Transient Brachial Plexus / Nerve Root Injury
- A burner or stinger is a transient UNILATERAL upper-limb injury causing BURNING pain, paraesthesia and weakness after a blow, typically in collision sports such as American football; it most often affects the UPPER TRUNK of the brachial plexus / the C5-C6 distribution, so there is weakness of the deltoid, biceps and rotator cuff (supraspinatus/infraspinatus) with numbness over the lateral arm and thumb, and the symptoms are brief, usually resolving within seconds to minutes.
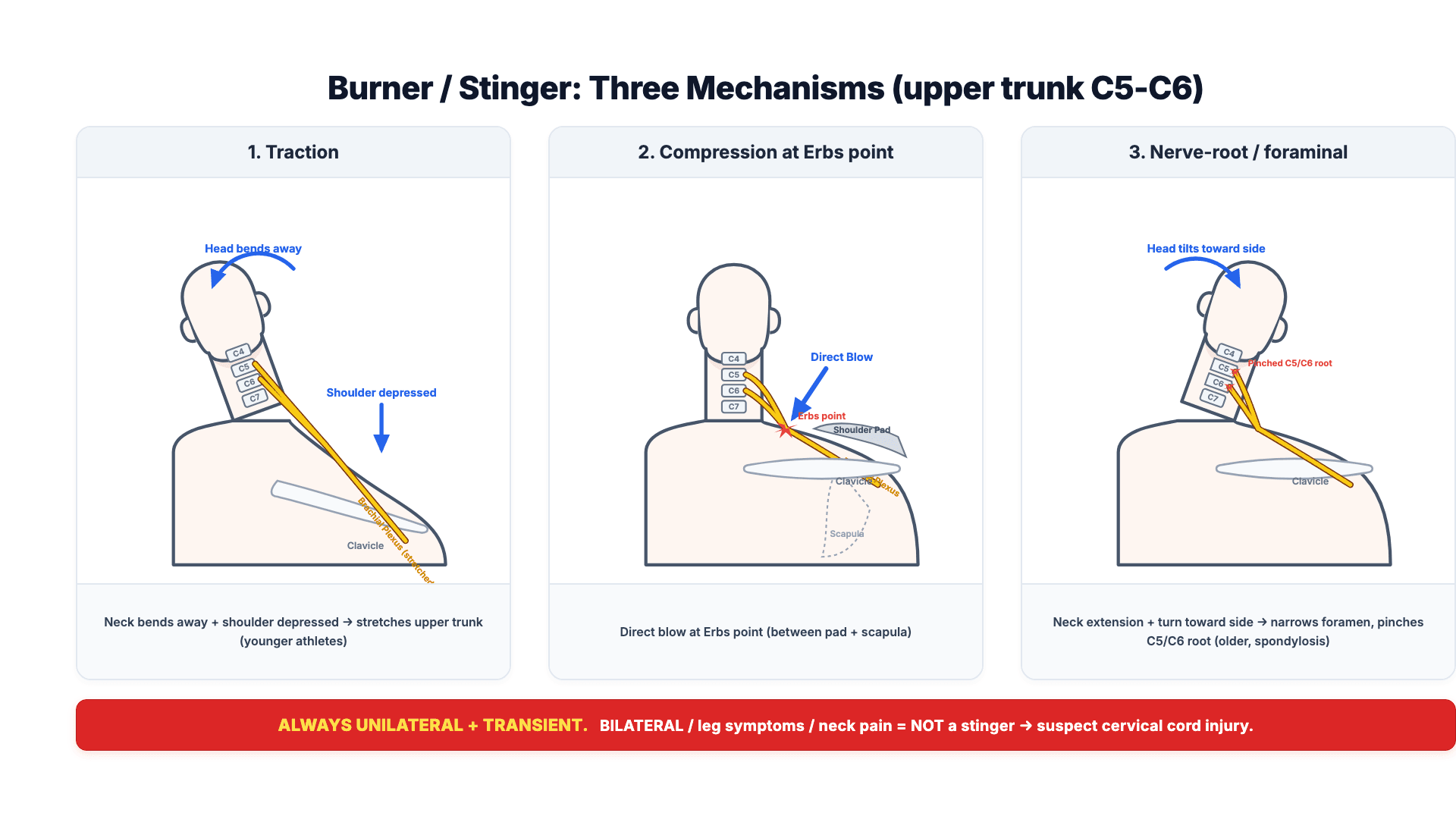
- There are THREE recognised MECHANISMS: (1) TRACTION - lateral flexion of the neck away from the affected side with depression of the shoulder, stretching the upper trunk (classic in younger athletes); (2) COMPRESSION - the fixed brachial plexus compressed between the shoulder pad and the superior-medial scapula at ERB'S POINT, which evidence suggests is a common mechanism in tackle football; and (3) NERVE-ROOT compression - neck extension with ipsilateral rotation narrowing the intervertebral foramen (more common in older athletes with cervical spondylosis).
- The single most important clinical rule is that a true stinger is ALWAYS UNILATERAL and TRANSIENT: if the symptoms are BILATERAL, involve the LOWER LIMBS, or are accompanied by NECK PAIN or midline cervical tenderness, the injury is NOT a stinger - it raises the possibility of a CERVICAL CORD or SPINE injury (including transient quadriparesis/cervical cord neurapraxia), and the athlete must be immobilised and fully evaluated and imaged.
- The DIAGNOSIS is clinical: a typical mechanism, transient unilateral upper-trunk symptoms, and a normal cervical spine with full painless range of motion once recovered; persistent or recurrent symptoms warrant further assessment (cervical spine imaging, and EMG/nerve conduction studies if weakness persists beyond about 2-3 weeks), and the differential includes cervical radiculopathy, peripheral nerve injury, thoracic outlet syndrome and (rarely) an atypical anatomical cause such as a postfixed plexus.
- RETURN TO PLAY is allowed only when the athlete has FULL, PAINLESS cervical range of motion and NORMAL upper-limb strength and sensation - a same-game return is acceptable for a brief, fully-resolved first stinger with a normal examination, but the athlete must NOT return while any weakness, numbness or neck symptoms persist.
- RECURRENT stingers should prompt evaluation for predisposing factors - cervical foraminal stenosis, congenital cervical canal stenosis (a low Torg-Pavlov ratio) and cervical spondylosis - with cervical imaging; PREVENTION includes neck and periscapular strengthening, proper tackling technique (heads-up tackling), and protective equipment such as a cervical orthosis/'cowboy collar' and shoulder-pad modification, which reduce recurrence.
- “Burner/stinger = transient UNILATERAL upper-trunk (C5-C6) burning pain/paraesthesia/weakness (deltoid, biceps, cuff; lateral arm/thumb) after a blow; resolves in minutes.
- “Three mechanisms: TRACTION (neck flexion away + shoulder depression, younger), COMPRESSION at Erb's point (shoulder pad vs scapula), NERVE-ROOT (extension+ipsilateral rotation, older/spondylosis).
- “ABSOLUTE rule: bilateral, lower-limb, or neck-pain symptoms = NOT a stinger (suspect cord/spine - immobilise/image). RTP only when full painless ROM + normal strength/sensation; recurrent -> cervical imaging.
Transient, UNILATERAL upper-trunk (C5-C6) burning pain, paraesthesia and weakness (deltoid, biceps, cuff; lateral arm/thumb) after a blow - resolves in minutes.
BILATERAL symptoms, any LOWER-LIMB involvement, or neck pain/midline tenderness - suspect a cervical cord/spine injury: immobilise and image.
Mechanisms, Diagnosis & the Red-flag Rule
A burner/stinger is a transient unilateral upper-limb burning pain, paraesthesia and weakness after a blow, affecting the upper trunk / C5-C6 (deltoid, biceps, cuff; lateral arm/thumb numbness), resolving in seconds to minutes. There are three mechanisms: traction (neck lateral flexion away + shoulder depression, younger athletes), compression at Erb's point (the fixed plexus between shoulder pad and superior-medial scapula), and nerve-root compression (neck extension + ipsilateral rotation narrowing the foramen, older athletes with spondylosis). The absolute rule is that a stinger is always unilateral and transient: bilateral symptoms, any lower-limb involvement, or neck pain/midline tenderness are NOT a stinger and raise a cervical cord/spine injury (or transient quadriparesis) - immobilise and image. Persistent or recurrent symptoms warrant cervical imaging and, if weakness persists, EMG/nerve conduction studies.
Return to Play, Recurrence & Prevention
- Return to play only when the athlete has full, painless cervical range of motion and normal upper-limb strength and sensation; a same-game return is acceptable for a brief, fully-resolved first stinger with a normal examination, but NOT while any weakness/numbness/neck symptoms persist.
- Investigate recurrent stingers: cervical imaging for foraminal stenosis, congenital canal stenosis (low Torg-Pavlov ratio) and spondylosis; EMG/NCS if weakness persists beyond about 2-3 weeks - the delay is deliberate, because denervation changes (fibrillation potentials) take roughly two to three weeks to appear, so an EMG performed earlier can be falsely reassuring.
- Exclude the dangerous differential: any bilateral/lower-limb/neck-pain features -> treat as a possible cervical cord/spine injury.
- Prevention: neck and periscapular strengthening, proper (heads-up) tackling technique, and protective equipment - a cervical orthosis/'cowboy collar' and shoulder-pad modification reduce recurrence.
The defining safety rule of burners and stingers is their unilaterality: a true stinger affects ONE arm and resolves quickly, so the moment symptoms are BILATERAL, involve the LOWER LIMBS, or come with neck pain or midline cervical tenderness, the diagnosis is NOT a stinger and a cervical spinal cord or spine injury - including transient quadriparesis/cervical cord neurapraxia - must be assumed, with spinal immobilisation and urgent imaging. Equally, an athlete with persisting weakness or numbness must not return to play, and a player with recurrent stingers needs cervical imaging to look for foraminal or congenital canal stenosis. Treating a cord injury as a 'stinger', or returning a still-symptomatic athlete, is the catastrophic error to avoid.
The 'Not a Stinger': Cervical Cord Neurapraxia
Bilateral or lower-limb symptoms point away from a stinger and towards transient quadriparesis / cervical cord neurapraxia, so the entity itself has to be known:
- What it is: cervical cord neurapraxia (CCN) / transient quadriparesis - a transient episode of bilateral (both arms, or all four limbs) sensory disturbance (burning, numbness, tingling) with or without motor weakness or paralysis, after an axial load with hyperextension or hyperflexion. It is the mirror image of a stinger: bilateral and central (cord) rather than unilateral and peripheral (plexus), and the legs may be involved. Symptoms resolve completely, usually within minutes, sometimes up to 24 to 48 hours.
- Why it happens: a transient cord compression/concussion (a "pincer" between osteophyte/disc and ligamentum flavum) in a developmentally narrow cervical canal - reduced functional reserve (less CSF cushioning the cord).
- Work-up: spinal immobilise, then MRI for canal diameter, cord signal change, disc/ligament injury and instability (the Torg-Pavlov ratio screens on a plain lateral film but has a high false-positive rate, so MRI is preferred - see our Torg Ratio topic; frank cord injury is covered in Spinal Cord Injury).
- Return to play (controversial): a single episode with a normal canal, no instability and no cord signal change may return; congenital/developmental stenosis, cord signal change, instability, ligamentous injury or recurrent episodes are relative-to-absolute contraindications to collision sport.
A stinger is unilateral and peripheral; cervical cord neurapraxia / transient quadriparesis is its bilateral, central mirror image - both arms (± legs), from transient cord compression in a narrow canal. Immobilise, get an MRI (canal diameter + cord signal), and treat stenosis, cord signal change, instability or recurrence as contraindications to return.
Localising It: Upper Trunk vs C5/C6 Root
- The upper trunk = C5 + C6, so the exam map is the same for both: deltoid (axillary, C5), biceps (musculocutaneous, C5-6) and the biceps reflex (C5-6), brachioradialis reflex and wrist extension (C6), supraspinatus/infraspinatus (suprascapular, C5-6); sensory lateral arm/shoulder (axillary, C5) and lateral forearm/thumb (C6).
- The common stinger is a post-ganglionic plexus TRACTION (or compression) injury: a traction/compression mechanism, no neck pain, a negative Spurling, and a multi-myotomal upper-trunk pattern - usually a transient neurapraxia that recovers fully.
- A nerve-ROOT radiculopathy (the third mechanism, the older spondylotic athlete) gives neck pain, a positive Spurling (extension + ipsilateral rotation reproduces the arm symptoms), and a single-root, dermatomal pattern - and points you to cervical imaging for spondylosis/foraminal stenosis.
- Why it matters: the distinction drives the work-up (image the root/spondylosis case) and the prognosis - and a true pre-ganglionic root avulsion (rare, high-energy) is a far graver, non-recovering lesion than a transient traction stinger. (Full plexus anatomy in our Brachial Plexus Anatomy topic; the root lesion in Cervical Radiculopathy and Nerve Root vs Peripheral Nerve.)
Upper trunk = C5 + C6 (deltoid/biceps/cuff; lateral arm/thumb). Separate the traction stinger (traction mechanism, no neck pain, negative Spurling, multi-myotomal, recovers) from a root radiculopathy (neck pain, positive Spurling, single-root dermatomal, older/spondylotic → image). A pre-ganglionic root avulsion is the rare, non-recovering extreme.
Mnemonics & Memory Aids
STINGER
Hook:STINGER: Single arm/transient, Three mechanisms, upper-trunk Injury, NOT a stinger if bilateral/legs/neck pain, Go back when normal, EMG/image if persistent, Reduce recurrence.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A footballer has burning pain and weakness down one arm after a tackle. What is a stinger and how do you assess it?”
“When can the athlete return to play, and how do you approach recurrent stingers?”
Recognition
- Transient UNILATERAL upper-trunk (C5-C6) burning pain/paraesthesia/weakness
- Deltoid, biceps, rotator cuff weakness; lateral arm/thumb numbness
- Resolves in seconds to minutes; collision sports
Mechanisms
- Traction: neck lateral flexion away + shoulder depression (younger)
- Compression at Erb's point (shoulder pad vs superior-medial scapula)
- Nerve-root: neck extension + ipsilateral rotation (older/spondylosis)
The red-flag rule
- Stinger is ALWAYS unilateral and transient
- Bilateral / lower-limb / neck-pain symptoms = NOT a stinger
- -> suspect cervical cord/spine injury (immobilise, image)
Return to play & recurrence
- RTP only with full painless cervical ROM + normal strength/sensation
- Persistent weakness -> cervical imaging; EMG/NCS if beyond 2-3 weeks
- Recurrent -> image (foraminal/congenital stenosis); prevent (strengthening, technique, orthosis)
Evidence & Key Studies
Upper trunk brachial plexopathy: the stinger syndrome (mechanism and prevention)
- The stinger/burner is an upper trunk brachial plexopathy; although often attributed to traction from lateral neck flexion, a common mechanism in tackle football is compression of the fixed brachial plexus between the shoulder pad and the superior-medial scapula at Erb's point.
- Electromyography and nerve-root stimulation localised the lesion to the upper trunk in affected players.
- An orthosis designed to protect the brachial plexus from the shoulder pad was effective in reducing the number of stinger episodes.
Brachial plexus radiculopathy mimicking a stinger: the importance of the differential
- A collegiate wrestler's apparent C7 'stinger' from a brachial plexus traction injury was ultimately due to a T1-T2 disc herniation impinging a postfixed brachial plexus, requiring surgery.
- The differential of a stinger includes cervical spine injury, peripheral nerve injury, spinal cord injury, thoracic outlet syndrome and brachial plexus radiculopathy.
- Persistent symptoms and anatomical variation (postfixed plexus) warrant imaging and a broad differential rather than assuming a simple stinger.
The localisation to the upper trunk, the recognition of a compression mechanism at Erb's point (shoulder pad against the superior-medial scapula) in addition to traction, and the effectiveness of a protective orthosis come from the cited Markey study; the importance of a broad differential (cervical spine, peripheral nerve, cord, thoracic outlet, radiculopathy) and the need to image persistent/atypical cases from the cited Kuzma report. The unilateral-and-transient definition, the C5-C6 distribution, the three mechanisms, the bilateral/lower-limb red-flag rule, the return-to-play criteria and the recurrent-stinger work-up are standard, well-established teaching. (See also our Cervical Spine Injury in Sport and Cervical Cord Neurapraxia topics.)