Primary restraint to lateral patellar translation in early flexion | Torn in nearly all first-time dislocations | MRI localises femoral versus patellar avulsion | Anatomic reconstruction restores stability when non-operative care fails
- Primary restraint in early flexion: the MPFL provides the majority of resistance to lateral patellar translation between 0° and 30° of knee flexion; beyond 30° the bony trochlea becomes the dominant stabiliser
- Torn in almost every first-time dislocation: acute lateral patellar dislocation produces an MPFL tear in over 90% of cases - the essential lesion that allows the patella to displace
- Location dictates management: MRI (axial T2 best) distinguishes femoral avulsion (repair or recon), patellar avulsion (anchors), and midsubstance (usually recon); bony avulsions may be reattached
- Femoral footprint is unforgiving: the isometric femoral attachment lies just distal and posterior to the adductor tubercle - malposition by even 5 mm dramatically increases graft tension or laxity through range
- Reconstruction is not always the first operation: most first-time dislocators are treated non-operatively with bracing, VMO/quad/hip strengthening and activity modification; surgery is reserved for recurrent instability, large osteochondral fragments, or high-risk anatomy
- “On a true lateral radiograph the femoral MPFL origin is approximately 1 mm anterior to the posterior cortical line of the femur and 2-3 mm proximal to the level of the posterior condyle flare - use this to check tunnel position
- “A positive apprehension test at 30° flexion that does not improve with quad contraction suggests significant soft-tissue laxity (MPFL insufficiency) rather than pure bony maltracking
- “In the acute setting do not miss the osteochondral fracture - medial patellar facet or lateral femoral condyle bone bruise on MRI is the footprint of the dislocation event
- “When planning reconstruction, measure TT-TG, patellar height (Caton-Deschamps or Insall-Salvati) and assess trochlear dysplasia on MRI - isolated MPFL reconstruction will fail if major bony factors are ignored
In more than 90% of first-time lateral patellar dislocations the MPFL is torn. It is the primary soft-tissue restraint to lateral translation in the first 30° of flexion. Without a competent MPFL the patella can escape laterally even with normal trochlear geometry.
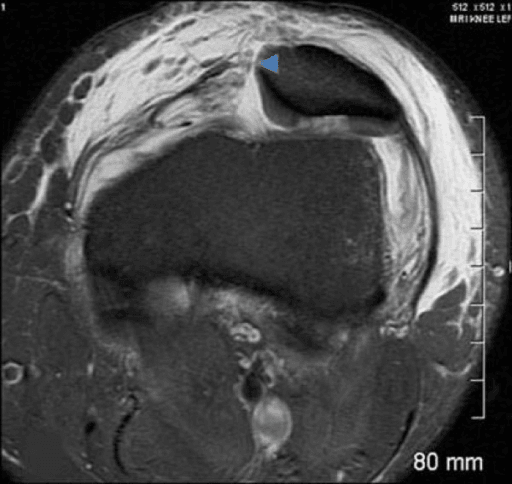
Axial T2 or fluid-sensitive sequences are the key. Look for discontinuity, retraction, and oedema at the femoral origin (just distal/posterior to adductor tubercle) or at the superomedial patellar border. A femoral-sided tear in good tissue may be repairable acutely; chronic or midsubstance tears need reconstruction.
The anatomic femoral attachment is isometric or near-isometric. A tunnel placed too proximal or anterior tightens in flexion and can cause pain or graft failure. Use the radiographic landmark on true lateral: ~1-2 mm anterior to the posterior condylar line, slightly proximal to the posterior condyle flare.
Recurrent instability after MPFL reconstruction is often due to untreated bony factors: trochlear dysplasia, elevated TT-TG (greater than 20 mm), patella alta, or femoral anteversion. Isolated soft-tissue reconstruction will not compensate for major malalignment.
Overview
The medial patellofemoral ligament (MPFL) is the primary soft-tissue restraint to lateral displacement of the patella in the first 30° of knee flexion. It is a thin, fan-shaped ligament that runs from the superomedial border of the patella to a point on the femur just distal and slightly posterior to the adductor tubercle. In the vast majority of acute lateral patellar dislocations the MPFL is torn, usually at its femoral or patellar attachment rather than in midsubstance. This tear is the essential lesion that permits the patella to escape laterally.
For the exam the story is straightforward: understand the anatomy and isometry, recognise the injury on MRI, know which patients can be treated non-operatively after a first dislocation, and be able to describe an anatomic reconstruction when surgery is indicated. The common viva traps are assuming every dislocator needs a reconstruction, forgetting to assess bony factors, and placing the femoral tunnel in a non-isometric position.
Anatomy
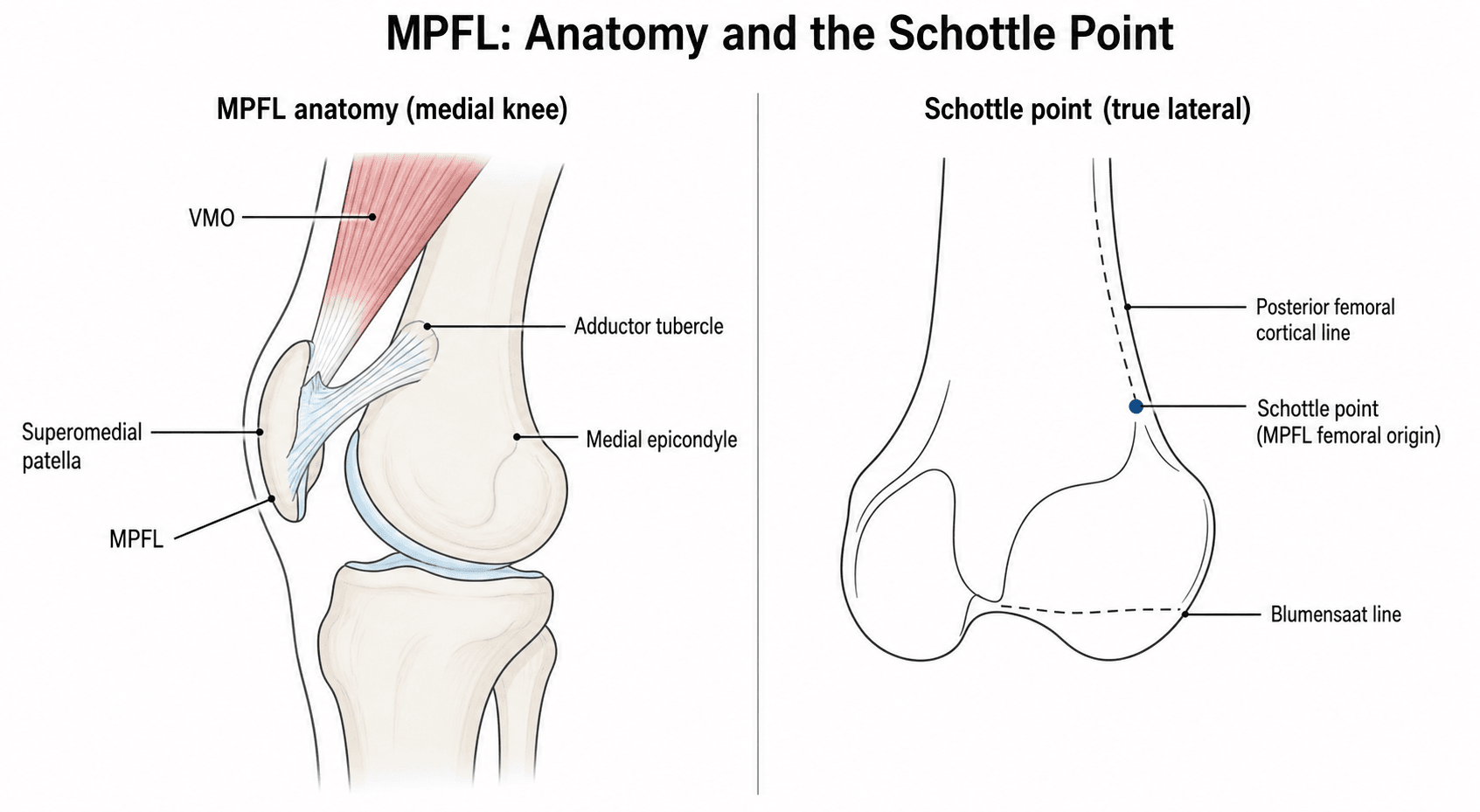
The MPFL is a capsular ligament that lies in the second layer of the medial knee, deep to the sartorius fascia and superficial to the capsule. It is approximately 50-60 mm long and 10-20 mm wide at its midpoint, fanning out toward the patella. Its fibres blend with the distal vastus medialis obliquus (VMO) aponeurosis, which is why VMO strengthening is part of every rehabilitation protocol.
Femoral origin: located in a sulcus between the adductor tubercle (proximal) and the medial epicondyle (distal). On a true lateral radiograph it lies roughly 1-2 mm anterior to the posterior cortical extension line of the femur and 2-3 mm proximal to the posterior condylar flare. This radiographic landmark is the single most useful intraoperative check for tunnel position.
Patellar insertion: the proximal third to half of the medial patellar border, with superficial fibres continuing into the VMO fascia. The insertion is broader than the femoral origin.
Biomechanical role: sectioning studies (Amis 2003) show that the MPFL provides 50-60% of the total resistance to lateral patellar translation at 0-30° of flexion. Beyond 30° the trochlear groove and lateral femoral condyle become the primary bony restraints. The ligament is tightest in extension and early flexion and slackens as the patella engages the trochlea.
Pathophysiology
Injury mechanism: the typical injury occurs during a twisting valgus movement or a direct blow to the medial patella with the knee in slight flexion. The patella translates laterally, the medial retinaculum and MPFL are loaded to failure, and the patella either spontaneously reduces or remains locked laterally. The classic bone-bruise pattern on MRI (medial patella and anterolateral femoral condyle) is the footprint of the dislocation event.
Why recurrence happens: once the MPFL is torn or stretched, the medial checkrein is lost. If the trochlea is dysplastic or the TT-TG distance is increased, the patella sits more laterally even in early flexion and the risk of repeat dislocation rises sharply. Over time, repeated subluxations can cause chondral wear on the medial patella and lateral trochlea and stretch the medial tissues further.
Healing and chronic changes: acute tears may scar in a lengthened position. Femoral avulsions in good tissue can heal with repair if addressed early; patellar avulsions with small bony fragments may require reattachment. Midsubstance tears have limited healing capacity. Chronic insufficiency leads to secondary changes in the medial retinaculum, VMO atrophy or inhibition, and progressive lateral facet overload.
Classification
There is no single universally used classification for MPFL injury, but three practical axes matter for decision-making.
- Features
- Superomedial border tear or small bony fragment with VMO
- Implication
- May heal or allow direct anchor repair
- Features
- Most common; near adductor tubercle
- Implication
- Best candidate for acute primary repair if tissue good
- Features
- Ligament fails in continuity
- Implication
- Rare; reconstruction usually required
Trochlear Dysplasia: The Dejour Classification
The topic refers repeatedly to "Dejour B-D" and the crossing sign and spur - the examiner will expect you to actually grade the trochlea. Trochlear dysplasia is the single most important bony risk factor for patellofemoral instability, and the Dejour classification (true lateral radiograph plus axial CT or MRI) is the standard.
The three radiographic signs on a true lateral:
- Crossing sign - the line of the trochlear floor crosses the anterior border of the lateral femoral condyle, meaning the groove becomes flat (flush with the condyle) at that point. This is the hallmark of dysplasia.
- Supratrochlear spur (boss) - a bony prominence projecting anteriorly above the trochlea.
- Double-contour sign - a second line behind the crossing line, representing a hypoplastic, medialised medial facet.
- Radiographic signs
- Crossing sign only
- Trochlear shape
- Shallow but still concave groove (mild)
- Radiographic signs
- Crossing sign + supratrochlear spur
- Trochlear shape
- Flat or convex trochlea
- Radiographic signs
- Crossing sign + double-contour
- Trochlear shape
- Asymmetric facets, convex lateral and hypoplastic medial facet (no spur)
- Radiographic signs
- Crossing sign + spur + double-contour (facet asymmetry / cliff)
- Trochlear shape
- Most severe; abrupt 'cliff' between facets
Quantitatively, a trochlear depth under 3 mm, a sulcus angle over 145 degrees, or a lateral trochlear inclination under 11 degrees support the diagnosis. Grades B and D (those with a spur) are the high-grade patterns most associated with failure of isolated soft-tissue surgery and are the ones in which a trochleoplasty may be considered in expert hands.
On a true lateral the crossing sign defines trochlear dysplasia (the groove goes flat). Add a supratrochlear spur and it is Dejour B; add a double-contour (hypoplastic medial facet) and it is C; have all three and it is D. The spur-containing grades (B and D) are high-grade and the ones where isolated MPFL reconstruction is most likely to fail without addressing the trochlea.
Clinical Presentation
First-time dislocation: the patient usually describes a twisting injury or fall with the knee giving way laterally. There is often an audible or palpable "pop", immediate swelling, and inability to bear weight comfortably. The patella may have reduced spontaneously or required manual reduction in the emergency department. Haemarthrosis is common.
Recurrent instability: patients report repeated "giving way" or "slipping" episodes, often with minimal trauma, a sense that the knee is "unstable" or "wobbly", and anterior or medial knee pain after episodes. They may describe the patella "jumping out and back in".
Examination:
- Look: effusion, bruising over the medial retinaculum, apprehension posture (patient holds the knee extended or in slight flexion and resists movement).
- Feel: tenderness along the medial patellar border or at the femoral origin (adductor tubercle region). Palpable defect in the retinaculum in some acute cases.
- Move: limited range due to pain and effusion; patellar apprehension test positive at 20-30° of flexion (patella is pushed laterally and the patient resists or reports impending dislocation). The test becomes negative or less positive once the patella is engaged in the trochlea in deeper flexion.
- Special tests: J-sign (patella jumps laterally in terminal extension), patellar tilt test (excessive lateral tilt), moving patellar apprehension test, and assessment for generalised ligamentous laxity.
Always examine the contralateral knee and assess for trochlear dysplasia (prominent lateral condyle, flat trochlea on palpation), Q-angle, and foot progression.
Investigations
Plain radiographs (essential first step):
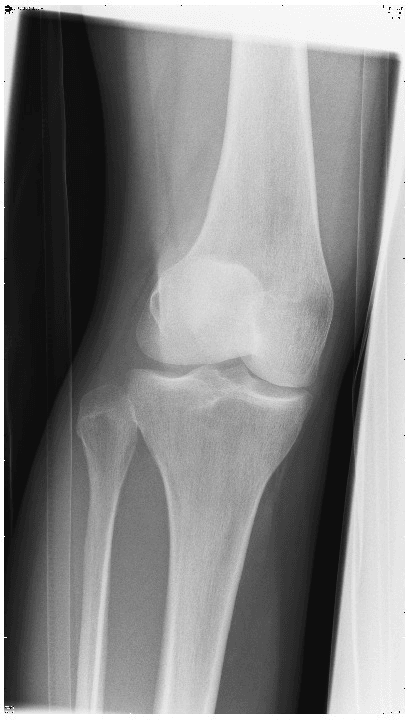
- AP, true lateral (for femoral tunnel planning and patellar height), and axial (Merchant or sunrise view at 30-45° flexion).
- Look for osteochondral fracture (medial patella or lateral femoral condyle), loose bodies, and the position of the patella on the axial view.
- On the true lateral, assess trochlear morphology (crossing sign, supratrochlear spur) and use the radiographic landmark for the MPFL femoral origin.
MRI (the investigation that changes management):
- Axial T2-weighted or PD fat-saturated sequences are best for the MPFL.
- Direct signs: discontinuity, retraction, wavy fibres, or avulsion at femoral or patellar end; surrounding oedema.
- Indirect signs: bone bruise on the medial patellar facet and anterolateral femoral condyle (the "kissing" contusion of dislocation), cartilage injury, VMO oedema or tear.
- MRI can also grade trochlear dysplasia, measure TT-TG (on superimposed slices), and assess patellar height and chondral surfaces.
CT (selected cases):
- True TT-TG distance when MRI measurement is uncertain or when planning tibial tubercle osteotomy.
- 3D reconstruction for complex trochlear dysplasia or when considering trochleoplasty (rare in most practices).
Ultrasound: can visualise the MPFL dynamically in experienced hands but is not routine for surgical planning.
Management
Indicated for the majority of first-time dislocations without large osteochondral fracture or loose body. Brief immobilisation (1-2 weeks), early motion, effusion control, and structured physiotherapy focusing on VMO activation, quadriceps and hip strengthening, and proprioception. Return to pivoting sport in 3-6 months when strength, confidence and apprehension have resolved. A patellar-stabilising brace may be used for confidence on return.
If a patient has had two or more documented dislocations and a compliant rehabilitation programme, the probability of further episodes without surgery is high. Isolated MPFL reconstruction gives good stability in properly selected patients, but the examiner will always ask what you would do with a TT-TG of 25 mm or a Dejour D trochlea.
Predicting Recurrence After a First-Time Dislocation
The decision to offer surgery after a first dislocation hinges on the risk of redislocation - and that risk is predictable from a handful of factors. This is what the examiner means by "high-risk anatomy".
- Why it raises risk
- More years and activity at risk; ligamentous laxity
- Strength
- Strongest single factor
- Why it raises risk
- Loss of the bony checkrein beyond early flexion
- Strength
- Major
- Why it raises risk
- Delayed trochlear engagement - the patella sits above the groove longer
- Strength
- Moderate
- Why it raises risk
- Lateral vector pulling the patella out of the groove
- Strength
- Moderate
- Why it raises risk
- Marker of global predisposing morphology and laxity
- Strength
- Moderate
These factors have been combined into validated tools - the Jaquith and Parikh model (skeletal immaturity, trochlear dysplasia, patella alta and contralateral instability, with recurrence rising from near zero with no factors to the great majority with all four) and the Patellar Instability Severity Score - but the practical message is the same: a young patient with a dysplastic trochlea and patella alta has a high redislocation risk, so early stabilisation is more readily justified, whereas a normal-anatomy adult with a first dislocation usually does well with rehabilitation.
The recurrence risk after a first dislocation is driven by young or skeletally immature age, trochlear dysplasia, patella alta and a previous contralateral dislocation (the Jaquith-Parikh factors; the Patellar Instability Severity Score combines similar variables). With none of these, redislocation is uncommon and rehabilitation is appropriate; with several, risk approaches the majority and earlier surgical stabilisation is reasonable even after a first event.
Complications
- Cause / timing
- Graft failure, malpositioned tunnels, untreated bony malalignment, poor patient selection
- Key point
- Most common reason for revision; always re-assess TT-TG, trochlear morphology and patellar height before the first reconstruction
- Cause / timing
- Over-tensioned graft, non-anatomic femoral tunnel, untreated cartilage injury
- Key point
- The graft should not turn the patella into a medial overload problem
- Cause / timing
- Large bone tunnels or aggressive drilling in small patellae
- Key point
- Use anchors or small-diameter double tunnels; avoid bridge fracture
- Cause / timing
- Prolonged immobilisation, overtensioning in flexion, scar formation
- Key point
- Early motion and correct tensioning are preventive
- Cause / timing
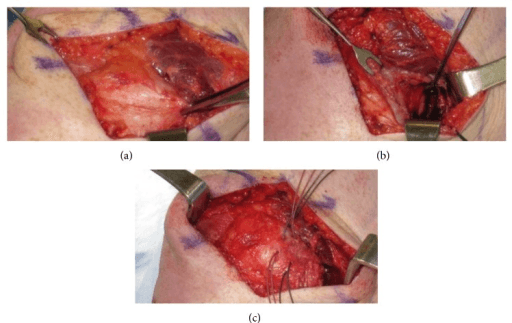
- Medial incision and graft harvest
- Key point
- Usually neurapraxia; warn patients about medial knee numbness
A femoral tunnel placed too far proximal or anterior will tighten dramatically in flexion, producing pain, limited motion, and eventual graft or cartilage failure. On a true lateral fluoroscopic image the correct point is only a few millimetres anterior to the posterior condylar line. If in doubt, check isometry with a suture or K-wire before committing to the tunnel.
Clinical Relevance
MPFL injury sits at the centre of the patellofemoral instability spectrum. A competent MPFL can compensate for mild trochlear dysplasia or a modestly elevated TT-TG; once it is torn, even normal anatomy may become symptomatic. The modern approach is "anatomic restoration": repair or reconstruct the ligament when tissue is adequate, and address major bony contributors (tubercle osteotomy, trochleoplasty) when they are the dominant drivers of instability. The examiner wants to hear that you can localise the tear, decide between repair and reconstruction, place the femoral tunnel correctly, and recognise when an isolated MPFL procedure is not enough.
Guidelines, Registries & Global Practice
-
Global epidemiology: Lateral patellar dislocation has an incidence of approximately 5-7 per 100,000 person-years, with the highest rates in adolescents and young adults, particularly females and those participating in pivoting or jumping sports. MPFL disruption is the essential soft-tissue lesion in the great majority of cases worldwide.
-
Guidelines and consensus: There is broad international agreement (AAOS, ESSKA, British Patellofemoral Group, and others) that most first-time dislocations without large osteochondral injury are managed non-operatively with structured rehabilitation. MPFL reconstruction is indicated for recurrent instability after adequate rehabilitation or when significant bony malalignment or osteochondral pathology requires addressing. Anatomic femoral tunnel placement using the radiographic landmark on a true lateral image is emphasised in all technical descriptions.
-
Registry evidence: Large joint registries (NJR, AJRR, AOANJRR, etc.) do not currently track isolated MPFL procedures in detail. Available case series and systematic reviews (including the 2020 properties review cited above) report good stability and return-to-sport rates after anatomic reconstruction in appropriately selected patients, with lower success when major bony factors are ignored. Revision rates are driven primarily by recurrent instability from technical error or untreated malalignment rather than by implant-related issues.
-
Global practice variation: In high-demand athletic or military populations some surgeons offer earlier reconstruction after a first dislocation with a clear, repairable or reconstructible tear. In lower-demand or paediatric populations a longer trial of non-operative care is common. Combined procedures (MPFL reconstruction plus tibial tubercle osteotomy or trochleoplasty) are performed more frequently in centres with expertise in complex patellofemoral dysplasia. No country-specific billing codes are relevant to clinical decision-making or examination content.
Memory aids
P-F-MMPFL Injury Locations
Hook:P-F-M - Patellar, Femoral, Midsubstance. MRI tells you which one you are dealing with and whether repair or reconstruction is realistic.
A-I-MReconstruction Principles
Hook:AIM for anatomic, isometric, and multifactor-aware reconstruction - or the graft will fail or the patient will have ongoing pain.
B-O-N-EWhen to Operate After First Dislocation
Hook:BONE - Bony fragment, Ongoing instability, No (normal) anatomy, Elite athlete. These are the main reasons to offer early stabilisation after a first dislocation.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 19-year-old university netball player sustains a first-time lateral patellar dislocation during a game. It reduces spontaneously. MRI shows a complete femoral-sided MPFL tear with a moderate effusion and typical bone bruises but no osteochondral fracture. She wants to return to competitive sport. What is your plan?”
“MRI after a first-time lateral patellar dislocation shows a clear disruption of the MPFL at its femoral origin with retraction of the ligament fibres and a small amount of oedema. The patellar insertion looks intact. There is no significant trochlear dysplasia and TT-TG is 16 mm. The patient has had two further subluxation episodes despite 4 months of physiotherapy. How do you proceed?”
“A 24-year-old has undergone MPFL reconstruction with hamstring graft 18 months ago. She had an initial improvement but now reports recurrent lateral subluxations and anterior knee pain. A true lateral radiograph shows the femoral tunnel is 8 mm proximal and 5 mm anterior to the expected anatomic point. How do you assess and manage this?”
Core Anatomy & Function
- Fan-shaped ligament from superomedial patella to femur (distal/posterior to adductor tubercle)
- Primary restraint to lateral translation in 0-30° flexion (~50-60% of resistance)
- Beyond 30° the bony trochlea becomes dominant
- Blends with VMO aponeurosis - hence VMO rehab is essential
Injury Pattern & Imaging
- Torn in greater than 90% of first-time lateral patellar dislocations
- Femoral avulsion most common; patellar avulsion or midsubstance also occur
- MRI (axial T2): look for discontinuity, retraction, oedema at femoral or patellar end
- Classic bone bruise: medial patella + anterolateral femoral condyle
Non-Operative Indications
- First-time dislocation without large osteochondral fracture or loose body
- Compliant patient willing to complete VMO/quad/hip programme
- No major bony malalignment (TT-TG less than 20 mm, mild dysplasia)
- Brace for comfort, early motion, progressive strengthening; 3-6 months to sport
Surgical Thresholds & Technique
- Recurrent instability after good rehab, large bony fragment, high-demand athlete with clear tear
- Femoral tunnel: 1-2 mm anterior to posterior condyle line on true lateral, slightly proximal to posterior condyle flare
- Graft: gracilis (preferred) or semitendinosus; double-bundle or broad configuration
- Tension at 30-60° with patella centred; avoid over-tensioning
Red Flags for Failure
- Untreated TT-TG greater than 20 mm or high-grade trochlear dysplasia
- Non-anatomic (proximal/anterior) femoral tunnel - tight in flexion, pain, eventual failure
- Patellar fracture from large tunnels or poor bone quality
- Over-tensioned graft causing medial overload and cartilage damage
Evidence
Anatomy and Biomechanics of the Medial Patellofemoral Ligament
- Cadaveric description: the MPFL is ~55 mm long (width reported 3-30 mm) running from the medial femoral epicondyle to the medial patella, overlaid by and merging with vastus medialis obliquus
- Despite being thin, the MPFL had a mean tensile strength of 208 N and is the primary passive restraint to lateral patellar displacement
- In vitro the patella subluxed most easily at ~20° of flexion, and the MPFL's restraining contribution was greatest in the extended knee (retinaculum tightest in full extension, slackening with flexion)
- The patellar insertion blends with the VMO aponeurosis, providing the rationale for including VMO/quadriceps control in rehabilitation
Avulsion-Tear Type Medial Patellofemoral Ligament Injury with a Small Bony Fragment in Lateral Patellar Dislocation
- Description of a subset of MPFL injuries in which a small bony fragment is avulsed with the ligament, usually from the patellar insertion
- The fragment is often visible on plain radiographs or CT and can be missed on MRI alone if not specifically sought
- Surgical findings confirmed that the fragment represents an avulsion at the patellar end; the ligament itself may remain in continuity or have additional intrasubstance damage
- Authors recommend careful radiographic and MRI assessment to identify these bony avulsions, as they may be amenable to direct repair or reattachment
Properties and Function of the Medial Patellofemoral Ligament: A Systematic Review
- Systematic review of 55 articles synthesising MPFL anatomy, material properties and functional behaviour (the main passive restraint to lateral patellar subluxation)
- Reported ultimate failure loads ranged 72-208 N, ultimate elongation 8.4-26 mm, and stiffness 8.0-42.5 N/mm - values that were inconsistent across studies
- The MPFL is close to isometric through the first ~50-60° of flexion then progressively shortens into deeper flexion, supporting graft fixation at flexion angles below 60°
- MPFL-deficient knees showed clear early-flexion patellar lateralisation with delayed trochlear engagement; morphology and attachment-site data remain inconsistent in the literature
Autograft Versus Allograft in Pediatric Medial Patellofemoral Ligament Reconstruction: A Systematic Review
- Systematic review of 23 studies: 849 knees in 808 paediatric patients (57.8% female, mean age 14.4 years, follow-up 46.2 months); 640 knees autograft, 209 allograft
- Patient-reported outcomes improved in both groups (Kujala, with significance in the autograft cohort); recurrent dislocation 5.5% (autograft) vs 9.1% (allograft), not statistically significant (p=0.07)
- Return-to-sport rates were similar (autograft 90.9% vs allograft 92.9%), but significantly more allograft patients returned at a level equal to or higher than pre-injury (90.9% vs 71.2%, p=0.0002)
- Data on allograft patients are sparse, limiting generalisability; the authors call for prospective comparison