Scapulothoracic Bursitis | Painful Crepitus | Osseous vs Soft-Tissue Causes | Arthroscopic Bursectomy
- Crepitus is not always pathological - painless snapping in many people is normal and needs no treatment
- Scapulothoracic articulation glides over ribs 2-7; the superomedial angle is the key trouble spot
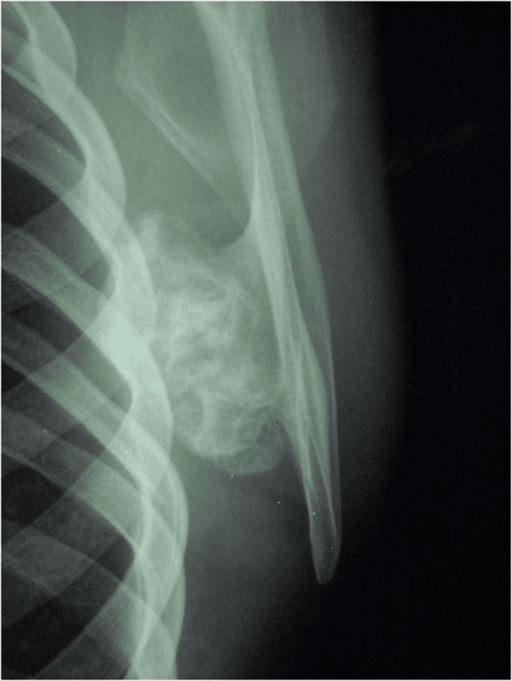
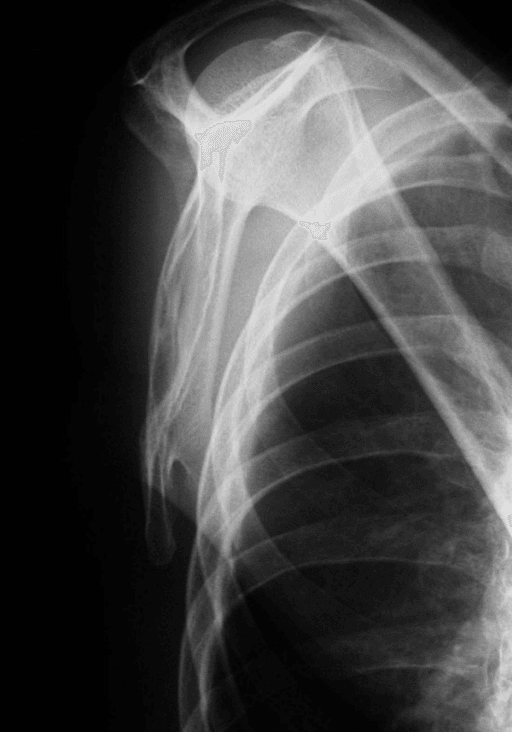
- Osteochondroma is the most common osseous cause - always exclude a bony lesion with CT
- Non-operative care first - therapy, posture, scapular stabilisation succeed in most patients
- Arthroscopic bursectomy with superomedial angle resection is the surgery of choice when conservative care fails
- “Distinguish painful crepitus (a problem) from painless snapping (usually normal)
- “A loud thumping/grinding sound suggests an osseous cause - get a CT
- “The dorsal scapular nerve and artery and the suprascapular nerve are at risk during surgery
- “Avoid resecting too much superomedial bone - risks detaching levator scapulae and serratus anterior
Painless scapular crepitus is common and usually benign - it does not need treatment. The syndrome is defined by pain plus crepitus. Do not investigate or operate on an asymptomatic snap. Examiners want you to recognise this distinction first.
A loud thumping or grinding noise, a palpable hard lump, or onset after trauma points to an osseous cause. The most common is an osteochondroma; others are malunited rib or scapular fractures, a prominent Luschka tubercle, and abnormal scapular curvature. CT is the investigation of choice.
Surgery near the superomedial angle endangers the dorsal scapular nerve and artery (medial border) and the suprascapular nerve (spinoglenoid/scapular notch). Keep bony resection of the superomedial angle limited (commonly cited around 2-3cm) to protect these and avoid stripping levator scapulae and serratus anterior.
A bursal local anaesthetic and steroid injection is both therapeutic and diagnostic - good temporary relief confirms the bursa/scapulothoracic space as the pain source and predicts a better surgical outcome. Poor injection response should make you reconsider the diagnosis before operating.
- Soft-Tissue (Bursal) Cause
- Soft grating, rubbing, snapping
- Osseous Cause
- Loud thumping, clunking, grinding
- Soft-Tissue (Bursal) Cause
- Inflamed/fibrotic bursa, muscle atrophy or fibrosis, overuse
- Osseous Cause
- Osteochondroma, malunited rib/scapula fracture, Luschka tubercle
- Soft-Tissue (Bursal) Cause
- Plain radiographs (often normal)
- Osseous Cause
- Plain films then CT (CT is definitive)
- Soft-Tissue (Bursal) Cause
- Diagnostic and therapeutic into the bursa
- Osseous Cause
- Less useful - lesion is structural
- Soft-Tissue (Bursal) Cause
- Therapy, posture, scapular stabilisation, injection
- Osseous Cause
- Resect the offending bony lesion
- Soft-Tissue (Bursal) Cause
- Arthroscopic bursectomy +/- superomedial angle resection
- Osseous Cause
- Excision of osteochondroma / bony prominence
- Soft-Tissue (Bursal) Cause
- Good relief, low recurrence
- Osseous Cause
- Excellent once mechanical block removed
Overview
Snapping scapula syndrome describes painful crepitus of the scapulothoracic articulation - the soft-tissue junction where the front (costal) surface of the scapula glides over the back of the rib cage. The patient feels and often hears a snapping, grinding or thumping as the shoulder blade moves, and this is accompanied by pain, typically over the superomedial corner of the scapula.
The key conceptual point for the exam is that crepitus alone is not a disease. Painless scapular snapping is found in a large proportion of normal people and requires no treatment. The clinical syndrome only exists when crepitus is symptomatic - that is, painful or functionally limiting.
It is a relatively uncommon and probably underdiagnosed condition. According to PubMed, the largest critical review of the literature found that the evidence base is dominated by small case series and technique papers, with no high-level trials, so much of management is guided by anatomical understanding and expert consensus rather than randomised data.
It is useful to separate two overlapping terms:
- Scapulothoracic bursitis - inflammation or fibrosis of a bursa in the scapulothoracic space, usually producing pain with a softer grating sensation.
- Scapulothoracic crepitus - the audible/palpable grinding, popping or thumping, which when loud is more suggestive of an underlying bony lesion.
Both can coexist, and both fall under the umbrella of snapping scapula syndrome.
Pathophysiology & Anatomy
The Scapulothoracic Articulation
The scapulothoracic "joint" is not a true synovial joint but a musculofascial gliding interface between the concave costal surface of the scapula and the convex posterior chest wall, spanning the levels of ribs 2 to 7. Smooth motion here is essential because scapulothoracic rhythm contributes roughly one-third of total shoulder elevation, positioning the glenoid to optimise glenohumeral function.
Several bursae lie within this space. Anatomical studies describe two consistent major (anatomic) bursae and several inconstant minor (adventitial) bursae:
- Infraserratus bursa - between the serratus anterior and the chest wall.
- Supraserratus bursa - between the subscapularis and the serratus anterior.
- Adventitial bursae - variable, often at the superomedial angle and inferior angle of the scapula; these develop in response to friction and are frequently the symptomatic ones.
The superomedial angle is the single most important location, because it is where the levator scapulae inserts, where adventitial bursae commonly form, and where bony abnormalities most often cause mechanical catching.
How Symptoms Arise
The space between scapula and ribs is normally cushioned by muscle (subscapularis and serratus anterior) and the bursae. Pathology develops when this cushioning fails or when the surfaces no longer glide smoothly:
- Reduced soft-tissue cushioning - muscle atrophy or fibrosis (for example after disuse, denervation or trauma) brings bone closer to bone.
- Bursal inflammation or fibrosis - repetitive overhead activity inflames a bursa, which then thickens and becomes painful and noisy.
- A mechanical block - an osseous lesion (most commonly an osteochondroma), a malunited rib or scapular fracture, a prominent Luschka tubercle (a bony prominence at the superomedial angle), or an abnormally curved/hooked scapula physically obstructs gliding.
- Altered scapular mechanics - scapular dyskinesis, postural rounding (thoracic kyphosis) and weakness of the scapular stabilisers change the contact pressures and provoke symptoms.
Classification
There is no single universally accepted formal classification. The clinically and surgically useful way to organise causes - and the way examiners expect you to think - is by whether the cause is soft-tissue or osseous, because this directs the treatment.
Scapulothoracic bursitis, muscle atrophy or fibrosis, and overuse changes. The noise is usually a softer rubbing or grating sensation. Treatment is therapy and injection first, with arthroscopic bursectomy if refractory.
A complementary descriptive approach grades severity by the character of the noise: a soft rubbing/grating sensation is usually bursal, whereas a loud thumping, clunking or grinding is more typical of an osseous cause and should always prompt cross-sectional imaging.
Clinical Presentation
History
- Symptomatic crepitus - snapping, grinding, popping or thumping with shoulder/scapular movement, particularly overhead activity.
- Pain - typically over the superomedial (and sometimes inferior) angle of the scapula; this is the feature that defines the syndrome.
- Triggers - repetitive overhead work or sport (throwers, swimmers, painters, manual and military load-bearing tasks). According to PubMed, the condition has been highlighted in military populations because of heavy upper-limb load-bearing.
- Onset after trauma - raises suspicion of a malunited rib/scapular fracture.
Examination
- Reproduce the crepitus - palpate over the superomedial angle while the patient circumducts the arm; feel and listen for the snap and localise tenderness.
- Assess scapular motion and dyskinesis - look for winging, asymmetry of scapular rhythm and posture (thoracic kyphosis, rounded shoulders).
- Look and feel for a mass - a discrete hard lump suggests an osteochondroma or other bony lesion.
- Examine the whole shoulder and cervical spine - to exclude glenohumeral and referred causes of pain.
The diagnostic-and-therapeutic injection doubles as a clinical test: if infiltrating local anaesthetic into the scapulothoracic bursa abolishes the pain, the bursa is confirmed as the source and the patient is likely to respond to bursectomy. A poor response should make you reconsider the diagnosis.
Investigations
The diagnosis is primarily clinical, but imaging is used to exclude an osseous cause and plan treatment.
- Role
- First-line; AP, lateral (Y) and tangential scapular views
- Key Point
- May show osteochondroma or malunion but commonly normal; costal-surface lesions are easily missed
- Role
- Investigation of choice for bony causes
- Key Point
- Best defines osteochondroma, scapular shape, Luschka tubercle and malunion for surgical planning
- Role
- Assesses the bursa and soft tissues
- Key Point
- Shows bursal fluid/thickening and excludes soft-tissue tumour; complements CT
- Role
- Dynamic assessment and injection guidance
- Key Point
- Can image the bursa in real time and guide accurate bursal injection
- Role
- Confirms pain source
- Key Point
- Relief after bursal local anaesthetic confirms the diagnosis and predicts surgical success
A loud mechanical noise, a palpable hard mass, or symptoms after trauma should never be dismissed as simple bursitis. Obtain a CT to exclude an osteochondroma, malunited fracture or other bony prominence - missing one means non-operative treatment and even bursectomy will fail.


Differential Diagnosis of Periscapular Pain and Snapping
The examination section says to exclude cervical, glenohumeral and referred causes — here is the differential the examiner expects for a painful or "snapping" scapula.
- Scapular winging (the key mimicking mechanical scapular disorder) — long thoracic nerve / serratus anterior palsy (medial winging) or spinal accessory nerve / trapezius palsy (lateral winging); confirm with a wall push-up (developed in the scapular-winging topic).
- Cervical spine — C5-C6 radiculopathy and facet pathology refer pain to the medial scapular border (dorsal scapular pain); always examine the neck and upper-limb neurology.
- Glenohumeral / subacromial referral — rotator cuff disease, subacromial impingement and glenohumeral instability can produce periscapular pain and an audible clunk.
- Other structural scapular/rib lesions — a scapular or rib tumour (osteochondroma the commonest), a rib or scapular stress or malunited fracture, and elastofibroma dorsi (a soft-tissue mass at the inferomedial scapula that itself can cause snapping).
- Myofascial / postural — periscapular myofascial trigger points and scapular dyskinesis from thoracic kyphosis (developed in the scapular-dyskinesis topic).
Before labelling a painful scapula "snapping scapula syndrome", exclude the mimics: scapular winging (long thoracic or spinal accessory palsy), cervical radiculopathy (C5-C6), referred glenohumeral/subacromial pain, and a structural lesion such as an osteochondroma, a rib/scapular fracture or an elastofibroma dorsi. The wall push-up, a neck and neurological examination, and cross-sectional imaging sort these out.
Management
The cardinal principle is non-operative treatment first for soft-tissue causes, reserving surgery for refractory cases, while osseous causes are treated by resecting the lesion.
- 1
Confirm it is symptomatic
Painful crepitus, not incidental painless snapping. Reassure and discharge if asymptomatic.
- 2
Exclude an osseous cause
Examine for a mass; obtain plain films and CT if any suspicion of a bony lesion or after trauma.
- 3
Treat osseous lesions structurally
Osteochondroma, malunion or Luschka tubercle - plan resection of the offending bony lesion.
- 4
Non-operative care for soft-tissue causes
Activity modification, NSAIDs, scapular stabilisation and posture rehabilitation for 3-6 months.
- 5
Diagnostic/therapeutic bursal injection
Local anaesthetic plus steroid into the bursa - confirms the source and may give lasting relief.
- 6
Surgery if conservative care fails
Arthroscopic bursectomy +/- superomedial angle resection after at least 6 months of failed non-operative treatment.
Non-Operative Management (first line)
- Activity modification and NSAIDs for symptom control.
- Structured physiotherapy - the cornerstone - focused on scapular stabilisation, periscapular strengthening, postural correction and addressing scapular dyskinesis.
- Bursal injection of local anaesthetic and corticosteroid - therapeutic and diagnostic. According to PubMed reviews, non-operative care succeeds in a high proportion of patients (commonly quoted as up to around 80%).
Operative Management
Surgery is indicated for symptomatic patients who fail at least 6 months of compliant non-operative treatment, or up front when a discrete bony lesion is the cause.
The preferred approach for refractory soft-tissue disease. The patient is positioned prone with the arm behind the back (the "chicken-wing" position) to lift the medial border of the scapula off the chest wall. Portals are placed medial to the medial border (typically about 3cm medial, at and below the level of the scapular spine), staying medial to avoid the suprascapular nerve laterally and working in the safe interval to protect the dorsal scapular neurovascular bundle. The inflamed bursa is debrided. Advantages over open surgery are less morbidity, better cosmesis and earlier return to activity.
Negative prognostic factors for surgery reported in the literature include older age, longer duration of symptoms and lower preoperative psychological scores - so careful patient selection (including a good response to diagnostic injection) matters as much as technique.
Scapular Osteochondroma: When to Worry About Malignant Transformation
Osteochondroma is the commonest osseous cause of snapping scapula, and a viva follow-up asks what would raise concern for malignant change — here are the red flags.
- Why the scapula matters. Osteochondromas are common and usually benign, but transformation to a secondary chondrosarcoma is more likely in flat/axial bones (scapula, pelvis, ribs) than in the long bones, and the risk is higher in multiple hereditary exostoses (MHE) — so a scapular lesion warrants particular attention.
- Red flags for transformation:
- A thick cartilage cap — greater than about 1.5-2cm in an adult on MRI/CT is the key alarm feature.
- Growth of the lesion after skeletal maturity.
- New or increasing pain not explained by mechanical snapping.
- Indistinct margins, a soft-tissue mass, or scattered/irregular calcification on cross-sectional imaging.
- What to do. Image with MRI (best for the cartilage cap) plus CT; if any red flag is present, treat as a possible low-grade chondrosarcoma and refer to a sarcoma unit rather than performing a simple shave excision.
- Excision principle. When excising a benign scapular osteochondroma, remove the entire cartilage cap and overlying perichondrium to prevent local recurrence (general osteochondroma management is developed in the osteochondroma topic).
Q: When excising a scapular osteochondroma for snapping scapula, what would make you worried about malignant transformation? A: A cartilage cap thicker than about 1.5-2cm in an adult (the key sign), growth after skeletal maturity, new/increasing pain, or indistinct margins/soft-tissue mass on MRI. Flat-bone (scapula/pelvis) location and multiple hereditary exostoses raise the baseline risk — investigate with MRI+CT and refer to a sarcoma unit rather than shaving it off.
Complications
Dorsal scapular nerve and artery (medial border), suprascapular nerve (scapular/spinoglenoid notch) and the spinal accessory nerve (trapezius) are all at risk. Careful portal placement and limited, subperiosteal resection protect them.
The chest wall lies immediately deep to the working space. Staying subperiosteal on the costal surface and controlling fluid pressure reduces the risk of pleural breach.
A meaningful minority continue to have pain after surgery. According to PubMed, many patients report ongoing shoulder disability even after operation, and a small number need revision - reflecting how often the precise pain source is uncertain.
Over-resection of the superomedial angle can detach the levator scapulae and serratus anterior, producing winging and a destabilised scapula. Keep the bony resection limited.
Clinical Relevance
Snapping scapula syndrome is a favourite viva topic because it tests anatomical reasoning rather than memorised algorithms. The examiner wants to see that you:
- Separate the benign from the pathological - painless crepitus needs no treatment.
- Reason from the scapulothoracic anatomy - ribs 2-7, the bursae, the superomedial angle and the surrounding neurovascular structures.
- Use imaging logically - CT to exclude and characterise an osseous cause.
- Sequence treatment correctly - non-operative care and a diagnostic injection before arthroscopic bursectomy with superomedial angle resection, and lesion excision for bony causes.
- Respect the dangers of surgery - the nerves at risk and the consequences of over-resection.
Guidelines, Registries & Global Practice
There are no formal national guidelines or arthroplasty-registry data for snapping scapula syndrome - it is an uncommon condition managed on the basis of small case series, technique papers and expert consensus. The points below summarise the consistent themes from the global literature.
- Consensus Position
- Treat only painful crepitus; painless snapping is usually normal
- Evidence Strength
- Strong consensus
- Consensus Position
- Non-operative care (scapular stabilisation, posture, injection) for at least 6 months
- Evidence Strength
- Consensus, up to ~80% success quoted
- Consensus Position
- CT is the investigation of choice to exclude/characterise osseous lesions
- Evidence Strength
- Strong consensus
- Consensus Position
- Arthroscopic bursectomy +/- partial (superomedial angle) scapulectomy
- Evidence Strength
- Low-level (Level IV) evidence, consistent results
- Consensus Position
- Excise the offending lesion (e.g. osteochondroma)
- Evidence Strength
- Case-series consensus
- Consensus Position
- No randomised trials exist; all recommendations are low-level
- Evidence Strength
- Acknowledged limitation
Global practice variation: the condition features in military and heavy-labour populations worldwide because of repetitive upper-limb load-bearing. Open surgery remains an option where arthroscopic scapulothoracic expertise or equipment is limited, but the international trend - reported from North American, European, Brazilian and Asian series - favours the arthroscopic approach for its lower morbidity, better cosmesis and earlier return to activity.
Memory Aids
SNAPSNAP - Causes of Snapping Scapula
Hook:If the scapula goes SNAP, think soft-tissue first, then bone.
SAFESAFE - Structures to Protect During Surgery
Hook:Stay SAFE: keep portals medial, resection limited, dissection subperiosteal.
CTCT FIRST - Working Up Loud or Lumpy Snapping
Hook:Loud thump or a lump? Get a CT FIRST before you label it bursitis.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 26-year-old competitive swimmer presents with 8 months of pain over the upper inner border of the right shoulder blade, with a grating sensation when she reaches overhead. She can demonstrate a soft snapping by circumducting the arm. There is tenderness over the superomedial angle of the scapula and no palpable mass. Plain radiographs are normal.”
“An 18-year-old man has a loud thumping snap from the left shoulder blade for two years and notices a hard lump under the inner border. There is a firm fixed mass at the medial scapula. He has no neurological symptoms.”
“A 40-year-old painter has had painful scapulothoracic crepitus for over a year. He has completed nine months of supervised physiotherapy and had two bursal injections that each gave several weeks of complete relief. CT shows no bony lesion. He wants definitive treatment. How will you proceed?”
Definition & Anatomy
- Painful crepitus of the scapulothoracic articulation (painless snapping is usually normal)
- Scapula glides over ribs 2-7; superomedial angle is the key trouble spot
- Major bursae: infraserratus and supraserratus; adventitial bursae at the angles
- Scapulothoracic rhythm contributes ~1/3 of shoulder elevation
Causes (SNAP)
- Soft-tissue: bursitis, muscle atrophy/fibrosis, overuse
- Osteochondroma - most common osseous cause
- Anatomy: Luschka tubercle, abnormal scapular curvature
- Prior fracture malunion (rib or scapula)
Investigations
- Plain films first (often normal; costal lesions easily missed)
- CT with 3D reconstruction = investigation of choice for bony causes
- MRI for bursa/soft tissue; ultrasound for dynamic assessment and injection
- Diagnostic bursal injection confirms the pain source
Management
- Non-operative first: scapular stabilisation, posture, NSAIDs, injection (up to ~80% success)
- At least 6 months conservative trial before surgery
- Surgery of choice: arthroscopic bursectomy +/- superomedial angle resection
- Osseous cause: excise the lesion (e.g. osteochondroma)
Surgical Safety
- At risk: dorsal scapular nerve/artery, suprascapular nerve, spinal accessory nerve
- Stay subperiosteal to avoid pneumothorax
- Limit superomedial resection (~2-3cm) to protect levator scapulae/serratus anterior
- Good injection response predicts better surgical outcome
Evidence Base
Critical Review of the Evidence Base (Landmark)
- 81 relevant articles, all low-level evidence (no RCTs)
- Likely an underdiagnosed condition
- Bursectomy +/- partial scapulectomy is the most effective surgery
- Continued disability after surgery is common
Arthroscopic Bursectomy - Mid-Term Outcomes
- 20 patients / 24 scapulae, mean 44-month follow-up
- VAS pain fell from 4.95 to 2.27 (significant)
- Mean ASES 79, subjective shoulder value 83
- Low recurrence; 2 patients required revision
Arthroscopic Debridement + Medial Scapulectomy with MRI Bony Parameters
- 8 patients, minimum 2-year follow-up, no complications
- Significant improvement in OSS, UCLA, Constant and VAS
- 5 of 8 needed additional medial scapulectomy
- Introduced MRI bony parameters for surgical planning
Predictors of Outcome After Arthroscopic Treatment
- Response to diagnostic injection guides patient selection
- Bursectomy + partial scapulectomy gives the best outcomes
- Negative predictors: older age, longer symptom duration
- Lower preoperative psychological score predicts worse results