Patella Alta (high-riding) and Patella Baja (low-riding) | Measured on the true lateral radiograph at 30 degrees flexion | Three main ratios, not interchangeable | Alta drives instability, Baja limits flexion
- A true lateral radiograph at approximately 30 degrees of knee flexion is required for accurate patellar height measurement - the femoral condyles should overlap perfectly
- Patella alta (high-riding patella) is the more common abnormality and is a recognised risk factor for recurrent patellar dislocation because the patella engages the trochlea later than normal during flexion
- Patella baja (low-riding patella) restricts knee flexion, increases patellofemoral contact pressures, and is most often seen after total knee arthroplasty, tibial tubercle osteotomy, or patellar tendon shortening
- The three ratios are NOT interchangeable - a knee classified as alta by one index may be normal by another, so state which index you are using and use the same one for serial follow-up
- Management depends on the cause and severity: instability from alta may need distalisation (tibial tubercle transfer), while baja may require tendon lengthening or Z-plasty in refractory cases
- “When asked to measure patellar height on a lateral knee X-ray in the viva, name the ratio you are using, draw the lines, and state whether it is alta, normal, or baja with the threshold value
- “Patella alta is a key modifiable risk factor in patellofemoral instability - alongside trochlear dysplasia, TT-TG distance, and patellar tilt - know how they interact
- “Post-TKA patella baja is usually iatrogenic from distal femoral resection level or scarring - mention it when discussing TKA complications
Patellar height is measured on a true lateral radiograph with the knee at approximately 30 degrees of flexion and the femoral condyles perfectly overlapped. An angled or rotated view gives misleading ratios. State the view quality before quoting a number.
The three main ratios (Insall-Salvati, Caton-Deschamps, Blackburne-Peel) do not classify patellar height consistently - a patient may be "alta" by one and "normal" by another. Always name which index you are using and use the same one for serial follow-up.
A high-riding patella engages the trochlear groove later in the flexion arc, spending more time in the unstable early-flexion zone. It is a correctable risk factor in recurrent patellar dislocation alongside trochlear dysplasia and an elevated TT-TG distance.
Post-TKA patella baja is the commonest acquired form and results from the level of distal femoral resection, patellar tendon scarring, or component positioning. It causes limited flexion, anterior knee pain, and difficulty with revision surgery.
Overview
Patellar height describes where the patella sits relative to the femoral trochlea and tibial plateau on the lateral knee radiograph. When the patella sits too high it is called patella alta; when it sits too low it is patella baja. Both are important because they alter the biomechanics of the patellofemoral joint and have specific clinical consequences.
Patella alta is the more common abnormality and is a well-established risk factor for recurrent patellar instability. The high-riding patella does not engage the trochlear groove until later in the flexion arc, meaning that through the range where most daily activities occur the patella is poorly constrained. Patella baja is less common but is an important iatrogenic problem after knee surgery - particularly total knee arthroplasty and tibial tubercle osteotomy - and causes restricted flexion, anterior knee pain, and difficulty with future revision surgery.
Three radiographic ratios are used to classify patellar height: the Insall-Salvati, Caton-Deschamps, and Blackburne-Peel indices. They are measured on a true lateral radiograph and each has different strengths and limitations - critically, they are not interchangeable, and a patient classified as alta by one may be normal by another.
For the exam, three themes recur: how to measure patellar height accurately (which view, which ratio, and the thresholds), what patella alta and baja mean clinically (instability versus stiffness), and what to do about them (when and how to correct patellar height surgically).
Anatomy and Pathophysiology
Normal patellofemoral biomechanics
The patella acts as a sesamoid bone within the quadriceps extensor mechanism, increasing the moment arm of the quadriceps by up to 30 percent and distributing compressive forces across the femoral trochlea. During knee flexion, the patella tracks within the trochlear groove, engaging the groove at approximately 20 to 30 degrees of flexion and deepening its congruence as flexion increases.
The stability of the patella depends on both static constraints (trochlear geometry, MPFL, medial patellofemoral complex, bony architecture) and dynamic constraints (vastus medialis oblique, quadriceps balance). Patellar height directly affects the timing of trochlear engagement.
Patella alta: biomechanical consequence
When the patella sits too high (a long patellar tendon), it enters the trochlear groove later in the flexion arc - typically beyond 30 to 40 degrees rather than at 20 degrees. This means that through the first 30 to 40 degrees of flexion, the patella is perched above the groove and relies almost entirely on soft-tissue restraints (principally the MPFL) for stability. The practical consequence is a significantly increased risk of lateral patellar dislocation, especially in early flexion or with a valgus and external rotation force.
Patella alta also increases patellofemoral contact pressures in mid-flexion because the patella engages a smaller, more proximal portion of the trochlea, concentrating load.
Patella baja: biomechanical consequence
When the patella sits too low (a short patellar tendon), the patella is driven into the trochlea earlier and with greater force during flexion. This causes:
- Increased patellofemoral contact pressures, leading to anterior knee pain and early arthrosis
- Restricted knee flexion because the extensor mechanism tightens early
- Shortened extensor lever arm, reducing quadriceps efficiency
In total knee arthroplasty, patella baja makes exposure difficult, increases the risk of patellar tendon avulsion during surgery, and can lead to patellar clunk or impingement against the femoral component.
Severe patella baja significantly complicates revision TKA. The shortened extensor mechanism limits surgical exposure, raising the risk of intraoperative patellar tendon avulsion. Strategies include a tibial tubercle osteotomy, quadriceps snip, or V-Y turndown - know these names for the exam.
Classification of Patellar Height
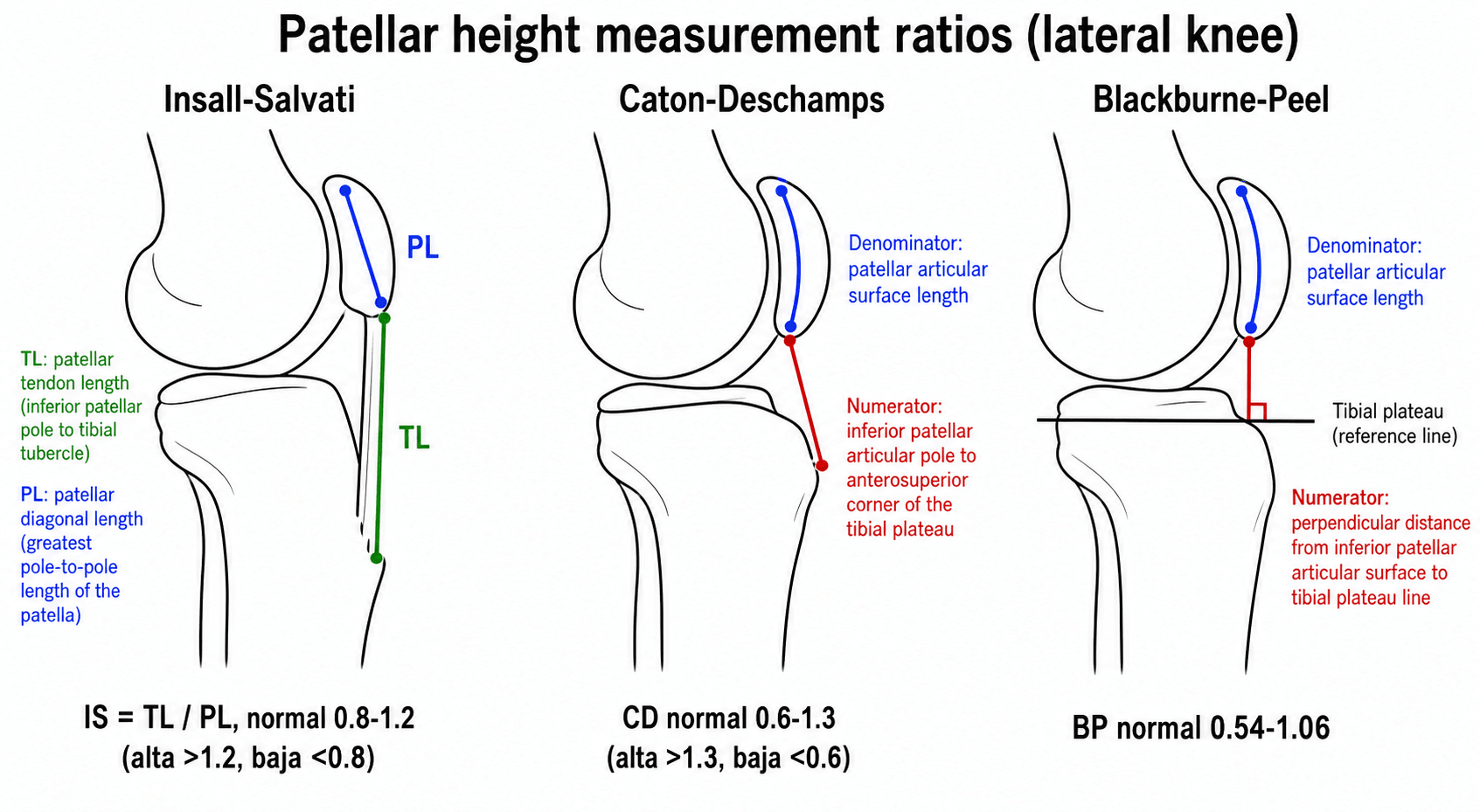
Patellar height is classified using radiographic ratios measured on a true lateral knee radiograph taken at approximately 30 degrees of knee flexion with the femoral condyles perfectly overlapped. The correct technique is critical because rotation and flexion angle change the measurements.
- Numerator
- Patellar tendon length (from lower patellar pole to tibial tubercle insertion)
- Denominator
- Patellar diagonal length (greatest pole-to-pole length)
- Normal range
- 0.8 to 1.2
- Alta threshold
- Greater than 1.2
- Baja threshold
- Less than 0.8
- Strength / weakness
- Most widely taught and recognised. Independent of knee flexion angle. Limitation: altered by patellar tendon disease (tendonitis, tendinosis, prior harvest) and patellar morphology
- Numerator
- Patellar tendon length
- Denominator
- Patellar articular surface length (not diagonal)
- Normal range
- Variable by study
- Alta threshold
- Uses articular surface rather than full diagonal
- Baja threshold
- Uses articular surface rather than full diagonal
- Strength / weakness
- Accounts for patellar shape variability. Less commonly cited in exams
- Numerator
- Distance from inferior patellar pole to anterosuperior corner of the tibial plateau
- Denominator
- Length of the patellar articular surface
- Normal range
- 0.6 to 1.3
- Alta threshold
- Greater than 1.3
- Baja threshold
- Less than 0.6
- Strength / weakness
- Reflects the functional relationship between patella and tibia. Preferred by many for pre-operative planning. Changes with tibial slope and tubercle position
- Numerator
- Perpendicular distance from the inferior patellar articular surface to the tibial plateau line
- Denominator
- Length of the patellar articular surface
- Normal range
- 0.54 to 1.06
- Alta threshold
- Greater than 1.06
- Baja threshold
- Less than 0.54
- Strength / weakness
- Uses a perpendicular measurement line rather than along the tendon. Less affected by inferior pole osteophytes. Can be harder to reproduce reliably
If asked "which ratio do you use?", a strong viva answer names the Insall-Salvati as the most recognised and then explains why the Caton-Deschamps may be preferred in pre-operative planning for distalisation surgery (because it reflects the functional patellofemoral relationship). The key point is that the ratios are not interchangeable - state which one you are using and apply its specific thresholds.
The non-interchangeability problem
A landmark study (Hunter et al., 2024) demonstrated that the three common patellar height indices do not consistently classify the same knee as alta, normal, or baja. The Insall-Salvati ratio can label a knee as alta while the Caton-Deschamps places it in the normal range, and vice versa. This happens because each ratio measures a different anatomical relationship:
- The IS ratio reflects tendon length relative to patellar size - so a patella with an unusually long diagonal will give a low IS ratio even if the functional height is normal
- The CD and BP ratios reflect functional engagement with the trochlea - but depend on accurate identification of the tibial plateau reference point
For clinical practice and exam answers, the important principle is: pick one index and use it consistently for that patient, and always name the index when communicating patellar height.
Alternative and Direct Measures of Patellar Height
The Insall-Salvati, Caton-Deschamps and Blackburne-Peel ratios are the three you must know, but a candidate who can name a further method or the direct cartilage measure scores well, especially when the standard ratios are confounded by patellar shape or unclear tibial landmarks.
- What it measures
- Patellar tendon length divided by the patellar ARTICULAR surface length (not the full diagonal)
- When it helps
- Corrects the standard Insall-Salvati when the patella has a long non-articular distal pole that falsely lowers the ratio; abnormal above about 2.0
- What it measures
- A lateral view at 90 degrees of flexion: a line along the anterior femoral cortex - the superior patellar pole normally lies at or just below this line
- When it helps
- Useful when the tibial landmarks are obscured (e.g. fracture, hardware); the patella projecting above the line indicates alta
- What it measures
- Direct measure of cartilage engagement: length of patellar cartilage overlapping trochlear cartilage divided by patellar cartilage length on sagittal MRI
- When it helps
- Measures TRUE patellofemoral engagement rather than an indirect bony ratio; a low value (roughly under 0.28 to 0.32) indicates alta and is unaffected by tendon or patellar bony morphology
The radiographic ratios are all INDIRECT - they infer engagement from bony or tendon landmarks. The MRI patellotrochlear index is the DIRECT measure of how much patellar cartilage actually overlaps trochlear cartilage, so it is the one to quote when the radiographic ratios disagree or when tendon or patellar morphology is abnormal. Knowing one alternative (the modified Insall-Salvati or Labelle-Laurin) and the direct MRI index sets a strong answer apart.
Clinical Presentation
Patella Alta
Patella alta may be asymptomatic and discovered incidentally, or it may present with features of patellofemoral instability:
The hallmark presentation. The patient describes the patella "popping out" to the lateral side, typically in early knee flexion (stepping off a kerb, pivoting, or dancing). Patella alta is one of four major risk factors alongside trochlear dysplasia, elevated TT-TG distance, and patellar tilt. Multiple risk factors compound the instability risk.
Increased patellofemoral contact pressures from late trochlear engagement cause retropatellar pain, especially on stairs, squatting, or prolonged sitting. Pain may be vague and attributed to "chondromalacia" if patellar height is not measured.
On active extension from a seated position, the patella may visibly track laterally as it leaves the trochlea in terminal extension - the so-called J-sign. This is a clinical clue to alta with or without trochlear dysplasia.
Positive patellar apprehension on lateral displacement in early flexion suggests instability. Combined with a lateral radiograph confirming alta, this strengthens the case for surgical stabilisation that includes distalisation.
Patella Baja
Patella baja typically presents after knee surgery or trauma and causes symptoms related to extensor mechanism tightness:
- Limited knee flexion - the most common symptom. The tight extensor mechanism prevents deep bending. Post-TKA patients who plateau at 70 to 90 degrees of flexion despite physiotherapy should have patellar height assessed.
- Anterior knee pain - increased patellofemoral contact pressures from the patella being driven into the trochlea during flexion.
- Extensor lag or weakness - a shortened lever arm reduces quadriceps mechanical advantage.
- Difficulty with stairs and rising from a chair - functional impairment from limited flexion and reduced extensor power.
In severe cases (often post-traumatic or after complex revision surgery), the patient may have a stiff knee with a palpably shortened patellar tendon.
Infrapatellar Contracture Syndrome
Infrapatellar contracture syndrome is the most important acquired cause of severe patella baja and is asked about directly in the viva. It is an exuberant fibrotic response of the anterior knee soft tissues - the infrapatellar fat pad, the patellar tendon and the peri-patellar retinaculum - after knee surgery, trauma or prolonged immobilisation. The contracting scar tethers the patella distally, producing progressive acquired baja together with loss of BOTH flexion and extension.
- Features
- Painful, warm, swollen knee with a quadriceps lag and disproportionate global loss of motion weeks after surgery
- Management principle
- Recognise early; anti-inflammatories and gentle supervised motion - do NOT operate during this inflammatory phase
- Features
- Marked fibrosis, worsening flexion and extension loss, a tight patellar tendon, restricted patellar glide and developing baja
- Management principle
- Continue non-operative care; surgery during active inflammation tends to re-scar
- Features
- Mature fibrosis with fixed patella baja, a low-riding immobile patella and patellofemoral arthrosis
- Management principle
- Once quiescent, arthroscopic or open release of scar and fat pad; severe fixed baja may need patellar tendon lengthening (Z-plasty)
The best treatment is prevention: early protected mobilisation after knee surgery and avoiding prolonged immobilisation. The Caton-Deschamps index falling on serial films confirms the progressive baja, and management is matched to the phase - aggressive physiotherapy and anti-inflammatories while the process is active, and surgical release reserved for the burnt-out stage.
The classic trap is to operate on an infrapatellar contracture during its active inflammatory phase - this provokes further scarring and worse stiffness. Treat the inflammation, restore motion non-operatively, and reserve release or patellar tendon lengthening (Z-plasty) for the residual burnt-out phase with established fixed baja.
Investigations
Plain radiography (first-line)
The true lateral knee radiograph at approximately 30 degrees of flexion is the standard investigation for patellar height. The femoral condyles should overlap perfectly; any rotation introduces error.
On the lateral view, the examiner can draw the lines for the Insall-Salvati, Caton-Deschamps, and Blackburne-Peel ratios and calculate patellar height directly.
Additional views:
- What it shows
- Patellar height ratios, trochlear morphology
- Key points
- Must have condylar overlap - rotate and re-shoot if not perfect
- What it shows
- Overall alignment, patellar position, tibiofemoral joint space
- Key points
- Patella may appear high or low on AP but height must be confirmed on lateral
- What it shows
- Patellar tilt, subluxation, trochlear dysplasia grade
- Key points
- Does not measure height but assesses patellar tracking in axial plane
- What it shows
- Overall limb alignment, mechanical axis
- Key points
- Useful when planning simultaneous corrective osteotomy with tubercle transfer
Cross-sectional imaging
- MRI is the gold standard for assessing the MPFL, trochlear cartilage, and patellar articular surface. It can also measure patellar height (the same ratios applied to sagittal MRI sequences) and the TT-TG distance (tibial tubercle to trochlear groove), which guides whether medialisation, distalisation, or both are needed. MRI also identifies patellar tendon pathology (tendinosis, partial tears) that may affect the Insall-Salvati ratio.
- CT is used for TT-TG measurement in some centres and for surgical planning in complex cases with prior hardware or malunion.
Measurement workflow for the exam
- Confirm the view is a true lateral with condylar overlap
- Choose and name the ratio you will use (Insall-Salvati is the default)
- Identify the landmarks (lower patellar pole, tibial tubercle, patellar diagonal, tibial plateau)
- Measure and state the threshold (IS: normal 0.8 to 1.2, alta above 1.2, baja below 0.8)
- Comment on other relevant features (trochlear dysplasia, patellar tilt, osteoarthritis)


Management
Patella Alta
Management depends on whether the alta is symptomatic and whether instability is the presenting problem.
- Management
- No treatment. Physiotherapy for quadriceps and VMO strengthening if mild symptoms
- Key points
- Not all alta needs surgery - treat the patient, not the number
- Management
- MPFL reconstruction PLUS consideration of tibial tubercle distalisation if IS ratio is significantly elevated (typically above 1.3 to 1.5)
- Key points
- Isolated MPFL reconstruction may fail if alta is severe - the tendon is still too long and the patella still engages late. Distalisation combined with medialisation addresses both the height and the TT-TG distance
- Management
- Physiotherapy first-line. Activity modification. Patellar taping or bracing
- Key points
- Surgical distalisation for anterior knee pain alone is controversial and less evidence-based than for instability
Tibial tubercle distalisation
When patellar height correction is indicated, the standard approach is a tibial tubercle osteotomy with distal transfer (often combined with medialisation to correct an elevated TT-TG distance):
- An osteotomy of the tibial tubercle is performed (usually a flat or step-cut)
- The tubercle fragment is slid distally by the calculated amount (based on the ratio excess above normal)
- Fixed with screws in the new position
- The Caton-Deschamps index is often preferred for planning the amount of distalisation because it directly measures the functional relationship
Important: overcorrection to patella baja must be avoided - aim for a normal CD index (around 1.0), not the lowest possible position. The amount of distalisation is calculated pre-operatively from the measured index.
Patella Baja
- Management
- Observation, physiotherapy for gradual flexion improvement, activity modification
- Key points
- Most post-TKA baja is mild and does not require surgical correction
- Management
- Revision surgery: consider component revision with improved joint line restoration, patellar tendon lengthening
- Key points
- The joint line should be restored to its anatomical level. A distal femoral augment or use of a thicker polyethylene insert may be needed
- Management
- Patellar tendon Z-plasty or V-Y lengthening with careful post-operative bracing in flexion
- Key points
- Modified Z-plasty (Weber et al.) has shown good results for severe post-surgical baja. Risk of re-shortening or extensor lag
- Management
- Tibial tubercle osteotomy for exposure, proximal transfer if baja is severe
- Key points
- The tubercle osteotomy provides exposure and can be repositioned more proximally during closure. Fix with screws and protect post-operatively
In the viva, when asked about managing patella alta in the setting of instability, the key algorithm is: "Is the TT-TG elevated? Is the patellar height elevated? Is there trochlear dysplasia?" - the surgical plan (MPFL reconstruction, tibial tubercle transfer with medialisation, distalisation, or trochleoplasty) depends on combining these factors.
Complications
Complications of untreated patella alta
- Recurrent patellar dislocation with cumulative damage to the patellar articular surface and the MPFL
- Patellofemoral osteoarthritis from chronic instability episodes, abnormal tracking, and increased contact pressures
- Psychological impact and activity restriction from fear of dislocation
- Quadriceps wasting and deconditioning from activity avoidance
Complications of untreated patella baja
- Progressive stiffness with permanent loss of knee flexion
- Patellofemoral arthrosis from chronically elevated contact pressures
- Functional disability (difficulty with stairs, sitting, driving)
- Patellar tendon rupture (rare, in severe cases with chronic tendon shortening and degeneration)
Complications of surgical treatment
- Specific complications
- Non-union or delayed union of the tubercle fragment, compartment syndrome (anterior), overcorrection to patella baja, hardware prominence requiring removal
- Prevention
- Adequate screw fixation (typically two cortical screws), maintain distal periosteal hinge for vascularity, post-operative bracing, calculate transfer distance precisely
- Specific complications
- Extensor lag, tendon re-rupture, re-shortening (recurrent baja), infection
- Prevention
- Careful tissue handling, protected post-operative mobilisation in flexion brace, patient selection
- Specific complications
- Graft failure, overconstraint, patellar fracture (from tunnel placement), arthrofibrosis
- Prevention
- Anatomical femoral tunnel placement, appropriate graft tensioning (not too tight), combined approach when alta is significant
Anterior compartment syndrome is a recognised complication of tibial tubercle osteotomy. The procedure breaches the anterior compartment and bleeding can raise compartment pressure. Monitor the patient closely post-operatively and maintain a low threshold for compartment pressure measurement or fasciotomy if the patient develops disproportionate pain, swelling, or neurological signs in the anterior compartment distribution.
Clinical Relevance
Patellar height assessment is a practical skill that appears across multiple exam stations. In the radiology viva, you may be handed a lateral knee X-ray and asked to measure and interpret patellar height - the key is a systematic approach: name the ratio, draw the lines, apply the thresholds, and relate the finding to the clinical picture. In the clinical viva, patella alta is an integral part of the patellar instability workup alongside trochlear dysplasia, TT-TG distance, and patellar tilt - knowing how these factors interact to determine the surgical plan is essential. In the basic science viva, the biomechanics of the patellofemoral joint and how patellar height affects trochlear engagement and contact pressures links anatomy to clinical decision-making.
Patella baja is most often encountered in the revision TKA setting where it complicates exposure and limits outcomes - knowing the strategies for dealing with a shortened extensor mechanism (tibial tubercle osteotomy, quadriceps snip, V-Y turndown) is a common exam question.
The key message for the exam: patellar height is a measurable, correctable risk factor that should be assessed in every patient with patellar instability and every post-TKA patient with limited flexion. Know the ratios, their thresholds, and their limitations.
Guidelines, Registries and Global Practice
- No single international guideline exists specifically for patellar height measurement or correction. The Insall-Salvati, Caton-Deschamps, and Blackburne-Peel ratios are the universally accepted radiographic indices, taught across all training programmes globally.
- Patellar instability management (which incorporates patellar height correction) is addressed by the International Patellofemoral Study Group (IPFSG) consensus statements and in the patellofemoral instability guidelines published by various national orthopaedic societies (including AAOS, BOA/BOAST, and DGOOC). The consensus is that patella alta should be assessed and corrected when significant in the setting of recurrent instability, typically as part of a tibial tubercle osteotomy with distalisation.
- TT-TG distance thresholds vary slightly between centres but the general consensus is: normal approximately 10 to 15 mm; surgical correction considered above 20 mm. The threshold may differ between CT-based and MRI-based measurements (CT values tend to be higher by 2 to 4 mm).
- Post-TKA patella baja is increasingly recognised as an outcome measure in arthroplasty registries. The National Joint Registry (NJR, UK) and Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) report on patellofemoral complications and revision rates. Joint line preservation during TKA is the key preventative measure and is emphasised in surgical technique guides from all major implant manufacturers.
- Global practice variation exists in the choice of patellar height index: the Insall-Salvati remains the most widely used in examinations and initial assessment, while the Caton-Deschamps is increasingly preferred for pre-operative planning of distalisation surgery in Europe. In Asian countries where patellofemoral instability surgery is common, the modified Insall-Salvati and CD indices are both used with population-specific normative data that may differ from Western reference ranges.
Memory aids
ICBPatellar Height Ratios
Hook:ICB - Insall, Caton, Blackburne - three ratios, all on the lateral view, and they are NOT interchangeable.
HIGHCauses of Patella Alta
Hook:The patella sits HIGH when the tendon is too long - congenital, growth-plate, or instability-related.
LOWCauses of Patella Baja
Hook:The patella sits LOW when the tendon shortens or is pulled down - surgery, scarring, or trauma.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“The examiner shows you a lateral knee radiograph of a 22-year-old woman with recurrent patellar dislocation and asks you to measure patellar height.”
“A 24-year-old woman has had four patellar dislocations. Her Insall-Salvati ratio is 1.45, TT-TG distance is 22 mm, and she has type B trochlear dysplasia on the Dejour classification. How do you plan her surgical management?”
“A 68-year-old woman presents 12 months after a primary total knee arthroplasty with anterior knee pain and flexion limited to 80 degrees despite physiotherapy. Her post-operative lateral radiograph shows a Caton-Deschamps index of 0.35. How do you manage this?”
Measurement Essentials
- True lateral radiograph, 30 degrees flexion, femoral condyles overlapped
- Insall-Salvati: tendon length / patellar diagonal. Normal 0.8-1.2
- Caton-Deschamps: lower pole to plateau / articular surface. Normal 0.6-1.3
- Blackburne-Peel: perpendicular to plateau / articular surface. Normal 0.54-1.06
- The three ratios are NOT interchangeable - name the one you use
Patella Alta
- High-riding patella from a long patellar tendon
- Major risk factor for recurrent patellar dislocation
- Patella engages trochlea LATE - unstable in early flexion
- Surgical: tibial tubercle distalisation (often with medialisation for TT-TG)
- Correct the height AND the instability (MPFL reconstruction may be needed)
Patella Baja
- Low-riding patella from a short patellar tendon
- Commonest after TKA, tibial tubercle osteotomy, or infrapatellar scarring
- Causes limited flexion, anterior knee pain, increased PF contact pressures
- Mild: observe and physiotherapy. Severe: tendon lengthening or joint line revision
- Complicates revision TKA exposure - know tibial tubercle osteotomy, quadriceps snip
Red Flags / Exam Traps
- Always name which ratio you are using - do not mix thresholds
- Patella alta: TT-TG + trochlear dysplasia + alta = combined surgical plan
- Post-TKA stiffness: check patellar height before attributing to arthrofibrosis
- Tibial tubercle osteotomy: risk of compartment syndrome (anterior)
- Avoid overcorrection - aim for normal height, not the extreme
Evidence
Common Radiographic Indices Do Not Consistently Identify Patella Alta and Lack Interchangeability
- Compared the Blackburne-Peel (BPI), Caton-Deschamps (CDI) and Insall-Salvati (ISR) indices on 100 lateral knee radiographs to assess agreement
- Patella alta was identified in 15 knees by BPI, 15 by CDI but 25 by ISR - and only 7 knees were classified alta by all three indices
- Inter-index correlations were modest (R = 0.71 BPI-CDI, 0.33 BPI-ISR, 0.29 CDI-ISR), so conversions between indices are not equivalent
- The three indices do NOT consistently classify the same knee as alta, normal or baja
Reliability and Interobserver Variability in Radiological Patellar Height Ratios
- Assessed interobserver reliability of five patellar-height ratios (Insall-Salvati, modified Insall-Salvati, Blackburne-Peel, Caton-Deschamps, Labelle-Laurin) on 22 knees
- Interobserver reliability was good for all (correlation coefficients 0.81-0.92), but the height classification (alta/normal/baja) differed between ratios in 68% of patients
- A patella could be classified alta, normal OR baja depending on which ratio was used
- The authors RECOMMEND the Blackburne-Peel method - it showed the lowest interobserver variability and best discriminated alta/normal/baja
Treatment of Patella Baja by a Modified Z-Plasty
- Described a modified Z-plasty for patellar-tendon lengthening in patella baja, using four reins (rather than the conventional two) to allow multifold tendon overlap
- Case series of 4 patients: median Caton-Deschamps ratio corrected from 0.53 to 1.03 at a median 34-month follow-up
- Median knee flexion improved from 108° to 143°; Lysholm 49→91, Tegner 2→6, and VAS pain 8.5→1
- No complications and no extension lag were observed; the technique is useful when allografts are unavailable