The medial triceps head dislocates over the medial epicondyle | Often snaps the ulnar nerve with it | Dynamic ultrasound is the key diagnostic test | Surgery when conservative care fails
- What it is: the medial head of the triceps (or an accessory anconeus epitrochlearis muscle) dislocates over the medial epicondyle during elbow flexion, producing a painful snap
- Ulnar nerve involvement is common: the dislocating muscle often carries the ulnar nerve with it, so patients may have both mechanical snapping and ulnar neuropathy symptoms (numbness in the little and ring fingers, weakness of the intrinsics)
- Dynamic ultrasound is the diagnostic gold standard: real-time imaging during active flexion and extension shows the muscle or nerve moving over the epicondyle — plain films and static MRI can miss it
- Conservative first: activity modification, avoiding provocative positions, NSAIDs, and night splinting; surgery (resection of the snapping portion of triceps, with ulnar nerve decompression or transposition if needed) for failed conservative care
- Think of it in overhead athletes: pitchers, javelin throwers, weightlifters, and gymnasts — anyone who repetitively loads the medial elbow in flexion
- “Feel for the snap yourself — place your fingers over the medial epicondyle and ask the patient to flex and extend the elbow actively; the snap is often palpable and audible
- “Always test for ulnar nerve symptoms — the presence or absence of neuropathy changes management (isolated resection versus resection plus nerve transposition)
- “Dynamic ultrasound beats MRI because the pathology is positional — a static scan in extension may look completely normal
- “Distinguish snapping triceps from isolated ulnar nerve subluxation and from medial collateral ligament injury — the history and examination are different
The diagnosis is made by real-time dynamic ultrasound with the patient actively flexing and extending the elbow. Static imaging (plain X-ray, MRI at rest) often appears normal because the dislocation only happens with motion. If you suspect snapping triceps, order dynamic musculoskeletal ultrasound.
The presence or absence of ulnar neuropathy is the critical branch point. Isolated snapping without neuropathy: resection of the snapping portion alone. Snapping with neuropathy: resection plus ulnar nerve decompression or anterior transposition. Always document sensation in the little finger and interosseous strength.
Isolated ulnar nerve subluxation (Type III) snaps without a clear triceps component. The history is a snap with flexion but no palpable muscle band. Management is cubital tunnel release with or without transposition. Do not assume every snapping medial elbow is triceps-related.
Baseball pitchers, javelin throwers, weightlifters, and gymnasts place repetitive valgus and flexion stress on the medial elbow. In this group, think of snapping triceps alongside ulnar collateral ligament injury and valgus extension overload.
Overview
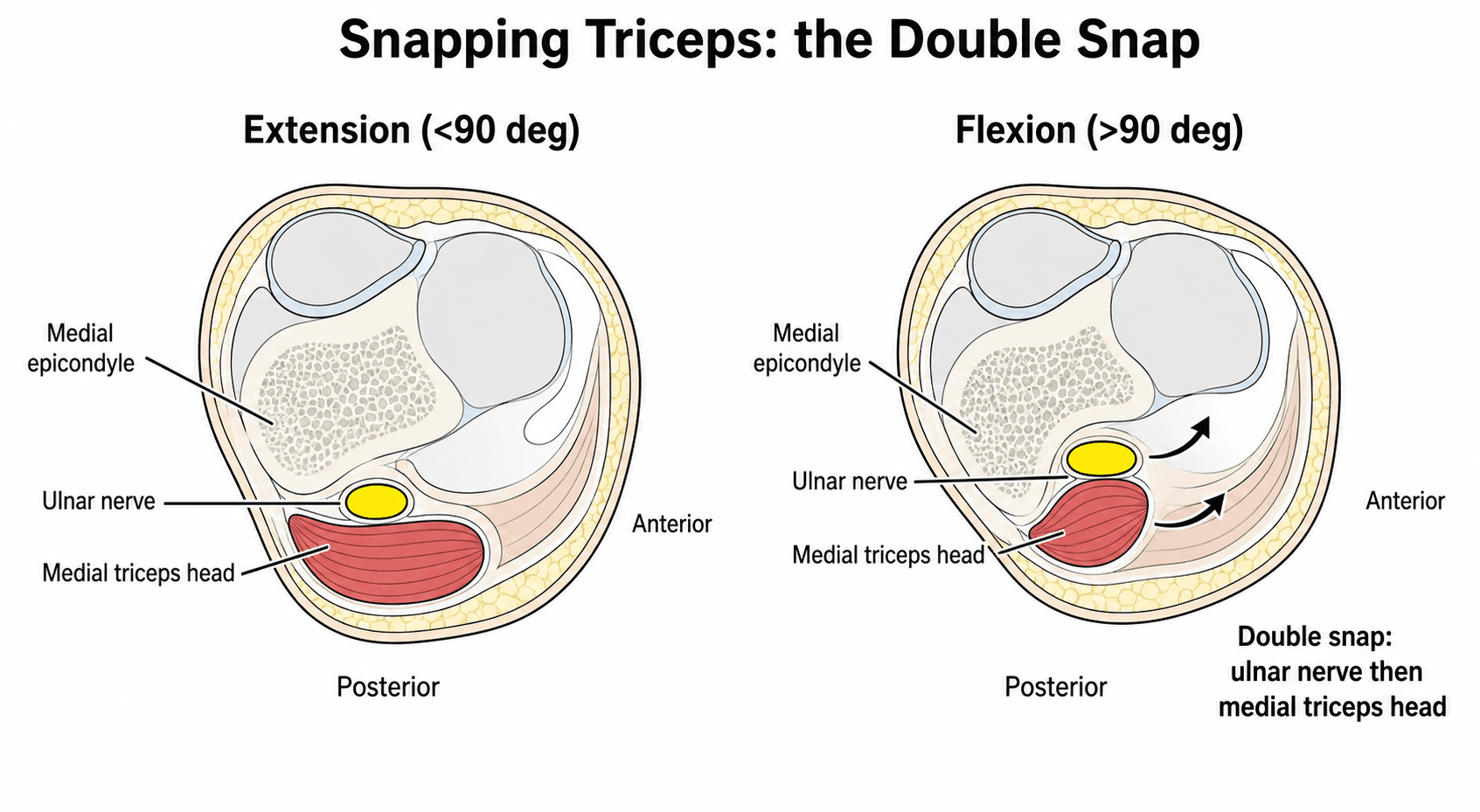
Snapping triceps syndrome is a cause of painful mechanical snapping over the medial aspect of the elbow. The condition occurs when the medial head of the triceps tendon or an accessory muscle band (the anconeus epitrochlearis) dislocates over the medial epicondyle during elbow flexion, often snapping back into place on extension. The snap is frequently accompanied by subluxation of the ulnar nerve, which lies in the cubital tunnel directly posterior to the medial epicondyle.
The syndrome is uncommon but well described in the literature, particularly in overhead throwing athletes, weightlifters, and gymnasts — anyone who repetitively loads the medial elbow in deep flexion. It can be unilateral or bilateral and may present with isolated mechanical symptoms or with combined mechanical snapping and ulnar neuropathy.
The examiner's challenge is to recognise the condition, distinguish it from isolated ulnar nerve subluxation and other causes of medial elbow pain, and confirm it with dynamic ultrasound — the diagnostic test of choice. Management is conservative initially; surgery (resection of the snapping structure, with or without ulnar nerve transposition) is reserved for patients with persistent symptoms.
Pathophysiology
Relevant anatomy
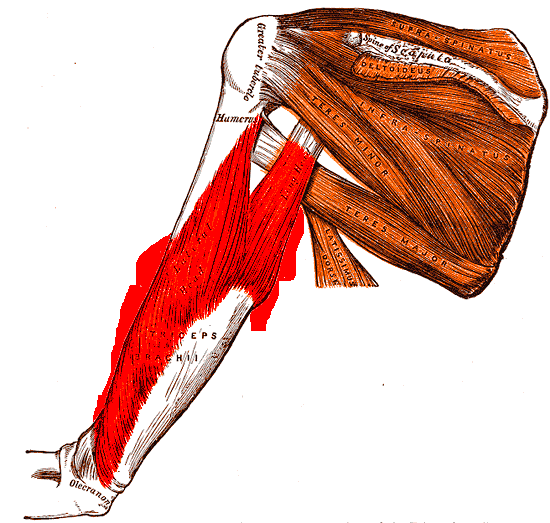
The medial head of the triceps brachii arises from the posterior aspect of the humerus distal to the radial groove and inserts onto the olecranon. In some individuals, an accessory muscle band — the anconeus epitrochlearis — arises from the medial head and crosses the cubital tunnel to insert onto the olecranon or the fascia over the medial epicondyle. This accessory band is present in approximately 10 to 25 percent of the population and is the anatomic substrate for snapping triceps in many cases.
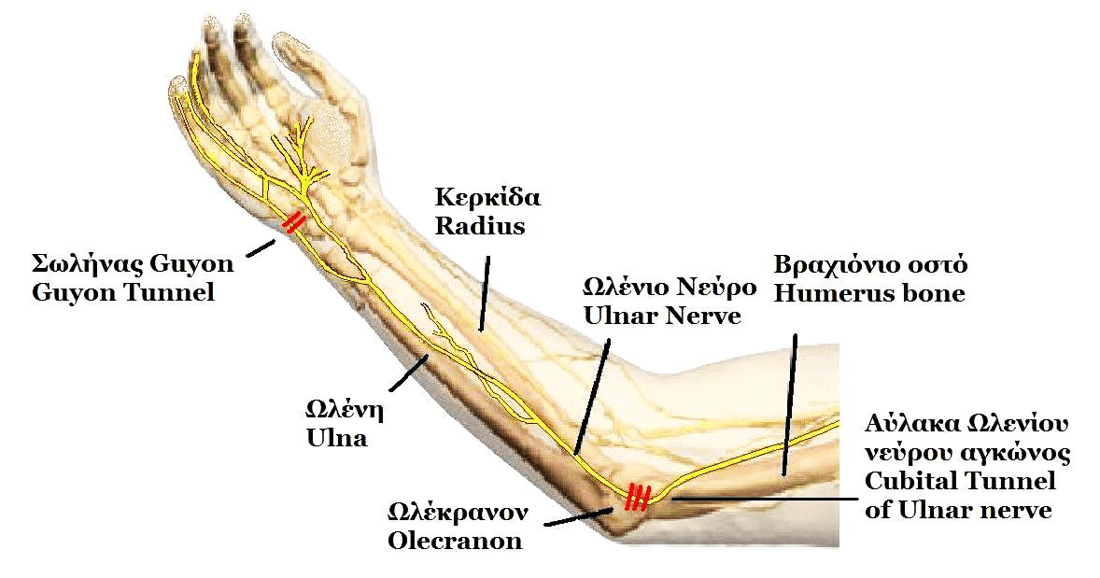
The ulnar nerve passes through the cubital tunnel, a fibro-osseous canal bounded by the medial epicondyle anteriorly, the olecranon posteriorly, and the Osborne ligament (a fascial band between the two heads of the flexor carpi ulnaris) distally. The roof of the cubital tunnel is formed by a fibrous arcade. When the elbow flexes, the cubital tunnel narrows and the ulnar nerve normally glides slightly. In snapping triceps, the dislocating triceps tendon or accessory muscle band pushes the ulnar nerve anteriorly over the medial epicondyle, producing both the mechanical snap and neural compression.
Pathophysiology
The fundamental problem is a mechanical conflict between a mobile structure (the medial triceps tendon or an accessory band) and a fixed bony prominence (the medial epicondyle). During elbow flexion:
- The triceps tendon or accessory band moves anteriorly relative to the humerus.
- It encounters the medial epicondyle and is forced to dislocate over it.
- The ulnar nerve, if adjacent to the dislocating structure, is carried with it.
- On extension, the structure snaps back into its normal position.
Repeated dislocation causes repetitive traction and compression of the ulnar nerve, leading to focal demyelination, inflammation, and in chronic cases axonal loss. The snapping tendon itself can become irritated and inflamed, producing localized pain.
The anconeus epitrochlearis is the classic anatomic variant responsible for snapping triceps, but any thickened or bifurcated medial triceps tendon can produce the same effect. The key concept is a mobile soft-tissue structure crossing a bony pulley.
Classification
Snapping elbow can be classified by the structure involved and by the presence or absence of ulnar nerve symptoms. This classification guides management.
- Structure involved
- Medial triceps head or accessory muscle band dislocates over medial epicondyle
- Ulnar nerve
- No neuropathy
- Management
- Conservative first; resection of snapping portion if symptoms persist
- Structure involved
- Dislocating triceps carries the ulnar nerve over the medial epicondyle
- Ulnar nerve
- Neuropathy present (sensory and/or motor)
- Management
- Resection of snapping portion plus ulnar nerve decompression or anterior transposition
- Structure involved
- Ulnar nerve subluxates alone without a clear triceps component
- Ulnar nerve
- Neuropathy usually present
- Management
- Cubital tunnel release with or without anterior transposition
Type II is the most common presentation in clinical practice because patients with a painless mechanical snap (Type I) often do not seek medical attention. The presence of ulnar nerve symptoms is the branch point that changes operative management from isolated resection to resection plus nerve transposition.
Grading Ulnar Neuropathy: The McGowan Classification
Because the ulnar nerve drives management here, the examiner expects you to grade the neuropathy, not just note its presence. The McGowan classification is the standard severity grade for cubital-tunnel / ulnar neuropathy at the elbow.
- Findings
- Intermittent paraesthesia and subjective sensory symptoms; NO motor weakness or wasting
- Implication
- Often responds to conservative care
- Findings
- Measurable sensory loss and/or weakness of the intrinsics; little or no wasting
- Implication
- Surgery usually indicated; good recovery potential
- Findings
- Marked intrinsic wasting, persistent weakness and sensory loss (axonal loss)
- Implication
- Decompression still worthwhile but recovery is often incomplete
The modified (Goldberg) McGowan system subdivides grade II into IIA (no muscle atrophy) and IIB (atrophy present), because atrophy worsens the prognosis. Dellon's mild/moderate/severe system is an alternative.
Use McGowan: grade I = sensory only (conservative often works), grade II = motor weakness without much wasting (operate, good prognosis), grade III = established intrinsic wasting and axonal loss (operate, but warn recovery may be incomplete). The modified system splits II into IIA (no atrophy) and IIB (atrophy). Higher grade and visible wasting push you towards earlier, more definitive surgery and more guarded counselling.
Clinical Presentation
History
Patients typically report a painful snapping or clicking sensation over the medial aspect of the elbow that occurs with flexion and resolves on extension. The snap may be audible and is often visible. Common features include:
- Mechanical symptoms: a palpable or audible snap with elbow flexion, often reproduced during everyday activities such as lifting, throwing, or push-ups
- Pain: aching or sharp pain localized to the medial epicondyle, worse after activity
- Ulnar nerve symptoms: numbness or tingling in the little and ring fingers, worse at night or with prolonged elbow flexion; in chronic cases, weakness of the interossei (difficulty spreading fingers) and thumb adduction (Froment sign)
- Activity history: overhead throwing, weightlifting, gymnastics, or occupations requiring repetitive elbow flexion under load
Physical examination
Inspection: there may be visible snapping over the medial epicondyle during active flexion and extension. Look for muscle wasting in the hand (interossei, hypothenar eminence) if chronic ulnar neuropathy is present.
Palpation: place the fingertips over the medial epicondyle and cubital tunnel and ask the patient to flex and extend the elbow actively. A palpable snap or subluxation of a tendon or nerve is often evident. Tenderness over the medial epicondyle and cubital tunnel is common.
Special tests:
- Ulnar nerve Tinel test: percussion over the cubital tunnel reproduces tingling in the ulnar nerve distribution — positive if neuropathy is present
- Elbow flexion test: holding the elbow in maximal flexion for 60 seconds reproduces ulnar nerve symptoms — positive in cubital tunnel syndrome or ulnar nerve subluxation
- Froment sign: the patient pinches a piece of paper between the thumb and index finger; weakness of the adductor pollicis (ulnar nerve) causes flexion of the thumb interphalangeal joint (compensation by flexor pollicis longus, median nerve)
- Wartenberg sign: the little finger drifts into abduction at rest due to weakness of the palmar interossei
Neurovascular examination: document sensation in the ulnar nerve distribution (dorsal and palmar aspects of the little finger and the ulnar half of the ring finger) and strength of the intrinsic hand muscles. Document two-point discrimination if neuropathy is suspected.
The most reliable examination finding is the reproducible snap with active flexion felt by the examiner's fingers over the medial epicondyle. If you can feel it yourself, you have made the diagnosis clinically. Always pair this with a full ulnar nerve examination because the presence of neuropathy changes management.
Investigations
Imaging
Dynamic musculoskeletal ultrasound is the first-line and most valuable imaging test. It is performed with the patient actively flexing and extending the elbow while the transducer is placed over the medial epicondyle in a longitudinal orientation. Real-time imaging demonstrates:
- Dislocation of the medial triceps tendon or an accessory muscle band over the medial epicondyle
- Concomitant subluxation of the ulnar nerve
- The relationship between the snapping structure and the nerve
- Any anatomic variant such as a bifurcated medial triceps head or anconeus epitrochlearis
Magnetic resonance imaging (MRI) is useful for evaluating associated pathology but is a static test and may miss the dynamic dislocation. MRI can demonstrate:
- Enlargement and increased signal of the ulnar nerve on T2-weighted or fat-suppressed sequences
- Fluid in the cubital tunnel
- An accessory muscle band or bifurcated triceps tendon
- Thickening or signal change in the triceps tendon
Plain radiographs are usually normal but should be obtained to exclude bony pathology such as an avulsion fracture, osteophyte, or loose body.
Electromyography (EMG) and nerve conduction studies are indicated if ulnar neuropathy is suspected. Findings may include:
- Slowing of ulnar nerve conduction velocity across the elbow
- Prolonged distal motor latency
- Denervation changes in the ulnar-innervated intrinsic hand muscles (positive sharp waves, fibrillation potentials, reduced recruitment)
Diagnostic approach
- Role
- First-line imaging; confirms diagnosis
- Key finding
- Real-time dislocation of triceps and/or ulnar nerve over medial epicondyle during flexion
- Role
- Static assessment of soft tissues and nerve
- Key finding
- Ulnar nerve enlargement and T2 hyperintensity; accessory muscle band; cubital tunnel fluid
- Role
- Exclude bony pathology
- Key finding
- Usually normal; may show osteophytes or loose bodies as alternative causes
- Role
- Assess ulnar neuropathy severity
- Key finding
- Slowing across elbow; denervation in intrinsic hand muscles
If a patient has classic history and examination but static MRI is normal, do not be reassured — the diagnosis is made by dynamic ultrasound. Always request a dynamic musculoskeletal ultrasound study with active elbow flexion and extension.
Management
Conservative treatment is the first-line approach for all patients, particularly those without significant ulnar neuropathy. It includes:
- Activity modification: avoidance of provocative activities such as overhead throwing, deep elbow flexion, and heavy lifting
- Night splinting: a thermoplastic splint holding the elbow in 30 to 45 degrees of flexion prevents extreme flexion during sleep and reduces ulnar nerve compression
- Non-steroidal anti-inflammatory drugs (NSAIDs): for pain relief and reduction of peritendinous inflammation
- Physical therapy: stretching of the triceps and flexor-pronator mass, strengthening of the periscapular and rotator cuff musculature (in throwers), and technique modification
- Nerve gliding exercises: if mild ulnar neuropathy is present, neural mobilisation exercises may reduce symptoms
Conservative management has variable success. Patients with an identifiable mechanical snap and mild symptoms may improve with activity modification alone. Those with persistent symptoms after 3 to 6 months of conservative care are candidates for surgery.
The critical operative decision is whether to transpose the ulnar nerve. If the nerve subluxates with the triceps and the patient has neuropathy, transposition is usually recommended to prevent ongoing traction and compression. In-situ decompression alone risks persistent symptoms if the nerve remains unstable.
Ulnar Nerve: Decompression and Transposition Options
When neuropathy or an unstable nerve accompanies the snapping triceps, you must choose how to handle the ulnar nerve - and the examiner will ask you to compare the options.
- What it does
- Release the Osborne ligament and cubital-tunnel roof; nerve left in its groove
- Notes / role in snapping triceps
- Least disruptive and preserves blood supply, but inadequate alone when the nerve subluxates - generally insufficient for snapping triceps
- What it does
- Nerve moved anterior to the epicondyle, held by a fascial sling in the subcutaneous plane
- Notes / role in snapping triceps
- Simple, removes the epicondyle as a pulley; works well in thin patients; risk of re-subluxation if poorly secured
- What it does
- Nerve placed deep to the flexor-pronator mass (Learmonth)
- Notes / role in snapping triceps
- Best padding and protection; favoured in throwers, revisions and thin patients; more dissection and longer recovery
- What it does
- Removes the bony pulley so the nerve no longer catches over it
- Notes / role in snapping triceps
- Avoids formal transposition but risks valgus instability (MCL origin) and flexor-pronator weakness
The key principle in snapping triceps is that the nerve is unstable (it subluxates with the muscle), so an in-situ decompression alone leaves it catching on the epicondyle - anterior transposition (subcutaneous or submuscular) is therefore preferred once the snapping portion is resected.
The options run from least to most disruptive: in-situ decompression, then subcutaneous transposition, then submuscular transposition, then medial epicondylectomy. In snapping triceps the nerve is unstable, so simple in-situ decompression is usually inadequate - choose an anterior transposition (submuscular is well-padded and favoured in throwers and revisions; subcutaneous is simpler) after resecting the snapping triceps portion. Medial epicondylectomy removes the pulley but risks valgus instability.
Complications
- Context
- Inadequate resection of the snapping structure
- Key point
- Ensure complete resection of the accessory band or dislocating tendon at index surgery
- Context
- Surgical traction or inadequate transposition
- Key point
- Handle the nerve delicately; transpose if unstable to prevent postoperative neuropathy
- Context
- Any elbow surgery
- Key point
- Early controlled mobilisation; avoid prolonged immobilisation
- Context
- Any open surgery
- Key point
- Standard perioperative antibiotics and sterile technique
- Context
- Rare; excessive bone removal or avulsion
- Key point
- Preserve the medial epicondyle and flexor-pronator origin
- Context
- Chronic compression with axonal loss
- Key point
- Set realistic expectations; recovery may take months and may be incomplete if denervation is advanced
Clinical Relevance
Snapping triceps syndrome is a high-yield topic because it tests the candidate's understanding of dynamic elbow pathology, ulnar nerve anatomy, and the interface between sports medicine and peripheral nerve surgery. Examiners may present it as:
- A sports-medicine case in an overhead athlete with medial elbow pain and snapping
- A peripheral nerve viva focusing on ulnar neuropathy at the elbow with an unstable nerve
- An imaging interpretation question showing dynamic ultrasound or MRI of the cubital tunnel
- A surgical technique question asking how to manage a patient with both snapping and neuropathy
The condition also illustrates broader principles: the importance of dynamic imaging for positional pathology, the need to assess nerve function in every case, and the concept that anatomic variants (the anconeus epitrochlearis) can produce clinically significant pathology.
Guidelines, Registries and Global Practice
- Diagnosis: Dynamic musculoskeletal ultrasound is the consensus first-line imaging test across orthopaedic and radiology literature worldwide. Static MRI and plain radiographs play supporting roles. There is no society guideline specific to snapping triceps, but the approach is consistent in sports-medicine and upper-extremity surgery literature from North America, Europe, and Asia.
- Conservative management: Activity modification, night splinting, and physiotherapy are universally accepted as first-line treatment. The duration of conservative trial varies (typically 3 to 6 months) depending on symptom severity and functional demands.
- Surgical approach: Resection of the snapping tendon or accessory muscle band is the standard operative treatment. The addition of ulnar nerve transposition when neuropathy is present is supported by case series and expert consensus, though no randomised trials compare in-situ decompression versus transposition specifically for snapping triceps.
- Athlete populations: Baseball pitchers (USA, Japan, Latin America), javelin throwers (Europe, Africa, Asia), and gymnasts (global) are the most frequently reported populations. Management principles are the same regardless of geographic setting, though access to dynamic musculoskeletal ultrasound and specialist hand/upper-extremity surgeons may vary by region.
- Prognosis: Most patients who undergo appropriate surgery (resection with or without nerve transposition) experience resolution of snapping and improvement in ulnar nerve symptoms. Recovery of chronic neuropathy may be incomplete if axonal loss is advanced.
Memory aids
SNAPSnapping Triceps Features
Hook:When the elbow goes SNAP, think of the triceps snapping over the medial epicondyle and taking the ulnar nerve with it.
CUREManagement Algorithm
Hook:The CURE for a snapping triceps is Conservative care first, Ultrasound to confirm, Resection if it fails, and Evaluate the ulnar nerve.
MUSCLEDifferential Diagnosis
Hook:When the elbow MUSCLEs are acting up, run through the differential to avoid misdiagnosing snapping triceps.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 22-year-old baseball pitcher presents with a 6-month history of painful snapping over the medial elbow when throwing. He also reports intermittent numbness in his little finger. The examiner asks you to take a history, examine him, and discuss your management.”
“A 30-year-old weightlifter has failed 6 months of conservative management for snapping triceps syndrome. He has moderate ulnar neuropathy with numbness in the little finger, positive Tinel and flexion tests, and EMG showing slowing across the elbow. The examiner asks you to describe your operative plan.”
“A 25-year-old gymnast reports a snap over the medial elbow with flexion. The examiner asks you to list the differential diagnosis and explain how you would distinguish between them.”
What It Is
- Medial triceps head or accessory band dislocates over medial epicondyle
- Often carries the ulnar nerve with it
- Painful snap with elbow flexion; may be audible and palpable
- Common in overhead throwers, weightlifters, gymnasts
Examination
- Feel the snap yourself over the medial epicondyle during active flexion
- Full ulnar nerve examination: Tinel, flexion test, Froment, Wartenberg
- Look for intrinsic hand wasting if chronic neuropathy
- Distinguish from isolated nerve subluxation and MCL injury
Investigations
- Dynamic ultrasound: first-line, shows real-time dislocation
- MRI: static assessment of nerve and soft tissues; may appear normal
- X-ray: exclude loose body or bony pathology
- EMG/NCS: quantify ulnar neuropathy if present
Management
- Conservative first: activity modification, night splint, NSAIDs, physiotherapy
- Surgery for failed conservative care or progressive neuropathy
- Type I (no neuropathy): resection of snapping portion alone
- Type II (neuropathy): resection plus ulnar nerve decompression/transposition
Operative Pearls
- Medial approach; identify and protect ulnar nerve throughout
- Resect the accessory band or dislocating tendon; preserve triceps function
- Transpose the nerve if unstable or neuropathy is moderate to severe
- Early mobilisation to prevent stiffness; return to sport at 3 to 6 months
Evidence
Snapping Triceps Syndrome: Review and Proposed Operative Treatment Algorithm
- Literature review of 24 studies (64 patients) with snapping triceps syndrome
- 90.6% (58/64) had coexisting ulnar nerve instability and 64.1% (41/64) had symptoms of ulnar neuropathy - so the two almost always travel together ('double snapping')
- Surgery was performed in 67.2%; strikingly, the snapping triceps had been unrecognised at a prior index elbow operation in 44.2% of operated patients
- Proposed an operative algorithm driven by ulnar nerve subluxation/neuropathy, with dynamic ultrasound as the key diagnostic test
Snapping Triceps Syndrome: Surgical Technique
- Detailed step-by-step surgical technique for resection of the snapping medial triceps head
- Described a medial approach with identification and protection of the ulnar nerve
- Emphasised resection of the dislocating tendon or accessory band while preserving triceps function
- Reported good outcomes with resolution of snapping and improvement in ulnar nerve symptoms when transposition was combined
Ultrasonographic Differential Diagnosis of Medial Elbow Pain
- Review of ultrasound findings in medial elbow pain including ulnar collateral ligament injury, ulnar neuropathy, and snapping triceps
- Described dynamic ultrasound technique for identifying ulnar nerve subluxation and snapping triceps
- Highlighted the utility of real-time imaging to distinguish between soft-tissue and neural causes of snapping
- Provided imaging criteria for cubital tunnel syndrome versus ulnar nerve instability
Bilateral Snapping Triceps Syndrome: A Case Report
- Case report of bilateral snapping triceps syndrome in a 23-year-old active man presenting with painful snapping on the medial side of both elbows during push-ups
- Two distinct, palpable and audible snaps per elbow ('double snapping') - the clinical hallmark of combined ulnar nerve and medial triceps head dislocation
- Dynamic ultrasonography showed BOTH the ulnar nerve and the medial head of the triceps dislocating anteriorly over the medial epicondyle during flexion
- Treated surgically with staged anterior subcutaneous ulnar nerve transposition plus partial resection of the snapping triceps portion; pain and snapping resolved and he was asymptomatic by 3 months