Coxa Saltans | Internal vs External | Iliopsoas vs ITB
- External Snapping (ITB): Visible snap over the lateral hip. 'I saw it pop out'.
- Internal Snapping (Iliopsoas): Deep audible snap/clunk with hip extension from flexion/abduction.
- Intra-articular: True mechanical symptoms (locking/catching) - usually painful.
- Voluntary: Many patients can reproduce the snap voluntarily.
- Ober's Test: Assessing ITB tightness is key for external type.
- “Ask the patient to reproduce the snap!
- “Psoas snap: Flexion + Abduction + External Rotation to Extension
- “ITB snap: Flexion/Extension in lateral decubitus
- “Painful vs Painless: Painless snapping requires NO treatment.
Rule out Labral Tears. Intra-articular pathology presents with sharp groin pain and mechanical locking/catching. Snapping is usually a clunk rather than a click. MRI Arthrogram is the gold standard discriminator.
Voluntary Snappers. Some patients (often adolescents) habitually snap their hip as a tic. Surgical treatment in painless voluntary snappers has unpredictable (often poor) outcomes. Avoid operating on the 'party trick'.
- External (ITB)
- Sometimes
- Internal (Iliopsoas)
- Often Loud 'Clunk'
- Intra-articular
- Click/Catch
- External (ITB)
- Visible 'Jump' of ITB
- Internal (Iliopsoas)
- Not visible
- Intra-articular
- Not visible
- External (ITB)
- Lateral (Greater Troch)
- Internal (Iliopsoas)
- Anterior (Groin)
- Intra-articular
- Deep Groin/C-sign
- External (ITB)
- Walking/Running
- Internal (Iliopsoas)
- Extension from Frog-leg
- Intra-articular
- Rotation/Pivoting
IIESnapping Hip Types
Hook:Two I's inside, One E outside.
FABER-EInternal Snapping Reproduction
Hook:From FABER into Extension snaps the Psoas.
Overview and Epidemiology
Snapping Hip Syndrome (Coxa Saltans) describes a palpable or audible snap occurring around the hip joint during movement. It is classified by the anatomical structure causing the snap.
Epidemiology
- Demographics: Most common in females (wider pelvis increases ITB angle) and adolescents/young adults.
- Athletes: Dancers (Ballet), Gymnasts, Runners.
- Psychosocial: Habitual snapping can be associated with anxiety/compulsion in adolescents.
Risk Factors and Associations
Anatomical Predisposition:
- Coxa vara (prominent greater trochanter increases ITB friction)
- Increased femoral anteversion
- Leg length discrepancy (longer leg has tighter ITB)
- Narrow bi-iliac width (common in dancers)
Activity-Related Factors:
- Sports involving repetitive hip flexion/extension (cycling, running)
- Dance (especially ballet with extreme hip positions)
- Martial arts (high kicks)
- Soccer (kicking sports)
Biomechanical Factors:
- Gluteal weakness (poor hip control)
- Core instability
- Tight hip flexors
- ITB tightness from overuse
Pathophysiology and Mechanisms
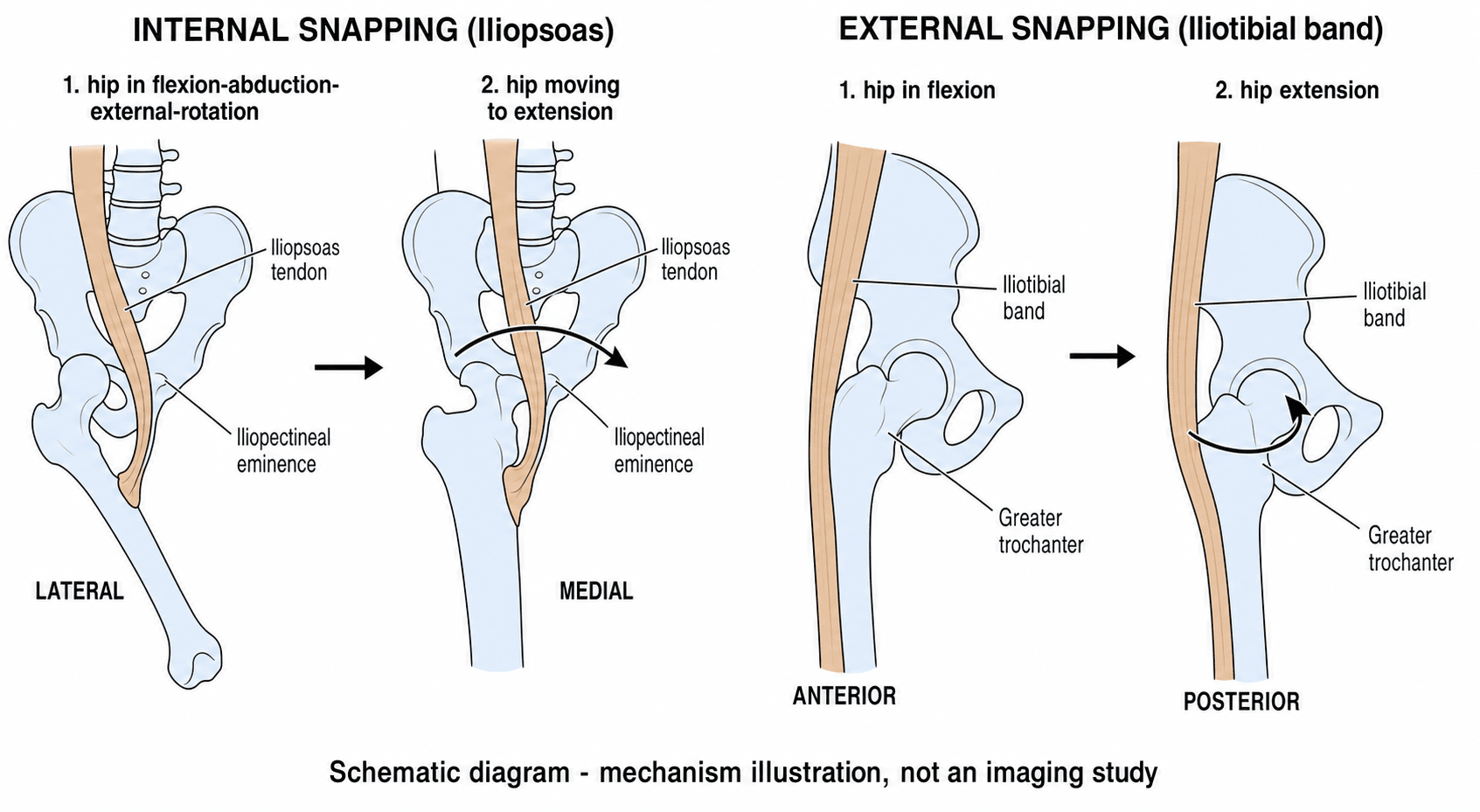
Internal Snapping
Structure: Iliopsoas Tendon. Mechanism: The tendon snaps over the Iliopectineal Eminence or the Femoral Head. Motion: Occurs when the hip moves from Flexion/Abduction/External Rotation (FABER) into Extension/Adduction/Internal Rotation. The tendon flips from lateral to medial across the eminence. Bursa: Often associated with Iliopsoas bursitis (pain).
Classification Systems
Anatomical Classification
Based on the location of the snap relative to the joint:
- Extra-articular Lateral (External): Iliotibial Band or Gluteus Maximus.
- Extra-articular Anterior (Internal): Iliopsoas Tendon.
- Intra-articular: Labrum, loose bodies, cartilage flaps.
This helps guide anatomical target.
Clinical Assessment
History
- Describe the sound: "Pop", "Click", "Clunk".
- Location:
- Lateral corresponds to External (Patient points to trochanter).
- Groin corresponds to Internal or Intra-articular.
- Pain: Is it painful? Painless snapping is physiologic and needs no treatment.
- Voluntary: Can you do it right now? (Demonstration is diagnostic).
Physical Examination
External Snapping:
- Ober's Test: Assess ITB tightness.
- Reproduction: Patient side-lying. Passive flexion/extension of hip while compressing ITB against greater trochanter. Palpable "jump".
Internal Snapping:
- Thomas Test: Assess Psoas tightness (fixed flexion deformity).
- Dynamic Test: Patient supine. Flex, Abduct, Externally Rotated hip actively extended. Palpable "clunk" anteriorly.
Intra-articular:
- FADIR Test: Impingement test / Labral loading.
- Scour Test: Grinding femoral head.
Investigations
Radiographs
- Usually Normal.
- Check for: Cam/Pincer FAI, DDH, Dysplasia (Intra-articular associations).
Dynamic Ultrasound
- Diagnostic of choice for Snapping.
- Real-time visualisation of the tendon snapping over bone.
- Can see bursitis.
- Can perform diagnostic injection.
MRI / MRA
- Role: Ruling out Intra-articular pathology (Labral tear).
- Internal: May show Iliopsoas bursitis.
- External: Gluteal tendinopathy / ITB thickening.
MRI Arthrography is gold standard for Labral tears.
Differential Diagnosis
The central exam skill is separating benign extra-articular snapping from intra-articular and other mimics of the painful, noisy hip.
- Location & Character
- Anterior groin, audible deep clunk
- Key Discriminator
- Reproduced extending from FABER; tendon flips over eminence
- Confirm With
- Dynamic ultrasound
- Location & Character
- Lateral, visible jump over trochanter
- Key Discriminator
- Visible/palpable jump; positive Ober
- Confirm With
- Clinical + dynamic US
- Location & Character
- Deep groin, C-sign, locking/catching
- Key Discriminator
- Mechanical locking, positive FADIR, cam/pincer on XR
- Confirm With
- MR arthrogram
- Location & Character
- Lateral, point tenderness, night pain
- Key Discriminator
- Tenderness over trochanter, abductor weakness, no true snap
- Confirm With
- MRI (gluteal tendinopathy)
- Location & Character
- Intermittent true locking
- Key Discriminator
- Episodic mechanical block, normal between episodes
- Confirm With
- CT / MRI / arthroscopy
- Location & Character
- Groin, activity-related, no snap
- Key Discriminator
- Pain with hop test, risk factors (RED-S)
- Confirm With
- MRI
- Location & Character
- Lower groin, no snap
- Key Discriminator
- Pain on resisted adduction / sit-up
- Confirm With
- MRI / clinical
Iliopsoas-Impingement Labral Lesion (Not the Same as FAI)
The evidence base and the controversies section both refer to a labral tear caused by iliopsoas impingement and to coexisting intra-articular pathology in most internal snappers, but the topic never explains this distinct entity. It is a high-yield discriminator because it is the one anterior labral tear where the tendon - not the bone - is the cause, so the treatment differs from FAI.
The mechanism: a tight or inflamed iliopsoas tendon lies directly in front of the anterior capsulolabral complex. With repetitive flexion-extension the tendon abuts and inflames the labrum directly at the level where it crosses it - the anterior labrum, around the 3 o'clock position (right hip) - producing a focal, localised "kissing" labral tear with overlying synovitis. This is distinct from a femoroacetabular impingement (FAI) tear, where a bony cam or pincer lesion drives the labral damage.
How to tell it apart from an FAI labral tear:
- Iliopsoas-impingement lesion
- Direct tendon abutment on the labrum
- FAI labral tear
- Bony cam/pincer abnormal contact
- Iliopsoas-impingement lesion
- Focal, directly anterior (~3 o'clock), isolated
- FAI labral tear
- Anterosuperior, often with chondral damage
- Iliopsoas-impingement lesion
- Normal alpha angle, no pincer over-coverage
- FAI labral tear
- Cam (raised alpha angle) and/or pincer present
- Iliopsoas-impingement lesion
- Localised synovitis/bruising deep to the psoas tendon
- FAI labral tear
- Labrochondral separation at the cam/pincer zone
- Iliopsoas-impingement lesion
- Address the iliopsoas (release at labral level) +/- labral debridement
- FAI labral tear
- Correct the bone (osteoplasty/rim trim) + repair labrum
Why it matters for management: this is the exception to the rule that the topic states elsewhere ("an isolated psoas release is inappropriate for intra-articular pathology"). When the labral lesion is genuinely caused by iliopsoas impingement - a focal anterior tear with normal bony morphology and an inflamed tendon - addressing the iliopsoas at the labral level is a legitimate part of treatment, alongside conservative care of the labral lesion. The danger is the reverse error: ascribing a labral tear to the psoas when there is an unrecognised cam/pincer behind it, doing a psoas release, and leaving the FAI undertreated. General labral-tear classification and repair technique are covered in the dedicated hip-labral-tear topic; here the point is the iliopsoas-specific lesion and how not to confuse it with FAI.
There are three reasons to release an iliopsoas tendon: internal snapping, iliopsoas tendinopathy after THA, and a labral tear caused by iliopsoas impingement. The labral one is a focal, directly anterior (~3 o'clock) "kissing" tear with normal bony morphology - if there is a cam or pincer behind it, that is FAI and you must treat the bone, not just the tendon.
Iliopsoas Tendinopathy After Total Hip Arthroplasty
The registry note flags iliopsoas impingement/tendinopathy after THA as a recognised cause of post-replacement groin pain, and the evidence base lists it as the third indication for iliopsoas release, but the entity itself is never developed. It is a classic "persistent groin pain after a well-fixed, non-infected THA" exam scenario.
the iliopsoas tendon runs immediately in front of the anterior acetabular rim. If the acetabular component is oversized, prominent, under-recessed (sitting proud of the anterior wall), or excessively retroverted/uncovered anteriorly - or a prominent screw or cement extrudes - the tendon catches on the hard metal edge during active hip flexion. The result is anterior groin pain (often with a clunk) on tasks that load active flexion: rising from a low chair, climbing stairs, getting out of a car, the straight-leg raise.
- Always exclude infection and loosening before labelling pain as iliopsoas - inflammatory markers, plain films for lucency/migration, and aspiration if there is any doubt.
- Examination: pain on resisted active hip flexion / resisted straight-leg raise, reproduced and localised anteriorly.
- Cross-sectional imaging: CT measures anterior acetabular-component overhang/prominence relative to the bony rim (and assesses version); MRI/ultrasound shows the inflamed tendon.
- Image-guided diagnostic injection: local anaesthetic into the iliopsoas tendon sheath - temporary relief confirms the diagnosis and is the key discriminator.
- Indication
- First line, all cases
- Action
- Activity modification, physiotherapy, NSAIDs
- Indication
- Diagnostic + therapeutic
- Action
- Local anaesthetic +/- steroid into the tendon sheath
- Indication
- Refractory pain, cup only mildly prominent and otherwise well-positioned
- Action
- Arthroscopic/endoscopic or open release
- Indication
- Cup grossly oversized, malpositioned, or retroverted
- Action
- Revise the component - treat the underlying cause
The decision turns on whether the cup is the problem: a well-positioned cup that is only slightly prominent can be managed with tendon release, but a grossly oversized or malpositioned component should be revised rather than chasing the tendon. Detailed acetabular revision technique is covered in the revision-THA topic; here the point is recognising iliopsoas tendinopathy as a treatable, component-related cause of post-THA groin pain.
Persistent anterior groin pain after a well-fixed, non-infected THA, worse on stairs and rising from a chair, with a positive resisted straight-leg raise - think iliopsoas impingement on a prominent anterior cup. Confirm with an image-guided local-anaesthetic injection; treat a mildly prominent well-positioned cup with tendon release, but revise a grossly oversized or malpositioned one.
Management Algorithm
Treatment Ladder
If painless: "It's noisy but normal." No treatment. Education.
Stretching (ITB/Psoas). Core strengthening. Gluteal strengthening. Activity modification.
Ultrasound-guided steroid injection into Iliopsoas bursa or Trochanteric bursa. Diagnostic + Therapeutic.
Only for refractory PAINFUL snapping (rare). Technique depends on type.
SIREManagement Hierarchy
Hook:SIRE: The King of treatments.
Surgical Technique
Arthroscopic Psoas Fractional Lengthening
Goal: Lengthen the tendon without complete release (preserve power). Technique:
- Hip Arthroscopy / Endoscopy.
- Transcapsular approach (from central compartment) or Endoscopic (from peripheral compartment at Lesser Trochanter).
- Fractional Lengthening: Cut the tendinous portion only (at the musculotendinous junction), preserving the muscular sleeve.
- Reduces tension and stops snapping while retaining flexion power.
- Risk: Hip flexion weakness and iliopsoas atrophy.
Preserve the tendon to preserve power.
Complications
- Risk
- Common (Internal)
- Note
- Radiological atrophy near-universal after tenotomy; early weakness usually compensates
- Risk
- ~5% arthroscopic / over 20% open
- Note
- Insufficient release, re-scarring; lower with arthroscopic technique
- Risk
- Rare
- Note
- Usually asymptomatic
- Risk
- Rare
- Note
- LFCN (external/anterior portals); genital paraesthesia with central-compartment psoas tenotomy
Detailed Rehabilitation
Specific Exercises by Phase
Phase 1: Mobilization & Activation (Weeks 0-4)
- Glute Bridges: 3 sets of 15. Focus on squeeze.
- Clamshells: 3 sets of 15. Banded resistance.
- Psoas Stretch: Kneeling lunge. Hold 30s.
- ITB Foam Roll: Patient guided self-myofascial release.
Phase 2: Strengthening (Weeks 4-8)
- Single Leg Deadlift (RDL): Excellent for posterior chain.
- Lateral Band Walks: Gluteus Medius recruitment.
- Bulgarian Split Squat: Eccentric Psoas control.
- Monster Walks: Forward/Backward with band.
Phase 3: Return to Sport (Weeks 8+)
- Plyometrics: Box jumps (landing mechanics).
- Cutting Drills: 45 degree cuts.
- Sport Specific: Kicking (soccer) or Pointe work (ballet).
Note: For Psoas release patients, avoid active hip flexion against resistance for first 4 weeks.
Postoperative Care
Rehabilitation Protocol
- Weight Bearing: WBAT with crutches for 2 weeks (Psoas release).
- ROM: Unlimited ROM immediately to prevent scarring (Use Stationary Bike).
- Strengthening:
- Week 1-4: Isometrics.
- Week 4-8: Concentric loading.
- Week 8+: Sport specific.
Return to Sport:
- External: 6-8 weeks.
- Internal: 12-16 weeks (due to weakness).
Outcomes and Prognosis
Prognostic Factors
- Pain: A painful snap that fails conservative care is the key surgical indication. Painless snapping (a large proportion of cases on ultrasound) is benign and does poorly with surgery.
- Weakness/atrophy after psoas surgery: Radiological iliopsoas atrophy is near-universal after arthroscopic tenotomy and early flexion weakness is common; most patients recover functional strength and return to sport.
- Recurrence: Arthroscopic release recurs far less often than open release (around 5% vs over 20% in pooled data).
Overall: Good outcomes in properly selected patients (refractory pain, failed a structured trial of physiotherapy).
Outcomes by Type (evidence-anchored)
External Snapping (ITB / gluteus maximus):
- The majority resolve with conservative management and surgery is rarely required.
- ITB Z-plasty for refractory cases resolves snapping in close to 100% of carefully selected hips, with durable results reported out to ~7 years.
- Endoscopic release offers lower morbidity than open Z-plasty for suitable patients.
Internal Snapping (Iliopsoas):
- Arthroscopic tenotomy resolves snapping in roughly 93% of hips.
- Iliopsoas atrophy is seen radiologically in most patients; early hip-flexion weakness usually compensates over time but may matter to elite athletes/dancers.
- Coexisting intra-articular pathology is found in the majority of internal snappers at arthroscopy.
Intra-articular:
- Outcomes depend on the underlying lesion (labral tear, loose body, FAI).
- Treat the primary pathology (e.g. labral repair, cam/pincer correction); an isolated psoas release is inappropriate and may worsen instability.
Guidelines, Registries & Global Practice
Global Epidemiology
- Snapping hip is reported in 5-10% of the general population in some series; many are painless and physiologic.
- Markedly over-represented in classical ballet (cohorts report internal snapping in up to ~90% of dancers, the large majority painless), gymnasts, runners, and football/soccer players.
- Female predominance is consistent across populations (over 80% female in surgical series), partly reflecting pelvic geometry and the dance/gymnastics population.
Society Guidance, Side by Side
No condition-specific international guideline exists for snapping hip; practice is consensus- and registry-poor. Relevant overlapping guidance:
- Relevant Position
- Conservative first-line; surgery only for refractory painful snapping
- Practical Implication
- Physiotherapy + activity modification before any release
- Relevant Position
- Image and treat the painful hip; rule out FAI/labral pathology before extra-articular surgery
- Practical Implication
- MR arthrogram for suspected intra-articular cause
- Relevant Position
- Painless snapping in dancers needs reassurance, not intervention
- Practical Implication
- Avoid operating on the 'party trick'
- Relevant Position
- Where surgery indicated, arthroscopic/endoscopic over open
- Practical Implication
- Lower recurrence and complication rates
Registry Note
Snapping hip itself is not tracked in arthroplasty registries (NJR, AJRR, AOANJRR, SHAR), but iliopsoas impingement/tendinopathy after THA is a recognised cause of post-replacement groin pain - check anterior acetabular component prominence and consider release or cup revision in refractory cases.
High- vs Limited-Resource Practice
- Well-resourced settings: Dynamic ultrasound and MR arthrogram readily available; image-guided injection and hip arthroscopy/endoscopy offered for refractory cases.
- Limited-resource settings: Diagnosis is clinical (history of reproducible snap + Ober/Thomas tests); management is reassurance, structured physiotherapy, and selective landmark-guided injection. Open Z-plasty remains a valid, low-technology option where endoscopy is unavailable.
Controversies & Areas of Uncertainty
Tenotomy at the level of the labrum/central compartment is the most-used site (over 90% in pooled series), but transcapsular release from the peripheral compartment has been associated with fewer cases of genital paraesthesia and better short-term scores in one RCT. The optimal location and technique remain undefined.
Both abolish snapping. Iliopsoas atrophy is near-universal regardless of technique, and high-quality comparative data on whether partial/fractional release truly preserves more strength than complete tenotomy are lacking.
Radiological atrophy is common, yet most patients recover functional strength and return to sport. Whether residual weakness is clinically meaningful for elite athletes and dancers (grand battement power) is debated and under-studied.
Coexisting intra-articular pathology (synovitis, chondropathy, labral lesions) is found in most internal snappers. Whether to add iliopsoas release when correcting FAI/labral pathology - versus treating the joint alone - is unresolved; over-release risks anterior microinstability.
MCQ Practice Points
Q: What structure does the psoas tendon snap over? A: Iliopectineal Eminence (pelvic brim) or the Femoral Head.
Q: What structure does the ITB snap over? A: Greater Trochanter. Specifically the posterior third of the ITB.
Q: What is the most common significant complication of psoas release? A: Hip Flexion Weakness. Can be permanent and disabling for athletes.
Q: What is the investigation of choice? A: Dynamic Ultrasound. Allows real-time visualization of the snapping event.
Q: Which demographic is most affected? A: Young Females. Particularly dancers and gymnasts (flexibility + anatomy).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 16-year-old female dancer complains of a loud 'clunk' in her groin when she extends her leg from a high kick. It is occasionally painful. She can reproduce it on demand.”
“A 22-year-old cyclist has lateral hip pain and a visible snap over the trochanter when walking. He has failed foam rolling and stretching. Ober's test is positive.”
“A 30-year-old footballer presents with groin pain and locking. He describes a deep 'clunk'. He has a positive FADIR test. Plain films show a Cam lesion.”
Classification
- Internal: Iliopsoas (Groin clunk)
- External: ITB (Lateral pop)
- Intra-articular: Labrum (Click/Catch)
- Voluntary vs Involuntary
Diagnosis
- Clinical Reproduction is key
- Dynamic Ultrasound = Gold Standard
- MRI to exclude labral tear
- Ober Test for ITB tightness
Management
- Painless = No treatment
- Painful = Physio + Injection
- Surgery = Last resort (Release/Lengthening)
- Risk: Flexion Weakness (Psoas)
Anatomy
- Psoas to Iliopectineal Eminence
- ITB to Greater Trochanter
- Labrum to Acetabular Rim
- Bursa involved in both
Evidence Base
Arthroscopic Iliopsoas Tenotomy - Outcomes & Safety
- Snapping resolved in 93% of hips
- Radiological psoas atrophy is near-universal (92%) but usually clinically tolerated
- Early flexion weakness common; most recover
- High-quality comparative data still lacking
Open vs Arthroscopic Iliopsoas Release
- Arthroscopic release has ~4x lower recurrence than open
- Fewer overall complications than open release
- Three distinct surgical indications recognised
- Effective regardless of indication
Dynamic Ultrasound Diagnosis of Snapping Hip
- Dynamic US localises the cause in over 90% of cases
- Provides real-time tendon-to-symptom correlation
- Iliopsoas was the dominant cause in this series
- A large proportion of snapping hips are painless
ITB Z-Plasty for Refractory External Snapping
- Z-plasty resolved snapping in 100% of hips
- Surgery for external snapping is rarely needed
- Patient selection is critical to results
- Predictable, durable outcomes when indicated
Peripheral vs Central Compartment Tenotomy (RCT)
- Peripheral-compartment release reduced genital paraesthesia
- Better 1-year WOMAC than central approach
- Intra-articular pathology coexists in most internal snappers
- Approach selection affects both outcome and complications
Modified Z-Plasty for Gluteus Maximus Tightness
- Gluteus maximus tightness is a distinct external-snap cause
- Modified Z-plasty gave durable 7-year results
- No abductor weakness or recurrence
- Functional impairment, not just noise, drove surgery