Shoulder Pain | Rotator Cuff Pathology | Conservative First | Surgery for Refractory Cases
- Primary impingement = structural narrowing (acromion, AC joint) vs Secondary impingement = rotator cuff weakness/instability
- Neer test (passive forward flexion) and Hawkins-Kennedy test (IR at 90° flexion) - highest sensitivity when combined
- Conservative treatment for 3-6 months before considering surgery - includes NSAIDs, physiotherapy, subacromial injection
- Subacromial decompression = arthroscopic acromioplasty + bursectomy - controversial efficacy vs sham surgery
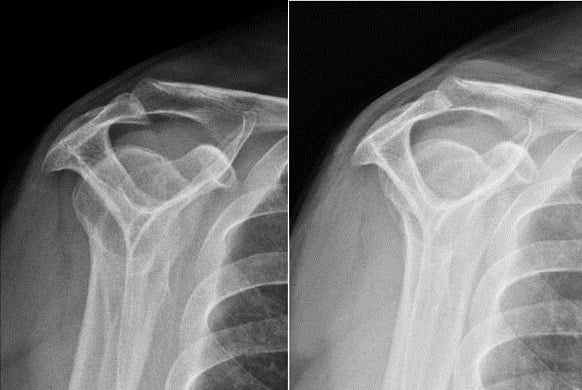
- Imaging - X-ray for bone abnormalities (acromion shape, spurs), MRI for rotator cuff tears and inflammation
- “Most common cause of shoulder pain in adults over 40 years
- “Neer and Hawkins-Kennedy are only moderately accurate (sensitivity ~72-79%) - combine tests and confirm with an injection test
- “CSAW (2018, Lancet) and FIMPACT (2018, BMJ) showed no benefit of arthroscopic decompression over placebo surgery
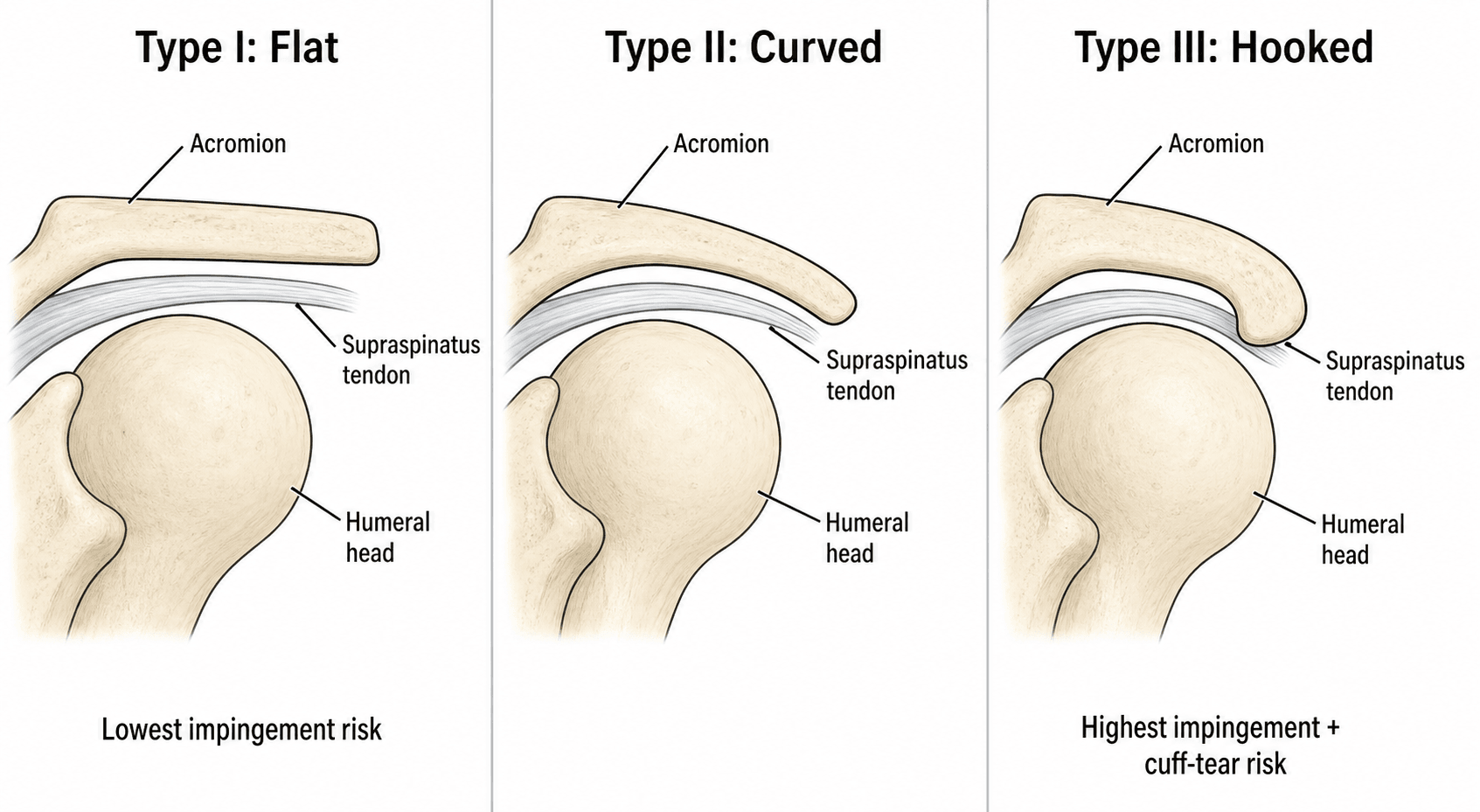
- “Bigliani classification of acromion shape (Type I flat, II curved, III hooked) - Type III highest impingement risk
Primary = structural narrowing (acromion morphology, spurs, AC joint arthritis). Secondary = rotator cuff weakness or instability causing superior humeral head migration. Treatment differs - address underlying cause.
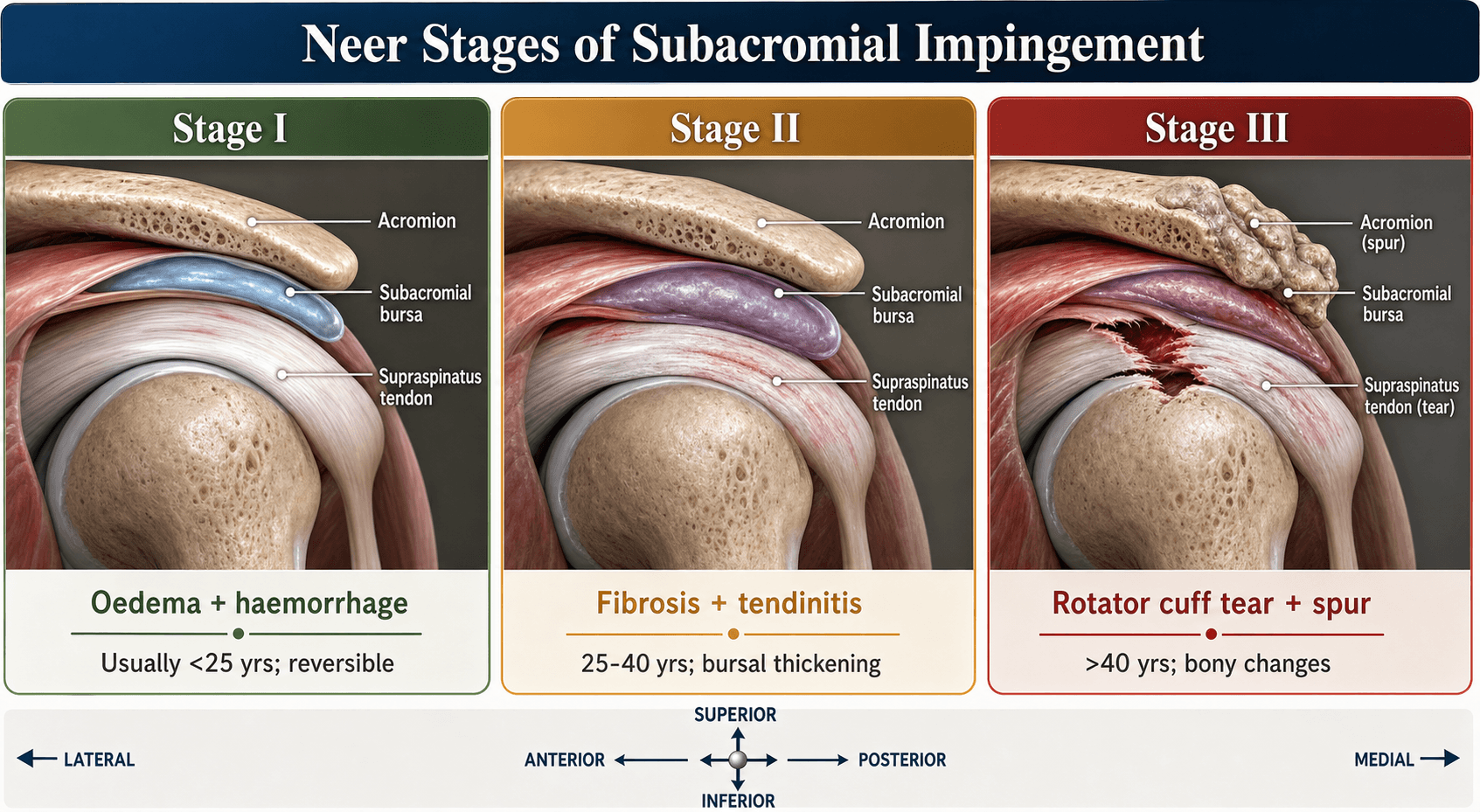
Stage I (under 25 years) = edema/hemorrhage, reversible. Stage II (25-40 years) = fibrosis/tendinitis. Stage III (over 40 years) = bone spurs, tears, irreversible. Guides prognosis and treatment.
Meta-analysis (Hegedus 2012) gives Neer sensitivity 72% / specificity 60% and Hawkins-Kennedy 79% / 59% - moderate, not confirmatory. Cluster tests and confirm with the subacromial injection test (lidocaine abolishes pain) for diagnosis.
CSAW (2018, Lancet) showed arthroscopic decompression no better than placebo surgery, and the Finnish FIMPACT (2018, BMJ) confirmed this at 24 months. The 2019 BMJ Rapid Recommendation advises against routine surgery; reserve it for highly selected refractory cases.
- Stage
- Stage I - Acute inflammation
- First-Line Treatment
- Rest, NSAIDs, early physio
- Key Pearl
- Rule out instability - may be secondary impingement
- Stage
- Stage II - Fibrosis/tendinitis
- First-Line Treatment
- Subacromial steroid injection + structured rehab
- Key Pearl
- Need 3-6 months total conservative trial before surgery
- Stage
- Stage III - Structural changes
- First-Line Treatment
- Consider surgery if failed conservative
- Key Pearl
- Manage cuff tear if present - may need repair not just decompression
FINSNeer Impingement Provocation Test Technique
Hook:FINS help the fish swim UP (forward flexion) - Neer test moves arm upward!
Overview and Epidemiology
Subacromial impingement syndrome (SIS) is the most common cause of shoulder pain in adults, accounting for 44-65% of all shoulder pain complaints. The condition results from mechanical compression of the rotator cuff tendons and subacromial bursa within the subacromial space during shoulder elevation.
SIS represents a spectrum of pathology from acute reversible inflammation to chronic irreversible tendon degeneration and tears. Understanding the distinction between primary (structural) and secondary (functional) impingement is critical for appropriate treatment selection. Recent high-quality RCTs have challenged traditional surgical approaches, making this a high-yield exam topic for evidence-based discussion.
- Age: Peak incidence 40-60 years
- Gender: Slightly more common in females (1.2:1)
- Occupation: Overhead workers, athletes (swimmers, throwers)
- Dominant arm: More commonly affected (60%)
- Work loss: Average 6-12 weeks for manual laborers
- Function: Significant disability in ADLs and sleep
- Progression: 5-10% develop full-thickness rotator cuff tears annually
- Economic: $3 billion annual healthcare costs (US data)
Anatomy
The subacromial space measures approximately 7-14mm in height. Any reduction below 7mm significantly increases impingement risk. This narrow corridor contains the supraspinatus tendon, long head biceps, subacromial bursa, and rotator cuff interval. Understanding this confined anatomy explains why even small changes (1-2mm bone spurs, bursal thickening) cause significant symptoms.
Primary Impingement (Extrinsic Compression)
Structural factors that narrow the subacromial space:
- Mechanism
- Hooked acromion reduces clearance by 3-5mm
- Prevalence
- 20-30% of population
- Clinical Significance
- Highest impingement risk - often requires acromioplasty
- Mechanism
- Osteophyte formation narrows outlet
- Prevalence
- 30-40% over age 50
- Clinical Significance
- Common in Stage III disease - visible on X-ray
- Mechanism
- Inferior osteophytes encroach on space
- Prevalence
- 25-35% over age 60
- Clinical Significance
- May require AC joint excision (Mumford procedure)
- Mechanism
- Mobile anterior acromion segment
- Prevalence
- 3-8% of population
- Clinical Significance
- Can be unstable - may need open fixation or excision
Secondary Impingement (Functional)
- Mechanism: Weak cuff cannot depress humeral head during elevation
- Superior migration: Head translates upward 2-4mm
- Cycle: Impingement causes pain → disuse → further weakness
- Treatment: Address weakness, not surgical decompression
- Mechanism: Subtle instability (microinstability) causes abnormal kinematics
- Population: Young athletes, especially overhead sports
- Presentation: Positive apprehension/relocation tests alongside impingement signs
- Treatment: Stability rehabilitation, not acromioplasty
SCABSubacromial Space Anatomical Boundaries
Hook:The SCAB forms when impingement causes inflammation - think of the inflamed bursa!
Pathophysiology
Pathological Cascade (Neer Stages)
Progressive Pathology
Pathology: Acute inflammatory response to mechanical irritation. Bursal edema, microhemorrhage in supraspinatus tendon.
Reversibility: Completely reversible with rest and conservative treatment.
Clinical: Acute onset pain, positive impingement tests, full strength initially.
Pathology: Chronic inflammation leads to bursal thickening (3-5mm), tendon fibrosis, early degeneration.
Reversibility: Partially reversible - fibrosis persists but symptoms can resolve.
Clinical: Chronic pain, night pain common, weakness developing, positive impingement tests.
Pathology: Anterior-inferior acromial spurs, greater tuberosity changes, partial or full-thickness rotator cuff tears.
Reversibility: Irreversible structural changes - symptom management only.
Clinical: Chronic pain, weakness, limited ROM, crepitus, positive impingement and cuff tear tests.
Classification Systems
Neer Classification of Impingement Stages
Historical but still clinically relevant staging system based on pathological changes and age.
- Age Range
- Under 25 years
- Pathology
- Reversible edema, hemorrhage, inflammation
- Treatment Approach
- Conservative only - rest, NSAIDs, physio
- Age Range
- 25-40 years
- Pathology
- Fibrosis, tendinitis, bursal thickening
- Treatment Approach
- Conservative first; surgery if failed 6 months
- Age Range
- Over 40 years
- Pathology
- Bone spurs, rotator cuff tears, irreversible
- Treatment Approach
- Often surgical - may need cuff repair not just decompression
While age ranges are guidelines, pathological stage matters more than chronological age. A 30-year-old overhead athlete may have Stage III disease, while a 50-year-old office worker may have Stage I. MRI and clinical exam determine stage, not just age.
FCHBigliani Acromion Classification
Hook:FCH = From Curve to Hook - progressive impingement risk increases!
EFTNeer Staging of Impingement
Hook:Edema, Fibrosis, Tears - impingement progresses with age!
Clinical Assessment
- Pain location: Anterolateral shoulder, radiates to deltoid insertion
- Aggravating factors: Overhead activities, reaching behind back, sleeping on affected side
- Onset: Gradual (chronic) vs acute (after injury/overuse)
- Occupation/sport: Overhead work (painters, carpenters), swimming, tennis, throwing
- Night pain: Common - suggests more advanced disease (Stage II-III)
- Weakness: Difficulty lifting, reaching - suggests cuff involvement
- Look: Muscle atrophy (supraspinatus, infraspinatus wasting), asymmetry
- Feel: Tenderness anterolateral acromion, AC joint, greater tuberosity
- Move: Painful arc 60-120° abduction, loss of active elevation
- Special tests: Impingement tests (Neer, Hawkins-Kennedy), cuff tests (Jobe, external rotation)
- Neurovascular: Exclude cervical radiculopathy, thoracic outlet syndrome
Key Special Tests
- Technique
- Passive forward flexion in IR, scapula stabilized
- Positive Finding
- Pain at terminal flexion
- Sensitivity
- 79-90%
- Specificity
- 31-53%
- Technique
- 90° forward flexion, passive IR
- Positive Finding
- Pain with IR movement
- Sensitivity
- 74-92%
- Specificity
- 25-58%
- Technique
- 10ml lidocaine subacromial injection, repeat Neer test
- Positive Finding
- Complete pain relief confirms impingement
- Sensitivity
- 75-95%
- Specificity
- 40-70%
- Technique
- Active abduction 0-180°
- Positive Finding
- Pain between 60-120° (most 70-110°)
- Sensitivity
- 33-98%
- Specificity
- 10-81%
Single test specificity is poor - Neer and Hawkins-Kennedy have high sensitivity (good for ruling OUT) but low specificity (many false positives). Combination approach: If BOTH Neer AND Hawkins-Kennedy are positive, combined specificity increases to 70-80%. Impingement injection test is most specific - complete pain relief confirms diagnosis and predicts good response to treatment.
C5 radiculopathy can present with shoulder pain, weakness, and positive impingement tests. Always check: Spurling test (cervical compression), reflexes (biceps, brachioradialis), dermatomal sensation. Key distinction: Cervical pathology causes pain with neck movement, not just shoulder movement. MRI cervical spine if diagnostic doubt.
Differential Diagnosis
- Pain / History
- Weakness predominates; difficulty initiating abduction; age over 60
- Discriminating Examination
- Positive drop-arm / external-rotation lag sign; weakness not abolished by injection
- Key Investigation
- MRI or ultrasound shows full-thickness defect
- Pain / History
- Global stiffness, diabetic, insidious; night pain
- Discriminating Examination
- Loss of PASSIVE external rotation - the hallmark distinguishing feature
- Key Investigation
- Clinical; X-ray normal, arthrogram shows reduced capsular volume
- Pain / History
- Pain localised to the top of the shoulder
- Discriminating Examination
- Tenderness over AC joint; positive cross-body adduction (scarf) test
- Key Investigation
- X-ray AC views; pain relieved by AC joint injection
- Pain / History
- Deep, activity-related pain; crepitus; older patient
- Discriminating Examination
- Restricted painful rotation; grinding on movement
- Key Investigation
- X-ray shows joint-space loss, osteophytes
- Pain / History
- Neck and radiating arm pain, paraesthesia
- Discriminating Examination
- Positive Spurling test; altered reflexes/dermatomes; neck-driven pain
- Key Investigation
- MRI cervical spine; normal subacromial injection test
- Pain / History
- Acute severe pain, may be self-limiting
- Discriminating Examination
- Marked tenderness, guarding; signs overlap with impingement
- Key Investigation
- X-ray/ultrasound shows calcium deposit in cuff
HNPClinical Impingement Tests
Hook:HNP tests Hunt for Neer's Pathology!
Investigations
Imaging Protocol
Views: AP, axillary lateral, outlet view (scapular Y with 10° caudal tilt)
Findings:
- Acromion shape: Bigliani Type I/II/III on outlet view
- Acromial spurs: Anterior-inferior undersurface
- AC joint: Arthritis, inferior osteophytes, distal clavicle hypertrophy
- Greater tuberosity: Sclerosis, cysts, cortical irregularity (chronic impingement)
- Os acromiale: Unfused acromial apophysis (axillary view best)
- Calcific tendinitis: Calcium deposits in rotator cuff
Limitations: Cannot visualize soft tissues (cuff, bursa). Normal X-ray does NOT rule out impingement.
Advantages: Real-time visualization during movement, operator-dependent, low cost
Findings:
- Bursal thickening: Normal under 2mm; pathological greater than 3mm
- Subacromial space: Measure distance during abduction (normal 6-14mm)
- Rotator cuff: Partial tears, full-thickness tears, tendinosis
- Dynamic assessment: Observe impingement during active elevation
Sensitivity/Specificity: 67-98% for cuff tears (operator-dependent)
Indications: Suspected cuff tear, failed conservative treatment, pre-operative planning
Findings:
- Subacromial space: Fluid, bursal thickening (bright T2), fibrosis
- Rotator cuff: Partial/full-thickness tears, tendinosis, muscle atrophy
- Acromion: Bone marrow edema adjacent to cuff (chronic impingement)
- AC joint: Cartilage loss, osteophytes, joint effusion
- Labrum/capsule: Associated instability (secondary impingement)
Sensitivity: 84-100% for full-thickness tears, 44-91% for partial tears
Under 40 years, acute onset, normal exam strength: X-ray only, trial conservative treatment. Over 40 years, chronic pain, weakness: X-ray + MRI to exclude cuff tear (5-10% annual tear risk in this population). Pre-operative planning: Always MRI to assess cuff integrity - do not offer isolated acromioplasty if significant cuff tear present (may need repair).
Bigliani acromial shape is subjective and poorly reproducible, so modern practice favours two quantitative measurements of lateral acromial coverage on a true AP radiograph. The critical shoulder angle (CSA) is the angle between the line joining the superior and inferior bony margins of the glenoid and the line from the inferior glenoid to the most lateral point of the acromion (normal roughly 30-35°). A high CSA (more than about 35°) increases the superior shear force the deltoid applies to the humeral head and is associated with degenerative rotator cuff tears, whereas a low CSA (less than about 30°) is associated with primary glenohumeral osteoarthritis. The related acromion index (lateral extent of the acromion relative to the glenoid) carries the same message — a more laterally-extending acromion correlates with cuff disease. A live debate: because the CSA is partly acromial, some advocate lateral acromioplasty to reduce a high CSA, but the evidence that altering the CSA changes outcomes is unproven, so it remains investigational rather than standard practice.
Management Algorithm
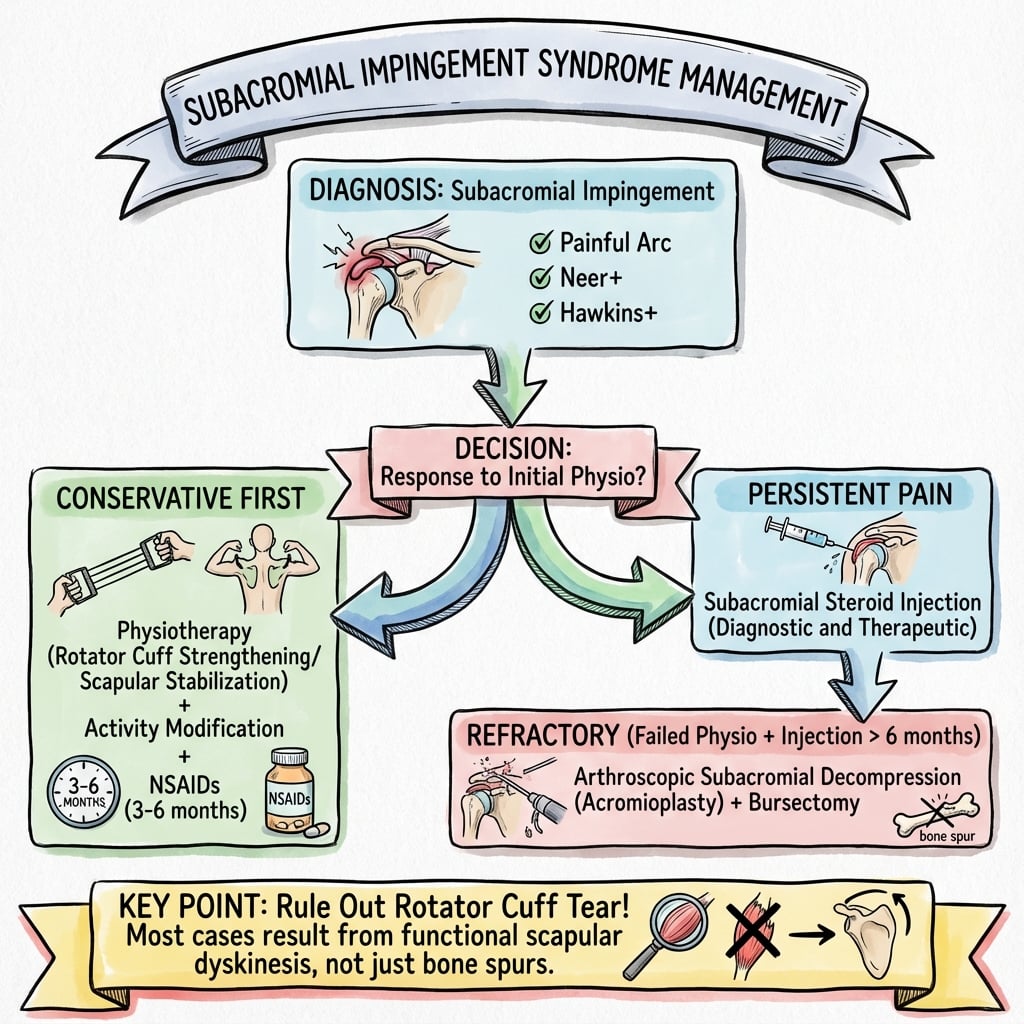
Conservative treatment is first-line for ALL patients and successful in 80-90% of cases. Minimum 3-6 month trial before considering surgery.
Conservative Management
Initial Management Goals
Primary objectives: Reduce pain and inflammation, maintain ROM, prevent stiffness
Treatment Protocol
- Avoid: Overhead activities, repetitive reaching, heavy lifting
- Modify: Work ergonomics (desk height, computer position)
- Sleep: Avoid lying on affected side; use pillow support
- Duration: 2-4 weeks strict avoidance, then gradual return
- NSAIDs: Ibuprofen 400mg TDS or naproxen 500mg BD for 10-14 days
- Ice therapy: 15-20 minutes TDS-QID (acute inflammation)
- Analgesics: Paracetamol 1g QID for additional pain relief
- Avoid: Prolonged immobilization (risk of frozen shoulder)
- Pendulum exercises: Passive ROM to prevent stiffness (days 1-7)
- Gentle ROM: Pulley exercises, wand exercises (weeks 1-3)
- Scapular stabilization: Early focus on periscapular muscles
- Avoid: Painful range, overhead strengthening too early
Over-aggressive rest (complete immobilization) increases frozen shoulder (adhesive capsulitis) risk by 2-3 fold. Maintain gentle ROM from week 1. If passive ROM is restricted (external rotation less than 50% of normal), suspect early capsulitis and intensify stretching.
Conservative Treatment Outcomes
Surgical Management
Absolute requirements for surgical consideration:
- Failed conservative treatment for minimum 3-6 months (optimal 6 months)
- Persistent symptoms significantly affecting quality of life
- Positive impingement signs on clinical exam
- Positive impingement injection test (confirms subacromial pathology)
- Structural abnormality on imaging (Type III acromion, spurs) - primary impingement
- Excluded secondary causes (instability, cuff weakness without structural lesion)
Contraindications: Secondary impingement, poor rehabilitation compliance, cervical pathology, significant cuff tears (may need repair).
Arthroscopic Acromioplasty and Bursectomy
Procedure: Arthroscopic removal of anterior-inferior acromion (5-7mm) and subacromial bursa.
Surgical Steps
Position: Beach chair or lateral decubitus
Portals: Posterior viewing, lateral working, anterior accessory
Diagnostic: Arthroscopy glenohumeral joint first - exclude labral pathology, cuff tears from articular side
Entry: Scope enters subacromial space via posterior portal
Bursa removal: Arthroscopic shaver debrides thickened, inflamed bursa
Visualization: Clear subacromial space to identify undersurface of acromion, CA ligament, and rotator cuff
Identify anterior-inferior acromion: The impinging prominence
Resection: Arthroscopic burr removes 5-7mm of bone, creating flat undersurface
Check: Ensure smooth undersurface, no residual spurs
CA ligament: Partial or complete release (controversial - can cause instability)
Hemostasis: Check for bleeding, irrigate
Closure: Simple portal closure
Immobilization: Sling for comfort only (24-48 hours)
Rehabilitation: Early ROM day 1, strengthening week 2-4
CSAW Trial (2018, Lancet, n=313): Arthroscopic subacromial decompression vs investigational arthroscopy only (placebo) vs no treatment. Result: No clinically important difference between decompression and placebo at 6 months. FIMPACT Trial (2018, BMJ, n=210): Decompression vs diagnostic arthroscopy (placebo) vs exercise - no benefit of decompression over placebo at 24 months. Conclusion: The 2019 BMJ Rapid Recommendation makes a strong recommendation against surgery for subacromial pain syndrome. Current practice: Highly selective surgery only after genuine failure of prolonged conservative care. In the exam, acknowledge this Level 1 evidence.
Complications
Conservative Treatment Complications
- Incidence
- 2-5%
- Risk Factors
- Prolonged immobilization, diabetic patients
- Management
- Maintain ROM exercises from onset, aggressive stretching if develops
- Incidence
- Rare with under 3 injections/year
- Risk Factors
- Greater than 3 steroid injections annually
- Management
- Limit to 3 injections maximum per year, space 3 months apart
- Incidence
- 5-10% annually
- Risk Factors
- Age over 50, chronic impingement, partial tear
- Management
- Regular review, MRI if worsening weakness
Surgical Complications
- Incidence
- 10-15%
- Risk Factors
- Secondary impingement, missed cuff tear, inadequate rehab
- Prevention/Management
- Exclude at outset - don't operate on secondary impingement
- Incidence
- 3-8%
- Risk Factors
- Prolonged immobilization, poor compliance with PT
- Prevention/Management
- Early ROM from day 1, supervised physiotherapy
- Incidence
- 2-5%
- Risk Factors
- Axillary nerve injury (open), detachment (open)
- Prevention/Management
- Limit deltoid split to less than 5cm from acromion, careful dissection
- Incidence
- Less than 1%
- Risk Factors
- Diabetes, immunosuppression, steroid injection pre-op
- Prevention/Management
- Antibiotic prophylaxis, aseptic technique, delay surgery 3 months post-injection
- Incidence
- 1-3%
- Risk Factors
- Excessive CA ligament release, over-resection of acromion
- Prevention/Management
- Preserve CA arch integrity, limit resection to 5-7mm
Most common cause: Operating on secondary impingement (rotator cuff weakness, instability). These patients have positive impingement signs but surgery does not address the underlying functional problem. Prevention: Thorough preoperative assessment to distinguish primary (structural) from secondary (functional) impingement. Young athletes with instability signs should NOT have acromioplasty.
Postoperative Care and Rehabilitation
Rehabilitation Timeline
- Immobilization: Sling for comfort only (not mandatory)
- Pain control: Ice, analgesics, limit opioids
- Early ROM: Pendulum exercises day 1, passive forward flexion to tolerance
- Goal: Prevent stiffness, control pain
- ROM: Active-assisted ROM all planes, wand exercises
- Sling: Discontinue when comfortable (usually 3-5 days)
- Avoid: Resisted exercises, heavy lifting
- Goal: Full passive ROM by week 2
- Strengthening: Begin rotator cuff and scapular exercises (isometric, then theraband)
- ROM: Full active ROM by week 4-6
- Functional: Light ADLs, desk work
- Goal: Restore muscle balance, endurance
- Advanced strengthening: Progressive resistance, sport-specific exercises
- Return to work: Manual labor by week 8-12 (depending on demands)
- Return to sport: Overhead athletes week 12-16
- Goal: Full function, return to activities
Week 2: Full passive ROM expected. Week 6: Full active ROM expected. Week 12: Return to overhead sports. Failure to achieve these milestones suggests complication (frozen shoulder, re-impingement) - investigate and intensify physiotherapy.
Outcomes and Prognosis
Conservative Treatment Outcomes
- Short-term (3-6 months)
- 60-70% improvement
- Long-term (1-2 years)
- 50-60% sustained
- Notes
- Best for Stage I, younger patients
- Short-term (3-6 months)
- 70-80% improvement
- Long-term (1-2 years)
- 60-70% sustained
- Notes
- Standard first-line approach
- Short-term (3-6 months)
- 75-85% improvement
- Long-term (1-2 years)
- 65-75% sustained
- Notes
- Injection benefits mainly short-term (under 12 weeks)
Surgical Outcomes
- Traditional Series
- 75-85% significant improvement
- CSAW Trial (2018)
- No difference vs sham surgery
- Interpretation
- Questions whether improvement is due to surgery or placebo/natural history
- Traditional Series
- 70-80% return to work/sport
- CSAW Trial (2018)
- Similar improvement in all 3 groups (surgery, sham, conservative)
- Interpretation
- Suggests natural improvement over time regardless of treatment
- Traditional Series
- 80-85% satisfied
- CSAW Trial (2018)
- High satisfaction in all groups including sham
- Interpretation
- Highlights powerful placebo effect of surgery
Prognostic Factors
- Age under 50 years: Better outcomes with both conservative and surgical treatment
- Short symptom duration (less than 6 months): Responds better to conservative treatment
- Positive injection test: Predicts good surgical outcome (if structural impingement)
- Type III acromion with spur: Clear structural abnormality (if primary impingement)
- Good rehabilitation compliance: Critical for both conservative and surgical success
- Secondary impingement: Surgery fails (instability or cuff weakness not addressed)
- Workers' compensation claims: Associated with worse outcomes (psychological factors)
- Chronic symptoms (over 2 years): Lower success rates
- Significant cuff tear: Need cuff repair, not just decompression
- Smoking, diabetes: Delayed healing, higher complication rates
Pre-CSAW (before 2018): Surgical outcomes quoted as 75-85% good-excellent results based on traditional case series. Post-CSAW (2018 onward): High-quality RCT showed no benefit over sham surgery, challenging these historical results. Current consensus: Surgery may still benefit highly selected patients (failed prolonged conservative treatment, clear structural abnormality, positive injection test), but expectations should be moderated given trial evidence. Quote realistic outcomes: "50-75% chance of significant improvement, but this may occur with continued conservative treatment as well."
Guidelines, Registries & Global Practice
Global Epidemiology
Shoulder pain is one of the three most common musculoskeletal presentations in primary care worldwide, and subacromial pain syndrome (the umbrella term now preferred over "impingement") accounts for the largest share of these complaints. Reported point prevalence of shoulder pain in adults ranges widely (roughly 7-26%) depending on case definition and population, with rotator-cuff related pain rising steeply with age and overhead occupational or sporting load. The condition is a leading driver of musculoskeletal disability and work absence globally, which is why the marginal effectiveness of surgery (CSAW, FIMPACT) carries such large system-level cost implications.
Major Guidelines Side by Side
- Position on Surgery
- Strong recommendation AGAINST subacromial decompression for atraumatic SAPS
- First-Line Care
- Education, analgesia, exercise therapy, selective injection
- Evidence Level
- GRADE - high-certainty evidence from CSAW + FIMPACT
- Position on Surgery
- Surgery not routine; reserve for failure of prolonged structured non-operative care
- First-Line Care
- Structured physiotherapy first; injection as adjunct
- Evidence Level
- Aligned with Level 1 RCT evidence
- Position on Surgery
- No strong endorsement of routine acromioplasty for isolated SAPS
- First-Line Care
- Exercise-based rehabilitation, activity modification
- Evidence Level
- Moderate / limited strength recommendations
- Position on Surgery
- Emphasises conservative care; surgery individualised for clear structural pathology
- First-Line Care
- Supervised exercise, scapular and cuff rehabilitation
- Evidence Level
- Consensus informed by RCT evidence
Registry and Practice Variation
There is no dedicated arthroplasty-style registry for soft-tissue shoulder procedures, but national hospital-episode datasets show that publication of CSAW and FIMPACT was followed by a documented fall in subacromial decompression rates in several high-income health systems. Substantial practice variation persists: decompression remains comparatively common where it is bundled with diagnostic arthroscopy or driven by procedure-based remuneration, while it is increasingly deprescribed in systems that have adopted the GRADE recommendation against it. In limited-resource settings the emphasis is overwhelmingly on exercise and analgesia, with arthroscopy reserved for the few centres with the equipment and expertise.
- Frame as subacromial pain syndrome (SAPS), not a purely mechanical "impingement" requiring decompression
- Discuss CSAW and FIMPACT - decompression no better than placebo surgery
- Offer a structured, supervised exercise programme as the primary treatment
- Reserve referral for surgery for clear structural pathology after genuine failure of prolonged non-operative care
- Informed consent: explicitly convey the placebo-controlled trial evidence and the GRADE recommendation against surgery
- Documentation: record non-operative treatment timeline, injection response and patient expectations
- Failure to improve: an expected outcome if adequately counselled, not necessarily a complication
- Alternative options: document discussion of continued conservative management versus surgery
Specific points to document in consent discussion:
- Success rate: 75-85% good-excellent results, but 10-15% no improvement (based on older data; CSAW suggests lower benefit)
- Recent evidence: CSAW and FIMPACT trials showed no benefit over placebo surgery, and the 2019 BMJ Rapid Recommendation advises against surgery - explain why still considering it in this individual (clear structural factors, failed prolonged conservative treatment)
- Complications: Infection (less than 1%), stiffness (3-8%), persistent pain (10-15%), nerve injury (rare, less than 1%)
- Recovery: 3-6 months to full function, early physiotherapy critical
- Alternative: Continued conservative treatment is a valid option even after failed initial trial
Medicolegal claims often arise from failure to discuss realistic expectations and recent evidence.
MCQ Practice Points
Q: The subacromial space is bounded superiorly by which structure? A: Coracoacromial arch (anterior acromion, coracoid process, and coracoacromial ligament). The inferior boundary is the superior surface of the rotator cuff (supraspinatus primarily). Normal subacromial space height is 7-14mm.
Q: According to Bigliani classification, which acromion type has the highest association with rotator cuff tears? A: Type III (hooked acromion) - 70% association with rotator cuff tears vs 24% for Type II (curved) and 13% for Type I (flat). Type III represents 40% of the population.
Q: What is the most specific test for diagnosing subacromial impingement syndrome? A: Neer impingement injection test - 10ml lidocaine injected into subacromial space. Complete pain relief (greater than 50% reduction) on repeat provocative tests confirms subacromial pathology. Sensitivity 75-95%, specificity 40-70%. Also predicts response to surgical decompression.
Q: The CSAW trial (2018) compared arthroscopic subacromial decompression to what control? A: Sham surgery (arthroscopic portal incisions without decompression) and active monitoring. Result: No significant difference in outcomes at 6-12 months. This Level 1 evidence challenged routine use of acromioplasty and emphasized conservative treatment.
Q: What is the minimum duration of conservative treatment recommended before considering surgery for subacromial impingement? A: 3-6 months of structured conservative treatment (physiotherapy, NSAIDs, ± steroid injection). 6 months is optimal. 80-90% of patients respond to conservative treatment within this timeframe. Premature surgery (less than 3 months) is a common cause of poor outcomes.
Q: What is the most common cause of failed arthroscopic subacromial decompression? A: Operating on secondary impingement (functional impingement due to rotator cuff weakness or instability). These patients have positive impingement signs but no structural narrowing - surgery does not address the underlying problem. Always distinguish primary (structural) from secondary (functional) impingement before recommending surgery.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old painter presents with 6 months of progressive right shoulder pain. He has difficulty working overhead and has night pain. Examination shows positive Neer and Hawkins-Kennedy tests, painful arc 70-110°, full strength on rotator cuff testing. X-ray shows a Type III acromion with small anterior-inferior spur. How would you assess and manage this patient?”
“A 28-year-old competitive swimmer presents with 4 months of shoulder pain during training. She has positive impingement signs. You also note positive apprehension and relocation tests. MRI shows subacromial bursal fluid but no cuff tear, normal labrum. How would you approach this case?”
“A 58-year-old manual laborer has failed 9 months of conservative treatment for subacromial impingement. He's had physiotherapy, 2 steroid injections with temporary relief only. X-ray shows Type III acromion with prominent spur. MRI shows bursal thickening, no rotator cuff tear. He's requesting surgery. How do you counsel him about surgical options and evidence?”
Key Anatomy
- Subacromial space = 7-14mm height (under 7mm = impingement risk)
- Boundaries: Superior = coracoacromial arch, Inferior = rotator cuff (supraspinatus)
- Bigliani Type III (hooked) acromion = 70% cuff tear association (vs 13% Type I flat)
- Structures at risk: Supraspinatus tendon, long head biceps, subacromial bursa
Classification
- Neer Stage I (under 25) = edema/hemorrhage = reversible = conservative only
- Neer Stage II (25-40) = fibrosis/tendinitis = conservative first, surgery if failed 6 months
- Neer Stage III (over 40) = spurs/tears = often surgical
- Primary (structural: acromion, spurs, AC joint) vs Secondary (functional: cuff weakness, instability)
Clinical Tests
- Neer test (passive forward flexion) = pooled sensitivity 72%, specificity 60% (Hegedus 2012)
- Hawkins-Kennedy (IR at 90° flexion) = pooled sensitivity 79%, specificity 59%
- Painful arc more specific (76%) - cluster tests rather than rely on one
- Neer injection test (10ml lidocaine subacromial) = abolition of pain confirms subacromial source = BEST diagnostic confirmation
Treatment Algorithm
- ALL patients: Conservative first - NSAIDs, physio (cuff/scapular strengthening), activity modification
- Failed 4-6 weeks: Add subacromial steroid injection (short-term benefit only, max 3/year)
- Failed 3-6 months (optimal 6): Consider surgery IF positive injection test + structural abnormality
- Surgery: Arthroscopic decompression (acromioplasty + bursectomy) - 75-85% success but CSAW trial showed no benefit over sham
Surgical Pearls
- Resect 5-7mm anterior-inferior acromion (excessive = instability risk)
- Complete bursectomy for visualization
- Assess cuff from articular side first (exclude tears needing repair)
- Early ROM day 1 postop (prevent stiffness), strengthen from week 2
Evidence Base and Key Trials
CSAW Trial - Arthroscopic Subacromial Decompression vs Placebo Surgery
- Multicentre placebo-controlled RCT across 32 UK hospitals: 313 patients with at least 3 months of subacromial pain and intact cuff, randomised to arthroscopic decompression (n=106) vs investigational arthroscopy only / placebo (n=103) vs no treatment (n=104)
- Primary outcome Oxford Shoulder Score at 6 months: decompression 32.7 vs arthroscopy-only 34.2, mean difference -1.3 points (95% CI -3.9 to 1.3) - not significant
- Both surgical groups beat no treatment by ~3-4 points, below the pre-specified clinically important difference of 4.5 points
- All six study-related complications were frozen shoulder (two per group)
FIMPACT Trial - Decompression vs Placebo Arthroscopy vs Exercise
- Finnish three-group, double-blind, sham-controlled RCT: 210 patients with shoulder impingement randomised to arthroscopic decompression vs diagnostic arthroscopy (placebo) vs exercise therapy
- At 24 months, no clinically relevant difference between decompression and placebo arthroscopy in pain at rest (-4.6 points) or on activity (-9.0 points)
- The small advantage of decompression over exercise did not exceed the 15-point minimal clinically important difference and was biased in favour of surgery
- Reinforces CSAW: decompression provides no benefit over placebo arthroscopy
Acromial Morphology and Subacromial Enthesophytes (Bigliani classification)
- Anatomical study of 423 dried scapulae applying the Bigliani classification (originally described in Orthop Trans 1986) plus a fourth convex type
- Distribution: type I flat 12.1%, type II curved 56.5%, type III hooked 28.8%, type IV convex 2.6%
- Coracoacromial-ligament enthesophytes were present in 37.7% of type III acromions versus 7.9% of type II and 2% of type I (p less than 0.05)
- Type III morphology with an enthesophyte is the combination most strongly associated with impingement and cuff tears
Corticosteroid Injections for Shoulder Pain - Cochrane Review
- Systematic review of 26 RCTs of corticosteroid injection for shoulder pain
- For rotator cuff disease, subacromial steroid showed a small benefit over placebo in some trials
- Pooled results of three trials showed no benefit of subacromial steroid over NSAID
- Any effect was small and not well maintained; methodological quality was variable
Ketola RCT - Arthroscopic Acromioplasty vs Supervised Exercise
- RCT of 140 patients with stage II impingement: supervised exercise alone (n=70) vs acromioplasty followed by the same exercise programme (n=70)
- At 24 months both groups improved with no significant difference in self-reported pain (p=0.65)
- Adding acromioplasty was considerably more costly with no extra clinical benefit
- Five-year follow-up (Bone Joint Res 2013, doi 10.1302/2046-3758.27.2000163) confirmed sustained improvement in both groups and no advantage for surgery
Diagnostic Accuracy of Shoulder Physical Examination Tests
- Systematic review with meta-analysis of individual shoulder examination tests (QUADAS-2 appraised)
- Subacromial impingement: Neer pooled sensitivity 72% / specificity 60%; Hawkins-Kennedy 79% / 59%; painful arc 53% / 76%
- No single test reliably makes a pathognomonic diagnosis; combinations add accuracy only marginally
- Emphasises a comprehensive history-plus-examination approach rather than reliance on one provocation test
BMJ Rapid Recommendation - Subacromial Decompression for Shoulder Pain
- GRADE-based international clinical practice guideline built on the CSAW and FIMPACT placebo-controlled trials
- Strong recommendation AGAINST subacromial decompression surgery for atraumatic subacromial pain syndrome
- Surgery gave no important improvement in pain, function or quality of life versus placebo surgery or other options
- Frozen shoulder may be more common after surgery; the panel judged almost all informed patients would decline the operation
Ketola Five-Year Follow-up - No Long-Term Benefit of Acromioplasty
- Five-year results of the 140-patient RCT (exercise alone vs acromioplasty plus exercise) for stage II impingement
- Mean VAS pain fell from ~6.5 to ~2 in both groups with no significant between-group difference
- Improvement continued between the two-year and five-year timepoints in both arms
- Acromioplasty was judged not cost-effective over structured exercise