MRI findings in acute dislocation:
- Femoral Avulsion: 60-70% (Most common).
- Implication: Good target for primary repair if acute (controversial).
- Mid-substance: 20-30%.
- Implication: Poor healing potential, reconstruction preferred.
- Patellar Avulsion: 10-20%.
- Implication: May look like medial rim fracture.
Note: In recurrent cases, the ligament is often attenuated/absent rather than discretely torn.
Clinical Assessment
History:
- Acute Presentation:
- Mechanism: Non-contact twisting injury, knee flexed and in valgus.
- Sensation: "Pop" or "crack" often heard.
- Observation: Patella dislocates laterally, often reduces spontaneously with knee extension.
- Aftermath: Rapid hemarthrosis (within 1-2 hours) indicating ligamentous tear or osteochondral fracture.
- Chronic/Recurrent Presentation:
- Mechanism: Minimal trauma (e.g., turning in bed, dancing).
- Sensation: "Giving way" rather than frank dislocation.
- Pain: Anterior knee pain, especially with stairs or prolonged sitting (Movie sign).
- Psychology: Fear of sports/activity (Kinesiophobia).
Physical Examination:
- Inspection (Standing):
- Coronal Alignment: Valgus knees (knock-knees) increase the Q-angle and lateral vector.
- Foot Posture: Pes planus (flat foot) leads to internal tibial rotation, increasing Q-angle.
- Patella Position: "Grasshopper eyes" appearance (high and lateral patellae).
- Inspection (Seated):
- J-Sign: Observe patellar tracking from 90 degrees flexion to full extension.
- Positive Sign: Patella deviates laterally in terminal extension as it exits the trochlea.
- Significance: Strong indicator of Patella Alta and Trochlear Dysplasia.
- Palpation:
- Medial Epicondyle / Adductor Tubercle: Site of MPFL femoral origin. Tenderness suggests acute tear.
- Medial Patellar Facet: Tenderness suggests MPFL avulsion or chondral injury.
- Lateral Femoral Condyle: Tenderness suggests "kissing contusion" bone bruise.
- Retinacular Integrity: Palpable defect in medial retinaculum.
- Specific Tests:
- Patellar Apprehension Test:
- Knee flexed to 20-30 degrees (relax hamstrings).
- Examiner pushes patella laterally.
- Positive: Patient contracts quadriceps, grabs examiner's hand, or expresses fear.
- Note: Pain alone is not a positive apprehension test (could be just PF OA).
- Patellar Glide:
- Assess medial/lateral translation in quadrants (1 quadrant = 25% width).
- Normal: 1-2 quadrants.
- Hyperlax: greater than 3 quadrants suggests incompetence of restraints.
- Beighton Score:
- Assess for generalized ligamentous laxity (greater than 4/9).
- Thumb to wrist, 5th finger extension greater than 90, Elbow hyperextension, Knee hyperextension, Palms to floor.
- Rotational Profile (Prone):
- Femoral Anteversion: Increased internal rotation (greater than 70 degrees) compared to external rotation.
- Tibial Torsion: Thigh-foot axis greater than 20 degrees external.
- Patellar Apprehension Test:
The Miserable Malalignment Syndrome
Triad of deformities creating a perfect storm for instability:
- Femoral Anteversion (Inward twisting of femur).
- External Tibial Torsion (Outward twisting of tibia).
- Genu Valgum (Knock knees). Result: Extreme lateral Q-angle. MPFL reconstruction alone WILL FAIL. Requires osteotomy (Derotational Femoral/Tibial).
Differential Diagnosis
The acutely swollen adolescent knee after a twisting injury has several mimics. The key discriminators are the mechanism, the location of tenderness, and the imaging pattern.
Differentiating the Painful / Unstable Adolescent Knee
| Condition | Distinguishing Feature | Confirmatory Finding |
|---|---|---|
| Patellar dislocation | Lateral giving way, medial tenderness, positive apprehension | MPFL tear plus kissing contusion (LFC and medial patella) on MRI |
| ACL rupture | Pivot injury with effusion but central/rotational instability | Lange/pivot-shift positive; MRI ACL discontinuity, bone bruise on LFC and posterolateral tibia |
| Osteochondritis dissecans | Insidious activity-related pain, may catch/lock | Lateral notch (tunnel) view and MRI subchondral lesion of medial femoral condyle |
| Meniscal tear | Joint-line tenderness, locking, McMurray positive | MRI meniscal signal reaching articular surface |
| Patellofemoral pain syndrome | Anterior pain with stairs/sitting, NO true instability | Normal alignment imaging; no apprehension, no dislocation history |
| Sleeve / tibial tubercle avulsion fracture | Acute inability to extend, focal bony tenderness | Lateral radiograph showing apophyseal/sleeve fragment |
Investigations
Standard Series:
- AP View: Generally normal, may show osteochondral fracture loose body.
- Lateral View (Most useful screening tool):
- Patella Alta: Calculate Caton-Deschamps Index (Articular surface length / Distance to Tibia).
- Normal: 0.8 - 1.2.
- Alta: Greater than 1.2.
- Trochlear Dysplasia:
- Crossing Sign: Trochlear floor crosses anterior femoral condyles. Represents a flat groove.
- Supratrochlear Spur: Prominence of proximal trochlea.
- Double Contour Sign: Medial condyle hypoplasia seen as a double line on the posterior aspect of the condyles.
- Patella Alta: Calculate Caton-Deschamps Index (Articular surface length / Distance to Tibia).
- Skyline (Merchant) View:
- Taken at 30 degrees flexion.
- Patellar Tilt: Angle between posterior condylar line and patellar axis.
- Subluxation: Congruence angle.
- Avulsion Fractures: Look closely at the medial patellar margin (MPFL avulsion fleck).
Management Algorithm
Conservative Management
-
Indication:
- First-time acute dislocation (without large loose body).
- Patients with low demands or minimal risk factors.
-
Phase 1 (0-2 Weeks):
- Reduction: Extend knee, gentle medial pressure.
- Immobilization: Extension splint or hinged brace locked in extension. Weight bearing as tolerated (WBAT).
- Goal: Allow MPFL to heal in reduced position (not stretched).
-
Phase 2 (2-6 Weeks):
- Motion: Unlocked brace 0-90 degrees.
- Strengthening:
- VMO Activation: Straight leg raises with external rotation.
- Gluteal Control: Clamshells, bridging. Correct dynamic valgus.
- Core Stability: Plank progressions.
- Taping: McConnell taping to unload tissues.
-
Phase 3 (6+ Weeks):
- Return to Sport: When strength greater than 90% of contralateral side and functional hopping test passed.
- Bracing: "J"-buttress brace (e.g., Tru-Pull) for sports.
Surgical Technique
Anatomic MPFL Reconstruction steps
- Graft Harvest: Gracilis tendon (single or double strand). Whip-stitched ends.
- Patellar Attachment:
- Exposure: small incision medial patella border.
- Location: Upper 1/3 of the medial border (junction of proximal and middle thirds).
- Fixation: Two suture anchors or parallel tunnel technique.
- Pearl: Ensure fixation is not intra-articular.
- Femoral Attachment (Critical Step):
- Exposure: Incision over medial epicondyle.
- Schottle's Point Identification:
- Radiographic landmarks (Lateral Fluoro):
- Extension of posterior cortical line.
- Proximal to posterior condylar line (2.5mm).
- Just posterior to Blumensaat's extended line.
- Radiographic landmarks (Lateral Fluoro):
- Pin Placement: Drill guidewire at Schottle's point.
- Isometry Check:
- Loop graft around pin. Range knee 0-90.
- Graft should be tightest at 0-30 degrees and slightly relax in deeper flexion.
- If gets tight in flexion implies Pin is too Proximal/High.
- If gets tight in extension implies Pin is too Distal/Low or Anterior.
- Tunnel & Fixation:
- Drill 6-7mm tunnel (careful of Notch/ACL).
- Fix with interference screw with knee at 30 degrees flexion.
- Tension: Zero tension. Just remove slack. Check lateral glide (10mm).
Complications
| Complication | Risk Factor | Prevention | Management |
|---|---|---|---|
| Recurrent Instability | Missed bony pathology (Alta/TT-TG), Tunnel Malposition | Address bony factors, Isometry check | Revision with TTO / Revision MPFL |
| Stiffness / Loss of Flexion | Over-tensioned MPFL (High/Proximal placement) | Proper femoral point check | MUA or Revision (Release) |
| Patellar Fracture | Drill holes / Anchors in patella (stress risers) | Careful drilling spacing (greater than 10mm apart) | ORIF or Suture repair |
| Physeal Arrest | Drilling across physis in immature patient | Fluoro guidance / Epiphyseal sparing technique | Bar resection / Growth correction |
| Anterior Knee Pain | Over-medialization / Over-tension / Cartilage overload | Check tracking intra-op, Don't over-constrain | Physio / Revision |
Postoperative Care
Protocol for Isolated MPFL Reconstruction:
- Immobilization: Hinged knee brace locked in extension for ambulation. Sleep in brace.
- Weight Bearing: Weight bearing as tolerated (WBAT) with crutches.
- ROM: Passive flexion 0-90 degrees limiting active extension (protects graft).
- Exercises: Quad sets, ankle pumps, SLR in brace.
- Goal: Wound healing, control effusion, quadriceps re-activation.
- Immobilization: Unlock brace 0-90 degrees for walking. Wean crutches when gait normal.
- ROM: Progress to full range of motion.
- Exercises:
- Stationary cycling (low resistance).
- Closed chain quads (mini-squats 0-45 deg).
- Heel raises.
- Proprioception drills.
- Precaution: Avoid open chain knee extension (e.g., knee extension machine).
- Immobilization: Discontinue brace.
- ROM: Should be full.
- Exercises:
- Leg press.
- Lunges.
- Elliptical trainer.
- Hamstring strengthening.
- Core/Gluteal stability.
- Testing:
- Isokinetic testing (greater than 90% limb symmetry).
- Hop tests (Single, Triple, Crossover).
- No apprehension on exam.
- Progression: Running to Agility/Cutting to Contact.
- Timeline: Usually 5-6 months for contact sports.
Outcomes
Natural History (Non-Operative):
- Recurrence rate after primary dislocation:
- Overall: 30-50%.
- History of contralateral dislocation: Risk increases significantly.
- Presence of Dysplasia + Open Physis: Risk up to 70%.
- Chronic pain and patellofemoral osteoarthritis are long-term sequelae of recurrent instability.
Surgical Outcomes:
- MPFL Reconstruction:
- Success: 90-95% prevention of further dislocations.
- Return to Sport: High rates (approx 85%), but often at a slightly lower level due to fear/guarding.
- Complications: Complication rate approx 15-20% (Stiffness is most common).
- TTO + MPFL:
- Similar success rates for stability.
- Higher procedural morbidity (Delayed union, screw prominence).
- Essential for correction of high-grade bony deformity.
The 'Sentinel' Lesion
An osteochondral fracture (loose body) occurs in a substantial minority of acute dislocations. Always scrutinize the radiograph and obtain MRI if effusion persists or mechanical symptoms (locking, catching) are present. A displaced, fixable osteochondral fragment converts a "non-operative" first dislocation into a surgical one.
Controversies and Areas of Uncertainty
Surgery after a first dislocation?
Most guidance still favours non-operative care for an isolated first dislocation. The debate is whether high-risk children (trochlear dysplasia plus skeletal immaturity plus alta) should be offered early stabilization, since their recurrence risk exceeds 50-88%. Trials are small; selection by risk model rather than blanket policy is the pragmatic position.
MPFL repair vs reconstruction
Acute repair of a femoral or patellar avulsion is intuitively attractive, but reported redislocation rates are higher than for anatomic reconstruction, especially when bony risk factors are present. Reconstruction is the default for recurrent instability.
Role of trochleoplasty
Trochleoplasty addresses the dysplastic groove directly but carries risks of chondral damage and stiffness. It is reserved for high-grade (Dejour B/D) dysplasia in specialist centres, and is generally avoided in the open-physis knee. Whether it should be added at the index operation or staged remains debated.
TT-TG distance reliability
The 20mm threshold is widely quoted but TT-TG varies with measurement modality (CT vs MRI), knee flexion and rotation, and has imperfect reproducibility. Some advocate TT-TG to posterior cruciate ligament ratio or sagittal patellotrochlear index to reduce these errors. Treat 20mm as a guide, not an absolute trigger.
Evidence Base
Recurrence in Skeletally Immature Patients (Landmark Cohort)
- Population-based cohort of 232 skeletally immature patients with first-time lateral dislocation (mean follow-up 12.1 years).
- Cumulative ipsilateral recurrence: 37% at 5 years rising to 54% at 20 years.
- Patella alta (HR 10.6), TT-TG 20mm or more (HR 18.7), and trochlear dysplasia (HR 23.7) were strongly associated with recurrence.
- Patellofemoral arthritis reached 17% at 20 years; osteochondral injury was the key driver (HR 25.7).
Radiographic Landmark for Femoral Tunnel (Schottle Point)
- Cadaveric study of 8 knees defining the radiographic femoral MPFL centre on a true lateral view.
- Point lies 1mm anterior to the posterior cortex extension line.
- 2.5mm distal to the posterior origin of the medial femoral condyle.
- Proximal to the level of the posterior point of Blumensaat's line.
Factors of Patellar Instability (Landmark Classification)
- Radiograph and CT analysis of 143 unstable knees versus controls established the four anatomic factors.
- Trochlear dysplasia (crossing sign) was present in 85% of unstable knees but only 3-6.5% of controls.
- TT-TG distance defined as pathological at 20mm or more (present in 56%).
- Patella alta defined as Caton-Deschamps index 1.2 or more (present in 24%).
Femoral Tunnel Position Determines Graft Length Change
- Intraoperative graft length change measured during passive motion in 27 MPFL reconstructions.
- Femoral tunnel position was the essential determinant of graft length change behaviour.
- Non-isometric (more proximal) tunnels produced grafts that lengthened in flexion; this impaired early recovery of range of motion.
- Patella height also influenced the length-change pattern.
Physeal-Sparing MPFL Reconstruction in Children
- Prospective case series of 21 children with open growth plates (mean age 12.2 years).
- Femoral fixation kept distal to the physis; no recurrent dislocations at mean 2.8-year follow-up.
- Kujala score improved significantly from 72.9 to 92.8.
- Two patients with high-grade trochlear dysplasia retained a positive apprehension sign.
Predicting Recurrence After First Dislocation (Risk Model)
- Retrospective review of 266 knees with first-time dislocation; overall non-operative recurrence 34.7%.
- On multivariate analysis trochlear dysplasia (OR 3.56) and skeletal immaturity (OR 2.23) were the strongest predictors.
- Four factors (trochlear dysplasia, skeletal immaturity, CDI greater than 1.45, contralateral dislocation history) drive the model.
- All four factors present predicts an 88% recurrence risk; any three about 75%; any two about 55%.
Exam Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Scenario 1: Acute First Dislocation
"A 14-year-old girl presents with a first-time lateral patellar dislocation. Reduced in ED. MRI shows a bone bruise and MPFL tear. Dysplasia is mild. Plan?"
Scenario 2: Recurrent Instability
"15-year-old boy, 3 prior dislocations. Now 'gives way' easily. X-ray: Caton-Deschamps 1.3. CT: TT-TG 24mm. Physis is closing."
Scenario 3: Intra-op Complication
"During MPFL reconstruction, you tension the graft at 90 degrees flexion. Post-operatively the patient has full flexion but lacks extension past 30 degrees. Why?"
MCQ Practice Points
Question 1
Q: The primary restraint to lateral patellar translation at 20 degrees of flexion is: A. Medial Patellomeniscal Ligament B. Medial Patellofemoral Ligament (MPFL) C. Trochlear Geometry D. VMO Muscle Answer: B. The MPFL contributes 60% of restraint in early flexion (0-30). Beyond 30, the trochlea takes over.
Question 2
Q: Which radiographic sign on lateral knee X-ray indicates Trochlear Dysplasia? A. Double PCL sign B. Crossing Sign C. Segond Sign D. Deep Sulcus Sign Answer: B. The Crossing Sign occurs when the curve of the trochlear floor crosses the anterior contour of the femoral condyles, indicating a flat/shallow groove.
Question 3
Q: Why is Tibial Tubercle Osteotomy (TTO) contraindicated in a 10-year-old? A. Poor bone stock B. Risk of Genu Recurvatum (growth arrest) C. High infection rate D. It is ineffective Answer: B. Performing an osteotomy on the tibial tubercle apophysis can cause premature closure of the anterior physis, leading to a recurvatum (hyperextension) deformity.
Question 4
Q: What is the normal limit for TT-TG distance on MRI? A. 10mm B. 15mm C. 20mm D. 25mm Answer: C. Values above 20mm are considered pathologic and a strong indication for medializing osteotomy. 15-20mm is borderline.
Question 5
Q: A 'J-Sign' on clinical examination indicates: A. ACL deficiency B. Meniscal tear C. Patella Alta and Dysplasia D. Patella Baja Answer: C. The J-Sign is the lateral deviation of the patella as it exits the trochlea in extension. It suggests the patella is engaging late (Alta) or the bony constraint is poor (Dysplasia).
Guidelines, Registries & Global Practice
Global Epidemiology:
- First-time lateral patellar dislocation incidence is approximately 23 per 100,000 person-years overall, peaking at roughly 108-148 per 100,000 in adolescents aged 14-18 years.
- Sex distribution is broadly even, with a relative female preponderance in many adolescent cohorts.
- Recurrence after a first dislocation is approximately 30-40% overall but rises to over 50% in skeletally immature patients with trochlear dysplasia or patella alta.
Side-by-Side: How Societies Frame Management
| Body | First Dislocation | Recurrent / Surgical Stance |
|---|---|---|
| AAOS / AOSSM (US) | Non-operative first line; image to exclude osteochondral fragment | MPFL reconstruction favoured over repair; correct bony factors a la carte |
| BOA / BASK (UK) | Reduction, short immobilization, structured physiotherapy | Reconstruction for recurrent instability; trochleoplasty in specialist centres for high-grade dysplasia |
| ESSKA (Europe) | Risk-stratify using dysplasia, alta, TT-TG, immaturity | Consensus supports anatomic MPFL reconstruction; reserves trochleoplasty for Dejour B/D |
| Paediatric consensus | Physeal-respecting planning mandatory | Avoid tibial tubercle osteotomy with open apophysis (recurvatum risk); soft-tissue or physeal-sparing techniques |
Registry and Outcome Notes:
- There is no large dedicated patellofemoral instability registry equivalent to arthroplasty registries; evidence rests on population cohorts (e.g. the Mayo/Olmsted County series) and institutional series.
- Reported redislocation rates after anatomic MPFL reconstruction are low (commonly under 5-10%), with stiffness and anterior knee pain the most frequent complications.
High- vs Limited-Resource Practice Variation:
- Well-resourced settings: MRI and CT (or low-dose CT/EOS) for TT-TG and rotational profile, image-guided anatomic reconstruction, and access to trochleoplasty.
- Limited-resource settings: Diagnosis and planning rely more on plain radiographs and clinical assessment; hamstring autograft is strongly preferred over allograft on cost and availability grounds, and complex bony realignment may be referred to tertiary centres.
Patellar Instability Essentials
Clinical summary
Key Numbers
- •TT-TG greater than 20mm (= Bad/Lateralised)
- •Caton-Deschamps greater than 1.2 (= Alta)
- •Sulcus Angle greater than 145 deg (= Dysplasia)
- •Recurrence 40-50% (Acute First Time)
Imaging Signs
- •Crossing Sign (Trochlear Dysplasia)
- •Double Contour Sign (hypoplastic medial condyle)
- •J-Sign (Clinical sign of maltracking)
- •MPFL Avulsion (Medial patella margin)
Surgery Rules
- •First time = Non-op (Brace + Physio)
- •Recurrent = MPFL Reconstruction
- •Bone problem (TT-TG greater than 20) = Bone Op (TTO)
- •Open Physis = No TTO (Soft tissue only)
Schottle Point
- •Proximal to Post Condylar Line
- •Distal to Physis
- •Between Post Cortex & Post Condyle
- •Center of MPFL femoral origin
CROSSFeatures of Trochlear Dysplasia
| C | Crossing Crossing Sign (Floor crosses condyles) |
| R | Rotated Internal rotation of femur (Anteversion) |
| O | Offset Double Contour |
| S | Shallow Sulcus angle greater than 145 |
| S | Spur Supratrochlear Spur (Type B) |
| C | Crossing Crossing Sign (Floor crosses condyles) | S | Shallow Sulcus angle greater than 145 |
| R | Rotated Internal rotation of femur (Anteversion) | S | Spur Supratrochlear Spur (Type B) |
| O | Offset Double Contour |
Hook:Anatomy of a bad groove.
LOCKEDIndications for Surgery
| L | Loose Body Osteochondral fracture |
| O | Osteotomy Required if TT-TG greater than 20mm |
| C | Chronic Recurrent instability |
| K | Kinesiophobia Fear avoidance affecting quality of life |
| E | Exam Findings Consistent apprehension + laxity |
| D | Dysplasia Severe Bony Dysplasia (High risk) |
| L | Loose Body Osteochondral fracture | C | Chronic Recurrent instability | E | Exam Findings Consistent apprehension + laxity |
| O | Osteotomy Required if TT-TG greater than 20mm | K | Kinesiophobia Fear avoidance affecting quality of life | D | Dysplasia Severe Bony Dysplasia (High risk) |
Hook:When to intervene surgically.