Isolated PF replacement | Young active patients | Joint-preserving alternative
- Strict patient selection: isolated PF arthritis, under 65 years, normal tibiofemoral joints
- Contraindications: inflammatory arthritis, TF OA grade greater than 2, patella baja, severe trochlear dysplasia
- Modern onlay (deeper-grooved, anterior-femur-resurfacing) designs show better survival than first-generation inlay designs (~82-90% vs ~70-75% at 10 years)
- Conversion to TKA is straightforward and uses standard primary TKA components in over 90% of cases
- Joint registries (NJR, AOANJRR): PFA revision rate roughly 2-3 times higher than primary TKA but bone stock preserved
- “Key indication: isolated PF arthritis in young active patient with normal TF compartments
- “Main reason for revision: progression of TF arthritis (not implant failure)
- “Outcomes comparable to TKA for pain relief but better ROM and function
- “Registry data favour cemented fixation and modern onlay (deeper-grooved) trochlear designs
Strict criteria essential. Isolated PF arthritis confirmed on weight-bearing radiographs and standing alignment films. TF compartments must be pristine. Under 65 years ideal. No inflammatory disease.
Absolute: Inflammatory arthritis, TF OA Outerbridge grade greater than 2, patella baja. Relative: Severe trochlear dysplasia (Dejour type D), obesity BMI over 35, high-demand occupation.
Precise component positioning critical. Trochlear component must match native groove anatomy. Patellar tracking assessed throughout ROM. Overstuffing causes anterior knee pain and stiffness.
Conversion to TKA straightforward. PFA preserves bone stock and femoral condyles. Use standard TKA components. Discuss conversion risk (15-25% at 10 years) during consent.
- Joint Status
- Isolated PF OA, pristine TF joints
- Treatment Choice
- Patellofemoral arthroplasty
- Key Pearl
- Preserves TF compartments, better ROM than TKA
- Joint Status
- PF OA + Outerbridge grade 2 TF changes
- Treatment Choice
- Consider TKA vs unicompartmental options
- Key Pearl
- Risk of early PFA failure due to TF progression
- Joint Status
- Tricompartmental arthritis
- Treatment Choice
- Total knee arthroplasty
- Key Pearl
- PFA contraindicated with TF involvement
ISOLATEDPFA Patient Selection Criteria
Hook:PFA success requires ISOLATED disease - one compartment only, with perfect patient selection!
NO-PFAPFA Contraindications
Hook:Say NO to PFA when inflammatory disease or TF involvement present - these guarantee failure!
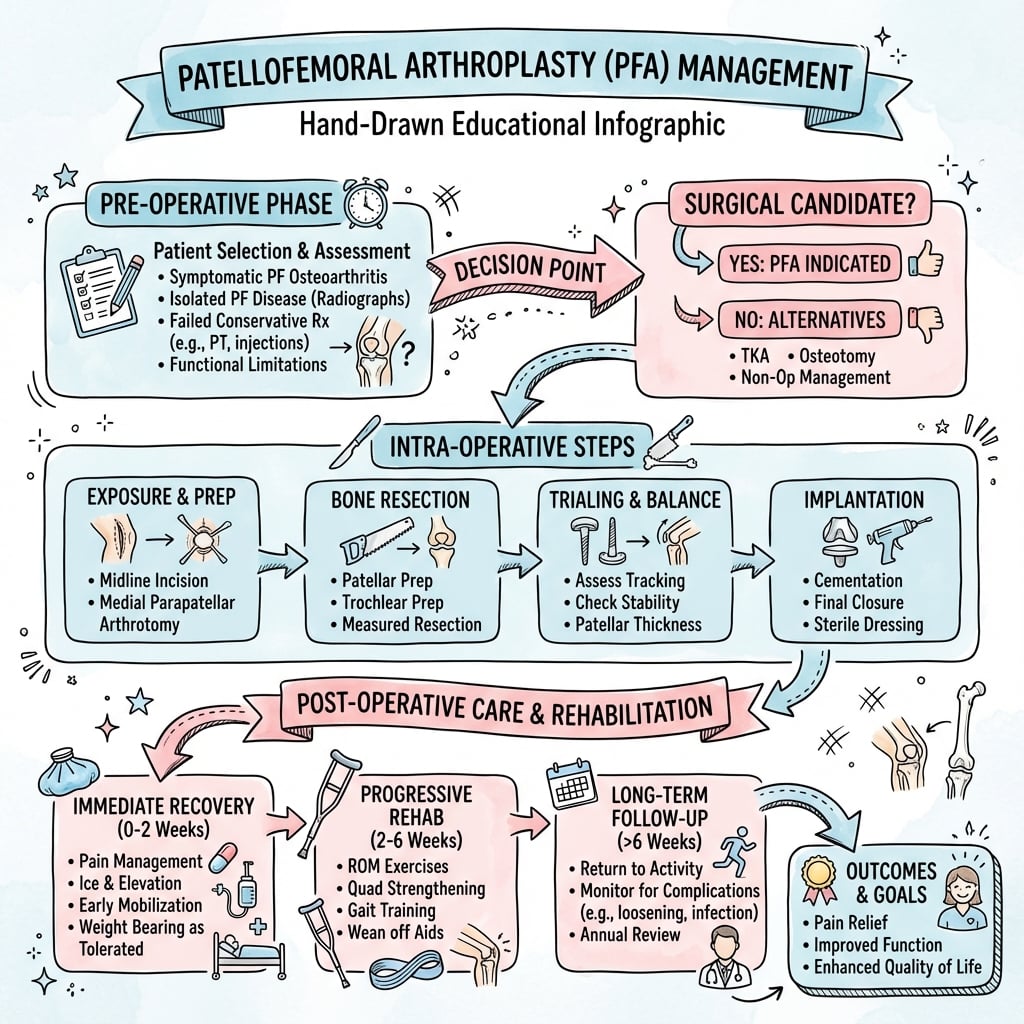
Overview and Epidemiology
Patellofemoral arthroplasty is a joint-preserving alternative to total knee arthroplasty for patients with isolated patellofemoral arthritis. The procedure involves replacement of the patellofemoral joint while preserving the native tibiofemoral compartments, femoral condyles, and cruciate ligaments.
Early PFA designs (1970s-1990s) had poor outcomes with high failure rates, leading to abandonment of the procedure. Modern implant designs introduced after 2000, particularly onlay (anterior-femur-resurfacing, deeper-grooved) trochlear components, have dramatically improved survival rates to approach those of unicompartmental knee arthroplasty.
- Age 40-60 years (though can extend to 70)
- Isolated anterior knee pain
- Failed conservative management over 6 months
- Radiographic isolated PF arthritis
- Active lifestyle goals
- BMI under 35
- Realistic expectations
- Isolated PF OA: 10% of all knee OA
- Post-traumatic PF arthritis common after fracture
- Trochlear dysplasia association in 50% cases
- Patella alta/baja alter mechanics
- Prior realignment surgery common history
Anatomy and Biomechanics
The patellofemoral joint experiences the highest contact stresses in the body (up to 6 times body weight during stair descent). The trochlear groove anatomy is highly variable between individuals, making component fit critical for successful PFA outcomes. Trochlear dysplasia (Dejour classification) must be assessed pre-operatively.
- Clinical Significance
- Normal depth 3-5mm, dysplasia less than 3mm
- Surgical Implication
- Shallow groove limits inlay component seating
- Clinical Significance
- Normal 138-145 degrees, dysplasia over 145 degrees
- Surgical Implication
- Wide angle increases lateral tracking forces
- Clinical Significance
- Normal 0.8-1.2, alta over 1.2, baja under 0.8
- Surgical Implication
- Baja is contraindication, alta needs lateral release
- Clinical Significance
- Normal under 20 degrees, abnormal over 20 degrees
- Surgical Implication
- High Q-angle may require tibial tubercle osteotomy
Patellofemoral Kinematics
The patella engages the trochlear groove at approximately 20 degrees of flexion. Contact area increases with flexion, shifting from inferior pole (30 degrees) to superior pole (90 degrees). Maximum contact stress occurs at 45-60 degrees flexion during activities like stair climbing.
- Walking: 0.5 times body weight
- Stair climbing: 3-4 times body weight
- Stair descent: 5-6 times body weight
- Squatting: 7-8 times body weight
- Running: 8-10 times body weight
- 20-30° flexion: Inferior pole contact
- 45-60° flexion: Mid-patellar ridge contact (peak stress)
- 90° flexion: Superior pole contact
- Over 120° flexion: Odd facet engagement
- Component must replicate native contact patterns
Classification Systems
Dejour Classification of Trochlear Dysplasia
- Features
- Crossing sign only, normal depth
- PFA Suitability
- Suitable for PFA
- Management
- A standard component tracks well
- Features
- Flat/convex trochlea, sulcus angle over 145°
- PFA Suitability
- Challenging for PFA
- Management
- May require onlay design or TKA
- Features
- Asymmetric lateral facet, cliff sign
- PFA Suitability
- Challenging for PFA
- Management
- Consider trochleoplasty alternative
- Features
- Cliff + vertical link + asymmetry
- PFA Suitability
- Contraindication to PFA
- Management
- TKA or trochleoplasty preferred
Severe dysplasia (Dejour C and D) is a relative to absolute contraindication for PFA. The abnormal trochlear anatomy makes component positioning difficult and increases risk of maltracking and instability. Types C and D have 3-4 times higher revision rates.
The choice between inlay and onlay designs has dramatic impact on outcomes. Modern, deeper-grooved trochlear designs (e.g. Avon, Journey PFJ) restore native trochlear geometry and constrain the patella, with pooled registry 10-year survival around 82-90%. First-generation designs with shallow, unconstrained grooves had higher maltracking and revision rates. Multiple national registries support cemented fixation and modern implant designs.
Clinical Assessment
- Pain location: Anterior knee, retropatellar, peripatellar
- Aggravating factors: Stairs, squatting, prolonged sitting (theater sign)
- Duration: Minimum 6 months failed conservative treatment
- Previous surgery: Prior realignment procedures common
- Trauma history: Post-fracture PF arthritis
- Activity level: Important for realistic expectations
- Mechanical symptoms: Locking suggests loose body
- Gait: Antalgic, avoid stairs
- Alignment: Varus/valgus deformity (suggests TF disease)
- Effusion: Significant effusion unusual in isolated PF OA
- Patellar tracking: J-sign indicates dysplasia/instability
- Crepitus: Patellofemoral crepitus on ROM
- ROM: Full ROM typical (unlike TF OA)
- Tenderness: Joint line tenderness suggests TF pathology
Exclude these findings before proceeding with PFA:
- Joint line tenderness on palpation (suggests TF arthritis)
- Fixed flexion deformity over 10 degrees (indicates posterior capsule contracture from TF disease)
- Varus/valgus thrust on gait (mechanical axis deviation from TF wear)
- Significant effusion (active TF synovitis more common than isolated PF)
Special Tests
Clinical Testing Protocol
Lateral translation of patella with knee in 20-30 degrees flexion. Positive test indicates dysplasia or prior instability. Not a contraindication but requires careful component positioning.
Compression of patella against trochlea with knee extension. Crepitus and pain confirm PF pathology. Useful for demonstrating isolated PF disease to patient.
Patient contracts quadriceps against resistance with knee extended. Pain indicates PF pathology. Low specificity but high sensitivity.
Ask about pain after prolonged sitting with knees flexed (at movies, theater). Classic for PF arthritis. Helps differentiate from TF disease.
Differential Diagnosis of Anterior Knee Pain
- Key Distinguishing Features
- Anterior/retropatellar pain, theater sign, PF crepitus, pristine TF joints, full ROM
- Relevance to PFA Decision
- The target diagnosis - PFA appropriate if confirmed
- Key Distinguishing Features
- Joint line tenderness, varus/valgus deformity, effusion, reduced ROM
- Relevance to PFA Decision
- Contraindication to PFA - proceed to TKA
- Key Distinguishing Features
- Younger patient, J-sign, apprehension, dysplasia, recurrent dislocation
- Relevance to PFA Decision
- Address instability first (TTO/MPFL/trochleoplasty), not PFA in isolation
- Key Distinguishing Features
- Focal inferior pole tenderness, load-related pain, normal joint space
- Relevance to PFA Decision
- Non-arthritic - PFA not indicated
- Key Distinguishing Features
- Polyarticular, morning stiffness, raised CRP/ESR, symmetrical involvement
- Relevance to PFA Decision
- Absolute contraindication to PFA
- Key Distinguishing Features
- Groin/thigh pain, abnormal hip ROM, dermatomal pattern, normal knee imaging
- Relevance to PFA Decision
- Treat the true source - knee arthroplasty inappropriate
Investigations
Imaging Protocol
AP standing: Assess TF compartments for OA, alignment Lateral: Measure Insall-Salvati ratio (patellar height), assess trochlear depth Skyline/Merchant view: 45-degree flexion, assess PF joint space, subluxation Long-leg alignment films: Mechanical axis, exclude varus/valgus malalignment
Key measurements: Insall-Salvati 0.8-1.2 normal, sulcus angle under 145 degrees, congruence angle less than 16 degrees.
Indications: Assess trochlear dysplasia severity, measure TT-TG distance if tracking abnormal Measurements: Dejour classification, sulcus angle, lateral trochlear inclination Patient-specific implants: Some systems require CT for custom component manufacture
Indications: Young patients, exclude meniscal pathology, assess cartilage status all compartments Findings: Full-thickness PF cartilage loss, confirm pristine TF cartilage, meniscal tears Limitation: May overestimate TF disease severity (high sensitivity, lower specificity)
Gold standard for cartilage assessment if uncertainty Allows grading of TF compartments (Outerbridge) Therapeutic: Loose body removal, chondroplasty Risk: May increase stiffness if PFA performed soon after
- PF joint: Narrowing, osteophytes, bone-on-bone contact
- TF compartments: MUST be pristine (no joint space narrowing)
- Alignment: Mechanical axis neutral (varus/valgus suggests TF disease)
- Patellar height: Insall-Salvati ratio 0.8-1.2 normal
- Trochlear depth: Greater than 3mm normal, less than 3mm dysplastic
- Full-thickness PF cartilage loss: Confirms isolated disease
- TF cartilage: Should be intact (Outerbridge grade 0-1)
- Bone marrow edema: Common in PF joint, indicates active disease
- Menisci: Usually intact in isolated PF OA
- Trochlear dysplasia: Assess severity and symmetry
Management Algorithm
Non-Operative Treatment (Mandatory 6-12 Months)
All patients must fail comprehensive conservative treatment before considering PFA.
Staged Conservative Protocol
- NSAIDs: Regular dosing for anti-inflammatory effect
- Activity modification: Avoid stairs, squatting, kneeling
- Weight loss: If BMI over 30, target 5-10% reduction
- Ice therapy: After activities to reduce inflammation
- Bracing: Patella-stabilizing brace if tracking abnormal
- VMO strengthening: Selective quadriceps exercises
- Hip abductor work: Gluteus medius weakness common
- Hamstring stretching: Reduce PF contact force
- Proprioception: Balance and stability exercises
- Taping: McConnell taping for symptom relief
- Corticosteroid: Intra-articular if significant synovitis
- Hyaluronic acid: May provide 3-6 months relief
- PRP: Limited evidence but low risk option
- Response: Good response suggests inflammatory component
Only if failed ALL conservative measures and isolated PF disease confirmed.
Conservative treatment success rate only 20-30% for established PF arthritis, but mandatory before surgery.

Surgical Technique
Pre-operative Planning
- Progression to TF OA: 15-25% require conversion to TKA at 10 years
- Infection: 1-2% deep infection risk
- Stiffness: 5-10% develop significant stiffness
- Anterior knee pain: 10-15% persistent pain despite well-positioned components
- Maltracking: Patellar instability or subluxation 3-5%
- DVT/PE: Standard arthroplasty risks, chemical prophylaxis used
- Revision: Overall revision rate 2.5 times higher than TKA
- Implants: PFA system (Avon, Journey PFJ, or similar), trial components
- Power tools: Oscillating saw, high-speed burr for trochlear preparation
- Imaging: C-arm for intra-operative imaging if needed
- Instruments: Specific PFA instrumentation set
- Cement: Antibiotic-loaded PMMA (registry data supports cemented fixation)
- Backup: Have TKA components available if conversion needed
Patient Positioning and Setup
Setup Checklist
Supine on standard operating table.
- Leg holder on operative side (allows controlled flexion-extension)
- Thigh tourniquet applied high on thigh
- Contralateral limb: Padded leg holder or well leg holder
- Hip bump: Small bump under ipsilateral hip for neutral rotation
- Placement: High on thigh to allow full access
- Pressure: 100mmHg above systolic (typically 300mmHg)
- Exsanguination: Elevation and Esmarch bandage
- Timing: Inflate after prep and drape, before incision
- Landmarks exposed: Anterior superior iliac spine to tibial tubercle visible
- Limb position: Ensure full ROM from extension to over 120 degrees flexion
- Prep: Chlorhexidine or iodine, circumferential limb prep
- Drape: Standard arthroscopy or knee replacement draping
Ensure the leg holder allows easy transition from full extension to over 120 degrees of flexion. You need to assess patellar tracking throughout the entire ROM intraoperatively, so positioning must facilitate this.
Technical Pearls and Pitfalls
- Mark native anatomy: Before resection, mark trochlear groove
- Minimal bone removal: Preserve bone stock for potential TKA conversion
- Perfect tracking: Do not accept maltracking, revise if needed
- Cement all components: Registry data support cemented fixation
- Assess TF compartments: Confirm pristine at time of surgery
- Restore patellar thickness: Avoid overstuffing (increases contact stress)
- Trial components: Always trial before cementing final components
- Notch the femur: Avoid posterior extension into condyles (fracture risk)
- Over-resect patella: Leave minimum 12mm bone stock
- Accept maltracking: Fix it intraoperatively, not postoperatively
- Routine lateral release: Only if tracking requires it after components placed
- Overstuff joint: Composite patellar thickness should equal native
- Miss TF disease: Confirm no cartilage damage before proceeding
- Poor component position: Even 2-3mm off leads to poor outcomes
TRACESurgical Steps for PFA
Hook:TRACE the patella through ROM - tracking assessment is the final critical step!
Bicompartmental Arthroplasty (PFA plus UKA)
The controversies name "bicompartmental arthroplasty combining PFA with a medial UKA" and "modular bicompartmental constructs", but the option is never developed.
- The problem it solves. When a patient has isolated PF arthritis PLUS one tibiofemoral (usually medial) compartment worn, while the other TF compartment and both cruciates are pristine, a TKA sacrifices two healthy structures. Bicompartmental arthroplasty resurfaces only the two diseased compartments (PF plus medial TF) and keeps the lateral compartment and the cruciates.
- Two ways to do it. Modular ("mix-and-match") - a separate PFA and a separate medial UKA implanted together, so each component is sized and positioned independently (the more forgiving option). Monolithic - a single implant spanning the PF and medial compartments (e.g. the Journey Deuce), which is technically demanding because one implant must fit two joints and leaves little room to adjust.
- Evidence and role. Selected series report function approaching TKA with more natural kinematics and cruciate preservation, but monolithic designs had high early revision (fit and overstuffing problems) and the modular approach lacks long-term comparative data - so it remains a niche option for younger patients at high-volume centres, not a mainstream alternative to TKA.
- The caveat. It roughly doubles the technical difficulty (two articulations to balance) and, like PFA, does not stop OA progressing in the untouched lateral compartment.
Q: What is bicompartmental arthroplasty and when might it be considered? A: Resurfacing the patellofemoral AND one (usually medial) tibiofemoral compartment while preserving the other TF compartment and both cruciates, for a patient with PF plus one-compartment OA who would otherwise need a TKA. It is done either modularly (a separate PFA plus medial UKA, sized independently) or with a monolithic implant (e.g. Journey Deuce). It offers more natural kinematics and bone/ligament preservation but is technically demanding, monolithic designs had high early revision, and long-term comparative data are lacking - so it stays a niche option, not a mainstream TKA alternative.
Overstuffing the Patellofemoral Joint
The topic warns against "overstuffing" as the cardinal technical pitfall - in the exam warning, the technique tabs, the pitfalls list and the complications - but never explains what it is, why it matters or how to avoid it.
- What it is. Overstuffing means the composite anterior thickness of the reconstructed joint (patellar bone remnant + patellar component + cement, together with the thickness of the trochlear component) is greater than the native patellofemoral thickness it replaced. The joint is made too "tight" in the anteroposterior direction.
- Why it matters. A thicker composite raises the patellofemoral contact force and retinacular tension through flexion, causing anterior knee pain, stiffness and loss of terminal flexion; the tight lateral retinaculum drives maltracking; and the higher stress increases patellar fracture and polyethylene wear risk. It is one of the commonest avoidable causes of a painful, stiff PFA.
- How to avoid it. Caliper the native patella before resection and resect enough bone that (bone remnant + component + cement) restores, not exceeds, the original patellar thickness; if the patella is thin, use a thinner polyethylene rather than under-resecting the bone. Choose a trochlear component that sits flush with the anterior femur (not proud), and confirm at trial that the patella is not overstuffed before cementing.
Q: What is "overstuffing" in patellofemoral arthroplasty and how do you avoid it? A: Making the composite patellofemoral thickness (patellar bone + component + cement, plus the trochlear component) greater than native - the joint becomes too tight anteroposteriorly. It raises patellofemoral contact force and retinacular tension, causing anterior knee pain, stiffness, loss of flexion and maltracking, and increases patellar-fracture/wear risk. Avoid it by calipering the native patella and restoring (not exceeding) its thickness, using a thinner polyethylene if the patella is thin, and seating the trochlear component flush with the anterior femur.
Complications
- Incidence
- 15-25% at 10 years
- Risk Factors
- Pre-existing Outerbridge grade 2 TF changes, age over 65
- Management
- Convert to TKA, use standard primary components
- Incidence
- 3-5% at 10 years
- Risk Factors
- Uncemented fixation, poor bone quality, malposition
- Management
- Revision PFA if TF intact, otherwise TKA
- Incidence
- 5-10%
- Risk Factors
- Component malposition, uncorrected dysplasia, inadequate lateral release
- Management
- Physiotherapy, consider revision or lateral release
- Incidence
- 10-15% persistent
- Risk Factors
- Overstuffing, maltracking, component malposition
- Management
- Exclude infection/loosening, physiotherapy, consider revision
- Incidence
- 1-2%
- Risk Factors
- Diabetes, immunosuppression, prior surgery
- Management
- Early: debridement and component retention. Late: two-stage revision
- Incidence
- 1-2%
- Risk Factors
- Over-resection (under 12mm), avascular necrosis, trauma
- Management
- Non-displaced: conservative. Displaced: ORIF, consider component removal
- Incidence
- 5-10%
- Risk Factors
- Overstuffing, poor rehabilitation, infection
- Management
- Physiotherapy, manipulation under anesthesia if severe
The most common reason for PFA revision is progression of arthritis to the tibiofemoral compartments, accounting for 50-60% of all PFA revisions. This is NOT a technical failure but rather disease progression. Emphasize this during consent - the 15-25% conversion rate at 10 years is expected, and conversion to TKA is straightforward with excellent outcomes.
Postoperative Care and Rehabilitation
Rehabilitation Timeline
- Analgesia: Multimodal analgesia (paracetamol, NSAIDs, opioids PRN)
- DVT prophylaxis: Chemical (enoxaparin or rivaroxaban) for 10-14 days
- Cryotherapy: Ice to knee for swelling and pain control
- Mobilization: Same day weight-bearing as tolerated with physiotherapy
- Straight leg raise: Begin isometric quadriceps exercises immediately
- ROM: Gentle flexion-extension exercises, target 90 degrees by day 1
- Weight-bearing: Full weight-bearing as tolerated (no restrictions)
- Gait aids: Progress from frame to crutches to stick to independent
- ROM exercises: Active-assisted flexion, aim for 100-110 degrees by discharge
- Quadriceps: Progressive strengthening, straight leg raise without lag
- Discharge: Typically day 1-3 for uncomplicated PFA
- Wound: Remove dressing day 2, check wound, apply simple dressing
- Physiotherapy: Supervised outpatient therapy 2-3 times per week
- ROM goal: Full extension, 120+ degrees flexion by week 6
- Strengthening: Progressive resistance exercises, closed chain preferred
- Proprioception: Balance and stability exercises
- Activities: Stairs, walking, cycling (stationary bike), swimming
- Wound: Sutures/staples removed at 10-14 days
- Strengthening: Gym-based program, increase resistance progressively
- Impact activities: Begin low-impact sports (golf, cycling)
- Functional goals: Stairs without aids, normal gait pattern
- Return to work: Sedentary work 2-4 weeks, physical work 6-12 weeks
- Sports: Gradual return to impact sports (tennis, jogging)
- Avoid: High-impact activities that increase PF contact force (running, jumping)
- Expected function: 90% pain relief, normal daily activities, some activity limitations
- Surveillance: Annual review for first 2 years, then biennial
- Radiographs: Baseline at 6 weeks, then annually to monitor for TF progression
- Registry: Submit implant and procedure data to the national joint registry (e.g. NJR, AOANJRR, AJRR)
- Watch for: Increasing pain, mechanical symptoms suggesting TF arthritis
Outcomes and Prognosis
Modern onlay PFA designs have dramatically improved outcomes compared to first-generation inlay designs, with 10-year survival approaching 90% in well-selected patients.
- PFA Result
- Excellent in 85-90% of patients
- Comparison to TKA
- Equivalent to TKA for isolated PF disease
- PFA Result
- Mean 125 degrees, often better than pre-op
- Comparison to TKA
- Superior to TKA (mean 115 degrees)
- PFA Result
- Mean improvement 15-20 points
- Comparison to TKA
- Equivalent to TKA
- PFA Result
- Higher rate low-impact sports
- Comparison to TKA
- Better than TKA for golf, cycling, swimming
- PFA Result
- 2.5 times higher than TKA (AOANJRR)
- Comparison to TKA
- Higher but conversion straightforward
- PFA Result
- Improved vs pre-op but 30% still avoid
- Comparison to TKA
- Similar to TKA
Poor prognostic factors that increase revision risk:
- Age over 65 years at time of surgery (2x revision rate)
- Pre-existing TF changes (Outerbridge grade 2 or higher)
- Severe trochlear dysplasia (Dejour type C or D)
- BMI over 35
- Inflammatory arthropathy (absolute contraindication)
- Onlay design implants (historical, no longer used)
Best outcomes: Age 40-60 years, BMI under 30, isolated PF disease, normal trochlear anatomy, modern onlay design implant.
Registry Evidence Snapshot
- PFA represents roughly 1-2% of all knee arthroplasties across major registries
- PFA revision rate consistently 2-3 times higher than primary TKA
- Cemented fixation: lower revision than uncemented across registries
- Most common reason for revision: progression to TF arthritis (~50-60%)
- Other reasons: loosening/lysis, maltracking, pain
- PFA is an effective bone-preserving option for isolated PF arthritis
- Patient selection is critical - exclude any TF disease
- Use cemented fixation (lower revision rate)
- Counsel patients about conversion risk (realistic expectation)
- Conversion to TKA has good outcomes (not a failed treatment)
Guidelines, Registries & Global Practice
Global Epidemiology
Isolated patellofemoral osteoarthritis accounts for roughly 10% of symptomatic knee OA and is more common in women and in patients with prior patellar instability, trochlear dysplasia, or post-traumatic deformity. PFA represents only about 1-2% of all knee arthroplasties worldwide, with volumes rising as modern designs and patient-specific instrumentation improve outcomes.
Society Guidance and Registry Evidence (Side by Side)
- Position on PFA
- Recognised option for isolated PF OA in appropriately selected patients
- Key Recommendation
- Emphasise strict selection and informed consent re higher revision/conversion than TKA
- Position on PFA
- Acceptable for isolated PF arthritis; TKA preferred where any TF disease
- Key Recommendation
- Reserve for true single-compartment disease; counsel on conversion risk
- Position on PFA
- Captures higher PFA revision rate vs TKA, driven by OA progression
- Key Recommendation
- Favours cemented fixation and modern trochlear designs
- Position on PFA
- PFA revision ~2-3x primary TKA; older age increases revision risk
- Key Recommendation
- Cemented fixation and careful selection (younger, isolated disease)
- PFA revision rate consistently 2-3 times higher than primary TKA
- Progression to TF arthritis is the dominant revision indication (~50-60%)
- Cemented fixation associated with lower revision than uncemented
- Older patients (especially over 65) have higher revision risk
- Conversion to TKA uses primary components in over 90% of cases
- Confirm truly isolated PF disease before proceeding (clinical, imaging, intra-op)
- Use a modern onlay/deeper-grooved trochlear design, cemented
- Antibiotic-loaded cement and routine VTE prophylaxis per local arthroplasty protocols
- Assess tracking with the no-thumbs test before closure
- Consent must include the realistic conversion-to-TKA risk
High- vs Limited-Resource Practice Variation
- Access to MRI/CT, intra-operative arthroscopy, and patient-specific or robotic instrumentation
- Wider implant range, including modern onlay and custom systems
- Mandatory or near-universal registry submission of implant data
- Enhanced-recovery pathways with short length of stay
- Diagnosis relies more on weight-bearing and skyline radiographs than MRI
- Where modern implants or revision capacity are scarce, primary TKA may be preferred for durability
- PFA reserved for clearly isolated disease where bone preservation is prioritised
- Registry capture may be incomplete, limiting local outcome data
- The 15-25% risk of conversion to TKA at 10 years (most common adverse outcome - progression of arthritis is expected in a subset)
- Higher revision rate than TKA, but conversion is straightforward with primary components
- Standard arthroplasty risks: infection, stiffness, VTE, persistent anterior knee pain
- Activity modification: avoid high-impact sport to preserve implant longevity
- Alternatives: TKA (more predictable long-term survival) and continued conservative care
- Confirmation of pristine tibiofemoral compartments (Outerbridge grade 0-1)
- Patellar tracking result (no-thumbs test)
- Component sizes and device identifiers for registry submission
- Any tracking difficulty requiring lateral release or component repositioning
- Inadequate consent regarding conversion risk
- Proceeding with PFA despite TF involvement found intra-operatively (should convert to TKA)
- Poor patient selection (inflammatory arthritis, severe dysplasia)
- Accepting maltracking without intra-operative correction
- Failure to monitor for TF progression (radiographic surveillance in early years)
Controversies and Areas of Uncertainty
PFA remains one of the more debated arthroplasty procedures. The exam-relevant controversies are:
Some surgeons favour PFA to preserve bone and ligaments in patients under 60, accepting a higher revision rate; others prefer the more predictable durability of TKA. No adequately powered long-term RCT settles this - the Warwick trial design addressed it but mature comparative data are limited.
The role of PFA (or bicompartmental arthroplasty combining PFA with a medial UKA) when both PF and one TF compartment are affected is unresolved. Modular bicompartmental constructs show outcomes comparable to TKA in selected series but with technical complexity and uncertain longevity.
Modern deeper-grooved (onlay-style) trochlear designs are generally felt to track better than first-generation inlay designs, yet terminology and best-design debates persist. Registry signals favour contemporary designs broadly rather than one specific philosophy.
Robotic-assisted and patient-specific instrumentation may reduce malposition-driven maltracking, but current evidence is short-term, non-randomised, and does not yet justify routine use over careful manual technique.
If asked "would you offer PFA or TKA to a 55-year-old with isolated PF arthritis?", there is no single right answer - demonstrate that you understand the trade-off (bone preservation and better ROM vs higher conversion risk), the need for meticulous selection, and the importance of honest consent. Committing dogmatically to one option without acknowledging the controversy is the trap.
MCQ Practice Points
Q: What is the normal Insall-Salvati ratio for patellar height, and what ratio would be considered patella baja (a contraindication to PFA)? A: Normal Insall-Salvati ratio is 0.8 to 1.2 (patellar tendon length divided by patellar height). Patella alta is ratio over 1.2, and patella baja is ratio under 0.8. Patella baja is a contraindication to PFA because the patella engages the trochlear groove at a higher flexion angle, making tracking difficult and increasing contact stresses. This leads to anterior knee pain and early failure.
Q: What is the Dejour classification of trochlear dysplasia, and which type is an absolute contraindication to PFA? A: Dejour classification has four types based on radiographic findings: Type A (crossing sign only, normal depth), Type B (flat or convex trochlea, sulcus angle over 145 degrees), Type C (asymmetric lateral facet with cliff sign), and Type D (cliff sign plus vertical link plus asymmetry). Type D is an absolute contraindication to PFA due to severely abnormal anatomy making component positioning impossible and tracking unreliable. Types B and C are relative contraindications with 3-4 times higher revision rates.
Q: What is the most common reason for revision after PFA, and how are these revisions typically managed? A: Progression of arthritis to the tibiofemoral compartments is the most common reason for PFA revision, accounting for 50-60% of all revisions. This is not a technical failure but expected disease progression. Management is conversion to total knee arthroplasty using standard primary TKA components in over 90% of cases. Outcomes after conversion are equivalent to primary TKA. This is a key counseling point pre-operatively - patients must understand the 15-25% conversion risk at 10 years.
Q: What does joint registry data show regarding fixation and revision risk for PFA? A: Across major national registries (e.g. NJR, AOANJRR), cemented PFA has lower revision rates than uncemented fixation, mirroring TKA registry trends. All PFA components (both trochlear and patellar) should therefore be cemented for optimal long-term survival. Registry data also consistently show PFA revision rates roughly 2-3 times higher than primary TKA, with progression of tibiofemoral arthritis as the dominant failure mode - but conversion to TKA is straightforward and uses primary components in over 90% of cases.
Q: What is the no-thumbs test and what does it assess after PFA? A: The no-thumbs test is performed by flexing and extending the knee throughout the full range of motion without manually touching or guiding the patella. If the patella tracks centrally through 0-120 degrees of flexion without requiring manual guidance, tracking is acceptable. If the surgeon needs to use their thumbs to manually guide the patella to keep it centered, tracking is inadequate and requires correction (lateral release or component revision). This is the gold standard intra-operative assessment of PFA tracking and must be performed before closure.
Q: What is the minimum acceptable posterior patellar bone stock after patellar resection during PFA, and what is the risk of violating this? A: Minimum acceptable posterior patellar bone stock is 12mm. Resecting more than this (leaving less than 12mm) dramatically increases the risk of intra-operative or post-operative patellar fracture. The patella experiences very high contact stresses (up to 6 times body weight during stair descent), so adequate bone stock is essential for load distribution. If the native patella is very thin, consider using a thinner polyethylene component rather than over-resecting the bone.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old active female presents with 2 years of anterior knee pain. She has failed 6 months of physiotherapy and intra-articular injection. Weight-bearing radiographs show isolated severe patellofemoral arthritis with bone-on-bone contact. The tibiofemoral compartments appear well preserved. She is asking about patellofemoral arthroplasty after researching online. How would you assess and counsel this patient?”
“You have just completed a patellofemoral arthroplasty. The trochlear and patellar components are cemented and cured. You perform the no-thumbs test and notice the patella subluxates laterally in early flexion (0-30 degrees) but then reduces and tracks centrally in deeper flexion. What would you do?”
“A 58-year-old patient returns 5 years after patellofemoral arthroplasty with increasing medial knee pain over the past 12 months. Initial PFA gave her excellent pain relief for 3 years. Examination shows medial joint line tenderness and small effusion. Radiographs show well-positioned PFA components without loosening, but new bone-on-bone medial compartment arthritis. How would you manage this patient?”
Patient Selection
- Isolated PF arthritis, pristine TF compartments (Outerbridge grade 0-1)
- Age 40-65 ideal, failed 6 months conservative treatment
- Contraindications: inflammatory arthritis, TF OA grade over 2, patella baja, severe dysplasia
- BMI under 35, realistic expectations about 15-25% conversion risk at 10y
Implant Types
- Onlay design (modern, second-generation) = resurfaces anterior femur, deeper groove = 82-90% 10y survival (Avon, FPV, Journey PFJ)
- Inlay design (first-generation) = sits flush in native groove = 70-75% 10y survival (Richards, Lubinus; largely historical)
- Cemented fixation better than uncemented across national joint registries
Surgical Steps
- Medial parapatellar approach, evert patella, assess TF compartments intra-op
- Trochlear prep: Mark native groove, minimal bone removal, precise component position
- Patellar prep: Leave minimum 12mm posterior bone stock to prevent fracture
- Cement both components, pressurize, allow full cure
- No-thumbs test throughout ROM: patella must track centrally without manual guidance
Critical Surgical Pearls
- Never accept maltracking - fix intra-op with lateral release or component revision
- Restore native patellar thickness - overstuffing causes pain and stiffness
- Avoid notching femoral condyles - weakens bone and risks supracondylar fracture
- Confirm TF compartments pristine before proceeding - any significant damage = TKA instead
Complications
- TF progression = 50-60% of revisions, 15-25% at 10 years, convert to TKA with primary components
- Anterior knee pain 10-15% persistent, causes: overstuffing, maltracking, malposition
- Patellar fracture 1-2%, avoid by leaving minimum 12mm bone stock
- Infection 1-2%, stiffness 5-10%, aseptic loosening 3-5% at 10y
Evidence Base and Key Trials

Warwick Patellofemoral Arthroplasty Trial (Design)
- Protocol for a randomised clinical trial (1:1) of PFA vs TKA in severe isolated patellofemoral arthritis
- Notes that isolated PF arthritis occurs in over 10% of patients needing knee replacement
- Primary endpoint: functional knee scores and quality of life at one year
- Secondary endpoint: complication rates for both procedures
- Articulated the bone- and ligament-preserving, less-invasive rationale for PFA over TKA
Avon PFJ Arthroplasty: 2-18 Year Single-Centre Cohort
- 558 Avon PFJ arthroplasties in 431 patients, follow-up up to 18 years
- Implant survival 77.3% at 10 years and 67.4% at 15 years
- 105 revisions; 61 (58%) for progression of osteoarthritis
- All revisions converted to primary knee systems without augmentation
- Operating surgeon had the strongest effect on survivorship; later cases survived better
PFA Survival: Systematic Review of Registries and Series
- Systematic review pooling case series and international joint registries (21 studies plus registry data)
- Registry survival 90.3% at 5 years and 82.2% at 10 years (conversion to TKA as endpoint)
- Survival fell to 73.7% at 15 years and 72.7% at 20 years
- Case-series survival (82.3% at 10 years) closely matched registry estimates
- Modern designs perform substantially better than first-generation implants
Return to Theatre: PFA vs TKA for Isolated PF OA
- Systematic review of re-operation after modern PFA versus TKA for isolated PF arthritis
- Weighted conversion/revision rate markedly higher for PFA than TKA (6.34 vs 0.11)
- Return to theatre for bony/soft-tissue procedures broadly similar between groups
- Manipulation under anaesthesia more common after TKA than PFA (1.23 vs 0.32)
- PFA trades higher conversion risk for lower stiffness-related reintervention
Avon PFJ Replacement: Independent Mid-Term Results
- Prospective independent series of 61 Avon PFJ replacements in 57 patients for isolated severe PF OA
- Mean follow-up ~5 years; only 2 revisions within the first 5 years
- Mean Oxford Knee Score 31.8 at 5 years, significantly better than pre-operative (p less than 0.001)
- Largest independent (non-designer) prospective Avon series at the time
- Confirms designer-series results are reproducible in independent hands
Robotic-Assisted PFA: Systematic Review and Meta-analysis
- Eight studies, 893 patients, evaluating robotic arm-assisted PFA
- Pooled survivorship 93.6% at mean 3.3 years
- Reduced revision risk vs manual PFA (RR 0.75, 95% CI 0.56-0.99) but wide CI
- Limited PROM and radiographic reporting; no randomised trials identified
- Robotic accuracy may improve component positioning and patellar tilt