A Sideline Life-Threatening Emergency
- EXERTIONAL HEAT ILLNESS is a spectrum - HEAT CRAMPS, HEAT EXHAUSTION, and EXERTIONAL HEAT STROKE - and EXERTIONAL HEAT STROKE (EHS) is the LIFE-THREATENING emergency: strenuous physical activity producing severe HYPERTHERMIA (core temperature over about 40 C / 104 F) together with central nervous system DYSFUNCTION (confusion, agitation, collapse, seizures, loss of consciousness).
- Unlike classic heat stroke, EHS can occur in YOUNG, HEALTHY individuals and even in TEMPERATE climates, when heat production exceeds the body's ability to dissipate heat; rising global temperatures and increased participation in endurance events are increasing its incidence.
- The DISTINCTION from heat exhaustion is the central one: HEAT EXHAUSTION has relatively preserved mental status (and core temperature usually below the heat-stroke threshold), whereas EHS has CNS dysfunction with severe hyperthermia - a collapsed/confused athlete who is HOT must be treated as heat stroke until proven otherwise.
- EARLY RECOGNITION and RAPID COOLING are essential to prevent MULTI-ORGAN FAILURE and DEATH; the recognised complications of EHS include ACUTE KIDNEY INJURY, COAGULOPATHY (DIC), LIVER dysfunction, rhabdomyolysis and neurological impairment.
- The GOLD-STANDARD treatment is WHOLE-BODY COLD-WATER IMMERSION, and the guiding principle is 'COOL FIRST, TRANSPORT SECOND' - aggressive on-site cooling to lower the core temperature rapidly takes priority over transport, because the duration of severe hyperthermia drives outcome; cooling should continue until a safe core temperature is reached.
- IN-HOSPITAL care focuses on continued cooling (if needed) and managing the complications (AKI, coagulopathy, liver dysfunction, rhabdomyolysis, neurological injury), with the orthopaedic/sideline relevance being recognition and immediate cooling at the event - PREVENTION (acclimatisation, hydration, work-rest cycles, heat-policy/wet-bulb-globe-temperature monitoring) reduces incidence.
- “Exertional heat stroke (EHS) = LIFE-THREATENING: severe hyperthermia (core >~40 C) + CNS dysfunction (confusion/collapse/seizure) during exertion. Distinguish from heat exhaustion (preserved mental status, lower core temp).
- “Occurs in YOUNG HEALTHY athletes even in TEMPERATE climates (heat production > dissipation). Untreated -> multi-organ failure (AKI, coagulopathy, liver, rhabdo) and death.
- “GOLD-STANDARD treatment = whole-body COLD-WATER IMMERSION; principle = 'COOL FIRST, TRANSPORT SECOND' (rapid on-site cooling before transport). Prevent with acclimatisation/hydration/work-rest/WBGT monitoring.
Severe hyperthermia (core >~40 C) + CNS dysfunction (confusion, collapse, seizure) during exertion = exertional heat stroke. Can occur in young healthy athletes even in temperate climates.
Cool first, transport second - whole-body cold-water immersion is the gold standard. Rapid cooling prevents multi-organ failure and death; continue until a safe core temperature.
Risk Factors: Who Collapses, and Why the First Week Matters
Exertional heat stroke is not a random misfortune, and an examiner asking "how would you have prevented this?" is asking for these. The dominant modifiable factor is acclimatisation state: the great majority of cases cluster in the first days of a preseason, training camp or military intake, before physiological adaptation has occurred. Acclimatisation takes roughly ten to fourteen days of progressive exposure, over which plasma volume expands, sweating begins earlier and at a higher rate, and sweat sodium falls - which is why an athlete returning from a break, or arriving from a cooler climate, is at risk even though they are fit.
The remaining factors group usefully:
- Environmental - high ambient temperature and humidity, since it is evaporation that does the cooling; this is why the wet-bulb globe temperature (WBGT), which combines temperature, humidity, radiant heat and wind, governs heat policies rather than the air temperature alone. Still air and full sun add further load.
- Equipment and clothing - occlusive kit is a major and often overlooked contributor. American football pads and helmet, body armour and full protective clothing prevent evaporation over much of the body surface, and helmet removal is part of the initial management.
- Individual - poor aerobic fitness, high body mass and adiposity, a recent febrile or gastrointestinal illness, sleep deprivation, dehydration at the start, and certain medications and supplements (stimulants, anticholinergics, some diuretics).
- A previous episode of exertional heat stroke, which confers an increased risk of a further one and is the reason recurrent cases warrant a search for an underlying myopathy or an inherent heat intolerance.
- Sickle cell trait, which is a risk factor for exertional collapse and rhabdomyolysis rather than for hyperthermia specifically, but shares the same high-intensity, unacclimatised setting.
- Motivation and supervision - the culture that rewards pushing through, and the absence of a mandated work-to-rest ratio, are why events and military selection produce clusters.
The Collapsed Athlete: Differential and the Hyponatraemia Trap
"Treat as heat stroke until proven otherwise" still requires a deliberate differential, because the dangerous mimic - exercise-associated hyponatraemia - needs the OPPOSITE fluid management.
- Core (rectal) temperature
- High (over ~40 C)
- Discriminating features
- CNS dysfunction WITH severe hyperthermia
- Immediate action
- Immediate cold-water immersion; cool first, transport second
- Core (rectal) temperature
- Normal or low
- Discriminating features
- Confusion/seizure with a NORMAL temperature; over-drinking (weight gain during the event); low serum sodium
- Immediate action
- Do NOT give hypotonic or large-volume fluids; hypertonic (3 per cent) saline if symptomatic; check serum sodium
- Core (rectal) temperature
- Normal
- Discriminating features
- No pulse, unresponsive
- Immediate action
- CPR and AED immediately (see the sudden-cardiac-death-athletes-screening topic)
- Core (rectal) temperature
- Often only mildly raised
- Discriminating features
- Muscle pain/weakness, rhabdomyolysis, collapse early in intense exertion
- Immediate action
- Supportive care; treat rhabdomyolysis (see the sickle-cell-disease-orthopaedic and rhabdomyolysis topics)
- Core (rectal) temperature
- Normal
- Discriminating features
- Hypoglycaemia: confusion that responds to glucose. Benign exertional collapse: conscious, normal mentation, resolves with legs raised
- Immediate action
- Check glucose; for benign collapse, lie supine with legs elevated
A collapsed, confused athlete is NOT always heat stroke. The two altered-mental-status emergencies are exertional heat stroke (core temperature high) and exercise-associated hyponatraemia (core temperature normal or low, from over-drinking). The discriminators are the rectal core temperature and the serum sodium - and the managements are opposite: EHS needs aggressive cooling, whereas EAH must NOT be given hypotonic or large-volume fluids (which worsen cerebral oedema) and is treated with hypertonic saline. This is why a rectal temperature, not a tympanic or oral reading, is taken in every collapsed athlete. Rhabdomyolysis, exertional sickling and sudden cardiac arrest complete the differential - see Rhabdomyolysis, Sickle Cell Disease in Orthopaedics and Sudden Cardiac Death in Athletes.
Enough about hyponatraemia to act on it
Because the two conditions are managed in opposite directions, a few specifics are worth carrying rather than looking up. Exercise-associated hyponatraemia arises from drinking more fluid than is lost, typically in slower participants in long events who take on water at every station; the giveaway on history is that the athlete has gained weight during the event rather than lost it. Symptoms track the sodium: nausea, headache and bloating at mild levels, progressing to confusion, seizures and respiratory arrest from cerebral and pulmonary oedema as it falls further.
The management rule is the one to remember. Do not give hypotonic fluid, and do not give volume for "dehydration" in a collapsed athlete until the sodium is known - in EAH that is precisely what precipitates the fatal cerebral oedema, and the reflex to run in a litre of saline is the error that kills. Symptomatic hyponatraemia is treated with a small bolus of hypertonic (3%) saline, repeated as needed to reverse the neurological signs, which is deliberately a small volume of very salty fluid rather than a large volume of slightly salty fluid. An athlete who is merely uncomfortable with a suspected mild case is managed by fluid restriction and observation, not by drinking more.
The Spectrum, Recognition & Treatment
Exertional heat illness spans heat cramps, heat exhaustion (preserved mental status, core usually below the heat-stroke threshold) and exertional heat stroke (EHS) - the life-threatening emergency of severe hyperthermia (core over ~40 C) with CNS dysfunction (confusion, collapse, seizure). EHS occurs in young, healthy athletes and even in temperate climates when heat production exceeds dissipation. Early recognition and rapid cooling prevent multi-organ failure (AKI, coagulopathy, liver dysfunction, rhabdomyolysis, neurological injury) and death. The gold-standard treatment is whole-body cold-water immersion, guided by 'cool first, transport second' - aggressive on-site cooling before transport, continued until a safe core temperature. Prevention (acclimatisation, hydration, work-rest cycles, wet-bulb-globe- temperature monitoring) reduces incidence.
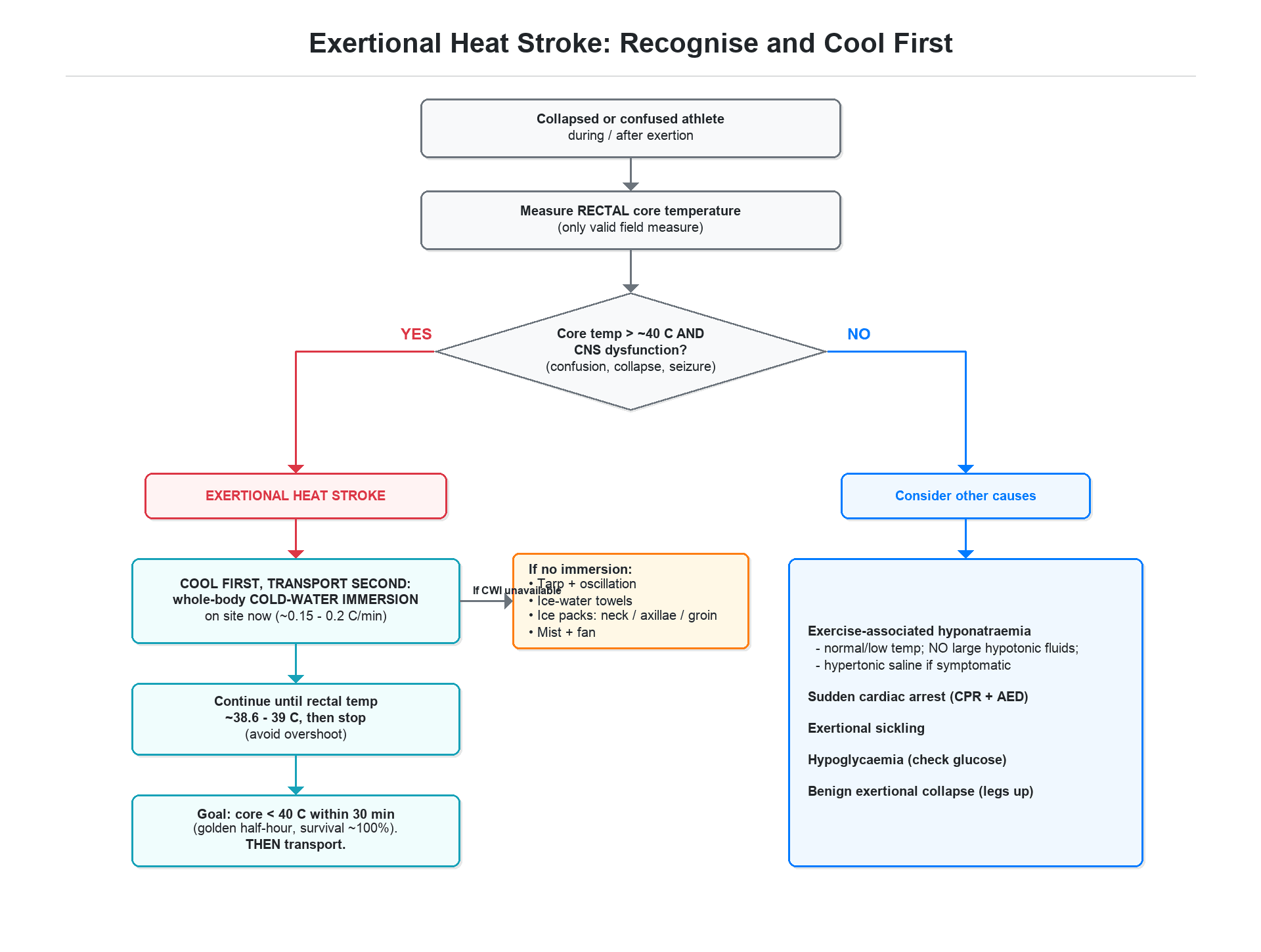
The single most important principle in exertional heat stroke is that outcome is driven by how long the core temperature remains dangerously high, so the priority is immediate, aggressive cooling - 'cool first, transport second' - rather than rushing the athlete to hospital while still hot. Whole-body cold-water immersion is the gold-standard cooling method and should be started on site without delay and continued until a safe core temperature is reached. The diagnosis hinges on recognising central nervous system dysfunction - confusion, agitation, collapse or seizures - together with severe hyperthermia in an athlete during exertion; this distinguishes heat stroke from heat exhaustion, which has relatively preserved mental status, and a collapsed or confused, hot athlete must be treated as heat stroke until proven otherwise. Crucially, exertional heat stroke can strike young, healthy individuals even in temperate climates, so it must not be dismissed because conditions seem unremarkable. Untreated or slowly cooled, it progresses to multi-organ failure - acute kidney injury, coagulopathy, liver dysfunction, rhabdomyolysis and neurological injury - and death; in-hospital care continues cooling and manages these complications, while prevention through acclimatisation, hydration, work-rest cycles and heat-policy (wet-bulb-globe-temperature) monitoring reduces the risk.
Cooling Method, Endpoint and Core-Temperature Measurement
"Cool first, transport second" is only safe if cooling is done correctly, measured correctly and stopped correctly.
- Cold-water immersion (CWI) cools at roughly 0.15-0.2 C per minute - far faster than any other field method.
- Survival approaches 100 per cent when the core temperature is brought below about 40 C within ~30 minutes of collapse (the "golden half-hour"), which is exactly why on-site cooling beats early transport.
- If immersion is impossible, use the next-best methods: tarp-assisted cooling with oscillation (the athlete in a water-filled tarp, rocked to circulate the water), continuously rotated ice-water-soaked towels to head/trunk/limbs, ice packs to neck, axillae and groin, and evaporative cooling (mist plus fanning) - all inferior to CWI.
- Rectal temperature is the only valid field measure of core temperature. Oral, axillary, tympanic, aural and temporal readings are inaccurate, underestimate the true core temperature, and must NOT be used to exclude heat stroke.
- Stop cooling at a core temperature of about 38.6-39 C (~101-102 F) to avoid overshoot into hypothermia.
- Secure airway, breathing and circulation alongside cooling; cooling is not delayed for venous access or transport.
What does not work, and what makes it worse
Two drug reflexes have to be actively suppressed, and both are popular wrong answers.
Antipyretics do nothing in heat stroke. Paracetamol, aspirin and NSAIDs work by lowering a hypothalamic set point that has been raised by pyrogens. In exertional heat stroke the set point is normal - the problem is that heat production has overwhelmed dissipation - so there is no set point to lower and no antipyretic effect to be had. Worse, they are actively unhelpful in this specific patient: paracetamol is hepatotoxic in an athlete whose liver is about to be injured, and NSAIDs are nephrotoxic and antiplatelet in one who is heading for acute kidney injury and coagulopathy. Dantrolene likewise has no established role, because this is not malignant hyperthermia - the pathophysiology is environmental and exertional heat load, not a ryanodine-receptor defect (contrast with Malignant Hyperthermia).
The other error is fluid by reflex. Cooling, not volume, is the resuscitation here, and until the sodium is known a large-volume hypotonic infusion risks converting a survivable collapse into fatal cerebral oedema if the diagnosis is actually exercise-associated hyponatraemia.
Give no antipyretic in exertional heat stroke - the hypothalamic set point is normal, so paracetamol and NSAIDs cannot lower the temperature, and both add hepatic, renal and platelet injury to an organ system already failing. Dantrolene is not indicated; this is not malignant hyperthermia. Nothing in the drug cupboard cools an athlete: cold-water immersion does, and every minute spent looking for a pharmacological alternative is spent above 40 degrees.
After the Field: Complications, Prevention and Return to Play
The complications do not all appear at once
Successful cooling on the field is the decisive intervention, but it is not the end of the illness, and the timing matters because the athlete who looks well at two hours can deteriorate later.
- Immediately - seizures, arrhythmia, aspiration and the consequences of a fall or collapse.
- Over the first 24 hours - rhabdomyolysis with hyperkalaemia and myoglobinuric acute kidney injury, best anticipated with creatine kinase, potassium, renal function and urine output rather than waited for.
- At 24 to 72 hours - hepatic injury, which characteristically peaks late; a small number progress to fulminant liver failure requiring transplantation. This is the complication most likely to be missed by an early discharge, and it is the reason a genuine exertional heat stroke is admitted and re-checked rather than sent home once cool and lucid.
- Also - disseminated intravascular coagulation, acute respiratory distress syndrome, and persisting neurological deficit, most often cerebellar, in those cooled slowly.
Prevention that is specific enough to implement
"Acclimatise, hydrate and monitor WBGT" is only useful if it names what to do. A workable heat plan means graduated acclimatisation over ten to fourteen days, with equipment introduced progressively rather than from day one; activity modified against WBGT thresholds with defined work-to-rest ratios and mandated fluid breaks; and, decisively, an immersion tub filled and on site before the session starts, because a policy that requires someone to fetch ice after the collapse has already lost the golden half-hour. The written emergency action plan should name who takes the rectal temperature, who starts immersion and who calls the ambulance, and it should be rehearsed. Sessions should also be structured so that an athlete can stop without penalty - the cultural point does more work than any of the physiological ones.
Return to play
Return is graded and unhurried, and the principle is that the athlete does not restart until the organ injury has resolved and heat tolerance has been demonstrated.
- Rest from exercise until symptom-free with normalised laboratory markers - creatine kinase, renal and liver function - which commonly takes at least a week and sometimes considerably longer.
- Graded reintroduction over subsequent weeks: light activity in a cool environment first, then increasing intensity, then increasing heat exposure, then full equipment - changing one variable at a time so that a failure identifies itself.
- Heat tolerance testing at around six weeks or more is used where recovery is slow, where the episode was severe, or before returning to a high-risk occupational setting; military services in particular use a standardised exercise-in-heat protocol to document tolerance before full clearance.
- A recurrent episode should prompt a search for a predisposing cause - an underlying myopathy, a malignant-hyperthermia-related susceptibility, or a persisting intolerance - and a frank reconsideration of the athlete's participation in the setting that caused it.
Mnemonics & Memory Aids
COOL
Hook:COOL: CNS dysfunction + Core >~40 C, Occurs in young/temperate, On-site immersion (cool first), Life-threatening (organ failure).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A young athlete collapses, confused and very hot, during a race. What is the diagnosis and what is your immediate priority?”
Spectrum
- Heat cramps; heat exhaustion (preserved mental status, core usually below threshold)
- Exertional heat stroke (EHS): severe hyperthermia (core >~40 C) + CNS dysfunction
- Can occur in young, healthy athletes even in temperate climates
Recognition
- Collapsed/confused/agitated, hot athlete during exertion
- CNS dysfunction + severe hyperthermia = heat stroke (not exhaustion)
- Measure core (rectal) temperature; treat as heat stroke until proven otherwise
Treatment
- Immediate aggressive cooling: 'cool first, transport second'
- Whole-body cold-water immersion = gold standard; continue until safe core temperature
- Hospital: continued cooling + manage complications (AKI, coagulopathy, liver, rhabdo, CNS)
Prevention
- Acclimatisation; hydration
- Work-rest cycles
- Wet-bulb-globe-temperature monitoring / heat policies
Evidence & Key Studies
Exertional heat stroke - recognition and management
- Exertional heat stroke is a life-threatening condition caused by strenuous physical activity leading to severe hyperthermia and central nervous system dysfunction; unlike classic heat stroke it can occur in young, healthy individuals and in temperate climates.
- Early recognition and rapid cooling are essential to prevent multi-organ failure and death; whole-body cold-water immersion is the gold-standard treatment, and 'cool first, transport second' is key to improving survival.
- In-hospital care focuses on continued cooling when necessary and managing complications such as acute kidney injury, coagulopathy, liver dysfunction and neurological impairment.
The definition of exertional heat stroke (life-threatening severe hyperthermia with CNS dysfunction occurring even in young healthy individuals in temperate climates), the central role of early recognition and rapid cooling, whole-body cold-water immersion as the gold-standard treatment, the 'cool first, transport second' principle, and the complications (acute kidney injury, coagulopathy, liver dysfunction, neurological impairment) come from the cited Stomeo review. The wider heat-illness spectrum (cramps/exhaustion), the distinction from heat exhaustion (preserved mental status), and prevention (acclimatisation, hydration, work-rest, wet-bulb-globe-temperature monitoring), the risk-factor profile, the ineffectiveness of antipyretics, the late hepatic peak and the graded return-to-play principles are standard, well-established teaching. (See also Rhabdomyolysis, Malignant Hyperthermia and Sudden Cardiac Death in Athletes.)