Failed Fusion Accessory Ossicle | Usually Incidental | Fracture Mimic
- Definition: A patella formed from more than one ossification centre that never fused, leaving an accessory bony fragment joined by a fibrocartilaginous synchondrosis.
- Frequency: Present in roughly 1-2% of people. The vast majority are asymptomatic and found incidentally.
- Most common type: Saupe type III - the superolateral fragment - accounts for about 75% and is where almost all symptomatic cases arise.
- The trap: It mimics a fracture. Smooth, rounded, corticated margins and a typical superolateral site point to bipartite, not a fresh break.
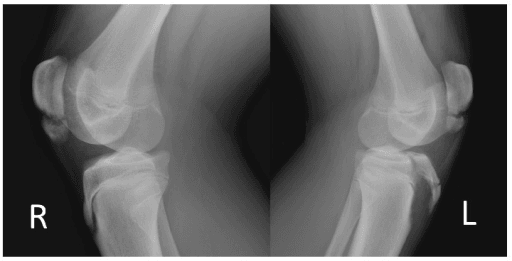
- Bilateral clue: Often bilateral - get a film of the other knee. A symmetrical superolateral ossicle strongly favours bipartite over acute fracture.
- Treatment: Almost always conservative. Surgery (fragment excision is the best-supported option) only for pain refractory to prolonged non-operative care.
- “The vastus lateralis inserts onto the superolateral fragment - its repeated traction is the proposed reason this type becomes painful and why lateral release can help.
- “Corticated, smooth, rounded edges = bipartite. Sharp, irregular, non-corticated edges with a matching donor site = fracture.
- “A skyline (tangential) view best profiles the superolateral fragment; the contralateral knee film is your free comparison.
- “MRI bone-marrow oedema across the synchondrosis indicates a SYMPTOMATIC (painful) bipartite, not just an incidental one.
Smooth and corticated = not acute. A rounded, well-corticated superolateral ossicle is bipartite. Don't take a patient to theatre or splint a fracture that isn't there.
Bipartite is often bilateral. A film of the opposite knee showing a mirror-image ossicle is strong evidence against an acute fracture.
Conservative care first. Most symptomatic cases settle with activity modification and rehab over weeks to a few months. Surgery is for genuine refractory pain.
Different entity. A dorsal defect of the patella is a focal lucency in the bone, not a separate ossicle with a synchondrosis. Don't merge the two.
Overview and Epidemiology
The patella normally develops from a main ossification centre that appears around age 3-6 years, often with one or more accessory (secondary) centres that should fuse by adolescence. A bipartite patella is the failure of one of these accessory centres to fuse, leaving a separate accessory bone fragment connected to the main patella by a fibrocartilaginous synchondrosis rather than solid bone. When more than one accessory centre persists it is termed a multipartite (tri-, quadripartite) patella.
- Prevalence: roughly 1-2% of the population. According to PubMed, an open-excision outcome series quotes a figure of about 2% (Pan and Hennrikus, Cureus 2022).
- Sex: more common in males.
- Laterality: frequently bilateral (a key diagnostic clue).
- Symptomatic minority: most are silent, incidental findings; only a small fraction ever become painful, typically in active adolescents and young adults after sport, overuse or direct trauma.
It is one of the classic "fracture mimics" of the knee. The examiner wants to know that you (1) recognise it, (2) do not over-treat it, and (3) know the evidence-based pathway for the rare painful fragment.
Pathophysiology and Anatomy
- Patella: the largest sesamoid bone, embedded within the quadriceps-patellar tendon (extensor) mechanism.
- Superolateral corner: the insertion zone of the vastus lateralis. The common type III fragment lies exactly here.
- Synchondrosis: the fibrocartilaginous bridge between fragment and main patella. It is the source of pain when the variant becomes symptomatic.
- The vastus lateralis (and the lateral retinaculum) attach onto or near the superolateral fragment.
- Repetitive or forceful quadriceps activity transmits traction (tensile) and shear forces across the synchondrosis.
- Overuse or a direct blow disrupts the synchondrosis, producing a painful pseudarthrosis / non-union with local inflammation and bone-marrow oedema.
- This explains both the clinical picture (activity-related superolateral pain) and the rationale for the two main surgical options: excise the fragment, or release the lateral traction (lateral release / vastus lateralis detachment).
According to PubMed, an MRI study found that trochlear dysplasia and patellofemoral maltracking are more frequent in symptomatic than asymptomatic bipartite patellae, suggesting abnormal patellar tracking loads the synchondrosis and contributes to symptoms (Atay, Cureus 2023).
Why Some Bipartites Hurt: The Trochlear Dysplasia Link
The pathophysiology and controversies sections both flag that maltracking is "associated" with the painful bipartite and raise — without answering — whether tracking should be addressed. It is worth developing, because it reframes the symptomatic bipartite as partly a patellofemoral-overload problem, not purely a local fragment.
What the data actually show. According to PubMed (Atay 2023, 46 MRI-confirmed bipartite patellae, 17 symptomatic), the symptomatic group had significantly more frequent and more severe trochlear dysplasia — a higher trochlear sulcus angle (p=0.007) and a shallower trochlear depth (p=0.006) — and a more dysplastic patella morphology (Wiberg type III/IV), than the asymptomatic group. Crucially, there was no significant difference in the tibial-tubercle-to-trochlear-groove (TT-TG) distance (p=0.247) (DOI). So the association is with the trochlear and patellar shape, not with tibial-tubercle lateralisation.
- Symptomatic bipartite
- More frequent and more severe
- Implication
- A shallow trochlea is the key associated abnormality
- Symptomatic bipartite
- More often dysplastic (type III/IV)
- Implication
- Disproportionate facet loads the superolateral corner
- Symptomatic bipartite
- No significant difference
- Implication
- Tubercle lateralisation is NOT the driver - so tubercle realignment is not the answer
The mechanism and the unresolved question. A shallow, dysplastic trochlea permits abnormal patellar tilt and tracking that concentrates load on the superolateral synchondrosis, tipping a previously-silent bipartite into a painful one. This explains why the painful bipartite clusters at the vastus-lateralis corner and why some are stubborn. It does not, however, translate into a realignment operation: because the abnormal parameter is the trochlea/patella shape rather than the TT-TG, tubercle-medialisation realignment is not indicated, and trochleoplasty is not standard for this benign condition. Current practice still treats the fragment (conservative, then excision or release), but recognising the dysplastic substrate justifies assessing and rehabilitating patellar tracking as part of conservative care. (The full patellofemoral-instability work-up — Dejour dysplasia grading, MPFL, TT-TG and trochleoplasty — belongs to the patellofemoral-instability topic.)
Q: A symptomatic bipartite patella is associated with which patellofemoral abnormality? A: Trochlear dysplasia (shallow trochlea, high sulcus angle) and a dysplastic patella (Wiberg III/IV) — not an increased TT-TG distance. The shallow trochlea allows tilt/tracking that overloads the superolateral synchondrosis. It argues for assessing tracking and rehabilitation, not for a tubercle-realignment operation.
Classification
The universal scheme is the Saupe classification, which groups bipartite patellae purely by the location of the accessory fragment:
- Location of Fragment
- Inferior pole
- Approximate Frequency
- ~5% (rarest)
- Exam Note
- Differentiate from sleeve / inferior-pole avulsion fracture
- Location of Fragment
- Entire lateral margin
- Approximate Frequency
- ~20%
- Exam Note
- Vertical lucency can mimic a longitudinal fracture
- Location of Fragment
- Superolateral corner
- Approximate Frequency
- ~75% (most common)
- Exam Note
- Where almost all symptomatic cases occur
By Saupe Type
- Type I (inferior pole): least common. The main pitfall is confusing it with an inferior-pole sleeve or avulsion fracture in a child or adolescent.
- Type II (lateral margin): a fragment running down the whole lateral edge; the linear lucency can look like a vertical fracture.
- Type III (superolateral): by far the most common and the type that becomes symptomatic, owing to vastus lateralis traction.
Clinical Assessment
- Incidental finding: most are discovered on a knee film taken for another reason and the patient has no complaint.
- When painful: an active adolescent or young adult with anterior or superolateral knee pain, brought on by sport, jumping, squatting or kneeling, and relieved by rest. Onset may follow a period of overuse or a direct blow to the front of the knee.
- Focal tenderness directly over the superolateral pole of the patella is the single most useful sign in symptomatic cases.
- Local swelling may be palpable over the fragment.
- Pain on resisted knee extension or with quadriceps loading (vastus lateralis traction).
- Full active extension is preserved - unlike an extensor-mechanism rupture or a displaced patellar fracture. Loss of active extension should make you doubt the diagnosis.
- Assess patellar tracking and instability, as maltracking/trochlear dysplasia is associated with symptomatic cases.
Investigations
Imaging:
- Plain radiographs (AP, lateral, skyline/tangential): the diagnosis is usually radiographic.
- Site: superolateral corner (type III) most often.
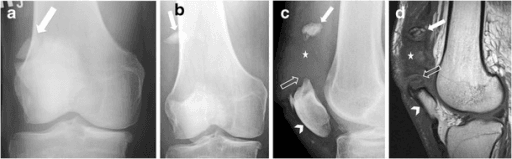
- Margins: smooth, rounded, corticated edges - the hallmark distinguishing it from a fracture.
- Skyline view: best profiles the superolateral fragment.
- Other knee: image it too - a bilateral, mirror-image ossicle strongly supports bipartite.
- CT: confirms the separate corticated fragment and synchondrosis; useful when the radiograph is equivocal or to plan surgery.
- MRI: the key test for deciding if a bipartite is the actual pain generator. Bone-marrow oedema straddling the synchondrosis (in the fragment and adjacent patella) indicates a symptomatic, painful synchondrosis; its absence suggests the bipartite is an innocent bystander. MRI also assesses trochlear dysplasia and tracking.
- Bone scan / SPECT: increased uptake at the synchondrosis can localise the pain source when MRI is unavailable, though it is less specific.
The most exam-relevant single point: corticated, smooth, superolateral, often bilateral = bipartite; sharp, irregular, non-corticated, with a matching donor defect and a clear injury = fracture. When unsure whether it is the source of symptoms, MRI marrow oedema across the synchondrosis is the tie-breaker.
Differential Diagnosis
- Bipartite Patella
- Smooth, rounded, corticated
- Acute Fracture
- Sharp, irregular, non-corticated
- Bipartite Patella
- Superolateral corner (type III)
- Acute Fracture
- Anywhere - often transverse mid-body
- Bipartite Patella
- Often bilateral / symmetrical
- Acute Fracture
- Unilateral, matches the injured knee
- Bipartite Patella
- No matching defect on main patella
- Acute Fracture
- Fragment edges match the donor site
- Bipartite Patella
- Often no single significant injury
- Acute Fracture
- Clear, usually higher-energy injury
- Bipartite Patella
- Preserved
- Acute Fracture
- May be lost if extensor mechanism disrupted
Other entities to consider:
- Dorsal defect of the patella - a focal lucency/cyst within the bone, not a separate ossicle with a synchondrosis.
- Inferior-pole sleeve / avulsion fracture - the main confounder for the rare type I; here active extension may be lost and the history is acute.
- Patellar stress fracture - particularly in athletes; marrow oedema may overlap, but a fresh fracture line and donor site differ.
- Osgood-Schlatter / Sinding-Larsen-Johansson - apophyseal pain at the tibial tubercle or inferior pole in adolescents; can coexist.
Dorsal Defect of the Patella: The Other Superolateral Lesion
The exam-warning and the differential both tell you not to confuse a bipartite patella with a dorsal defect of the patella, and a viva follow-up asks you to distinguish them — but the entity is never explained. It sits at the same superolateral corner, which is exactly why they are confused.
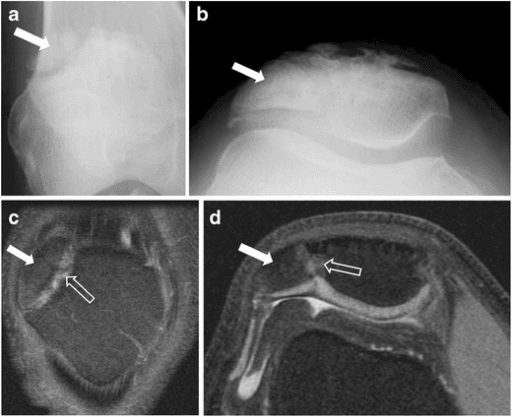
- What it is: a dorsal defect of the patella (DDP) is a well-defined, rounded, lucent defect in the subchondral bone of the superolateral patella, typically around 1 to 2 cm, filled with fibrous tissue. It is usually found incidentally in adolescents and young adults, is frequently bilateral, is almost always asymptomatic, and characteristically resolves spontaneously as the skeleton matures.
- The key difference from bipartite: a dorsal defect is a focal lucency within an intact, continuous patella — there is no separate ossicle and no synchondrosis. A bipartite is a discrete corticated fragment joined to the main bone by a fibrocartilaginous synchondrosis. On MRI the articular cartilage overlying a dorsal defect is intact, which both confirms the diagnosis and separates it from osteochondritis dissecans.
- The developmental link (why the topic says "do not merge them"): DDP and the superolateral (type III) bipartite are thought to share a developmental origin at the superolateral corner — the same region loaded by the vastus lateralis — and the two can coexist. They are nonetheless distinct lesions.
- Dorsal defect of patella
- Lucent defect WITHIN an intact patella
- Bipartite patella
- Separate ossicle + fibrocartilaginous synchondrosis
- Dorsal defect of patella
- Superolateral subchondral bone
- Bipartite patella
- Superolateral corner (type III)
- Dorsal defect of patella
- Intact
- Bipartite patella
- Continuous over the synchondrosis
- Dorsal defect of patella
- Usually resolves with skeletal maturity
- Bipartite patella
- Persists; usually remains asymptomatic
- Dorsal defect of patella
- Mistaken for OCD, infection or tumour
- Bipartite patella
- Mistaken for an acute fracture
Why it matters: a dorsal defect is benign and self-limiting and needs no treatment — the danger is mistaking its lucency for osteochondritis dissecans, an infection or a tumour and over-investigating or biopsying it. Recognising the intact overlying cartilage on MRI and the typical superolateral, often-bilateral pattern settles it.
Q: How does a dorsal defect of the patella differ from a bipartite patella? A: A dorsal defect is a benign lucent defect within an intact patella (no separate fragment, intact overlying cartilage, usually resolves with maturity); a bipartite is a separate corticated ossicle joined by a synchondrosis. Both favour the superolateral corner. The dorsal defect's trap is mimicking OCD/tumour; the bipartite's trap is mimicking a fracture.
Management
The guiding principle is simple: incidental bipartite needs no treatment; the rare painful bipartite is treated conservatively first, and surgically only if pain is refractory.
First-Line: Non-operative (most patients)
Indication: symptomatic bipartite with confirmed painful synchondrosis (or strong clinical picture) and no other cause.
- Activity / load modification: reduce the offending loading (jumping, kneeling, deep squatting).
- Relative rest with a short period of immobilisation in some protocols, followed by graded return.
- Physiotherapy: quadriceps and core conditioning, correction of patellar maltracking, hip-knee kinematics.
- Analgesia / NSAIDs for pain control.
- Time: most settle over weeks to a few months.
According to PubMed, a pooled paediatric/adolescent review found that about three-quarters of symptomatic knees resolved with conservative management at a median of around two months, with surgery reserved for the refractory minority (Hines et al, J Child Orthop 2024).
Complications
The commonest "complication" is diagnostic - over-treating an incidental variant as an acute fracture, or vice versa missing a real fracture by dismissing it as bipartite.
Symptoms can persist or recur after surgery, sometimes from residual ossicles, an inadequate release, or an unaddressed maltracking problem.
Excising a large fragment that carries a meaningful portion of articular surface can leave an incongruent patellofemoral joint - favour a patella-preserving technique for big fragments.
Aggressive vastus lateralis detachment or extensive surgery can weaken the extensor mechanism; preserving quadriceps function is a stated goal of treatment.
Clinical Relevance and Controversies
- Best operation is unsettled. Multiple systematic reviews agree that excision, lateral release, ORIF and arthroscopic variants all give good results, but the literature is entirely low-level (case series), so no technique is proven superior (McMahon et al 2016; Hines et al 2024).
- How long is "enough" conservative care? Thresholds for moving to surgery (often 3-6 months) are pragmatic rather than evidence-defined; earlier surgery within a relatively short window of refractory symptoms has been linked to better outcomes in younger patients in some reviews.
- Who actually gets symptomatic? The association with trochlear dysplasia and maltracking (Atay 2023) raises the question of whether tracking should be addressed alongside the fragment - currently not standard.
- Confirming the pain source. Because a bipartite can be an innocent bystander, MRI marrow oedema (or local uptake on bone scan) before committing to surgery is increasingly emphasised.
Guidelines, Registries & Global Practice
There are no dedicated national society guidelines for bipartite patella; practice is driven by systematic reviews and consensus. The picture below is consistent across regions.
- Consensus Position
- No treatment; reassure
- Evidence Base
- Universally accepted (review, Atesok 2008)
- Consensus Position
- Conservative care; majority resolve
- Evidence Base
- ~75% resolution (Hines 2024, paediatric/adolescent)
- Consensus Position
- No proven superior technique; excision best for return to sport
- Evidence Base
- Systematic reviews (McMahon 2016, Matic 2015)
- Consensus Position
- Prefer patella-preserving (lateral release) over excision
- Evidence Base
- Review consensus (Atesok 2008)
- Consensus Position
- Arthroscopic excision / release safe and effective
- Evidence Base
- Systematic review (Loewen 2021)
Global epidemiology: prevalence is broadly quoted around 1-2% of the population worldwide, more common in males and frequently bilateral. There is no implant or arthroplasty registry relevance for this condition, as management is non-implant (conservative, fragment excision, or soft-tissue release).
Memory Aids
ILSSaupe Classification by Location
Hook:I-L-S = Inferior, Lateral, Superolateral, in increasing frequency (1, 2, 3).
SMOOTHBipartite vs Fracture on X-ray
Hook:If it is SMOOTH, think bipartite, not break.
PAINWhen the Bipartite Is Genuinely Painful
Hook:True symptomatic bipartite ticks all of PAIN; an incidental one ticks none.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is this and how will you manage it?”
“How do you manage a symptomatic bipartite patella?”
“Give me your reasoning, and what you would do next.”
MCQ Practice Points
Q: Which Saupe type of bipartite patella is most common and most likely to be symptomatic?
A: Type III (superolateral corner) - roughly 75% of cases and nearly all painful ones, due to vastus lateralis traction across the synchondrosis.
Q: What single radiographic feature is most useful for distinguishing bipartite patella from an acute fracture?
A: Smooth, rounded, corticated margins (a fresh fracture has sharp, non-corticated edges and a matching donor defect). The frequent bilateral occurrence is a further clue.
Q: On MRI, what indicates that a bipartite patella is the genuine source of a patient's pain?
A: Bone-marrow oedema straddling the synchondrosis (in the fragment and adjacent patella). Its absence suggests the bipartite is an incidental bystander.
Q: A young athlete fails conservative care for a symptomatic bipartite patella. Which operation gives the best return-to-sport result?
A: Fragment excision (open or arthroscopic). For a large fragment carrying articular surface, a patella-preserving lateral release is preferred to avoid patellofemoral incongruity.
Core Facts
- Failed-fusion accessory ossicle joined by a synchondrosis
- ~1-2% prevalence; usually asymptomatic and incidental
- Often bilateral - image the other knee
- Saupe type III (superolateral) ~75%, most common and symptomatic type
Saupe Classification
- Type I: inferior pole (~5%, rarest)
- Type II: lateral margin (~20%)
- Type III: superolateral corner (~75%)
- Vastus lateralis traction explains painful type III
Bipartite vs Fracture
- Bipartite: smooth, rounded, corticated, superolateral, bilateral
- Fracture: sharp, non-corticated, matching donor defect, acute history
- Active extension preserved in bipartite
- MRI marrow oedema across synchondrosis = symptomatic
Management
- Incidental: no treatment, reassure
- Painful: conservative first (most resolve)
- Refractory: fragment excision (best return to sport)
- Large articular fragment: lateral release to preserve patella
Evidence Base
Treatment Alternatives for Symptomatic Bipartite Patella
- Bipartite patella is usually an asymptomatic incidental finding; in adolescents it can cause anterior knee pain after trauma or overuse.
- Most patients improve with non-surgical treatment; surgery is reserved for failure of conservative care.
- Excision is the most popular operation with good results, but for a large fragment with articular surface, excision may cause patellofemoral incongruity - lateral release or vastus lateralis detachment are alternatives that reduce traction on the fragment.
Systematic Review: Managing the Painful Bipartite Patella
- Reviewed 22 studies of conservative care, open and arthroscopic excision or fixation, and soft-tissue release.
- All methods produced good-to-excellent results with acceptable complication rates.
- No firm guidance on the single best technique; patella-conserving methods may be more appropriate for larger fragments.
Return to Activity in Athletes - Systematic Review
- 20 studies, 125 patients / 130 knees with symptomatic bipartite patella.
- Surgery returned most athletes (~85%) to their prior level without symptoms.
- Excision of the painful fragment gave the best return-to-sport results, with ~91% returning without symptoms.
Arthroscopic Management - Systematic Review
- 11 studies / 43 patients; most underwent arthroscopic lateral release, fewer had arthroscopic excision.
- All but one patient (who sustained postoperative trauma) were pain-free after arthroscopic treatment.
- Mean return to sport ~2.6 months.