Repetitive-stress osteolysis of the lateral clavicle | Young athletic adults, especially weightlifters | Diagnose on Zanca view and MRI | Most respond to activity modification; surgery is distal clavicle excision
- What it is: a painful, self-limiting but often recurrent osteolysis of the lateral end of the clavicle caused by repetitive microtrauma or direct injury to the acromioclavicular joint
- Who gets it: young athletic adults, especially weightlifters (bench press, overhead press, push-ups), overhead athletes, and manual labourers - classically called 'weightlifter's shoulder'
- How it presents: insidious aching pain over the AC joint, worse with cross-body adduction, overhead activity, and at night; local tenderness over the distal clavicle
- The key investigation: a Zanca view (15-degree cephalic tilt anteroposterior radiograph) shows osteopenia, cystic change, tapering or erosion of the distal clavicle; MRI confirms bone marrow oedema and excludes other pathology
- Management: stop the offending activity, modify technique, physiotherapy, and NSAIDs; if symptoms persist beyond 6 to 12 months, distal clavicle excision (open or arthroscopic) gives reliable relief
- “The Zanca view is essential - a standard AP shoulder often misses the subtle osteopenia and cystic change at the distal clavicle
- “Cross-body adduction test reproduces pain by compressing the AC joint - it is sensitive but not specific
- “Always ask about bench-press volume, overhead lifting, and training changes - the history is often diagnostic
- “MRI is the best second-line test when radiographs are equivocal or when you need to exclude rotator cuff or labral pathology
A standard shoulder AP will often miss distal clavicle osteolysis. The Zanca view (15-degree cephalic tilt AP centred on the AC joint) is the view that shows the osteopenia, cystic change, and tapering of the lateral clavicle. Always request it when you suspect this diagnosis.
Ask specifically about bench-press volume, overhead lifting, push-ups, and training changes. Distal clavicle osteolysis is a repetitive-stress injury; the activity history is usually more revealing than any single physical sign.
AC joint osteoarthritis also causes AC joint pain and cross-body adduction tenderness, but it occurs in older patients and shows joint-space narrowing, osteophytes, and subchondral sclerosis rather than osteolysis and cystic change of the distal clavicle.
When non-operative management fails, the operation is resection of the distal 5 to 10 mm of clavicle (open or arthroscopic). Do not fuse the AC joint or perform a Weaver-Dunn for isolated osteolysis - excision is the evidence-based procedure.
Overview
Distal clavicle osteolysis is a painful, non-infectious resorption of the lateral end of the clavicle that most often affects young athletic adults. It was first described in weightlifters and is still commonly called "weightlifter's shoulder", although it is now recognised in anyone who loads the acromioclavicular joint repetitively - overhead athletes, manual labourers, and military personnel.
The condition is important because it is often misdiagnosed as rotator cuff tendinopathy, AC joint arthritis, or a cervical radiculopathy. The history of repetitive loading (especially bench press or overhead press) and the characteristic imaging on a Zanca view usually make the diagnosis straightforward once it is considered. Most cases respond to activity modification and physiotherapy; a minority need surgical excision of the distal clavicle, which is a reliable and low-morbidity operation.
For the exam, the key threads are: the mechanism (repetitive microtrauma versus post-traumatic), the imaging (Zanca view and MRI), the differential (AC arthritis, rotator cuff disease, cervical spine), and the treatment (activity modification then distal clavicle excision).
Anatomy
The acromioclavicular joint
The acromioclavicular (AC) joint is a diarthrodial synovial joint between the lateral end of the clavicle and the medial facet of the acromion. It is surrounded by a thin capsule reinforced by the superior and inferior AC ligaments. The coracoclavicular ligaments (conoid and trapezoid) sit medial to the joint and are the main vertical stabilisers; they do not cross the joint itself but are critical to AC joint mechanics.
The AC joint has a small meniscus-like intra-articular fibrocartilaginous disc that degenerates with age. In young athletes this disc is still present and the joint surfaces are relatively congruent. The joint is subjected to compressive, shear, and rotational forces with every overhead movement and loaded upper-limb exercise.
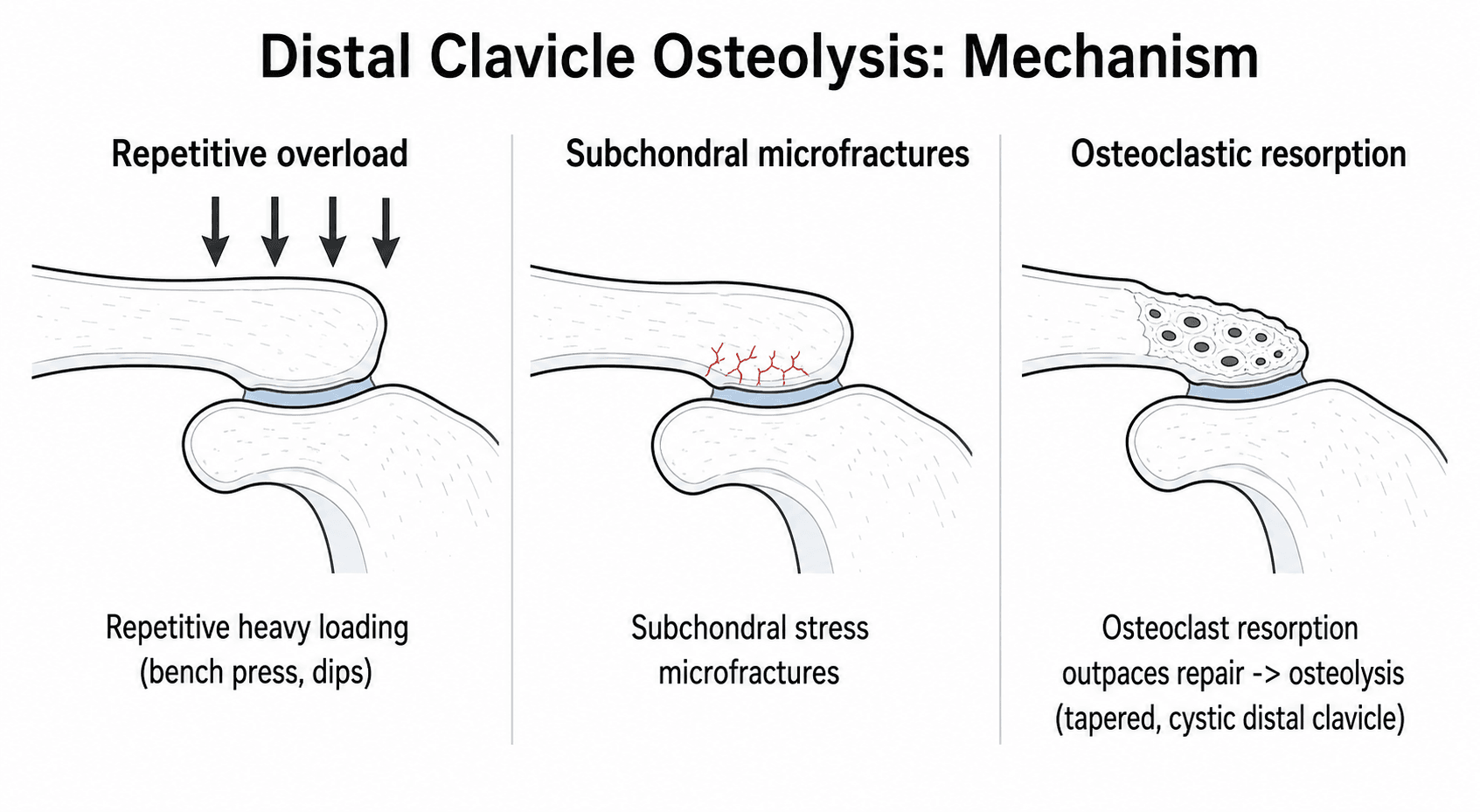
Pathophysiology of osteolysis
The exact mechanism is not fully understood, but the leading theory is repetitive microtrauma causing an imbalance between bone resorption and formation at the distal clavicle:
- Mechanical overload: high-volume bench pressing, overhead pressing, push-ups, and heavy manual work apply repeated compressive and shear forces across the AC joint. The distal clavicle, with its relatively small cross-sectional area and cortical shell, is vulnerable to stress-induced bone resorption.
- Vascular compromise: some authors propose that repetitive loading impairs the subchondral blood supply of the lateral clavicle, leading to avascular bone resorption similar to osteonecrosis.
- Inflammatory cascade: microfractures and trabecular damage trigger an inflammatory response with osteoclast activation, producing the cystic change and tapering seen on imaging.
The process is not neoplastic, not infectious, and not truly inflammatory in the sense of rheumatoid arthritis. It is a stress response of bone that can stabilise or even reverse if the loading is removed.
The pathophysiology is stress-induced bone resorption, not infection or tumour. If asked in a viva, emphasise repetitive microtrauma, osteoclast activation, and the potential for reversal with activity modification.
Pathophysiology
Mechanism of osteolysis
The exact mechanism is not fully understood, but the leading theory is repetitive microtrauma causing an imbalance between bone resorption and formation at the distal clavicle:
- Mechanical overload: high-volume bench pressing, overhead pressing, push-ups, and heavy manual work apply repeated compressive and shear forces across the AC joint. The distal clavicle, with its relatively small cross-sectional area and cortical shell, is vulnerable to stress-induced bone resorption.
- Vascular compromise: some authors propose that repetitive loading impairs the subchondral blood supply of the lateral clavicle, leading to avascular bone resorption similar to osteonecrosis.
- Inflammatory cascade: microfractures and trabecular damage trigger an inflammatory response with osteoclast activation, producing the cystic change and tapering seen on imaging.
The process is not neoplastic, not infectious, and not truly inflammatory in the sense of rheumatoid arthritis. It is a stress response of bone that can stabilise or even reverse if the loading is removed.
The pathophysiology is stress-induced bone resorption, not infection or tumour. If asked in a viva, emphasise repetitive microtrauma, osteoclast activation, and the potential for reversal with activity modification.
Classification
Mechanism: Repetitive microtrauma from weightlifting, overhead sport, or manual labour.
Typical patient: Young adult male weightlifter or overhead athlete.
Management emphasis: Activity modification is the cornerstone; surgery only after prolonged failure.
There is no universally accepted radiographic staging system for distal clavicle osteolysis. In practice, severity is described by the extent of bone loss (mild tapering versus marked osteolysis) and the response to activity modification.
Clinical Presentation
History
The typical patient is a man aged 20 to 40 years who reports insidious aching pain over the AC joint, often localised to the lateral end of the clavicle. The pain is:
- Worse with cross-body adduction (reaching across the chest), overhead activity, and pushing movements
- Exacerbated by bench press, overhead press, dips, and push-ups
- Often present at night, especially when lying on the affected side
- Associated with a recent increase in training volume or intensity in weightlifters
In post-traumatic cases there is a history of a direct blow to the point of the shoulder or a fall onto an outstretched hand. In iatrogenic cases there is a history of previous AC joint surgery with hardware or synthetic ligament.
Examination
- Inspection: there may be subtle swelling or prominence over the AC joint, but often the shoulder looks normal.
- Palpation: tenderness over the distal clavicle and AC joint is the most consistent sign. Palpate with the thumb posterior to the clavicle and the index finger anterior to feel the joint line.
- Active and passive range of motion: usually full, but pain at the extreme of cross-body adduction and end-range flexion/abduction.
- Special tests:
- Cross-body adduction test: the arm is passively brought into 90 degrees of flexion and then adducted across the chest. Pain over the AC joint is positive. This test compresses the AC joint and reproduces symptoms.
- Active compression test (O'Brien test): the arm is forward-flexed to 90 degrees, adducted 10 to 15 degrees across the body, and internally rotated with the thumb down. The patient resists downward pressure. Pain localised to the AC joint (rather than deep in the shoulder) suggests AC joint pathology.
- Paxinos test: the examiner's thumb is placed on the posterior aspect of the acromion and the index finger on the distal clavicle; squeezing together reproduces AC joint pain.
The cross-body adduction test is sensitive for AC joint pathology but not specific - it will also be positive in AC joint arthritis and osteolysis. The key is to combine the test with the patient's age, activity history, and imaging.
Investigations
Radiographs
The Zanca view is the single most important radiograph. It is an anteroposterior view with a 15-degree cephalic tilt, centred on the AC joint, which projects the joint clear of the scapular spine and humeral head.
Findings on the Zanca view include:
- Osteopenia of the lateral clavicle
- Subchondral cystic change within the distal clavicle (and occasionally the medial acromion)
- Tapering, pointing, or erosion of the lateral clavicle tip
- Widening of the AC joint space due to bone loss rather than true dislocation
- Loss of the normal cortical margin at the distal clavicle
A standard shoulder AP may miss these subtle changes because the AC joint is superimposed on the scapular spine and humeral head. Always request a Zanca view when distal clavicle osteolysis is suspected.
Magnetic resonance imaging
MRI is the best second-line investigation. It is indicated when:
- Radiographs are equivocal
- There is suspicion of associated pathology (rotator cuff tear, labral tear, cervical radiculopathy)
- Symptoms are atypical and the diagnosis is uncertain
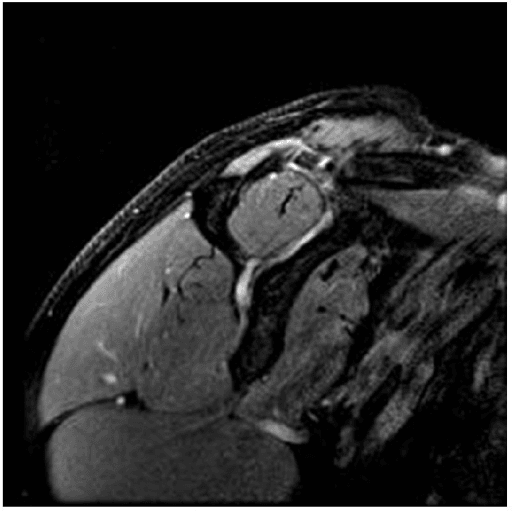
MRI findings:
- Bone marrow oedema in the distal clavicle on fluid-sensitive sequences (T2 fat-suppressed or STIR)
- Subchondral cystic change within the distal clavicle
- Joint effusion and capsular thickening
- Absence of a mass or destructive lesion (helping to exclude tumour or infection)
Other imaging
- CT scan: rarely needed, but can delineate bone loss and cystic change when surgical planning is complex (for example after previous surgery or fracture)
- Bone scintigraphy: not routine, but will show focal increased uptake in the distal clavicle if performed
- Ultrasound: can demonstrate AC joint effusion and guide injection, but is not diagnostic for osteolysis
- Role
- First-line investigation
- Key findings
- Osteopenia, cystic change, tapering, loss of cortical margin at distal clavicle
- Role
- Second-line; equivocal radiographs or associated pathology
- Key findings
- Bone marrow oedema, subchondral cysts, joint effusion; excludes tumour and infection
- Role
- Pre-operative planning or complex cases
- Key findings
- Bone loss quantification, cyst mapping, post-surgical anatomy
- Role
- Injection guidance only
- Key findings
- Joint effusion and synovitis; not diagnostic for osteolysis

Differential Diagnosis: Causes of a Resorbed Distal Clavicle
Osteolysis is only one cause of a lucent, tapered or eroded distal clavicle. The examiner's favourite trap is the patient whose film looks like "weightlifter's shoulder" but whose resorption is systemic - so know the full list and the features that should redirect you.
- Clue that points to it
- Young athlete, repetitive loading or prior AC injury
- Typical pattern
- Usually UNILATERAL, isolated to the loaded shoulder
- Clue that points to it
- Subperiosteal resorption elsewhere (radial border of phalanges), raised calcium and PTH
- Typical pattern
- Often BILATERAL distal clavicle resorption
- Clue that points to it
- Other small-joint erosive disease, morning stiffness, seropositivity
- Typical pattern
- Bilateral, erosive, with marginal erosions
- Clue that points to it
- Skin changes, Raynaud phenomenon, acro-osteolysis of the tufts
- Typical pattern
- Resorption with soft-tissue calcinosis
- Clue that points to it
- Fever, raised inflammatory markers, aggressive destruction
- Typical pattern
- Rapid, ill-defined lysis crossing the joint
- Clue that points to it
- Older patient, night pain, weight loss, known primary
- Typical pattern
- Destructive lytic lesion, possible soft-tissue mass
The practical rule: isolated, unilateral distal clavicle change in a young loader is osteolysis; anything bilateral, systemic, aggressively destructive, or in an older patient with constitutional symptoms needs bloods (calcium, PTH, inflammatory markers, myeloma screen) and often MRI or biopsy before it is dismissed as weightlifter's shoulder.
A young weightlifter with unilateral AC pain and a tapered clavicle has osteolysis. Bilateral distal clavicle resorption should prompt thoughts of hyperparathyroidism (check calcium and PTH, look for phalangeal subperiosteal resorption) or rheumatoid / collagen-vascular disease; an aggressive lytic lesion with night pain or constitutional symptoms must exclude infection or malignancy (metastasis, myeloma) before labelling it weightlifter's shoulder.
Management
Non-operative treatment is successful in the majority of cases and should be pursued for at least 6 months before considering surgery.
1. Activity modification: complete cessation of the offending activity (bench press, overhead press, push-ups, dips). This is the single most important step. Many athletes resist this, but without it other treatments fail.
2. Technique modification on return: when symptoms settle, return with a narrower grip, reduced range of motion (avoiding deep descent to the chest), scapular retraction, and reduced load. Some athletes switch to dumbbells to allow more natural scapular movement.
3. Physiotherapy: scapular stabilisation, rotator cuff strengthening, thoracic mobility, and posture correction. The goal is to reduce abnormal loading across the AC joint.
4. NSAIDs: a short course (2 to 4 weeks) for pain relief and to reduce inflammation.
5. Corticosteroid injection: an intra-articular AC joint injection can provide diagnostic confirmation and therapeutic relief. It is not curative but can break the pain cycle while rehabilitation proceeds.
Resection of more than 10 mm of the distal clavicle risks compromising the coracoclavicular ligament attachments and causing posterior clavicular instability (the clavicle subluxes posteriorly through the deficient AC joint). Aim for 5 to 10 mm and preserve the superior capsule and ligament.
Arthroscopic Distal Clavicle Excision: Direct vs Indirect
When the candidate says "arthroscopic excision," the examiner will ask how. There are two recognised arthroscopic routes, and each has a characteristic pitfall.
- Technique
- Portals placed directly into the AC joint from above (anterosuperior and posterosuperior)
- Strengths and pitfalls
- Excellent view of the whole distal clavicle and easy posterosuperior resection; but the space is small and the working room limited
- Technique
- Enter the subacromial space and resect the clavicle from below through the inferior AC joint
- Strengths and pitfalls
- Allows concurrent subacromial decompression and glenohumeral/cuff inspection; but the POSTEROSUPERIOR corner is easily UNDER-resected, the commonest cause of residual pain
Whichever route is used, the principles are the same: resect roughly 5 to 8 mm, confirm an even gap throughout the arc of motion (especially the posterosuperior corner), and preserve the superior and posterior AC capsule and ligaments to protect against posterior instability. "Co-planing" (shaving the adjacent acromial undersurface to match) is optional and many surgeons avoid it to limit bleeding and reactive bone.
Both arthroscopic routes work, but the indirect (subacromial) approach has a classic pitfall: the posterosuperior corner of the clavicle is left under-resected, the leading cause of persistent post-operative pain. Whichever approach you choose, check the resection through a full arc of motion and preserve the posterior and superior AC capsule to avoid creating posterior clavicular instability.
Complications
Non-operative complications
The main risk of non-operative management is chronic pain and functional limitation if the patient continues to load the AC joint. There is no risk of malignant transformation or systemic disease.
Surgical complications
- Resection inadequacy or excess: too little resection leaves symptomatic bone; too much risks posterior clavicle instability
- Posterior clavicle instability: caused by excessive resection or loss of the superior AC ligament and capsule; presents with painful clicking and prominence
- Infection: low risk (less than 1 percent) but possible with any open or arthroscopic procedure
- Neurovascular injury: the suprascapular nerve and cephalic vein are at risk during open approaches; careful dissection avoids them
- Persistent pain: if the diagnosis was incorrect or there is associated pathology (rotator cuff, cervical spine) that was not addressed
- Deltoid detachment: specific to open approaches where the deltoid is taken off the clavicle; reattachment failure causes weakness
Clinical Relevance
Distal clavicle osteolysis is a favourite of sports-medicine and shoulder vivas because it tests the candidate's ability to link history, mechanism, and imaging in a young athletic patient. The examiner will expect you to:
- Recognise the weightlifter's shoulder presentation and ask about training volume
- Request a Zanca view and describe the characteristic osteopenia, cystic change, and tapering
- Distinguish it from AC joint arthritis (older patient, osteophytes, joint-space narrowing) and rotator cuff disease (painful arc, weakness, positive impingement signs)
- Counsel on activity modification as the first and most important treatment
- Describe distal clavicle excision when non-operative care fails, including the critical detail of not resecting more than 10 mm
It also appears in trauma and upper-limb practice because post-traumatic and iatrogenic forms are increasingly seen after AC joint stabilisation surgery. Knowing how to manage subacromial osteolysis after hook plate fixation (hardware removal, then excision if needed) is a practical skill.
Guidelines, Registries and Global Practice
- Diagnosis: there is no single international guideline for distal clavicle osteolysis, but the diagnosis is established by characteristic history (repetitive loading in a young adult), physical examination (AC joint tenderness, positive cross-body adduction), and imaging (Zanca view showing osteopenia, cystic change, and tapering of the distal clavicle). MRI is widely used as a second-line test to confirm bone marrow oedema and exclude associated pathology.
- Non-operative management: activity modification is the consistent first-line recommendation across sports medicine and shoulder surgery literature worldwide. Cessation of bench press, overhead press, push-ups, and dips for a minimum of 6 to 12 weeks is standard, with gradual return under physiotherapy guidance and technique modification.
- Surgical management: distal clavicle excision (resection arthroplasty) is the accepted operative treatment when non-operative care fails. Both open and arthroscopic techniques are described and yield comparable outcomes. The recommended resection is 5 to 10 mm of the distal clavicle, with preservation of the superior AC ligament and capsule to prevent posterior clavicle instability.
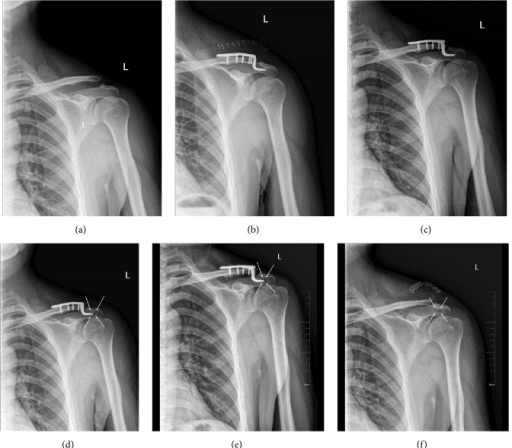
- Iatrogenic osteolysis: subacromial osteolysis after hook plate fixation is a recognised complication. Early plate removal (typically 3 to 6 months after implantation) is recommended to prevent this. Hardware removal is the first step; distal clavicle excision is reserved for persistent symptoms.
- Emerging therapies: platelet-rich plasma and other biologic injections have been reported in case series and small studies, but high-quality evidence is lacking and these are not yet standard of care.
Memory aids
BENCHRisk Factors and Associations
Hook:Think of the BENCH press - the exercise most strongly linked to distal clavicle osteolysis.
OSTEOLRadiographic Features
Hook:OSTEOL - the six radiographic and MRI clues that point to osteolysis rather than arthritis.
MODIFYManagement Steps
Hook:MODIFY everything about the patient's loading before you operate - activity, technique, and shoulder mechanics.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old man presents with 3 months of aching pain over the top of his right shoulder. He trains 5 days per week and has recently increased his bench press from 80 kg to 110 kg. On examination there is tenderness over the AC joint and pain with cross-body adduction. The shoulder AP radiograph is reported as normal.”
“A 35-year-old man had a clavicle hook plate inserted 8 months ago for a Rockwood type III AC joint dislocation. He now complains of persistent pain over the lateral clavicle and AC joint, worse with overhead activity. Radiographs show lucency around the hook tip and erosion of the undersurface of the acromion.”
“You are shown a Zanca view of a 32-year-old weightlifter with AC joint pain. The distal clavicle shows osteopenia, subchondral cystic change, and tapering of the lateral tip. The joint space appears widened. The examiner asks you to interpret the film and differentiate the findings from AC joint osteoarthritis.”
Definition and Mechanism
- Painful osteolysis of the lateral clavicle from repetitive microtrauma
- Classic in weightlifters (bench press, overhead press)
- Also post-traumatic and iatrogenic (hardware-related)
- Stress-induced bone resorption, not infection or tumour
History and Examination
- Young adult, insidious AC joint pain, worse with cross-body adduction
- Recent increase in training volume or intensity
- Tenderness over distal clavicle; cross-body adduction test positive
- O'Brien and Paxinos tests may localise pain to AC joint
Imaging
- Zanca view (15-degree cephalic tilt AP) - shows osteopenia, cysts, tapering
- MRI for equivocal cases or associated pathology - bone marrow oedema in distal clavicle
- CT rarely needed; ultrasound for injection guidance only
Management
- Activity modification first - stop bench press, overhead press, push-ups
- NSAIDs, physiotherapy (scapular stabilisation), AC joint injection
- Surgery: distal clavicle excision (5-10 mm), open or arthroscopic
- Preserve superior AC ligament; do not resect more than 10 mm
Evidence
Frequency, Imaging Findings, Risk Factors, and Long-Term Sequelae of Distal Clavicular Osteolysis in Young Patients
- Retrospective review of 1,432 consecutive shoulder MRIs in 13-19 year-olds: atraumatic DCO present in 6.5% (93 patients), of whom 24% were female
- The combination of an overhead sport (basketball, volleyball, tennis, swimming) plus supplemental weight training was the key risk factor (odds ratio 38, p=0.01)
- 93% responded to conservative therapy; MRI showed distal clavicle marrow oedema, and oedema severity correlated with pain
- Long-term sequelae at 2 years: 71% developed AC joint osteoarthritis (vs 35% controls) with flattening of the distal clavicle and AC joint widening to a mean of 5.0 mm (vs 2.4 mm controls)
A Sports Medicine Clinician's Guide to the Diagnosis and Management of Distal Clavicular Osteolysis
- Comprehensive clinical review of distal clavicle osteolysis for sports medicine practice
- Emphasises activity modification as the cornerstone of treatment, with cessation of bench press and overhead loading
- Describes the Zanca view as the key radiographic investigation and MRI for equivocal cases
- Recommends distal clavicle excision (open or arthroscopic) for refractory cases after 6 to 12 months of non-operative care
Distal Clavicular Osteolysis Treated With Platelet-Rich Plasma: A Case Report
- Case report of refractory atraumatic distal clavicle osteolysis after failure of activity modification, analgesia and physiotherapy
- Treated with a single ultrasound-guided platelet-rich plasma injection of the acromioclavicular joint, with symptomatic improvement
- First published account of PRP used specifically for distal clavicle osteolysis (no prior efficacy studies existed)
Involvement of the Acromion in Cases of Distal Clavicular Osteolysis
- Retrospective MRI review of 128 cases of DCO in 127 patients (93 male, mean age 39.5 years, mean symptom duration ~13 months)
- Describes a variant in which osteolysis crosses the AC joint to involve the anterior acromion as well as the distal clavicle - present in 42 cases (32.8%)
- Acromial involvement was commoner in males (p=0.049); maximum bench-press weight was the only other significant associated factor (p=0.027), implicating load
- 62.5% reported weightlifting and 45.3% an antecedent trauma history