Fatigue vs Insufficiency | High-Risk Sites | RED-S | Imaging Continuum | Load Management
- Fatigue fractures = abnormal stress on normal bone; insufficiency fractures = normal stress on abnormal bone
- Five high-risk sites: femoral neck (tension side), anterior tibial cortex, tarsal navicular, 5th metatarsal base, hallux sesamoid
- MRI is gold standard — X-rays are normal in up to 70% initially
- RED-S (Relative Energy Deficiency in Sport) is the modern term replacing 'female athlete triad' and includes male athletes
- Tension-side femoral neck fractures need urgent fixation — risk of displaced fracture and AVN
- “If X-ray is normal but clinical suspicion is high, get an MRI — do not wait for X-ray changes
- “Tension-side femoral neck stress fracture = ORIF, do not trial non-operative management
- “Anterior tibial 'dreaded black line' = high risk, consider intramedullary nailing
- “RED-S screening is mandatory in any athlete with recurrent stress fractures
High-risk sites are on the tension side of bone or in areas of poor vascularity. They have a high rate of nonunion, delayed union, or progression to complete fracture and require aggressive (often surgical) management. Low-risk sites are on the compression side and usually heal with activity modification.
Superolateral cortex. This is the most dangerous stress fracture in sport. Non-union and displacement risk is high. Urgent internal fixation with cannulated screws is standard. Do NOT trial non-operative management in athletes — a displaced femoral neck fracture in a young adult is catastrophic (AVN, OA).
The anterior mid-tibial cortex is a tension-side location. A visible radiolucent line on lateral X-ray = 'dreaded black line'. Propensity to propagate to complete fracture. In athletes, intramedullary nailing or excision and bone grafting may be required.
Every athlete with a stress fracture needs RED-S screening: dietary intake, menstrual history (females) or testosterone (males), BMI trends, training load, and previous stress fractures. RED-S is the commonest underlying factor in recurrent stress fractures in endurance athletes.
- Site Risk
- Low-risk (posterior-medial tibia) until proven otherwise
- Imaging
- MRI with Fredericson grading
- Management
- Relative rest, graded return over 6-8 weeks if low-grade
- Site Risk
- High-risk: femoral neck until excluded
- Imaging
- Urgent MRI (not X-ray — may be normal)
- Management
- If tension-side: urgent ORIF; if compression-side: NWB + repeat MRI
- Site Risk
- High-risk: tarsal navicular
- Imaging
- CT to confirm fracture line; MRI for marrow oedema
- Management
- NWB cast 6 weeks minimum; ORIF if displaced or nonunion
- Site Risk
- RED-S related — all sites at risk
- Imaging
- MRI of symptomatic site + DEXA scan + blood panel
- Management
- Multidisciplinary: nutrition, endocrinology, psychology, modified training
NAFFSHigh-Risk Stress Fracture Sites
Hook:NAFFS — Not A Friendly Fracture Site! These five locations demand aggressive management.
Overview and Epidemiology
Stress fractures account for up to 20% of all injuries in sports medicine clinics and are the most common overuse injury in military recruits and distance runners. High-risk stress fractures (femoral neck tension side, navicular, anterior tibia, 5th metatarsal base, sesamoid) can progress to complete fracture or nonunion if missed. The diagnosis is clinical first — a high index of suspicion is essential because early X-rays are often normal. Every stress fracture in an athlete warrants RED-S screening.
- Incidence: 5-30% of runners and military recruits
- Most common site: Tibia (posterior-medial cortex, low-risk)
- Female athletes: 2-4 times higher risk than males (RED-S / menstrual dysfunction)
- Military: Up to 5% of recruits during basic training
- Training errors: Rapid increase in volume, intensity, or frequency (greater than 10% per week)
- Low energy availability: Disordered eating, RED-S
- Bone density: Low BMD, osteoporosis, prior stress fracture
- Biomechanical: Leg length discrepancy, foot type, running surface
- Medications: Bisphosphonates (atypical fractures), corticosteroids, aromatase inhibitors
Pathophysiology
Stress fractures result from an imbalance between microdamage accumulation and bone remodelling repair. Normal bone undergoes constant remodelling: osteoclastic resorption creates cavities that osteoblasts fill with new bone. When repetitive loading outpaces repair, microdamage coalesces into a fatigue fracture. If the bone itself is weakened (osteoporosis, RED-S), even normal physiological loads cause insufficiency fractures. The key concept is that stress fractures are a continuum — from bone stress reaction (oedema, no fracture line) to frank cortical fracture.
- Fatigue Fracture
- Abnormal repetitive load on normal bone
- Insufficiency Fracture
- Normal physiological load on weakened bone
- Fatigue Fracture
- Runner, military recruit, dancer, athlete
- Insufficiency Fracture
- Elderly, osteoporotic, bisphosphonate user, rheumatoid arthritis
- Fatigue Fracture
- Normal bone mineral density
- Insufficiency Fracture
- Low BMD, osteomalacia, metabolic bone disease
- Fatigue Fracture
- Load management, relative rest, return to sport
- Insufficiency Fracture
- Treat underlying bone health (vitamin D, bisphosphonate review, DEXA)
- Fatigue Fracture
- Tibia, metatarsals, femoral neck, navicular, fibula
- Insufficiency Fracture
- Vertebral body, sacrum, pubic ramus, femoral neck, calcaneus
Normal cycle: Osteoclast resorption (2-3 weeks) followed by osteoblast formation (3-4 months)
With overuse: Increased resorption outpaces formation
Weeks 1-2: Oedema and microcracks (bone stress reaction)
Weeks 3-4: Microcracks coalesce if loading continues
Weeks 4-8: Cortical fracture line becomes visible
Key point: Removing the load early allows the remodelling cycle to catch up
Compression side: Bone can remodel and heal under compression. Usually low-risk (e.g., inferomedial femoral neck, posterior-medial tibia)
Tension side: Bone fails under tensile stress — fracture propagates rather than heals. High-risk (e.g., superolateral femoral neck, anterior tibial cortex)
Clinical implication: Tension-side fractures need urgent fixation or strict non-weight-bearing; compression-side fractures can often be managed conservatively
Classification and Types
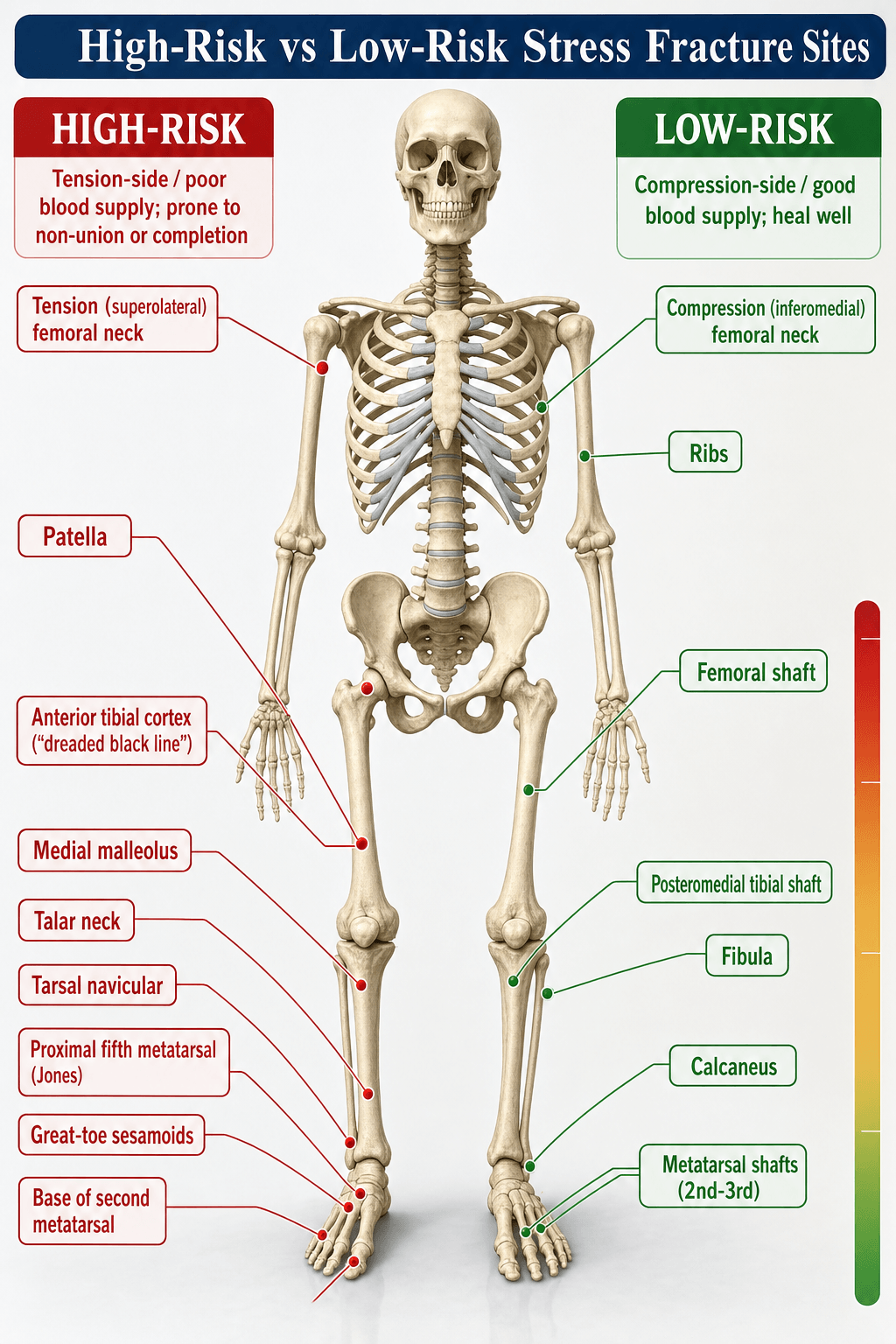
High-Risk vs Low-Risk Stress Fracture Sites
- Site
- Femoral neck
- Side/Location
- Tension (superolateral) side
- First-Line Treatment
- Urgent cannulated screw fixation
- Site
- Anterior tibial cortex
- Side/Location
- Tension (anterior) mid-shaft
- First-Line Treatment
- IM nail or excision + bone graft if refractory
- Site
- Tarsal navicular
- Side/Location
- Central third (watershed)
- First-Line Treatment
- NWB cast 6-12 weeks; ORIF if displaced
- Site
- 5th metatarsal base
- Side/Location
- Jones fracture (proximal diaphysis)
- First-Line Treatment
- Percutaneous screw (athletes) vs NWB cast
- Site
- Hallux sesamoid
- Side/Location
- Medial (tibial) sesamoid
- First-Line Treatment
- NWB + sesamoid pad; excision if refractory
- Site
- Posterior-medial tibia
- Side/Location
- Compression (posteromedial) cortex
- First-Line Treatment
- Relative rest, graded return 6-8 weeks
- Site
- Femoral neck (compression)
- Side/Location
- Inferomedial side
- First-Line Treatment
- NWB until pain-free, then progressive WB
- Site
- 2nd-4th metatarsal shaft
- Side/Location
- Mid-shaft (march fracture)
- First-Line Treatment
- Stiff shoe / walking boot 4-6 weeks
- Site
- Fibula
- Side/Location
- Distal third (compression)
- First-Line Treatment
- Relative rest; occasionally boot for comfort
- Site
- Calcaneus
- Side/Location
- Posterior (compression)
- First-Line Treatment
- Relative rest, progressive weight-bearing
The distinction between high-risk and low-risk sites is the most important classification in exam settings — it directly determines management.
The risk-factor list mentions bisphosphonates, but the atypical femoral fracture is a discrete high-yield entity in its own right - an insufficiency-type stress fracture of the femoral lateral cortex caused by long-term suppression of bone remodelling (prolonged bisphosphonate, and also denosumab, use lets microdamage accumulate).
- ASBMR diagnostic criteria (major - need most of five): fracture in the subtrochanteric-to-supracondylar diaphysis; transverse or short-oblique orientation beginning at the lateral cortex; minimal or no trauma; localised periosteal/endosteal thickening ("beaking" or flaring) of the lateral cortex; non-comminuted or minimally comminuted. Minor features: generalised cortical thickening, prodromal thigh/groin pain, bilaterality, and delayed healing.
- Always image the opposite femur - AFFs are bilateral in a substantial proportion of patients.
- Management:
- Prodromal thigh pain with an incomplete AFF (a lateral-cortex lucent line and beaking, no complete break): stop the bisphosphonate ("drug holiday"), optimise calcium and vitamin D, consider an anabolic agent (teriparatide) to promote healing, and proceed to prophylactic cephalomedullary nailing if pain persists or a lucent line/"dreaded black line" is present.
- Complete AFF: cephalomedullary (intramedullary) nailing.
Exam point: an AFF is a lateral-cortex transverse subtrochanteric/diaphyseal insufficiency stress fracture from long-term bisphosphonate-suppressed remodelling - look for prodromal thigh pain and lateral-cortex beaking, image both femurs, stop the bisphosphonate, and treat with prophylactic or definitive cephalomedullary nailing.
The imaging section name-drops the pars interarticularis, but spondylolysis is the classic stress fracture of the lumbar spine and the commonest structural cause of low back pain in the adolescent athlete - an essential inclusion in any stress-fracture overview.
- Who and where: a fatigue fracture of the pars interarticularis, most often at L5 (then L4), in young athletes doing repetitive lumbar hyperextension and rotation - cricket fast bowlers, gymnasts, dancers, divers and throwers. It may be unilateral or bilateral; bilateral lesions can progress to spondylolisthesis.
- Presentation: activity-related extension low back pain; the single-leg hyperextension (stork) test reproduces the pain.
- Imaging: the oblique radiograph "Scotty dog with a collar" (lucency through the pars) is classic, but MRI is now first-line in the young (no radiation; pars marrow oedema indicates an early, active lesion with healing potential); SPECT/CT or limited CT characterises whether the defect is acute (healable) or chronic/established (terminal).
- Management: activity restriction/relative rest, core and anti-extension physiotherapy, and a period of antilordotic bracing in selected cases. An early oedematous lesion can heal with rest; a chronic established defect usually will not unite but is frequently asymptomatic. Surgical repair or fusion is reserved for refractory pain or a progressive slip - monitor with standing lateral radiographs.
Exam point: spondylolysis is a pars interarticularis stress fracture (usually L5) in the adolescent hyperextension-sport athlete - extension back pain with a positive stork test, diagnosed by MRI (active oedematous lesion = healable), managed with rest, physiotherapy and bracing, and watched for progression to spondylolisthesis.
Clinical Assessment
- Activity profile: Recent increase in training volume, intensity, or frequency
- Pain onset: Gradual, initially post-exercise, then during exercise, then at rest
- Pain pattern: Activity-related, improves with rest, night pain in severe cases
- Risk factors: Menstrual history, dietary intake, prior stress fractures, medications
- Inspection: May be unremarkable; check for overlying swelling or warmth
- Palpation: Localised bony tenderness (most sensitive clinical sign)
- Special tests: Hop test (positive = pain on single-leg hop = tibial stress fracture until proven otherwise), fulcrum test (femoral shaft), tuning fork (low sensitivity)
- Gait: Antalgic gait in severe cases, especially femoral neck
Clinical presentation: Groin or anterior thigh pain worse with weight-bearing, possible night pain, positive log roll, pain on axial compression. Hop test: The patient should NOT be asked to hop if a femoral neck stress fracture is suspected — this may displace it. If suspected clinically, proceed directly to MRI on crutches and non-weight-bearing until fracture is excluded. A displaced femoral neck fracture in a young athlete has a high risk of AVN and is an orthopaedic emergency.
- Pain Location
- Groin, anterior thigh
- Key Examination Finding
- Pain on axial compression, positive log roll, night pain
- Urgency
- URGENT — MRI same day, NWB until excluded
- Pain Location
- Anterior shin, worse with jumping
- Key Examination Finding
- Localised anterior cortical tenderness, pain on hopping
- Urgency
- HIGH — confirm with CT/lateral X-ray for 'dreaded black line'
- Pain Location
- Dorsal midfoot, deep ache
- Key Examination Finding
- Tenderness over navicular tuberosity, pain on toe-walking
- Urgency
- HIGH — CT to confirm fracture line
- Pain Location
- Lateral foot, base of 5th MT
- Key Examination Finding
- Tenderness at proximal diaphysis, pain with inversion
- Urgency
- HIGH — distinguish from tuberosity avulsion (zone 1)
- Pain Location
- Posteromedial shin, bilateral possible
- Key Examination Finding
- Diffuse posteromedial tenderness, positive hop test
- Urgency
- LOW — MRI for grading, relative rest
- Pain Location
- Plantar first MTP, worse with toe-off
- Key Examination Finding
- Tender plantar-medial sesamoid, pain with hallux extension
- Urgency
- MODERATE — distinguish bipartite from fracture
Hop test: Single-leg hopping reproduces tibial stress fracture pain. Positive = stress fracture until proven otherwise. Do NOT perform if femoral neck stress fracture is suspected.
Fulcrum test: Patient sits with lower legs dangling off table edge. Examiner applies downward pressure on distal femur while using the other hand as a fulcrum under the mid-thigh. Pain at the fulcrum point = femoral shaft stress fracture.
LEAFRED-S Assessment
Hook:A LEAF falls when the tree lacks nutrients — RED-S is low energy availability starving the skeleton!
Investigations
Imaging Protocol
Views: AP and lateral of the symptomatic bone; specific views depending on site (e.g., Ferguson view for sacrum, oblique foot for 5th MT)
Look for: Periosteal reaction, cortical thickening, callus, lucent fracture line, 'dreaded black line' (anterior tibia)
Important: Normal X-rays do NOT exclude a stress fracture — sensitivity is only 15-30% in the first 2-3 weeks
Sequences: STIR (oedema-sensitive), T1 (anatomy and fracture line), T2 fat-sat
Findings: Bone marrow oedema (early), periosteal oedema, fracture line (late)
Grading: Fredericson grade 1-4 (see Classification tab)
Clinical correlation: Grade does not always correlate with symptoms; use both to guide management
Indication: When fracture line needs precise characterisation (navicular, anterior tibial cortex, pars interarticularis)
Strength: Superior cortical detail; confirms whether a fracture line has propagated through cortex
Limitation: Less sensitive than MRI for early marrow oedema (grade 1-2 Fredericson)
DEXA scan: Bone mineral density at lumbar spine and hip; Z-score less than -1.0 in a young athlete is concerning
Blood panel: Calcium, phosphate, vitamin D (25-OH), PTH, alkaline phosphatase, TFT, sex hormones (oestradiol / testosterone), cortisol, FBC, ferritin
Purpose: Identify underlying metabolic bone disease, endocrine dysfunction, and nutritional deficiency
- Suspected stress fracture → X-ray first (may be normal, do NOT be reassured)
- X-ray normal, clinical suspicion persists → MRI (gold standard, do not delay)
- MRI shows fracture line at high-risk site → CT to characterise (navicular, anterior tibia)
- Recurrent stress fracture or RED-S suspected → DEXA + metabolic panel + vitamin D
Do NOT use bone scan as first-line — MRI provides grading and anatomic detail that bone scan cannot.


Management Algorithm
High-Risk Stress Fracture Management
Principle: High-risk sites on the tension side or with poor vascularity require aggressive management. Non-operative treatment often fails.
Femoral Neck Stress Fractures
- Location
- Superior cortex of femoral neck
- Management
- Urgent cannulated screw fixation (2-3 screws)
- Prognosis
- Good if fixed before displacement; AVN risk if displaced
- Location
- Inferior cortex of femoral neck
- Management
- NWB 4-6 weeks, repeat MRI to confirm healing; fix if progresses
- Prognosis
- Generally good; monitor for progression to tension side
- Location
- Any location, complete fracture
- Management
- Emergency ORIF (cannulated screws or sliding hip screw)
- Prognosis
- Guarded: AVN rate up to 30-60% in young adults
Tension-side femoral neck stress fractures in young adults are one of the few true orthopaedic emergencies in sports medicine. A displaced femoral neck fracture in a patient aged less than 50 years carries a devastating risk of avascular necrosis (up to 30-60%). Urgent internal fixation with parallel cannulated screws or a sliding hip screw is the standard of care. Do NOT trial non-operative management in an athlete with a tension-side fracture.
GRAFTImaging and Management Approach
Hook:GRAFT a plan — Grade, Rest, Assess RED-S, Fix the high-risk ones, and give it Time!
Complications
- Risk Sites
- Femoral neck (tension), anterior tibia
- Incidence
- Up to 30% if tension-side femoral neck treated non-operatively
- Prevention / Management
- Urgent fixation for high-risk sites; NWB until excluded
- Risk Sites
- 5th MT base (Jones), navicular, anterior tibia, sesamoid
- Incidence
- 15-30% for Jones fracture non-operative; up to 40% navicular if delayed
- Prevention / Management
- Early surgical fixation in athletes; adequate NWB duration; rule out RED-S
- Risk Sites
- Femoral neck (displaced), navicular (proximal pole)
- Incidence
- Up to 30-60% in displaced femoral neck (young adults)
- Prevention / Management
- Fix before displacement; do NOT allow WB on tension-side femoral neck
- Risk Sites
- Any site (especially tibia, metatarsals)
- Incidence
- 10-20% recurrence; up to 50% with untreated RED-S
- Prevention / Management
- RED-S screening, DEXA, vitamin D optimisation, training load management
- Risk Sites
- Anterior tibia, 5th MT, navicular, sesamoid
- Incidence
- Common in high-risk sites treated non-operatively
- Prevention / Management
- Adequate immobilisation; surgical fixation if no healing by 3-4 months
- Risk Sites
- Femoral neck (post-displacement or AVN), navicular
- Incidence
- Up to 40% after displaced femoral neck fracture
- Prevention / Management
- Fixation before displacement is the best prevention
The most important principle in stress fracture management is prevention. This includes: gradual training progression (no more than 10% increase per week), adequate nutrition and energy availability, screening for RED-S, optimising vitamin D and calcium, addressing biomechanical factors, and using appropriate footwear. A displaced femoral neck stress fracture in a young athlete can be career-ending — early recognition and fixation before displacement is critical.
Outcomes and Prognosis
- Treatment
- Relative rest 6-8 weeks
- Return to Sport
- 6-10 weeks with graded programme
- Long-Term Outlook
- Excellent; full return expected
- Treatment
- Cannulated screw fixation
- Return to Sport
- 3-4 months post-fixation
- Long-Term Outlook
- Good if fixed before displacement; monitor for AVN
- Treatment
- Emergency ORIF
- Return to Sport
- 6-12 months; may not return to elite sport
- Long-Term Outlook
- Guarded: AVN rate 30-60%; risk of secondary OA
- Treatment
- Intramedullary nailing
- Return to Sport
- 3-4 months post-op
- Long-Term Outlook
- Good union rate; anterior knee pain common
- Treatment
- Strict NWB 6-8 weeks
- Return to Sport
- 4-6 months
- Long-Term Outlook
- Good if treated early; nonunion risk if poorly compliant
- Treatment
- Percutaneous IM screw
- Return to Sport
- 8-12 weeks post-op
- Long-Term Outlook
- Excellent union rate in athletes with fixation
- Treatment
- NWB + sesamoid pad 6-8 weeks
- Return to Sport
- 3-4 months
- Long-Term Outlook
- Variable; excision may be needed in refractory cases
Best prognosis: Low-risk site, early diagnosis (grade 1-2 MRI), compliant with relative rest, adequate nutrition, no RED-S
Poor prognosis: High-risk site, delayed diagnosis, displacement, untreated RED-S, recurrent fractures, low vitamin D
Key message: Time to diagnosis is the single most important prognostic factor. A femoral neck stress fracture diagnosed and fixed before displacement has a good prognosis; a displaced fracture may end a career.
Guidelines, Registries & Global Practice
- Tibial stress fractures are the most common stress fracture worldwide in runners and military personnel
- Femoral neck stress fractures represent less than 10% of stress fractures but carry the highest morbidity
- Female athletes: 2-4 times increased risk across all sports, driven by RED-S / low energy availability
- Military recruits: Incidence of 5-10% during basic training; tibial and metatarsal sites predominate
- High-resource: Early MRI, DEXA scanning, multidisciplinary RED-S teams, surgical fixation for high-risk sites in athletes
- Limited-resource: X-ray and clinical diagnosis; prolonged casting for high-risk sites; limited access to MRI may delay diagnosis
- Universal principle: Clinical diagnosis (localised bony tenderness, activity-related pain) should trigger non-weight-bearing and imaging even when X-rays are normal
- Surgical fixation: Concentrated in specialist centres globally; percutaneous techniques have improved outcomes for Jones and navicular fractures
- Imaging Approach
- MRI gold standard; CT adjunct for navicular and tibial cortex
- High-Risk Management
- Surgical fixation for tension-side femoral neck and displaced navicular
- RED-S Approach
- IOC RED-S consensus; multidisciplinary screening mandatory
- Imaging Approach
- MRI first-line; Fredericson grading to guide return to play
- High-Risk Management
- Conservative for compression-side; operative for tension-side
- RED-S Approach
- Position stand on female athlete triad / RED-S; Z-score screening
- Imaging Approach
- MRI recommended; bone scan where MRI unavailable
- High-Risk Management
- Fix tension-side femoral neck; NWB cast for navicular
- RED-S Approach
- RED-S consensus statement; multidisciplinary team model
- Imaging Approach
- MRI-based classification; early imaging in at-risk athletes
- High-Risk Management
- Surgical fixation for high-risk sites in elite athletes
- RED-S Approach
- RED-S consensus 2014/2018 — comprehensive multisystem approach
- Imaging Approach
- CT for fracture line assessment in specific sites
- High-Risk Management
- Fixation principles: cannulated screws for femoral neck, IM screws for 5th MT
- RED-S Approach
- Nutritional and endocrine optimisation as part of fracture management
There is no dedicated arthroplasty or fracture registry for stress fractures, as most are treated non-operatively and managed in sports medicine rather than surgical settings. The evidence base is predominantly retrospective case series and expert consensus rather than randomised controlled trials. Key guidance comes from the IOC RED-S consensus statements, the ACSM Female Athlete Triad position stand, and the Fredericson MRI classification — these form the backbone of exam answers on this topic.
Record in every stress fracture presentation:
- Site and risk classification (high-risk vs low-risk)
- Imaging performed and Fredericson grade (if MRI done)
- RED-S screening status (completed / not completed / referral made)
- Weight-bearing status and activity restrictions prescribed
- Follow-up imaging plan and expected timeline
- Multidisciplinary team involvement (nutrition, psychology, endocrinology)
A missed high-risk stress fracture that progresses to a complete fracture or nonunion is a recurring source of medicolegal claims. Always document risk classification, imaging results, and the rationale for operative versus non-operative management.
Controversies & Areas of Uncertainty
Percutaneous screw fixation in athletes offers faster and more reliable return to sport, but non-operative management with NWB casting can succeed in non-athletes. The optimal screw diameter, solid vs cannulated, and need for bone graft remain debated. Refracture after screw removal is a recognised concern.
Pneumatic leg braces reduce tibial bending stress and may accelerate return to sport for posterior-medial tibial stress fractures, but evidence from randomised trials is limited. They are NOT appropriate for anterior tibial cortex fractures (tension side).
There is no universally agreed return-to-play protocol for athletes recovering from RED-S. The IOC consensus provides a framework but clear quantitative thresholds for energy availability, BMD recovery, and menstrual restoration remain debated. Some advocate a minimum 6-month period of normal menses before full training resumes.
Bisphosphonates increase BMD and may reduce stress fracture risk in military recruits, but they are NOT recommended in pre-menopausal women due to theoretical teratogenicity and the risk of atypical femoral fractures with long-term use. The role of bisphosphonates in treating (rather than preventing) stress fractures is unproven and controversial.
MCQ Practice Points
Q: What is the most important distinction in the management of stress fractures? A: High-risk vs low-risk sites. High-risk sites (femoral neck tension side, anterior tibial cortex, tarsal navicular, 5th metatarsal base, hallux sesamoid) are on the tension side or in poorly vascularised areas and require aggressive, often surgical, management. Low-risk sites (posterior-medial tibia, fibula, 2nd-4th metatarsals) are on the compression side and heal with activity modification.
Q: A runner has suspected tibial stress fracture. X-rays are normal. What is the next best investigation? A: MRI with STIR and T1 sequences. MRI is the gold standard for bone stress injuries with near 100% sensitivity. It detects marrow oedema (grade 1-2 Fredericson) weeks before X-ray changes appear and can identify fracture lines (grade 3-4). Do NOT wait for X-ray changes to appear — this delays diagnosis and risks fracture progression.
Q: A 25-year-old runner has groin pain and a tension-side femoral neck stress fracture on MRI. What is the management? A: Urgent cannulated screw fixation. Tension-side (superolateral) femoral neck stress fractures have a high rate of propagation to complete fracture and displacement. A displaced femoral neck fracture in a young adult has a 30-60% AVN rate. Fixation with 2-3 parallel cannulated screws before displacement is the standard of care. Do NOT trial non-operative management.
Q: What is RED-S and which athletes should be screened? A: Relative Energy Deficiency in Sport (formerly 'female athlete triad') is a multisystem disorder caused by low energy availability affecting metabolic rate, menstrual function (females), testosterone (males), bone health, immune function, and psychological wellbeing. Every athlete with a stress fracture should be screened for RED-S, especially endurance athletes, those with recurrent fractures, amenorrhoea, low BMI, or disordered eating patterns.
Q: What is a Jones fracture and why is it significant? A: A Jones fracture is a fracture at the metaphyseal-diaphyseal junction of the 5th metatarsal (Zone 2), distal to the tuberosity. It is significant because this region is a watershed area of vascularity with a high rate of nonunion (up to 30% non-operative). In athletes, percutaneous intramedullary screw fixation is recommended for reliable union and faster return to sport. It must be distinguished from a Zone 1 tuberosity avulsion fracture (which heals reliably non-operatively).
Q: What is the 'dreaded black line' and how is it managed? A: The 'dreaded black line' is a radiolucent line seen on lateral X-ray at the anterior tibial cortex, representing a tension-side stress fracture with cortical disruption. It is 'dreaded' because the fracture can propagate to a complete fracture under continued loading. Management in athletes is typically intramedullary nailing for reliable healing and return to sport; non-operative management with extended NWB is reserved for non-athletes but has a high failure rate.
Clinical Imaging
Imaging Approach to Stress Fractures
- Sensitivity
- Low initially (15-30%); improves to 50-70% by 3 weeks
- When Positive
- Periosteal reaction, cortical lucency, callus, fracture line
- Limitation
- Normal in first 2-3 weeks; cannot rule out stress fracture
- Sensitivity
- High (near 100% for bone stress injury)
- When Positive
- Bone marrow oedema (STIR), fracture line (T1), periosteal oedema
- Limitation
- Gold standard; Fredericson grading system guides management
- Sensitivity
- Moderate — excellent for cortical detail
- When Positive
- Cortical breach, fracture line (especially tibial anterior cortex, navicular)
- Limitation
- Misses marrow oedema early; used to confirm fracture line at specific sites
- Sensitivity
- High sensitivity (approaching 100%)
- When Positive
- Focal increased uptake (positive within 24-72 hours of onset)
- Limitation
- Low specificity; radiation exposure; largely replaced by MRI
- Sensitivity
- Low — limited role
- When Positive
- Periosteal reaction, cortical irregularity
- Limitation
- Operator-dependent; not recommended as primary imaging
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 24-year-old elite female distance runner presents with a 3-week history of progressive left groin pain worse with running and now present with walking. She has been amenorrhoeic for 8 months. She trains 120 km per week and has a BMI of 17.5. X-rays of the hip are reported as normal. How do you manage this patient?”
“A 22-year-old professional basketball player presents with a 6-week history of deep aching dorsal midfoot pain that worsens with running and jumping. He has been playing through pain. Examination reveals localised tenderness over the tarsal navicular. X-rays are normal. What is your diagnosis and management plan?”
Classification
- Fatigue fracture = abnormal load on normal bone (athletes, military)
- Insufficiency fracture = normal load on abnormal bone (osteoporosis, metabolic)
- High-risk sites = NAFFS: Navicular, Anterior tibia, Femoral neck (tension), Fifth MT base, Sesamoid
- Tension-side fractures propagate and need fixation; compression-side fractures heal with rest
Imaging
- X-ray: normal in 70-85% early; do NOT be reassured by a normal film
- MRI (STIR + T1): gold standard; Fredericson grade 1-4 guides management
- CT: adjunct for cortical fracture line (navicular, anterior tibia, pars)
- Bone scan: sensitive but non-specific; largely replaced by MRI
High-Risk Site Management
- Femoral neck tension side = urgent cannulated screw fixation (Fullerton classification)
- Anterior tibial cortex = IM nail in athletes; 'dreaded black line' on lateral X-ray
- Navicular = NWB cast 6-8 weeks (non-displaced); ORIF if displaced
- 5th MT Jones = percutaneous screw in athletes; NWB cast in non-athletes
RED-S
- Formerly 'female athlete triad'; affects males and females
- Low energy availability causes hypothalamic suppression, hormonal disruption, low BMD
- Screen every stress fracture patient: diet, menses/testosterone, BMI, training load
- DEXA Z-score less than -1.0 in young athlete = investigate further
Key Exam Answers
- Normal X-ray does NOT exclude stress fracture — proceed to MRI
- Tension-side femoral neck fracture = operate, do NOT trial conservative
- Fredericson grade 4 = fracture line visible on both STIR and T1 MRI
- Greater than 10% weekly training volume increase is a key risk factor for recurrence
Evidence Base and Key Trials
Tibial stress reaction in runners. Correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system
- Established the Fredericson MRI grading system (grades 1-4) for tibial stress injuries
- MRI detected stress injuries 2-4 weeks before radiographs showed abnormalities
- Grade correlated with clinical severity and guided return-to-play timelines
- STIR sequence was the most sensitive for early bone marrow oedema
American College of Sports Medicine position stand: the female athlete triad
- Formalised the Female Athlete Triad as low energy availability, menstrual dysfunction, and low BMD
- Established screening guidelines for at-risk athletes including DEXA criteria
- Z-score less than -1.0 at lumbar spine or hip in a young athlete warrants further investigation
- Energy availability below 30 kcal/kg lean body mass per day disrupts luteinising hormone pulsatility
Low-risk stress fractures
- Classified stress fractures into high-risk and low-risk sites based on biomechanics and healing potential
- High-risk sites: femoral neck (tension), anterior tibial cortex, tarsal navicular, 5th metatarsal base, sesamoid
- Low-risk sites: posterior-medial tibia, fibula, 2nd-4th metatarsals, calcaneus, femoral shaft
- Tension-side fractures propagate and require aggressive management; compression-side fractures heal with rest
Femoral neck stress fractures
- Classified femoral neck stress fractures into tension-side (superolateral) and compression-side (inferomedial)
- Tension-side fractures have a high propensity for displacement and require urgent internal fixation
- Compression-side fractures can be managed non-operatively with NWB and close monitoring
- Displaced fractures carry AVN risk up to 30% and require emergency ORIF
Fractures of the base of the fifth metatarsal distal to the tuberosity: classification and guidelines for non-surgical and surgical management
- Classified proximal 5th metatarsal fractures into acute (Type I), delayed union (Type II), and nonunion (Type III) based on radiographic and clinical features
- Type I (acute) fractures in athletes benefit from early intramedullary screw fixation for reliable union
- Non-operative treatment with NWB casting had a high nonunion rate for Jones fractures (up to 30%)
- Type II and Type III fractures require ORIF with bone grafting