Common shoulder injury in young athletes | Direct fall onto the point of the shoulder | Graded by the Rockwood classification | Low grades treated nonoperatively, high grades debated
- Mechanism is a direct blow to the point of the shoulder with the arm adducted (a fall in contact sport or off a bike) - the force drives the acromion down and away from the clavicle
- The Rockwood classification (types I to VI) drives treatment: it is based on the direction and amount of clavicle displacement and which ligaments are torn
- Low-grade injuries (types I and II) are treated nonoperatively with a sling and early movement, and long-term outcomes are good despite some later radiographic changes
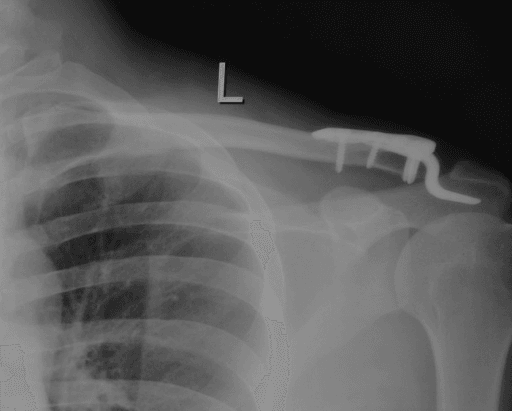
- High-grade injuries (types IV, V and VI) are generally treated surgically because the clavicle is grossly displaced (buttonholed posteriorly, markedly elevated, or driven downward)
- Type III is the real controversy: meta-analyses show no clear functional advantage for early surgery, so most are given a trial of nonoperative care, with surgery reserved for those who stay symptomatic
- “The acromioclavicular ligaments resist horizontal (anteroposterior) translation; the coracoclavicular ligaments resist vertical (superior) translation - know which fails in which grade
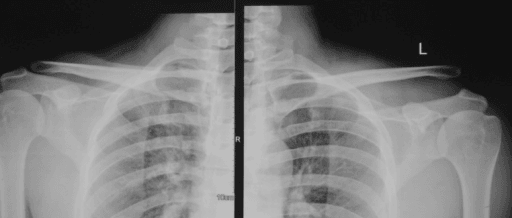
- “Always image and assess BOTH shoulders so you can compare the coracoclavicular distance - the clavicle does not rise, the arm and scapula drop under gravity
- “A type IV injury (clavicle buttonholed posteriorly through trapezius) is best seen on the axillary view - never forget the axillary radiograph
- “Counsel every patient that the cosmetic bump may persist even after good treatment - function, not appearance, is the goal
The acromioclavicular (AC) ligaments resist horizontal (anteroposterior) translation; the coracoclavicular (CC) ligaments - conoid and trapezoid - resist vertical (superior) translation. Examiners love asking which fails in which grade, so anchor every answer on this.
The Rockwood classification (I to VI) is the framework for management. I and II are nonoperative, IV, V and VI are generally operative, and III is the controversy - learn the dividing lines, not just the list.
A type IV injury has the clavicle buttonholed posteriorly through the trapezius - it can look deceptively mild on the AP film. The axillary view is essential and is what reveals it. Always request it.
Grade by comparing the coracoclavicular distance with the normal side. Remember the clavicle does not truly "rise" - the arm and scapula sag under gravity, so weighted stress views are now largely abandoned.
Overview
The acromioclavicular joint is the small joint where the lateral end of the clavicle meets the acromion of the scapula. It is one of the few bony links between the arm and the axial skeleton, and it is injured surprisingly often - typically in young, active people who fall directly onto the point of the shoulder during contact sport, cycling, or a simple trip.
For the exam, the whole topic hangs on three ideas: the anatomy (two ligament groups controlling two directions of stability), the Rockwood classification (which grades the injury and decides treatment), and the management debate (low grades are easy - nonoperative; high grades are operative; type III is genuinely contested). Get these three threads clear and you can answer almost any question on this joint.
Anatomy and Biomechanics
The acromioclavicular joint is a plane synovial joint with a small fibrocartilaginous disc that degenerates from early adulthood. Its stability comes from two separate ligament groups, and understanding which controls which direction is the single most useful piece of knowledge in this topic.
- Where it runs
- Directly across the joint (superior part is the strongest)
- What it controls
- Horizontal (anteroposterior) stability - stops the clavicle sliding front-to-back
- When it fails
- Torn first - their loss allows the clavicle to translate backward (key in type IV)
- Where it runs
- From the coracoid process up to the undersurface of the clavicle
- What it controls
- Vertical (superior) stability - stops the clavicle riding upward
- When it fails
- Torn in higher grades - their loss increases the coracoclavicular distance
- Where it runs
- Posteromedial, cone-shaped
- What it controls
- Main restraint to superior displacement and a key rotational control
- When it fails
- Failure is central to the vertical instability of types III and above
- Where it runs
- Anterolateral, flatter
- What it controls
- Resists axial compression and helps horizontal control
- When it fails
- Contributes to instability as displacement increases
- Where it runs
- Muscle fascia draping over the joint and clavicle
- What it controls
- Adds a final layer of soft-tissue restraint
- When it fails
- Stripped only in the worst injuries - its loss permits gross displacement (types IV to VI)
The practical message is that an injury progresses in a predictable order: first the AC ligaments (horizontal instability), then the CC ligaments (vertical instability and an increased CC distance), and finally the deltotrapezial fascia (gross displacement). This sequence is exactly what the Rockwood classification captures.
Anatomy of Coracoclavicular Reconstruction
When coracoclavicular reconstruction is chosen, restoring the anatomic footprints of the conoid and trapezoid matters, because anatomic reconstruction controls both vertical and rotational/horizontal stability better than a non-anatomic transfer.
- Position
- Posteromedial (at the conoid tubercle)
- Approximate attachment from the lateral clavicle end
- About 45 mm medial to the lateral end of the clavicle
- Position
- Anterolateral (the trapezoid line)
- Approximate attachment from the lateral clavicle end
- About 25 mm medial to the lateral end of the clavicle
- Anatomic reconstruction places the graft and tunnels at these two footprints to recreate both the conoid and trapezoid, restoring vertical stability and the rotational/horizontal control that a single central construct cannot.
- Non-anatomic reconstruction (the modified Weaver-Dunn coracoacromial-ligament transfer) is biomechanically weaker than the native CC ligaments and is now mostly reserved for chronic cases or as an augment.
- Tunnels must be carefully sized and placed - drilling at or near these footprints is exactly where the recognised complication of a clavicle or coracoid fracture around the tunnel arises.
For anatomic CC reconstruction, remember the two footprints measured from the lateral end of the clavicle: conoid at about 45 mm (posteromedial), trapezoid at about 25 mm (anterolateral). Recreating both restores vertical AND rotational control, which is why anatomic graft reconstruction outperforms the non-anatomic Weaver-Dunn transfer - at the cost of tunnel-related fracture risk.
Pathophysiology
The injury is a mechanical failure of restraints in sequence, driven by a single force. A direct downward blow to the point of the shoulder (with the arm adducted) drives the acromion and scapula downward and medially while the clavicle, strutted against the sternum, stays put. The result is that the energy is concentrated across the acromioclavicular ligaments and then the coracoclavicular ligaments.
The failure cascade:
- Low energy stretches or partially tears the AC ligaments only - the joint stays reduced (type I) or subluxes a little (type II), and because the CC ligaments hold, the clavicle does not ride up.
- Higher energy completes the AC tear and then ruptures the CC ligaments - the clavicle loses its vertical restraint and the coracoclavicular distance increases (type III).
- The greatest energy also strips the deltotrapezial fascia, removing the last soft-tissue restraint and allowing gross, fixed displacement - posterior (IV), severe superior (V), or inferior (VI).
Because the clavicle is anchored medially at the sternoclavicular joint, the apparent "elevation" of the clavicle is really the arm and scapula dropping under the weight of the limb once the restraints fail - the basis for comparing both shoulders rather than relying on weighted stress views.
The late pathophysiology explains the chronic problems: a torn intra-articular disc and an unstable joint drive post-traumatic osteoarthritis and distal clavicle osteolysis, while a malreduced joint produces scapular dyskinesis and persistent pain even when the acute injury looked modest.
A common exam phrasing: "the clavicle is elevated." Strictly, the clavicle stays put and the weight of the arm pulls the scapula and shoulder downward, so the clavicle only appears to rise. This is why old weighted stress views were unreliable and are no longer routine - and why you always compare both sides on one film.
Classification (Rockwood)
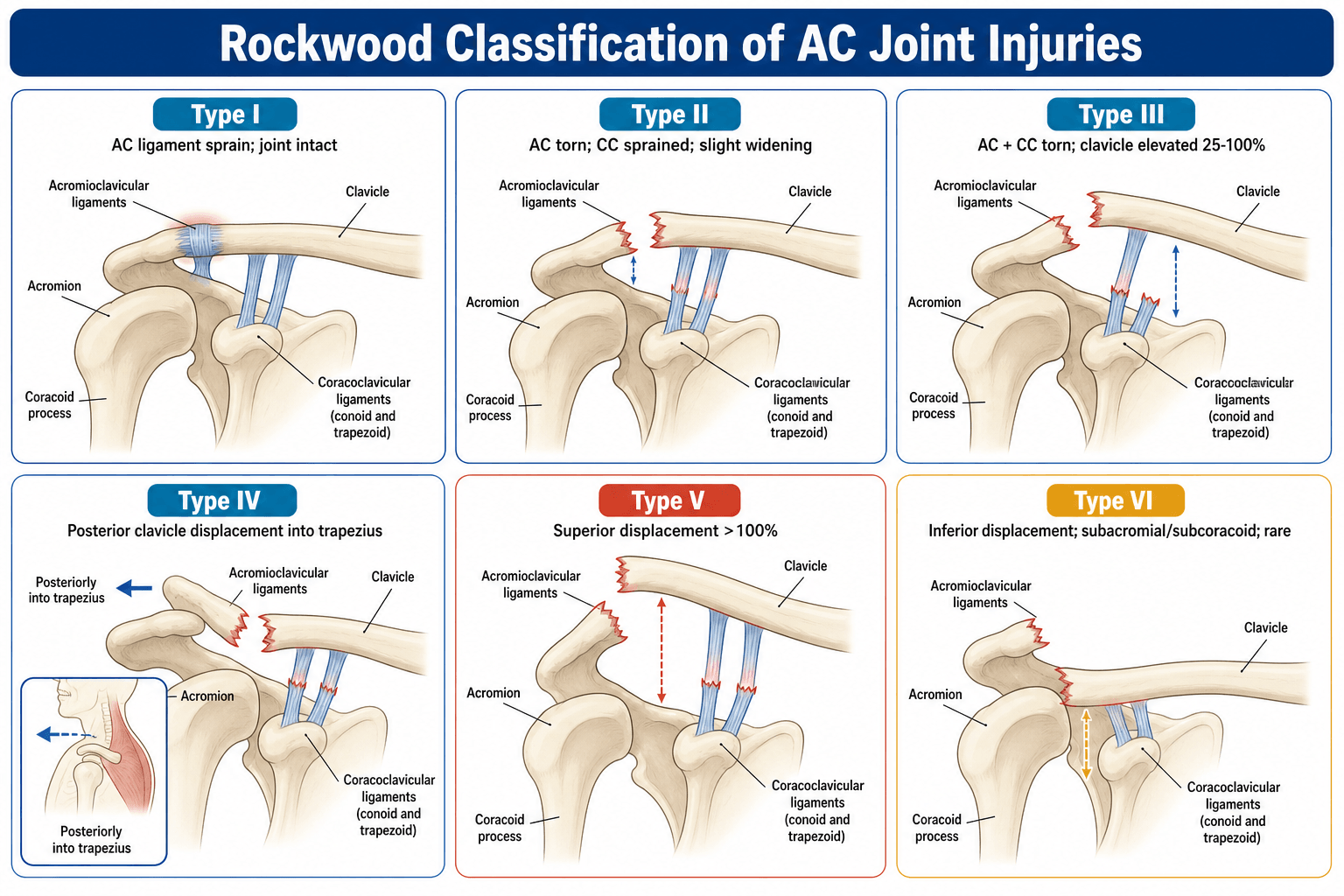
The Rockwood classification divides acromioclavicular injuries into six types based on the direction and degree of displacement and which structures are torn. It expanded the older three-type Tossy system to capture the severe displacement patterns (types IV to VI).
Type I is an AC ligament sprain with no displacement and a normal radiograph - the joint is stable. Type II is a complete AC ligament tear with intact CC ligaments: the joint subluxes and the AC space widens, but the coracoclavicular distance stays near normal because the vertical restraint is preserved. Both are managed nonoperatively.
- What is torn
- AC ligaments sprained (not torn)
- Displacement
- None - joint stable, radiograph normal
- Usual treatment
- Nonoperative: sling, analgesia, early movement
- What is torn
- AC ligaments torn, CC ligaments intact
- Displacement
- Joint subluxed, slightly widened; CC distance near normal
- Usual treatment
- Nonoperative: sling and rehabilitation
- What is torn
- Both AC and CC ligaments torn
- Displacement
- CC distance increased 25 to 100 percent versus the normal side
- Usual treatment
- Controversial - usually a trial of nonoperative care first
- What is torn
- AC and CC torn; clavicle buttonholes posteriorly through trapezius
- Displacement
- Posterior displacement - seen on the axillary view
- Usual treatment
- Operative - displacement will not reduce itself
- What is torn
- AC and CC torn plus deltotrapezial fascia stripped
- Displacement
- Gross superior displacement - CC distance more than 100 percent of normal
- Usual treatment
- Operative
- What is torn
- AC and CC torn; clavicle driven inferior (subcoracoid)
- Displacement
- Very rare; clavicle lies below the coracoid
- Usual treatment
- Operative
Some surgeons split type III into IIIA (stable, asymptomatic with rehabilitation) and IIIB (symptomatic, dynamically unstable scapula) to help decide who might benefit from surgery - but the headline for the exam is simply that III is the grey zone between clearly nonoperative (I and II) and clearly operative (IV to VI).
Clinical Presentation and Examination
The typical patient is a young athlete who fell directly onto the point of the shoulder and now has pain, swelling, and often a visible step or bump at the lateral clavicle.
Direct fall onto the adducted shoulder (rugby, cycling, skiing). Pain localised to the top of the shoulder, worse with overhead and cross-body movements and when carrying a bag on that side.
A step deformity or prominent lateral clavicle (the more severe, the more obvious). Inspect the skin - tenting or threatened skin in a high-grade injury is an urgent surgical sign.
Tenderness directly over the joint. Test vertical stability (press the clavicle down - it springs back, the "piano-key" sign) and horizontal stability (anteroposterior translation), because horizontal instability pushes a borderline type III toward surgery.
Cross-body (cross-arm) adduction reproduces pain by compressing the joint. Scapular dyskinesis (an abnormally moving shoulder blade) suggests a dynamically unstable, symptomatic type III.
Investigations
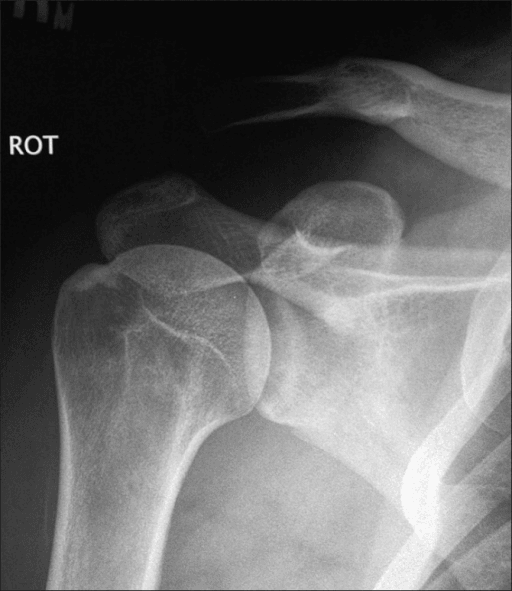
Diagnosis is clinical and radiographic. The aims of imaging are to confirm the injury, exclude an associated fracture, and grade it accurately, because the grade decides treatment.
- What it shows
- The joint and the coracoclavicular distance, compared with the normal side
- Why it matters
- The mainstay - lets you measure the increase in CC distance that defines the grade
- What it shows
- A cleaner, less overpenetrated picture of the joint
- Why it matters
- The dedicated view for the acromioclavicular joint - removes overlap from the scapular spine
- What it shows
- Anteroposterior position of the clavicle relative to the acromion
- Why it matters
- The only way to reliably detect the posterior displacement of a type IV
- What it shows
- Displacement with a weight pulling the arm down
- Why it matters
- Largely abandoned - painful, often unhelpful, and the arm-drop concept makes them unreliable
- What it shows
- Ligament detail and associated intra-articular or rotator cuff injury
- Why it matters
- Not routine; reserved for diagnostic doubt or to plan complex or chronic reconstruction
If you remember only one investigation point: always look at (or ask for) the axillary view. A type IV injury can look modest on the AP film, and missing the posterior displacement of the clavicle means missing an operative injury. The Zanca view is the dedicated AP view for grading.
Management
Treatment is decided by the Rockwood grade, modified by the patient's symptoms, demands, and dynamic instability.
Low-grade injuries are managed nonoperatively and do very well. The plan is simple:
- Sling for comfort for a short period (days to a couple of weeks)
- Analgesia and ice early
- Early range-of-motion and a graded return to strengthening and sport
- Counsel that a small bump may persist and that late radiographic changes (distal clavicle osteolysis, ossification, mild degeneration) are common but usually do not cause symptoms
A small minority develop persistent pain from post-traumatic acromioclavicular arthritis or distal clavicle osteolysis, which can later be treated with a distal clavicle excision if injection and rehabilitation fail.
In a very high-grade injury (often a type V), the displaced clavicle can tent or threaten the overlying skin. Skin compromise risks an open injury and demands urgent surgical reduction rather than a wait-and-see approach. Always examine the skin over the prominent clavicle.
Complications
- When it happens
- After any displaced injury, treated either way
- What to do
- Counsel beforehand - function is the goal, the bump often remains
- When it happens
- Late, after low- and high-grade injuries alike
- What to do
- Injection and rehabilitation first; distal clavicle excision if it fails
- When it happens
- After surgery, especially with suture-only constructs
- What to do
- A leading cause of revision - choose a construct matched to the injury
- When it happens
- Hook-plate erosion of the acromion; button or suture cut-out
- What to do
- Plan hook-plate removal once healed; counsel about implant-related reoperation
- When it happens
- Around drill tunnels for CC reconstruction
- What to do
- A recognised technical complication - careful tunnel placement and sizing
- When it happens
- After operative treatment
- What to do
- The single commonest surgical complication - meticulous technique and counselling
The key exam point is that surgery is not risk-free: the complication profile (infection, hardware problems, loss of reduction, and fractures around tunnels) is exactly why the evidence pushes toward nonoperative care for type III injuries that are settling.
Clinical Relevance
Acromioclavicular injuries are bread-and-butter for the shoulder, trauma, and sports clinics and a favourite viva topic because they test clear, structured thinking. In clinic the everyday task is grading the injury correctly and counselling a young athlete on a realistic recovery. In the viva the examiner will push you on the anatomy (which ligament controls which direction), on not missing a type IV (axillary view), and on the type III debate - where a candidate who quotes the evidence and offers a sensible "trial of nonoperative care, surgery for failures" plan stands out. Knowing which grade goes which way, and why, is the core that examiners probe.
Guidelines, Registries and Global Practice
- Consensus across regions is strongest at the extremes: types I and II are managed nonoperatively, and types IV, V and VI are managed operatively. This is reflected in major trauma and sports-medicine teaching worldwide (AAOS-aligned US practice, BOA/UK practice, and AO Foundation principles for the surgical constructs).
- Type III is where guidance differs, but the difference is one of threshold rather than principle. The pooled evidence (multiple meta-analyses) shows no clear functional advantage for early surgery, so most guidance now favours an initial trial of nonoperative care with surgery reserved for persistent symptoms - a position increasingly shared across the FRCS, FRACS, and ABOS curricula.
- The "type IIIA versus IIIB" refinement (stable and asymptomatic versus dynamically unstable and symptomatic) is used in many centres to select the minority of type III patients for surgery, particularly overhead athletes and heavy manual workers.
- Global practice variation in the surgical technique (hook plate versus suture-button versus tendon-graft reconstruction, open versus arthroscopic) largely reflects local expertise, implant availability, and cost rather than clear evidence that one is superior - the systematic-review data show comparable outcomes between open and arthroscopic methods.
Memory aids
ACDCRockwood Grades by Ligament Damage
Hook:Climb the ACDC ladder: AC sprain, Complete AC tear, Dislocation of both ligaments, then Catastrophic types IV to VI.
PSIDirections of Displacement (Types IV, V, VI)
Hook:The severe grades go in three directions - PSI: Posterior (IV), Superior (V), Inferior (VI).
BUMPWhat To Check On Examination
Hook:Examine the BUMP - Bump and tenderness, Up-down stability, Movement front-to-back, Provocation and skin.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old rugby player fell onto the point of his shoulder and has a visible bump and tenderness over the lateral clavicle. The examiner shows an AP radiograph with the distal clavicle elevated and asks how you would classify and manage it.”
“A 38-year-old manual labourer has a grossly prominent clavicle after a motorbike crash, with the skin tented over it. The coracoclavicular distance is more than double the normal side. How do you proceed and what are the surgical options and risks?”
Anatomy
- AC ligaments resist horizontal (anteroposterior) displacement
- CC ligaments (conoid and trapezoid) resist vertical (superior) displacement
- Conoid is the main superior restraint; trapezoid resists axial compression
- Deltotrapezial fascia stripped only in the worst injuries (types IV to VI)
Rockwood Classification
- I - AC sprain, normal radiograph; II - AC torn, CC intact, subluxed
- III - both AC and CC torn, CC distance up 25 to 100 percent (controversial)
- IV - posterior (buttonholed through trapezius); V - superior over 100 percent
- VI - inferior (subcoracoid), very rare
Investigations
- AP both shoulders to compare coracoclavicular distance
- Zanca view - dedicated AP view of the joint
- Axillary view - essential to detect a type IV
- Weighted stress views largely abandoned; MRI only for doubt or planning
Management and Red Flags
- Types I to II nonoperative; types IV to VI operative; type III trial of nonoperative first
- No clear functional benefit from early surgery for type III (meta-analyses)
- Tented or threatened skin (often type V) means urgent surgery
- Surgery carries real risk - loss of reduction about 20 percent, infection commonest
Evidence
Operative Versus Nonoperative for Acute High-Grade Dislocations (Systematic Review and Meta-Analysis)
- Meta-analysis of 19 comparative studies, 954 patients with acute high-grade (Rockwood III to V) injuries
- No clinically meaningful difference in functional outcome scores (DASH; Constant difference small and likely not clinically significant)
- Surgery gave better cosmetic appearance and radiographic reduction
- Nonoperative treatment gave faster return to work and far fewer implant complications and infections
Surgical Versus Conservative Treatment of Rockwood Type III (Meta-Analysis)
- Meta-analysis of 10 trials specifically addressing Rockwood type III dislocations
- No significant difference between surgery and conservative care in pain, strength, post-traumatic arthritis, or functional scores (Constant, UCLA, DASH and others)
- Conservative care had less ossification of the coracoclavicular ligament and less distal clavicle osteolysis
- Surgery was better only at maintaining anatomic reduction
Operative Techniques for Acromioclavicular Reconstruction (Systematic Review and Meta-Analysis)
- 58 articles, 1704 patients across many reconstruction techniques (suture-button, TightRope, tendon graft, Weaver-Dunn)
- Overall failure (loss of reduction) rate 20.8 percent and overall complication rate 14.2 percent
- Commonest complications were infection (6.3 percent), coracoid or clavicle fracture (5.7 percent), and hardware or button failure (4.2 percent)
- No difference between open and arthroscopic techniques in loss of reduction, complications, or revision
Long-Term Outcome of Nonoperative Rockwood I and II Injuries (Cohort Study)
- Cohort of 75 patients with Rockwood I and II injuries, median follow-up about 7 years
- Good functional outcome: mean Constant score 88.6 in the injured shoulder versus 93.3 in the uninjured side (small, clinically minor difference)
- Radiographic changes were common - distal clavicle osteolysis in 31 percent and ligament ossification in 29 percent of injured shoulders
- These radiographic changes did not translate into clinically relevant loss of function