Post-traumatic calcification at the MCL femoral attachment | AP knee radiograph is diagnostic | Usually self-limiting | Surgery only for refractory cases
- What it is: post-traumatic calcification or ossification at or near the femoral attachment of the medial collateral ligament of the knee, classically seen as a curvilinear density on AP radiograph medial to the femoral condyle
- Mechanism: typically follows an MCL sprain or direct blow to the medial knee; the calcification appears 3 to 6 weeks after injury and may represent heterotopic ossification within the damaged ligament
- Clinical picture: medial knee pain, stiffness, and restricted flexion after a recent knee injury; local tenderness over the medial femoral epicondyle; the patient may have forgotten the original injury
- Imaging: AP radiograph of the knee is usually diagnostic - look for calcification or ossification medial to the femoral condyle at the MCL origin; MRI shows low-signal deposit and assesses MCL integrity
- Management: predominantly conservative (rest, protected weight-bearing, physiotherapy, NSAIDs); surgical excision is rarely needed and only for refractory cases after at least 6 to 12 months of failed conservative treatment
- “The Pellegrini-Stieda lesion is one of the few orthopaedic diagnoses you can make from a single AP knee radiograph - look for the characteristic curvilinear calcification medial to the femoral condyle
- “Named after Pellegrini (1905) who described the radiographic finding and Stieda (1908) who described the associated medial knee injury - examiners love a quick historical note
- “Do NOT confuse with a medial femoral condyle avulsion fracture: the Pellegrini-Stieda calcification is separate from the cortex and lies within the MCL substance, whereas an avulsion fragment is a detached piece of bone
The Pellegrini-Stieda lesion is a spot diagnosis on an AP knee radiograph. Look for a curvilinear or comma-shaped calcification medial to the femoral condyle, at the expected location of the MCL femoral attachment. It lies separate from the cortex - this distinguishes it from an avulsion fracture.
The most common mistake is confusing it with a medial femoral condyle avulsion fracture or a medial meniscus calcification. Key difference: the Pellegrini-Stieda calcification is within the MCL substance and separate from the bone cortex, while an avulsion fragment is a detached piece of cortical bone.
The calcification appears 3 to 6 weeks after the injury - it is not visible on the initial X-ray. If you see it on a film taken immediately after trauma, think avulsion fracture instead. The delayed appearance is a hallmark of the lesion and reflects the biology of heterotopic ossification.
The vast majority of Pellegrini-Stieda lesions resolve with conservative management - rest, protected weight-bearing, physiotherapy, and NSAIDs. Surgical excision is a last resort for cases that remain painful and stiff after at least 6 to 12 months of non-operative treatment.
Overview
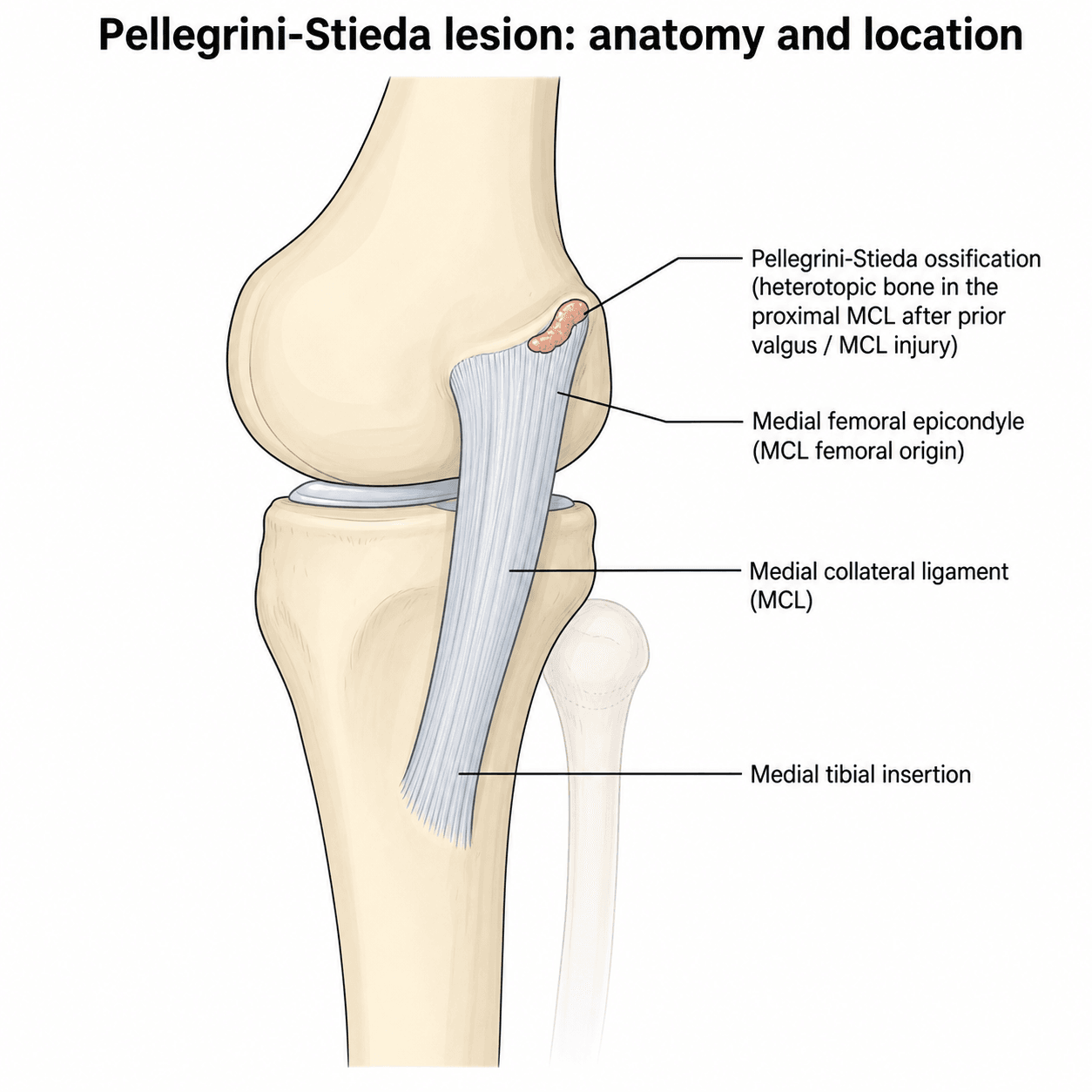
The Pellegrini-Stieda lesion is a post-traumatic calcification or ossification that develops at or near the femoral attachment of the medial collateral ligament (MCL) of the knee. It appears as a characteristic curvilinear or comma-shaped density on the AP knee radiograph, lying medial to the femoral condyle, and is one of the classic "spot diagnoses" in orthopaedic radiology.
The condition is named after Pellegrini (1905), who first described the radiographic appearance of medial knee calcification, and Stieda (1908), who reported on the associated medial knee injury. It is not a true fracture or a ligament tear but rather a form of heterotopic ossification - new bone formation within the substance of the injured MCL.
Clinically, it presents with medial knee pain, tenderness over the medial femoral epicondyle, and restricted knee flexion, typically developing weeks after an MCL sprain or a direct blow to the medial knee. The calcification is not visible on the initial X-ray and typically appears 3 to 6 weeks after the injury, which is an important diagnostic clue.
For the exam, three threads recur: recognising the lesion on the AP radiograph (and not confusing it with an avulsion fracture), understanding the pathophysiology (heterotopic ossification in a healing ligament), and knowing that management is almost always conservative.
Anatomy
The medial collateral ligament is a broad, flat ligament on the medial side of the knee. It originates from the medial femoral epicondyle and inserts onto the medial tibial metaphysis, about 5 to 7 cm distal to the joint line. It has two layers:
- Superficial MCL (tibial collateral ligament): the larger, more superficial portion, running from the medial epicondyle to the proximal tibia
- Deep MCL: blends with the joint capsule and attaches firmly to the medial meniscus
The Pellegrini-Stieda lesion forms at or near the femoral attachment of the MCL, where the ligament is tightly bound to the medial epicondyle. The adductor magnus tendon and the medial head of gastrocnemius are also nearby structures that may contribute to the pattern of calcification in some cases.
Pathophysiology
The exact mechanism of the Pellegrini-Stieda lesion remains debated, but the prevailing theory is that it represents heterotopic ossification within the damaged MCL:
- Trauma: an MCL sprain (often a valgus injury) or a direct blow to the medial knee damages the ligament fibres at or near the femoral attachment
- Inflammatory response: the damaged tissue releases inflammatory mediators and growth factors (including BMPs) that stimulate mesenchymal stem cell differentiation into osteoblasts
- Mineralisation: over the following weeks, calcium is deposited in the damaged tissue, forming an immature calcific deposit that progressively matures
- Maturation: the calcification may mature into true lamellar bone (ossification) with organised trabeculae, or it may remain as amorphous calcification
The Pellegrini-Stieda lesion is sometimes called "Pellegrini-Stieda disease" or "Pellegrini-Stieda syndrome" - the terms are used interchangeably. The key idea is heterotopic ossification in the MCL after trauma, not a separate disease entity.
Classification
There is no single universally accepted classification system for the Pellegrini-Stieda lesion. The most practical approach is to describe the lesion by its radiographic maturity, which correlates with clinical behaviour and management:
- Radiograph: thin, faint, curvilinear calcification adjacent to the medial femoral epicondyle
- Timing: 2 to 6 weeks after injury
- Clinical: often asymptomatic or causes mild local pain and stiffness
- Management: usually resolves with conservative treatment over weeks to months
- Prognosis: excellent - most settle without intervention
If asked to classify, describe what you see on the radiograph (thin and curvilinear vs dense and beak-like) and relate it to the stage of maturation. The practical implication is that early lesions almost always settle, while mature beak-type lesions are the ones that occasionally need surgery.
Clinical Presentation
The patient typically presents with medial knee pain and stiffness following a recent knee injury, often an MCL sprain or a direct blow to the medial side of the knee. Key clinical features include:
- Preceding MCL injury (valgus stress, direct blow, or sporting injury) 3 to 6 weeks earlier
- The patient may have forgotten the original injury or considered it minor
- Gradual onset of medial knee pain that worsens with activity
- Stiffness and difficulty bending the knee, especially beyond 90 degrees of flexion
- Symptoms may be worse at night or after exercise
- Localised tenderness over the medial femoral epicondyle (the MCL origin)
- Restricted knee flexion compared to the contralateral side
- Mild medial joint line swelling or fullness
- Pain on valgus stress testing (but the MCL is usually stable, not lax)
- The patient may have a limp due to pain and stiffness
Important clinical patterns
- Asymptomatic lesions: many Pellegrini-Stieda lesions are discovered incidentally on radiographs taken for other reasons and cause no symptoms
- Delayed presentation: the calcification appears weeks after injury, so the patient may present with persistent medial knee pain that was expected to have resolved by now
- Bilateral lesions: rare but possible, typically in patients with bilateral knee injuries or systemic conditions predisposing to heterotopic ossification
Medial knee calcification can also occur with chondrocalcinosis (CPPD), soft tissue calcification from renal failure, tumoral calcinosis, or previous surgery. Correlate the radiographic finding with the clinical history and examine the patient - if the calcification is not at the MCL femoral attachment or the story does not fit, consider alternative diagnoses.
Assessing the Underlying MCL: Valgus Stress Testing
The clinical section notes "pain on valgus stress testing (but the MCL is usually stable)" without developing how the test is performed or graded — yet interpreting the valgus stress test is the key examination skill for the underlying MCL injury that produced the lesion.
- Finding
- Medial joint-line opening with a firm endpoint
- Interpretation
- ISOLATES the superficial MCL (cruciates and posterior capsule relaxed) - the standard test for MCL injury
- Finding
- Medial opening in full extension
- Interpretation
- A RED FLAG - implies posteromedial-corner and/or cruciate involvement, i.e. a more severe combined injury, not an isolated MCL sprain
- Finding
- Tenderness, no laxity, firm endpoint
- Interpretation
- Partial fibre injury; heals quickly
- Finding
- Increased laxity at 30 degrees but a firm endpoint
- Interpretation
- Partial tear
- Finding
- Laxity with a soft or absent endpoint
- Interpretation
- Complete tear (most isolated grade III MCL injuries still heal non-operatively in a hinged brace)
In the Pellegrini-Stieda patient, valgus stress at 30 degrees typically reproduces PAIN but the ligament is STABLE - the calcification sits within a healed MCL. Frank laxity instead signals ongoing MCL insufficiency. Always test in FULL EXTENSION too: medial opening there points to a posteromedial-corner or cruciate injury and changes the whole management, so it must not be missed.
Investigations
Plain radiography
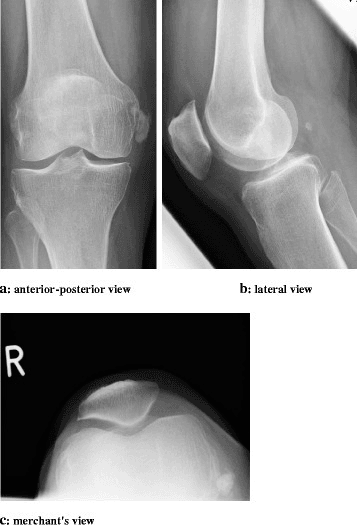
The AP radiograph of the knee is the first-line and often the only investigation needed. The Pellegrini-Stieda lesion appears as a curvilinear or comma-shaped area of calcification or ossification lying just medial to the femoral condyle, at the expected location of the MCL femoral attachment. It is separate from the femoral cortex (unlike an osteophyte) and does not extend into the joint (unlike a loose body).
The lateral view is less helpful because the calcification is superimposed on the femur, but it may show the lesion projected anteriorly if the deposit is large.
MRI
MRI is not routinely required but is useful when:
- The diagnosis is uncertain (to confirm the calcification is within the MCL)
- There is concern about associated ligament or meniscal injury
- Surgical excision is being considered (to plan the approach and assess the MCL integrity)
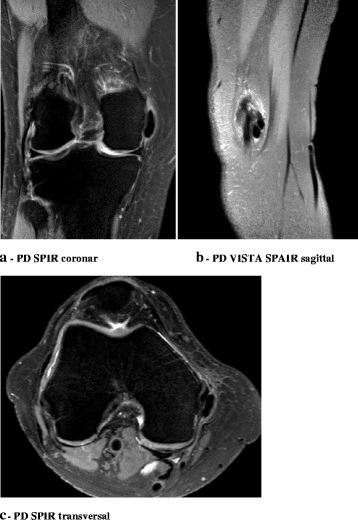
On MRI, the Pellegrini-Stieda lesion appears as an area of low signal on all sequences (T1, T2, and PD) at the MCL femoral attachment, consistent with calcification. There may be surrounding soft tissue oedema in the acute phase.
CT
CT is occasionally used for pre-operative planning to define the exact size and location of a mature ossified lesion before excision. It clearly shows the relationship of the bony mass to the femoral cortex.
- When to request
- First-line in any patient with medial knee pain after injury
- What it shows
- Curvilinear calcification medial to the femoral condyle at the MCL origin
- Key point
- Usually diagnostic - the classic spot diagnosis
- When to request
- Always obtained alongside the AP view
- What it shows
- Less specific but may show the lesion if large
- Key point
- Part of the standard knee series
- When to request
- If diagnosis uncertain, suspected associated injury, or planning surgery
- What it shows
- Low-signal deposit at MCL femoral attachment; assesses MCL integrity and other structures
- Key point
- Confirms location and excludes other pathology
- When to request
- Pre-operative planning for surgical excision
- What it shows
- Defines the size, shape, and cortical relationship of the ossified mass
- Key point
- Helps plan surgical approach and extent of excision
Management
Conservative management (the mainstay)
The vast majority of Pellegrini-Stieda lesions are managed non-operatively. Treatment follows a progressive approach:
- Rest from provocative activities
- Protected weight-bearing with crutches if needed
- Hinged knee brace to protect the MCL from valgus stress
- NSAIDs for pain and inflammation
- Cryotherapy (ice) for local swelling
- Avoid passive stretching or forced flexion
Surgical technique
When surgical excision is indicated, the approach involves:
- Medial incision over the area of calcification
- Identification and protection of the MCL fibres
- Careful excision of the calcific or ossific mass from within the ligament substance
- Preservation or repair of the MCL if its integrity is compromised
- Post-operative immobilisation in a hinged brace, followed by gradual rehabilitation
Reported outcomes of surgical excision are generally good, but the evidence base is limited to small case series and case reports. The key principle is to exhaust conservative treatment first.
In a viva, always start with conservative management and explain why you would persevere with it. Only mention surgery as a last resort, after documenting failure of at least 6 to 12 months of non-operative treatment. The examiner wants to hear that you understand the natural history and would not rush to operate.
Complications and Prognosis
- Frequency
- Common in the first 3-6 months; most settle with time
- Management
- Continue conservative treatment; NSAIDs; reassure patient about expected time course
- Frequency
- Common, especially with larger or beak-type lesions
- Management
- Gentle physiotherapy; surgical excision if mechanical block persists beyond 6-12 months
- Frequency
- Rare - the underlying ligament is usually intact
- Management
- Assess MCL stability clinically; brace if mild laxity; consider MCL reconstruction if unstable
- Frequency
- Reported in some case reports
- Management
- Careful surgical technique with preservation of MCL fibres; post-operative bracing; consider NSAID prophylaxis
- Frequency
- Very common - many lesions leave a small residual calcific density
- Management
- No treatment needed if the patient is pain-free and functional
Prognosis
The overall prognosis is very good. Most Pellegrini-Stieda lesions resolve or become asymptomatic within 6 to 12 months with conservative management. The calcification may partially or fully resorb on serial radiographs, but even if a residual density remains, it is usually of no clinical significance. The small minority of patients who require surgical excision generally achieve good outcomes, although the evidence base is limited.
Heterotopic Ossification: Prophylaxis and Context
The topic repeatedly frames the lesion as heterotopic ossification, draws the parallel to HO after hip arthroplasty, and suggests "NSAID prophylaxis" to reduce recurrence - but the HO prophylaxis framework it relies on is never set out. The principles are extrapolated from the arthroplasty and trauma literature, because there is no Pellegrini-Stieda-specific high-level evidence.
- How it works
- Inhibit prostaglandin-mediated osteoblast differentiation from mesenchymal precursors
- Practical use
- A short course (commonly about 2 to 6 weeks) after a high-risk injury or after excision; gastrointestinal and renal caution
- How it works
- Same anti-prostaglandin effect with less gastrointestinal risk
- Practical use
- Alternative where indomethacin is poorly tolerated
- How it works
- Blocks proliferation of pluripotent mesenchymal cells
- Practical use
- Reserved for very high-risk cases (mainly hip surgery), given within roughly 24 hours before to 72 hours after surgery
The reference grading for HO (around the hip) is the Brooker classification: I = islands of bone in soft tissue; II = spurs leaving over 1 cm between opposing surfaces; III = spurs leaving under 1 cm; IV = apparent ankylosis. Risk factors include male sex, prior HO, ankylosing spondylitis or DISH, and extensive surgical dissection. For the Pellegrini-Stieda lesion specifically there is NO high-level evidence for prophylaxis - a short post-injury or post-excision NSAID course is used by extrapolation to reduce formation or recurrence.
Clinical Relevance
The Pellegrini-Stieda lesion is relevant across several exam scenarios:
- Sports medicine: a complication of MCL injuries in athletes; understanding it explains why some medial knee sprains take longer than expected to settle
- Radiology viva: a classic spot diagnosis on the AP knee radiograph; knowing it and distinguishing it from avulsion fractures and other calcifications is a recurring theme
- Trauma: follows knee injuries including fractures and ligament disruptions; the delayed appearance of calcification is a key teaching point about the timeline of heterotopic ossification
- Basic science: the biology of heterotopic ossification (mesenchymal stem cell differentiation, BMP signalling, mineralisation) can be explored through this lens
- Operative surgery: rare indication for surgical excision, but the approach and principles (protect the MCL, excise the mass, rehabilitate) are examinable
The lesion connects anatomy (MCL origin), pathology (heterotopic ossification), radiology (AP knee interpretation), and management (conservative patience) in a single topic - which is exactly what examiners look for.
Guidelines, Registries and Global Practice
- No specific guidelines exist for the Pellegrini-Stieda lesion from any major orthopaedic society (AAOS, BOA, EFORT). Management is based on expert opinion, case series, and general principles of heterotopic ossification treatment.
- Conservative management is the universal standard across all regions: rest, protected mobilisation, physiotherapy, and NSAIDs. The time course and expected recovery are the same regardless of geography.
- Surgical excision is reported in case series from multiple countries (Japan, India, Europe, North America) with broadly similar indications: persistent symptoms after at least 6 to 12 months of failed conservative treatment, with a mechanical block from a mature lesion.
- Prevention: some surgeons recommend a short course of NSAIDs after MCL injury to reduce the risk of heterotopic ossification, extrapolating from the hip arthroplasty literature, but there is no high-quality evidence specific to the Pellegrini-Stieda lesion.
- Global epidemiology: the lesion is reported worldwide with no clear geographic or ethnic predilection. It is more common in athletes and active individuals who sustain MCL injuries, and may be under-diagnosed in regions where knee injuries are managed non-operatively without follow-up radiography.
- Minimally invasive techniques such as ultrasound-guided percutaneous lavage and extracorporeal shockwave therapy have been reported in individual cases, but remain experimental without Level 1 or 2 evidence.
Memory aids
MEDIALPellegrini-Stieda Features
Hook:Think MEDIAL - the lesion is on the MEDIAL side, at the MCL, and is diagnosed on the MEDIAL side of the AP radiograph.
CALCIFYDifferential Diagnosis
Hook:CALCIFY reminds you what NOT to confuse it with - and that calcification is the key radiographic finding.
RESTEDManagement Approach
Hook:Keep the patient RESTED - rest, gentle exercises, analgesia, and time. Surgery is the rare exception.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner shows you an AP knee radiograph with a curvilinear calcification medial to the femoral condyle. They ask: 'What is this and what is its significance?'”
“A 28-year-old footballer presents with persistent medial knee pain and stiffness 8 weeks after a valgus injury to the knee. Initial X-rays at the time of injury were normal. Examination shows tenderness over the medial femoral epicondyle and flexion limited to 90 degrees. How do you investigate and manage this?”
“A 45-year-old woman has had medial knee pain and progressive loss of flexion for 14 months after a fall onto the medial aspect of her knee. AP radiograph shows a well-formed bony spur projecting from the medial femoral epicondyle. Flexion is limited to 80 degrees. She has had physiotherapy and NSAIDs for 10 months without improvement. What is your management?”
Definition and Pathology
- Post-traumatic calcification or ossification at the MCL femoral attachment
- A form of heterotopic ossification within the damaged ligament
- Appears 3-6 weeks after injury on radiograph
- Named after Pellegrini (1905) and Stieda (1908)
Radiographic Appearance
- AP knee: curvilinear or comma-shaped calcification medial to femoral condyle
- Separate from the femoral cortex (not an avulsion fracture)
- Three stages: thin/curvilinear (early) to dense (established) to bony spur/beak (mature)
- MRI: low signal on all sequences at MCL origin
Clinical Features
- Medial knee pain 3-6 weeks after MCL sprain or direct blow
- Tenderness over the medial femoral epicondyle
- Restricted knee flexion (may be a mechanical block in mature lesions)
- MCL is usually stable on valgus testing
Management
- Conservative first: rest, brace, physiotherapy, NSAIDs
- Most resolve in 3-12 months
- Surgery only after 6-12 months of failed conservative treatment
- Surgical excision: medial approach, protect MCL, remove calcific mass
Differential Diagnosis
- Avulsion fracture of the medial epicondyle (cortical fragment, present on initial X-ray)
- Chondrocalcinosis / CPPD (calcification in meniscus or cartilage)
- Medial loose body (mobile, within the joint)
- Soft tissue calcification from renal failure or tumoral calcinosis
Evidence Base
The Pellegrini-Stieda Lesion of the Knee: An Anatomical and Radiological Review
- Cadaveric study of 6 fresh-frozen knees: the superficial MCL origin (n=3) or the gastrocnemius muscle origin (n=3) was marked with radio-opaque fluid and imaged to recreate the conditions under which Pellegrini and Stieda studied the lesion
- On conventional radiographs the markings showed a random distribution; the Stieda/gastrocnemius group showed no overlap of markings at all
- No position comparable to the original Pellegrini and Stieda images could be reproduced from the cadaveric markings
- Conventional X-ray of the knee could NOT reproduce a distinction between the superficial MCL and the gastrocnemius as the origin of the lesion
Ultrasound-guided Percutaneous Lavage as Treatment for Pellegrini-Stieda Syndrome
- Case report of a 52-year-old woman with one week of severe right medial knee pain and stiffness from a calcific Pellegrini-Stieda lesion within the MCL, treated with ultrasound-guided percutaneous lavage (UGPL / barbotage)
- The technique involves needle aspiration and saline lavage of the calcific deposit under ultrasound guidance, similar to the treatment of calcific tendinitis of the shoulder
- Pain-free walking and bending at follow-up; Lower Extremity Functional Scale improved to 64/80 at 1 week and 72/80 at 1 month, with no complications
- The authors proposed that the pathomechanism may be similar to calcific tendinitis of the rotator cuff (reactive calcification with pre-calcific, formative, resorptive and healing phases)
Unicompartmental Knee Arthroplasty for Knee Osteoarthritis With the Pellegrini-Stieda Lesion: A Case Report
- Case report of end-stage medial-compartment knee osteoarthritis with a co-existing Pellegrini-Stieda lesion (ossification at the MCL origin) treated by unicompartmental knee arthroplasty (UKA)
- During postoperative follow-up the ossification lesion gradually DISAPPEARED and did not relapse
- The authors attributed the resolution to UKA correcting the abnormal biomechanics of the varus osteoarthritic knee
- A co-existing Pellegrini-Stieda lesion did not preclude a successful UKA
The Pellegrini-Stieda Lesion Dissected Historically
- Historical and systematic review (4,997 PubMed/MEDLINE articles screened, 37 analysed) tracing the original descriptions by Pellegrini (1905) and Stieda (1908) and the evolving views on the lesion's origin
- Proposed origins of the medial knee calcification include the MCL, medial gastrocnemius, adductor magnus, vastus medialis, and the deep/superficial MCL
- The MCL was most often cited as the origin (54% overall; 25% on MRI, 57% at surgery), but many cases remained undecided (e.g. 50% on MRI)
- The eponym fits because Pellegrini and Stieda held two different views on the origin; MRI is a noninvasive and relatively accurate method to determine it