Proximal tendon angiofibroblastic hyperplasia | Eccentric loading key | Contraindication to steroids | VISA-P score
BLAZINA CLASSIFICATION
Critical Must-Knows
- Pathology is degenerative, not inflammatory (tendinosis vs tendinitis)
- Inferior pole of patella is classic site of tenderness (Bassett's sign)
- Eccentric strengthening on decline board is gold standard rehab
- Steroid injections are contraindicated due to rupture risk
- Surgical debridement indicated after 6 months of failed conservative care
Clinical Pearls
- "Tenderness is typically at the proximal posterior patellar tendon (inferior pole)
- "Pain induced by extension against resistance
- "Bassett's sign: tenderness palpated in full extension disappears in flexion
- "Ultrasound shows hypoechoic area and neovascularization
Critical Exam Points for Jumper's Knee
Terminology Matters
It is a tendinopathy/tendinosis, NOT an acute inflammatory "tendinitis". Histology shows angiofibroblastic hyperplasia, mucoid degeneration, and absence of inflammatory cells. Use "tendinopathy" in the exam.
Steroid Contraindication
NEVER inject corticosteroids into the patellar tendon. It causes collagen necrosis and significantly increases the risk of acute tendon rupture. This is an immediate fail point in vivas.
Bassett's Sign
Bassett's sign distinguishes patellar tendinitis from other anterior knee pain. Localization of tenderness at distal pole of patella in full extension, which disappears in 90 degrees flexion (tendon tension prevents deep palpation).
Differential Diagnosis
Rule out Sinding-Larsen-Johansson (apophysitis) in adolescents, patellofemoral pain syndrome, and Hoffa's fat pad impingement. Location and patient age are key discriminators.
Quick Decision Guide - Anterior Knee Pain
| Condition | Location | Key Feature | Management |
|---|---|---|---|
| Patellar Tendinopathy | Inferior pole patella | Pain with jumping/eccentric load | Eccentric rehab |
| Patellofemoral Pain | Retropatellar/diffuse | Pain with stairs/sitting (movie sign) | VMO strength, tracking |
| Osgood-Schlatter | Tibial tubercle | Adolescent, prominent tubercle | Rest, self-limiting |
| Sinding-Larsen-Johansson | Inferior pole patella | Adolescent apophysitis | Rest, self-limiting |
| Hoffa's Fat Pad | Infrapatellar medial/lateral | Pain with full extension (impingement) | Extension block taping |
MADTendinosis Pathology - MAD
| M | Mucoid degeneration Ground substance changes |
| A | Angiofibroblastic hyperplasia Disorganized collagen + neovessels |
| D | Disorganized collagen Loss of parallel bundle arrangement |
| M | Mucoid degeneration Ground substance changes |
| A | Angiofibroblastic hyperplasia Disorganized collagen + neovessels |
| D | Disorganized collagen Loss of parallel bundle arrangement |
Hook:The tendon is MAD, not inflamed
EEERehab Principles - EEE
| E | Eccentric loading Key to remodeling |
| E | Education Long recovery timeframe (3-6 months) |
| E | Extracorporeal shockwave Adjunct therapy option |
| E | Eccentric loading Key to remodeling |
| E | Education Long recovery timeframe (3-6 months) |
| E | Extracorporeal shockwave Adjunct therapy option |
Hook:EEE for Excellent tendon remodeling
6-FAILSurgical Indications - 6-FAIL
| 6 | 6 months duration Minimum trial of conservative care |
| F | Failed rehab No improvement with eccentrics |
| A | Activity limitation Cannot compete at desired level |
| I | Imaging confirming pathology MRI/US shows focal degeneration |
| L | Localization Pain localized to inferior pole |
| 6 | 6 months duration Minimum trial of conservative care | I | Imaging confirming pathology MRI/US shows focal degeneration |
| F | Failed rehab No improvement with eccentrics | L | Localization Pain localized to inferior pole |
| A | Activity limitation Cannot compete at desired level |
Hook:Surgery only after 6 months of FAILure
Overview and Epidemiology
Patellar tendinopathy, commonly known as Jumper's Knee, is an overuse injury describing pain at the inferior pole of the patella. It is characterized by focal degeneration of the proximal patellar tendon.
Epidemiology:
- Prevalence: High in jumping sports (volleyball 40%, basketball 30%)
- Age: Typically 15-30 years old
- Gender: Male greater than Female (2:1)
- Risk Factors:
- Extrinsic: Hard playing surfaces, increased training volume
- Intrinsic: Poor quadriceps flexibility, vertical jump height (higher jumpers at higher risk), ankle dorsiflexion stiffness
The Jumper's Paradox
Ironically, better athletes are more prone to this condition. Higher vertical jump ability correlates with increased load on the extensor mechanism during landing (eccentric phase), leading to higher injury risk.
Pathophysiology and Mechanisms
Anatomy:
- Patellar Tendon: Connects patella to tibial tubercle
- Inferior Pole: Most common site of pathology (proximal posterior aspect of tendon)
- Vascularity: Posterior proximal insertion is a relatively hypovascular zone ("watershed area")
Pathophysiology (Tendinosis vs Tendinitis):
- Historically termed "tendinitis" implying inflammation
- Current understanding: Degenerative process (Tendinosis)
- Histology:
- Angiofibroblastic hyperplasia: Neovascularization with nerve ingrowth (pain source)
- Mucoid degeneration: Increased ground substance
- Collagen disorganization: Loss of parallel type I collagen bundles
- Absence of inflammatory cells: No neutrophils or macrophages
Why is it painful?
If inflammation is absent, why does it hurt? Pain is driven by neovascularization accompanying neoinnervation (sensory nerve ingrowth) into the degenerative area. Sclerosing therapy targets these neovessels.
The Continuum Model (Cook & Purdam):
Rather than a binary "inflamed versus degenerate" view, tendon pathology is best understood as a continuum, which guides load-based rehabilitation:
| Stage | Tendon state | Reversibility | Management focus |
|---|---|---|---|
| Reactive tendinopathy | Non-inflammatory cell/matrix response to acute overload | Reversible | Reduce load, relative rest, isometrics |
| Tendon disrepair | Greater matrix breakdown, increased cells and vessels | Potentially reversible | Load modification, progressive loading |
| Degenerative tendinopathy | Areas of cell death, disorganised matrix, neovessels | Largely irreversible | Strengthen surrounding intact tissue ("treat the doughnut, not the hole") |
Treat the doughnut, not the hole
In a degenerate tendon, the focal abnormal region (the "hole") will not heal back to normal. Rehabilitation works by loading and strengthening the surrounding intact tendon (the "doughnut") so the tendon-muscle unit tolerates load - which explains why imaging change lags clinical recovery.
Classification Systems
Blazina Classification (Clinical)
Used to grade severity and guide treatment.
| Stage | Symptoms | Function | Treatment |
|---|---|---|---|
| Phase 1 | Pain only after activity | No functional impairment | Ice, NSAIDs, eccentric rehab |
| Phase 2 | Pain during and after activity | Can still compete/perform | Activity mod + intense rehab |
| Phase 3 | Pain during and after | Unable to compete at level | Prolonged rest, consider surgery |
| Phase 4 | Complete tendon rupture | Loss of extension | Surgical repair |
Blazina Transition
Progression from Phase 2 to Phase 3 is the critical tipping point. Once performance is affected (Phase 3), surgical consideration becomes more relevant if rehab fails.
Blazina staging is the most commonly used system in clinical practice.
Clinical Presentation and Assessment
History:
- Anterior knee pain localized to inferior patellar pole
- Aggravated by jumping, landing, deceleration (eccentric load)
- "Movie sign" (pain with prolonged sitting) - can overlap with PFPS
- History of recent increase in training volume
Physical Examination:
Physical Exam Findings
| Manoeuvre | Finding | Significance |
|---|---|---|
| Palpation | Tenderness at inferior pole of patella | Classic site (proximal insertion) |
| Bassett's Sign | Tenderness in extension, disappears in flexion | Differentiates from diffuse PFPS |
| Decline Squat Test | Pain on single-leg decline squat | Loading test for tendinopathy |
| Quad Atrophy | VMO wasting | Chronic inhibition |
| Hamstring/Quad tightness | Reduced flexibility | Predisposing factor |
Bassett's Sign Explained:
- Extension: Patterns tendon is lax; inferior pole palpation is possible.
- Flexion (90 deg): Tendon tightens ("trampoline"); deep palpation of the posterior aspect of the proximal tendon is impalpable.
- Positive sign = Tenderness present in extension, absent in flexion.
Check Hip and Ankle
Always examine the hip (restriction, FAI) and ankle (dorsiflexion restriction). Stiffness above or below forces the knee to absorb more kinetic energy during landing, overloading the tendon.
Investigations
1. Radiographs (X-ray):
- Usually normal
- May show:
- Elongated inferior patellar pole (impingement theory)
- Intratendinous calcification (chronic)
- Osgood-Schlatter or Sinding-Larsen-Johansson sequelae
2. Ultrasound (US):
- First-line imaging modality
- Findings:
- Tendon thickening
- Hypoechoic area (focal degeneration)
- Doppler flow (neovascularization) - correlates with pain
- Advantages: Dynamic, cheap, bilateral comparison
3. MRI:
- High sensitivity (95%)
- Findings: Increased signal intensity on T2/STIR in proximal posterior tendon
- Useful to rule out other pathology (meniscus, cartilage, bone edema)
- Note: MRI signal abnormalities can be present in asymptomatic athletes ("imaging-clinical mismatch"). Treat the patient, not the scan.
Imaging Modality Comparison
| Modality | Pros | Cons |
|---|---|---|
| Ultrasound | Dynamic, shows neovascularization, cheap | Operator dependent |
| MRI | Anatomy definition, rules out other pathology | Expensive, static, high false positive rate |
| X-ray | Rules out bony pathology | Misses soft tissue pathology |
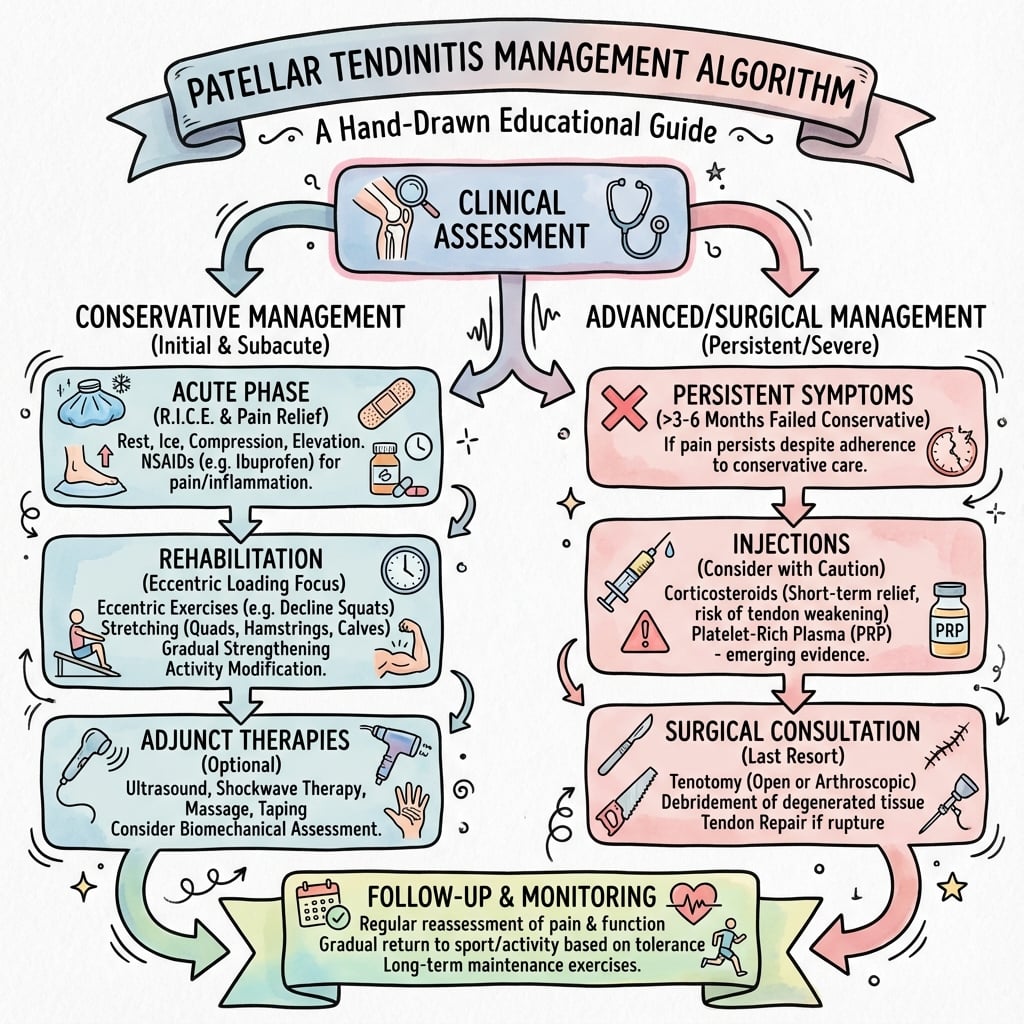
Management
Initial Management (Phase 1-2):
- Relative Rest: Avoid aggravating activities (jumping)
- Ice: For symptom control
- NSAIDs: Short course for analgesia (not healing)
- Biomechanical correction: Orthotics, technique modification
Rehabilitation Protocol (Gold Standard):
- Isometric loading: (e.g., Spanish squat hold) - analgesia effect
- Isotonic loading: Slow heavy resistance
- Eccentric loading: Decline board squats
- Functional/Plyometric: Return to sport progression
Eccentric Strengthening (Decline Board):
- Decline board (25 degrees) isolates patellar tendon (removes calf contribution)
- Perform single-leg squats
- "Pain allowed" protocol (mild pain acceptable during exercise)
- 3 sets x 15 reps, twice daily, 12 weeks minimum
Decline Board Mechanism
The 25-degree decline board increases the knee extension moment and isolates the patellar tendon by minimising calf/ankle-dorsiflexion and hip contribution. In Purdam's pilot, decline-board eccentrics dropped mean VAS from 74 to 29 over 12 weeks while flat-foot squats barely changed - the slope, not the eccentric mode alone, drives the benefit.
Adherence to the eccentric program is the single most important factor in conservative success.
Surgical Technique
Arthroscopic Patellar Tenotomy/Debridement:
Setup:
- Supine, tourniquet, standard portals (AL, AM)
- Knee flexed 90 degrees
Steps:
- Diagnostic scope: Rule out other pathology (plica, meniscal tear, chondromalacia)
- Visualization: View retropatellar fat pad and posterior aspect of patellar tendon
- Debridement:
- Shaver used to resect retropatellar fat pad (visualize proximal tendon insertion)
- Identify "boggy" or degenerate area at inferior pole (proximal posterior tendon)
- Resect focal degenerative tissue
- Some surgeons perform inferior pole osteoplasty (resecting bony beak)
Advantages:
- Smaller incisions
- Faster rehabilitation
- Addresses intra-articular pathology
- Visualizes posterior tendon (site of pathology) without disrupting anterior fibers
Arthroscopy is increasingly preferred for its diagnostic utility and lower morbidity.
Complications
Complications Management
| Complication | Risk Factors | Management |
|---|---|---|
| Tendon Rupture | Steroid injections, aggressive early load | Surgical repair (quad/hamstring augmentation) |
| Persistent Pain | Inadequate resection, wrong diagnosis | Revision surgery vs salvage |
| Infrapatellar Numbness | Damage to infrapatellar branch of saphenous nerve | Observation (often permanent) |
| Infection | Open surgery | Antibiotics +/- debridement |
Tendon Rupture:
- The most devastating complication
- Rare in virgin cases, risk increases with multiple steroid injections
- Requires complex surgical reconstruction (often needs augmentation due to poor tissue quality)
Saphenous Nerve Injury:
- Infrapatellar branch runs transversely across proximal tibia/tendon
- Transverse incisions risk injury causing lateral numbness
- Longitudinal incisions safer
Postoperative Care and Rehabilitation
- Goal: Wound healing, pain control
- WBAT with crutches if needed
- ROM as tolerated
- Isometric quads
- Goal: Normal gait, full ROM
- Closed chain strengthening
- Cycling
- Proprioception
- Goal: Hypertrophy and strength
- Start eccentric loading program
- Increase resistance
- Single leg squats
- Goal: Return to sport
- Plyometrics initiation
- Sport-specific drills
- Return to play when strength over 90% contra-lateral side
Recovery is Slow
Patients must be counseled that surgery is NOT a quick fix. Biology of tendon healing combined with need for strength recovery means return to sport typically takes 4-6 months.
Outcomes and Prognosis
- Conservative: 60-80% success rate with proper eccentric program
- Surgical: 70-90% good/excellent results
- Return to Play:
- 50-60% return to previous level of sport
- Many return to sport but at a lower level or with residual symptoms
- Refractory cases: Consider other diagnoses (Hoffa's fat pad, plica) or look for biomechanical contributors (hip/ankle).
Evidence Base
- Non-randomised pilot in 17 patients (22 tendons) with chronic patellar tendinopathy.
- Decline-board (25 degree) eccentric squats reduced mean VAS from 74.2 to 28.5 over 12 weeks (p=0.004); flat-foot squats only fell 79.0 to 72.3 (p=0.144).
- Six of nine decline-board tendons returned to sport versus one in the flat-squat group.
- RCT of 39 men: peritendinous corticosteroid (CORT), eccentric decline squats (ECC) and heavy slow resistance (HSR), 12 weeks.
- All groups improved at 12 weeks, but CORT gains deteriorated by 6 months while ECC and HSR were maintained.
- HSR produced the highest treatment satisfaction and elevated collagen network turnover; CORT and HSR reduced tendon swelling and vascularisation on ultrasound.
- Randomised controlled trial of 35 patients (40 knees) with grade-IIIB patellar tendinopathy: open patellar tenotomy versus eccentric decline-squat training.
- No difference in VISA score between groups at 12 months; both improved (mean VISA 30 to 70).
- Five of 20 eccentric-training knees required secondary surgery at 3 to 6 months.
- Systematic review of 13 RCTs of treatments for patellar tendinopathy.
- Strong evidence for eccentric training; moderate evidence for heavy slow resistance as an alternative.
- Only limited evidence for surgery, sclerosing injections and shockwave; low-intensity pulsed ultrasound was ineffective.
- Double-blind RCT of 23 patients who had failed nonoperative care: single leukocyte-rich PRP injection plus eccentric exercise versus dry needling plus eccentric exercise.
- PRP improved VISA more than dry needling at 12 weeks (25.4 vs 5.2 points, p=0.02).
- By 26 weeks the groups were equivalent - the early PRP advantage dissipated over time.
- Cross-sectional study of 613 elite Norwegian athletes across 9 sports.
- Overall current prevalence 14.2%, ranging 0% (cycling, orienteering) to 44.6% in volleyball and 31.9% in basketball.
- Prevalence higher in men (13.5%) than women (5.6%); mean symptom duration 32 months.
- Proposes a continuum of tendon pathology: reactive tendinopathy, tendon disrepair, and degenerative tendinopathy.
- Reactive and early disrepair are potentially reversible with load modification; degenerative tendon shows irreversible matrix and cell change.
- Reframes management around staging tendon along the continuum rather than a binary 'inflamed vs degenerate' view.
- Original development and validation of the Victorian Institute of Sport Assessment (VISA) questionnaire for jumper's knee.
- Eight-item, 0-100 score with excellent test-retest and inter-tester reliability (r greater than 0.95).
- Mean scores: 95 in asymptomatic controls, 55 in clinic patients, 22 pre-operatively, recovering to 75 by 12 months post-surgery.
Clinical Decision Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Elite Basketball Player with Knee Pain
"A 24-year-old professional basketball player presents with 6 months of anterior knee pain. It warms up during play but hurts significantly afterwards. He is struggling to dunk. How do you assess him?"
Failed Conservative Management
"This patient has failed 6 months of supervised eccentric rehab and shockwave therapy. MRI shows focal mucoid degeneration at the proximal posterior tendon. Discuss surgical options."
Mechanism of Decline Squats
"Why do we prescribe decline board squats specifically? What is the biomechanical rationale?"
MCQ Practice Points
Pathology
Q: What is the primary histological finding in patellar tendinopathy? A: Angiofibroblastic hyperplasia and mucoid degeneration, with a distinct absence of inflammatory cells (tendinosis, not tendinitis).
Classic Sign
Q: What is Bassett's Sign and what does it indicate? A: Tenderness at the inferior pole of the patella in full extension that disappears in 90 degrees of flexion. It is pathognomonic for patellar tendinopathy.
Contraindication
Q: Why are corticosteroid injections contraindicated in the patellar tendon? A: They inhibit collagen synthesis and cause necrosis, leading to a significantly increased risk of acute tendon rupture.
Imaging Findings
Q: What are the characteristic ultrasound findings? A: Thickening of the tendon, hypoechoic areas (focal degeneration), and Doppler flow (neovascularization) which correlates with pain.
Rehabilitation
Q: What is the gold standard rehabilitation protocol? A: Eccentric strengthening, specifically using a 25-degree decline board to isolate the patellar tendon mechanism.
Classification
Q: What defines Stage 3 in the Blazina classification? A: Pain during and after activity that causes a decrease in sports performance. This is often the tipping point for considering surgery.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Patellar tendinopathy is fundamentally a load-related overuse disorder, so prevalence tracks explosive leg-extensor sport worldwide rather than any single region. In a cross-sectional study of 613 elite Norwegian athletes, overall current prevalence was 14.2%, peaking at 44.6% in volleyball and 31.9% in basketball, with zero cases in cycling and orienteering.
- Symptoms are typically chronic and performance-limiting: mean symptom duration was 32 months and mean VISA score 64 in affected athletes.
- Men are affected roughly twice as often as women (13.5% versus 5.6% in the same elite cohort), consistent with greater jump height and explosive loading.
Outcome Measurement (international standard):
- The VISA-P (Victorian Institute of Sport Assessment - Patella) is the validated, internationally adopted patient-reported outcome (8 items, 0-100). It was developed and validated with excellent reliability (r greater than 0.95) and is the comparator used in essentially all modern trials. Cross-culturally adapted versions exist in many languages, making it the common currency for comparing studies across countries.
Major Guidance & Evidence Synthesis - Side by Side
| Source | Position on patellar tendinopathy | Evidence level |
|---|---|---|
| Larsson systematic review (KSSTA, Europe) | Strong evidence for eccentric training; moderate for heavy slow resistance; only limited evidence for surgery, sclerosing and shockwave | Strong (eccentrics) / Limited (surgery, injections) |
| BJSM / international sports-medicine consensus | Progressive tendon loading (eccentric or heavy slow resistance) first line; load management rather than complete rest; isometrics for in-season analgesia | Moderate-Strong |
| NICE / UK CKS (musculoskeletal overuse) | Activity/load modification, structured physiotherapy-led loading, analgesia; corticosteroid injection discouraged for load-bearing tendons | Consensus / Low-Moderate |
| JBJS RCT evidence base (surgery) | Open tenotomy offers no advantage over eccentric training at 12 months; reserve surgery for failure of at least 3 to 6 months of structured loading | Level I (single RCT) |
Practice Variation:
- There is no joint-registry equivalent for tendinopathy (registries cover arthroplasty/implants), so the evidence base is trial- and consensus-driven rather than registry-driven.
- Practice differs mainly in the interventional middle ground: PRP, sclerosing/high-volume injection and extracorporeal shockwave are used more readily in some sports-medicine systems (often physician-led, before any surgical referral), whereas other systems move from supervised loading straight toward surgical opinion. The high-level evidence for these adjuncts remains limited, so their use reflects local resources and clinician preference rather than strong guideline mandate.
- The one near-universal agreement across all guidance is that structured progressive loading is first line and intratendinous corticosteroid is avoided because of rupture risk and inferior long-term outcomes.
Patellar Tendinitis Essentials
Clinical summary
Key Facts
- •Degenerative process (tendinosis), NOT inflammatory
- •Inferior pole of patella is classic site
- •Bassett's sign: Tender extension, non-tender flexion
- •Decline board eccentric squats = Gold Standard rehab
Must Know
- •NO STEROIDS (rupture risk)
- •VISA-P score is key monitoring tool
- •Surgery only after 6 months failed rehab
- •Return to sport takes 4-6 months post-op
Imaging
- •Ultrasound: Hypoechoic, thick, Doppler flow
- •MRI: T2 high signal posterior proximal tendon
- •X-ray: Usually normal (rule out other causes)
- •Doppler flow correlates with active pain
Surgical Options
- •Arthroscopic debridement (posterior tendon)
- •Open debridement
- •Tenotomy
- •Inferior pole osteoplasty (if impingement)