Metastatic Disease | Mirels' Score | IMN vs Arthroplasty | Palliative Treatment
- Mirels' score ≥8 = prophylactic fixation recommended (≥9 = 33% fracture risk at 6 months, ≥10 = 50% risk)
- Life expectancy over 3-6 months = surgery beneficial (use Katagiri or PATHFx score to estimate)
- Surgical principles: Fix normal bone to normal bone, bypass lesion by ≥2 cortical diameters, cement augmentation, construct must outlast patient
- IMN for diaphyseal lesions, arthroplasty for periarticular - cemented implants for immediate stability
- Postoperative radiation essential - 30 Gy in 10 fractions at 2-3 weeks postop for local control
- “Mirels' score ≥8 = prophylactic fixation - Site (1-3), Pain (1-3), Lesion (1-3), Size (1-3)
- “Most common primaries: Breast, Lung, Prostate, Kidney, Thyroid (BLT with Kosher Pickle - BL P K T)
- “Fix normal bone to normal bone, bypass lesion by ≥2 cortical diameters, cement augmentation for lytic lesions
- “Nonunion common (radiotherapy impairs healing) but not problematic if construct stable - durable fixation more important than biological healing
Mirels' score ≥8 = prophylactic fixation recommended - Score ≥9 = 33% fracture risk within 6 months, ≥10 = 50% risk. Calculate: Site (UL 1, LL 2, peritroch 3), Pain (mild 1, mod 2, functional 3), Lesion (blastic 1, mixed 2, lytic 3), Size (under 1/3 cortex 1, 1/3-2/3 is 2, over 2/3 is 3).
Life expectancy over 3-6 months = surgery beneficial - Use Katagiri or PATHFx score. Factors: primary tumor type (breast/prostate better than lung/melanoma), visceral mets, multiple bone mets, performance status. If under 3 months, consider non-operative.
Fix normal bone to normal bone, bypass lesion by ≥2 cortical diameters, cement augmentation for lytic lesions, construct must outlast patient - IMN for diaphyseal, arthroplasty for periarticular. Allow immediate weight bearing.
Postoperative radiation essential - commonly 30 Gy in 10 fractions, around 2-3 weeks postop. Improves and maintains function and reduces reoperation to the treated site. Coordinate with radiation oncology. Nonunion common but not problematic if construct stable.
- Mirels' Score
- ≥8
- Life Expectancy
- over 3-6 months
- Treatment
- Prophylactic fixation
- Mirels' Score
- N/A
- Life Expectancy
- over 3-6 months
- Treatment
- IMN or arthroplasty
- Mirels' Score
- Any
- Life Expectancy
- over 3-6 months
- Treatment
- IMN + cement
- Mirels' Score
- Any
- Life Expectancy
- over 3-6 months
- Treatment
- Arthroplasty (cemented)
SPLSMirels' Score Components
Hook:SPLS: Site (1-3), Pain (1-3), Lesion (1-3), Size (1-3) - Score ≥8 = prophylactic fixation!
BLT K PMost Common Primaries
Hook:BLT K P: Breast, Lung, Thyroid, Kidney, Prostate - most common primaries metastasizing to bone!
Overview and Epidemiology
Pathological fractures of the femur occur through bone weakened by disease (most commonly metastatic cancer). Treatment is palliative - goal is to restore function, relieve pain, and improve quality of remaining life. Surgery is indicated if life expectancy over 3-6 months and Mirels' score ≥8 for impending fractures.
Most Common Primary Tumors
BLT with Kosher Pickle (BL P K T):
- Breast: Most common (lytic or blastic)
- Lung: Lytic metastases
- Prostate: Blastic metastases
- Kidney: Lytic metastases (hypervascular)
- Thyroid: Lytic metastases
Lytic vs Blastic:
- Lytic: Lung, kidney, thyroid, breast, melanoma (weaken bone)
- Blastic: Prostate, breast (may be mixed)
- Mixed: Breast (can be both)
Pathological fracture treatment is palliative, not curative - goal is to restore function, relieve pain, and improve quality of remaining life. Surgery beneficial if life expectancy over 3-6 months. Construct must outlast patient (median survival 6-12 months, so fixation must last 12-24 months minimum).
Epidemiology
- Incidence: 5-10% of patients with bone metastases develop pathological fractures
- Location: Femur most common (proximal femur 50%, shaft 30%, distal 20%)
- Age: Peak 50-70 years (cancer population)
- Gender: Depends on primary tumor (breast = female, prostate = male)
- Laterality: Usually unilateral, but bilateral possible
Anatomy and Pathophysiology
Femoral Anatomy
The femur:
- Proximal: Head, neck, greater/lesser trochanter
- Shaft: Diaphyseal region
- Distal: Condyles, metaphysis
- Blood supply: Endosteal and periosteal
Metastatic involvement:
- Proximal femur: 50% of pathological fractures (weight-bearing, high stress)
- Shaft: 30% (diaphyseal lesions)
- Distal: 20% (metaphyseal lesions)
Pathophysiology
Metastatic spread:
- Hematogenous: Tumor cells spread via bloodstream
- Bone tropism: Certain tumors prefer bone (breast, prostate, lung, kidney, thyroid)
- Lytic vs blastic: Depends on primary tumor type
Bone destruction:
- Lytic lesions: Osteoclast activation destroys bone (weakened cortex)
- Blastic lesions: Osteoblast activation forms abnormal bone (may be weaker)
- Mixed lesions: Combination of both
Fracture mechanism:
- Normal bone: Requires high energy
- Pathological bone: Low energy (pathological fracture) or normal activity (impending fracture)
- Location: Proximal femur most vulnerable (weight-bearing, high stress)
If no known primary cancer, MUST obtain tissue diagnosis before surgery - treating undiagnosed lesion as metastasis when it's actually primary bone sarcoma is catastrophic error. Use CT-guided biopsy or open biopsy following oncologic principles.
Classification Systems
Mirels' Score for Impending Fracture
Site:
- Upper limb: 1 point
- Lower limb: 2 points
- Peritrochanteric: 3 points
Pain:
- Mild: 1 point
- Moderate: 2 points
- Functional (affects activities): 3 points
Lesion type:
- Blastic: 1 point
- Mixed: 2 points
- Lytic: 3 points
Size:
- Less than 1/3 cortex: 1 point
- 1/3 to 2/3 cortex: 2 points
- Over 2/3 cortex: 3 points
Interpretation:
- Score ≥8: Prophylactic fixation recommended
- Score ≥9: 33% fracture risk within 6 months
- Score ≥10: 50% fracture risk within 6 months
Mirels' score guides prophylactic fixation decisions.
Clinical Assessment
History
Cancer history:
- Primary tumor: Type, stage, treatment history
- Metastases: Known bone metastases, visceral metastases
- Systemic therapy: Chemotherapy, radiation, immunotherapy
- Performance status: ECOG or Karnofsky score
Fracture history:
- Mechanism: Low energy (pathological) or normal activity (impending)
- Pain: Location, severity, functional impact
- Function: Ambulatory status, weight-bearing ability
Physical Examination
Inspection:
- Deformity (if complete fracture)
- Swelling
- Skin condition (previous radiation, surgical scars)
Palpation:
- Tenderness over lesion/fracture
- Crepitus (if complete fracture)
- Soft tissue mass (if large tumor)
Range of Motion:
- Hip ROM (if proximal)
- Knee ROM (if distal)
- Pain with movement
Neurovascular Status:
- Distal pulses and sensation
- Motor function
Assess performance status and goals of care - surgery is palliative. If patient is bedbound with weeks to live, surgery may not benefit. If ambulatory with months to live, surgery can restore function and improve quality of life.
Associated Conditions
- Visceral metastases: Liver, lung, brain
- Other bone metastases: Multiple skeletal lesions
- Systemic therapy: Ongoing chemotherapy
- Radiation: Previous radiation to affected area
Investigations
Standard X-ray Protocol
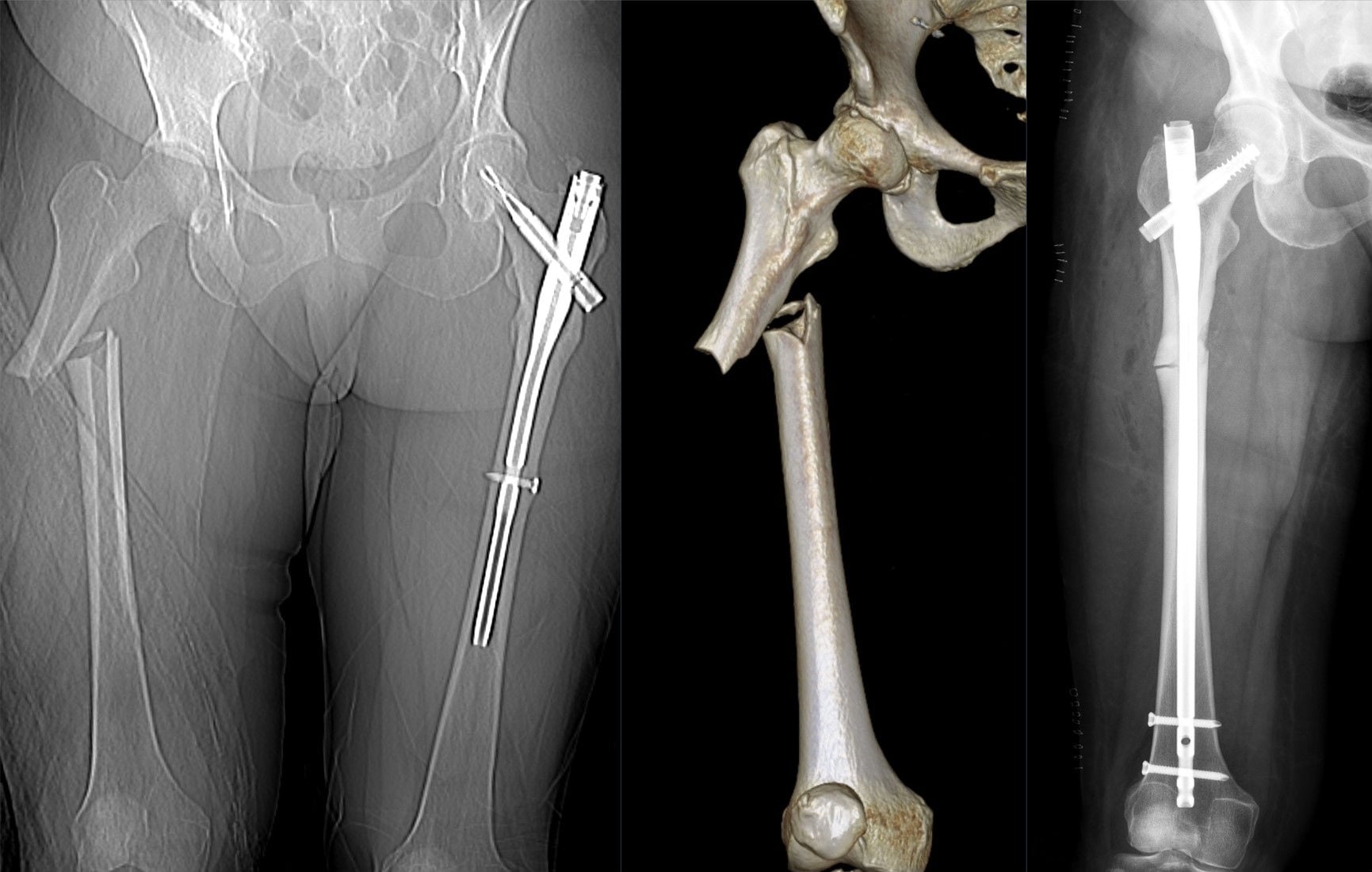
Views: AP and lateral femur (full length).
Key findings:
- Fracture: Complete or impending (lytic lesion)
- Lesion characteristics: Lytic, blastic, or mixed
- Size: Assess cortical destruction (Mirels' score)
- Location: Proximal, shaft, or distal
Full-length views essential - assess entire femur for other lesions.
Differential Diagnosis of a Destructive Femoral Lesion
- Typical Age
- Over 40, known/likely primary
- Key Discriminators
- Multiple lesions, known cancer, lung/breast/prostate/kidney/thyroid
- Action Before Fixation
- Confirm primary; biopsy if solitary or no primary
- Typical Age
- 50-70
- Key Discriminators
- Multiple punched-out lytic lesions, paraprotein, raised ESR, anaemia
- Action Before Fixation
- SPEP/serum free light chains, marrow - medical, not always surgical
- Typical Age
- Bimodal / any
- Key Discriminators
- Solitary, aggressive periosteal reaction, soft-tissue mass, no known primary
- Action Before Fixation
- STOP - refer to tumour unit, biopsy along future resection track. NEVER nail
- Typical Age
- Any
- Key Discriminators
- Permeative lesion, relatively well patient, B-symptoms
- Action Before Fixation
- Biopsy - chemo/radiotherapy responsive
- Typical Age
- Elderly
- Key Discriminators
- No discrete lesion, generalised osteopenia, low-energy
- Action Before Fixation
- Treat as fragility fracture; investigate if atypical
- Typical Age
- Over 55
- Key Discriminators
- Cortical thickening, bony expansion, raised ALP, bowing
- Action Before Fixation
- Bisphosphonates; pathological fracture risk in lytic phase
- Typical Age
- On long-term antiresorptive
- Key Discriminators
- Lateral cortical beaking, transverse subtrochanteric/diaphyseal fracture
- Action Before Fixation
- Distinct entity - prophylactic/therapeutic nailing, stop drug
A solitary destructive femoral lesion in a patient without an established cancer diagnosis must be treated as a possible primary bone sarcoma until proven otherwise. Biopsy through an inappropriate track or intramedullary nailing of a sarcoma contaminates the canal, converts a limb-salvageable tumour into an amputation, and worsens survival. Refer to a specialist musculoskeletal oncology unit for staging and biopsy before any fixation.
Management Algorithm
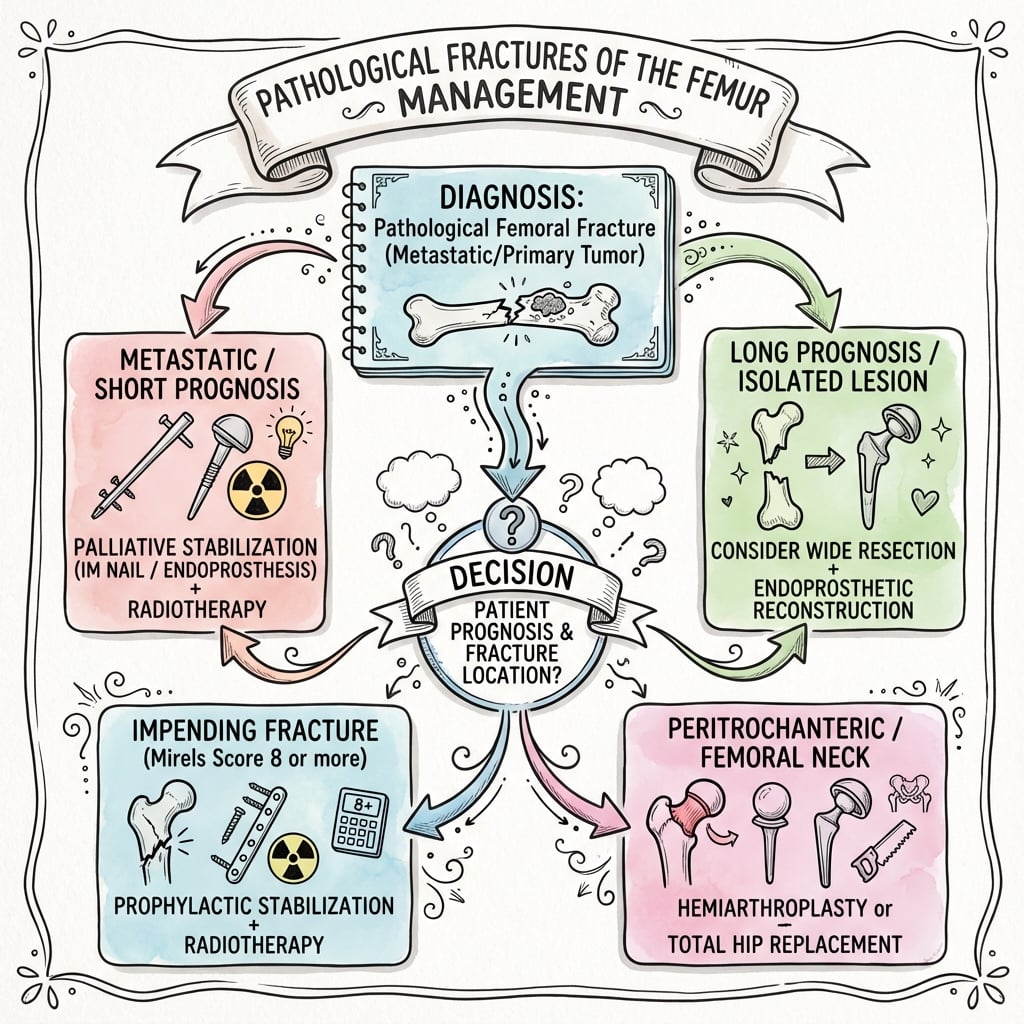
Management Pathway
Pathological Fracture Management
Confirm metastatic disease (history, imaging, biopsy if needed). Stage with CT chest/abdomen/pelvis. Estimate life expectancy (Katagiri or PATHFx score). Calculate Mirels' score if impending fracture.
If life expectancy over 3-6 months and Mirels' score ≥8 (impending) or complete fracture, proceed with surgery. If under 3 months, consider non-operative (palliative care).
Diaphyseal lesion: IMN + cement augmentation. Periarticular lesion: Arthroplasty (cemented). Fix normal bone to normal bone, bypass lesion by ≥2 cortical diameters.
Postoperative radiation essential - 30 Gy in 10 fractions at 2-3 weeks postop. Provides local control and pain relief. Coordinate with radiation oncology.
Surgical Technique
Intramedullary Nailing
Indications:
- Diaphyseal lesions (shaft)
- Proximal or distal shaft lesions
Technique:
- Long nail: From proximal to distal metaphysis
- Bypass lesion: Minimum 2 cortical diameters (4x bone diameter) beyond lesion
- Interlocking: Both ends (static locking)
- Cement augmentation: Inject PMMA through cortical window at lesion site
- Cement timing: After nail insertion (or before - cement first technique)
Advantages:
- Less invasive
- Allows immediate weight bearing
- Good stability
IMN is gold standard for diaphyseal pathological fractures.
Minimize tumor spillage during surgery - use gentle handling, copious irrigation. If open approach, consider curettage through limited window. Postoperative radiation provides local control, but minimizing spillage reduces risk.
FIXSurgical Principles
Hook:FIX: Fix normal to normal, Involve bypass ≥2 diameters, X-ray (cement) augmentation!
Distal and Periarticular Femoral Reconstruction
The classification table names a "distal 20%" of femoral pathological fractures and says "IMN or arthroplasty", but the surgical-technique section only develops the diaphyseal nail and the proximal arthroplasty - leaving the distal femur, a genuine exam scenario, undeveloped. The reconstruction is driven by how much of the distal metaphysis/condyles is destroyed and whether the joint surface is involved.
A distal-third or supracondylar lesion with a preserved articular block and enough distal bone to hold fixation is reconstructed with a retrograde intramedullary nail (spanning to the proximal metaphysis, bypassing the lesion by two cortical diameters) or a distal femoral locking plate, with cement augmentation of the lytic defect. Nail protects the whole diaphysis; a locked plate/condylar construct is preferred when the canal cannot be safely engaged distally.
When the condyles are destroyed or the joint surface is involved, fixation has nothing durable to purchase and a distal femoral endoprosthetic replacement (tumour megaprosthesis with a hinged knee) is the reliable option - it resects the disease, gives immediate stability and immediate weight-bearing, and outlasts the patient. The trade-off is a much larger operation with its own infection and mechanical-failure profile.
- The same first principles still apply: confirm the diagnosis (never treat a solitary distal femoral lesion as metastasis without excluding sarcoma), estimate survival, protect the whole bone, allow immediate weight-bearing, and give post-operative radiotherapy to a fixation (not usually to a megaprosthesis).
- Why not just plate everything: an isolated locked plate across a lytic distal femoral lesion in poor bone can fatigue and fail; combine with cement, or choose a load-bypassing nail or an endoprosthesis when destruction is extensive.
Q: How does distal femoral metastatic reconstruction differ from the diaphysis? A: Judge by condylar bone stock and joint involvement. Intact condyles with a metadiaphyseal lesion → retrograde nail or distal femoral locking plate + cement (bypass the lesion, protect the diaphysis). Destroyed condyles or an involved joint surface → distal femoral endoprosthetic replacement (hinged tumour prosthesis), because fixation has no durable purchase. Same principles otherwise: exclude sarcoma, immediate weight-bearing, adjuvant radiotherapy to fixations.
The Hypervascular and Embolic Femur: Bleeding and Marrow-Embolism Control
The topic repeatedly flags renal cell and thyroid hypervascularity, pre-operative embolisation, and that long intramedullary implants carry a roughly 12% embolic complication rate (Alvi & Damron) - but never sets out how to manage these two femur-specific operative hazards.
- Pre-operative embolisation of hypervascular metastases. Renal cell carcinoma and thyroid (and sometimes hepatocellular) femoral metastases can bleed catastrophically during curettage/nailing. Trans-arterial embolisation within ~24-48 hours before surgery substantially reduces intra-operative blood loss and transfusion, and is strongly considered for large, vascular lesions - especially when open debulking or arthroplasty is planned. It does not remove the higher local-progression risk of renal cell disease (odds ratio ~5 after nailing; Arpornsuksant/Levin), which is a separate reason to consider resection/endoprosthesis over a nail for RCC.
- Bone-marrow/tumour fat embolism during reaming. Passing a long reamed intramedullary device down a tumour-laden femoral canal pressurises marrow, fat and tumour into the venous system and can cause intra-operative hypoxia, hypotension and, rarely, fatal embolism (the ~12% non-fatal embolic-event rate is the price of whole-bone protection). Mitigate with anaesthetic vigilance and communication, venting/decompressing the canal, slow and gentle reaming (or reamer-irrigator-aspirator to lower intramedullary pressure), and avoiding over-pressurisation of cement. In a frail patient with a short prognosis this embolic risk is a legitimate reason to accept a shorter construct rather than reflexively spanning the whole bone.
Q: A patient with a hypervascular renal cell femoral metastasis needs fixation - what specific femoral precautions apply? A: Pre-operative trans-arterial embolisation (~24-48 h before) to cut catastrophic intra-operative haemorrhage; and because reaming a tumour-filled femur drives marrow/fat/tumour embolism (part of the ~12% embolic-complication rate of long nails), warn the anaesthetist, vent the canal, ream slowly (consider RIA) and avoid cement over-pressurisation. For RCC also weigh resection/endoprosthesis over nailing given its higher local-progression risk.
Complications
- Incidence
- Common (radiation-impaired healing)
- Risk Factors
- Tumor progression, radiotherapy, poor bone
- Prevention/Management
- Not problematic if construct stable
- Incidence
- Reoperation ~6%
- Risk Factors
- Inadequate bypass, no cement
- Prevention/Management
- Bypass ≥2 diameters, cement augmentation
- Incidence
- ~5% at 12 months (higher in RCC)
- Risk Factors
- Renal cell primary, older age, no adjuvant RT
- Prevention/Management
- Postoperative radiotherapy, embolise RCC
- Incidence
- Low
- Risk Factors
- Tumor progression, short implant
- Prevention/Management
- Long implant, bypass lesion widely
- Incidence
- ~12%
- Risk Factors
- Long reamed intramedullary devices
- Prevention/Management
- Vent canal, slow reaming, anaesthetic vigilance
- Incidence
- Increased vs elective
- Risk Factors
- Immunosuppression, prior radiation
- Prevention/Management
- Prophylactic antibiotics, careful technique
Nonunion / Impaired Union
- Cause: Tumour at the fracture site, radiotherapy-impaired osteogenesis, poor bone stock. Bony union is the exception rather than the rule, particularly after a completed (versus prophylactically fixed) fracture.
- Prevention: Fixate impending lesions before they fracture; durable cement-augmented load-sharing constructs.
- Management: Not problematic if construct stable - the construct, not bony healing, carries the patient. Radiographic nonunion is acceptable if the patient is comfortable and functional.
Fixation Failure / Reoperation
- Magnitude: Symptomatic failure requiring reoperation is uncommon (~6% with a bone-protecting long-implant strategy; Alvi & Damron).
- Cause: Inadequate bypass of lesion, no cement augmentation, disease progression.
- Prevention: Bypass lesion by ≥2 cortical diameters, cement augmentation, long implant protecting the whole bone.
- Management: Revision fixation or conversion to (revision) arthroplasty.
Local Tumour Progression
- Magnitude: Lower than historically taught - cumulative incidence around 5% at 12 months after intramedullary nailing (Arpornsuksant/Levin), and new disease distant from the index lesion is rare.
- Cause: Renal cell carcinoma primary, older age, omission of adjuvant radiotherapy.
- Prevention: Postoperative radiotherapy; preoperative embolisation and consideration of resection/endoprosthesis for renal cell metastases.
- Management: Additional radiotherapy or surgical revision if symptomatic.
Postoperative Care
Immediate Postoperative
- Immobilization: None (early mobilization)
- Weight bearing: Immediate weight bearing as tolerated (construct designed for this)
- ROM: Early hip/knee ROM (immediate)
- PT: Ambulation training, strengthening
Rehabilitation Protocol
Weeks 0-2:
- Weight bearing as tolerated
- Ambulation training
- Hip/knee ROM exercises
- Pain management
Weeks 2-4:
- Postoperative radiation: 30 Gy in 10 fractions (2-3 weeks postop)
- Continue ambulation
- Progressive activity
Weeks 4-12:
- Full activity as tolerated
- Continue monitoring
- Systemic therapy (if indicated)
Return to Function
Goals:
- Pain relief
- Restore ambulation
- Improve quality of life
- Maintain function until death
Timeline: Immediate weight bearing - goal is rapid return to function.
Outcomes and Prognosis
Overall Outcomes
Surgical fixation outcomes:
- Success rate: 80-90% (pain relief, function restoration)
- Functional outcomes: 70-80% return to ambulation
- Complications: 20-30% (nonunion, failure, recurrence)
Median survival:
- Overall: 6-12 months (varies by primary tumor)
- Breast/prostate: 12-24 months (better prognosis)
- Lung/melanoma: 3-6 months (poorer prognosis)
Functional Outcomes
Return to ambulation:
- Timeline: Immediate (weight bearing as tolerated)
- Rate: 70-80% return to ambulation
- Factors: Performance status, life expectancy, rehabilitation
Pain relief:
- Immediate: 80-90% pain relief with surgery
- Long-term: Maintained with radiation
- Factors: Tumor type, radiation response
Long-Term Prognosis
Survival:
- Depends on primary tumor: Breast/prostate better than lung/melanoma
- Visceral metastases: Poorer prognosis
- Multiple bone metastases: Poorer prognosis
Local control:
- With adjuvant radiotherapy: better functional outcome and fewer reoperations to the treated site (Townsend)
- Local progression after nailing: around 5% at 12 months in contemporary series (Arpornsuksant/Levin)
- Higher-risk primary: renal cell carcinoma (consider embolisation and resection/endoprosthesis)
Factors Affecting Outcomes
Positive factors:
- Good performance status
- Longer life expectancy (over 6 months)
- Single or few bone metastases
- Responsive to systemic therapy
Negative factors:
- Poor performance status
- Short life expectancy (under 3 months)
- Multiple bone metastases
- Visceral metastases
- Poor response to systemic therapy
Prevention and Return to Sport
Prevention
Primary prevention:
- Early detection and treatment of primary cancer
- Systemic therapy for metastatic disease
- Bisphosphonates or denosumab (prevent skeletal-related events)
Secondary prevention (after diagnosis):
- Monitor bone metastases with imaging
- Calculate Mirels' score for impending fractures
- Prophylactic fixation if score ≥8
Return to Function
Goals (palliative):
- Pain relief
- Restore ambulation
- Improve quality of life
- Maintain function until death
Timeline: Immediate - goal is rapid return to function, not return to sport.
Guidelines, Registries & Global Practice
Global Epidemiology
- Bone is the third most common site of metastasis after lung and liver; breast, prostate, lung, kidney and thyroid account for the large majority of skeletal metastases worldwide.
- The femur is the most frequently affected long bone, and the proximal femur is the commonest site of long-bone pathological/impending fracture requiring surgery.
- With rising cancer incidence and improving systemic therapy (longer survival with metastatic disease), the absolute number of patients living with skeletal metastases - and at risk of pathological fracture - is increasing globally.
Side-by-Side Guidance
- Emphasis
- Multidisciplinary, durable single-operation construct
- Practical Recommendation
- Stabilise the whole bone, allow immediate weight-bearing, adjuvant radiotherapy
- Emphasis
- Metastatic bone disease pathway, urgent specialist referral
- Practical Recommendation
- Discuss at MDT; suspected primary sarcoma must NOT be operated on locally - refer to a bone tumour centre
- Emphasis
- Biomechanically sound, load-sharing fixation
- Practical Recommendation
- Bypass lesion, cement augmentation for defects, protect the entire bone
- Emphasis
- Survival-adapted, function-focused palliation
- Practical Recommendation
- Use prognostic scores; reserve major reconstruction for adequate predicted survival
- Emphasis
- Skeletal-related event prevention
- Practical Recommendation
- Antiresorptives (bisphosphonate or denosumab) to reduce skeletal-related events
Registry and Practice Variation
- National sarcoma/bone-tumour referral pathways (e.g. UK) consistently warn against local fixation of unbiopsied solitary lesions.
- Arthroplasty registries (NJR, AOANJRR, SHAR) capture tumour/endoprosthetic and long-stem revision arthroplasty used for metastatic proximal femoral disease.
- Contemporary cohorts show low local progression (~5% at 12 months) and reoperation (~6%) after appropriate fixation.
- High-resource settings: routine MDT, prognostic scoring (Katagiri/PATHFx), endoprosthetic options, preoperative embolisation for renal cell, ready adjuvant radiotherapy.
- Limited-resource settings: later presentation with completed fractures, restricted access to endoprostheses, embolisation and radiotherapy - intramedullary nailing with cement is often the pragmatic durable option.
- Universal principles: confirm diagnosis, protect the whole bone, allow early weight-bearing, and coordinate oncological care where available.
Pathological fractures are a common viva topic. Know that treatment is palliative (not curative), Mirels' score ≥8 = prophylactic fixation, life expectancy over 3-6 months = surgery beneficial, surgical principles (fix normal to normal, bypass ≥2 diameters, cement augmentation), IMN for diaphyseal vs arthroplasty for periarticular, and postoperative radiation essential. Be prepared to discuss Mirels' score calculation and life expectancy estimation.
Controversies and Areas of Uncertainty
Mirels' system is sensitive but not very specific, so strict application over-predicts fracture and can lead to over-treatment. Many units now individualise the decision using lesion location, functional pain, axial versus bending load, response to systemic therapy and survival estimate rather than the threshold of 8 alone. CT-based structural rigidity analysis is an emerging, more specific alternative still being validated.
For peritrochanteric/subtrochanteric metastatic lesions there is genuine debate between cephalomedullary nailing (faster, less invasive, but relies on diseased bone healing) and proximal femoral endoprosthetic replacement (resects the disease, durable, immediate stability, but bigger operation). Choice depends on bone destruction, primary tumour, survival estimate and surgeon experience - no high-level RCT exists.
Fixing an impending fracture is technically easier, allows shorter stay and better function than fixing after the bone breaks - but a proportion of prophylactically fixed bones would never have fractured, so some patients are over-treated. Balancing over-treatment against the morbidity of a completed pathological fracture remains judgement-based.
Protecting the whole bone with long intramedullary implants reduces reoperation, but reaming/insertion carries a real fat/tumour embolic risk (around 12% non-fatal physiologic events). Whether to always span the entire bone, or to accept a shorter construct in frail patients, is unresolved (Alvi & Damron).
Postoperative radiotherapy improves function and reduces reoperation, but the optimal regimen (single fraction vs 30 Gy in 10, exact timing, whether to irradiate the whole implant) is not standardised and varies between guidelines and registries.
Hypervascular renal and thyroid metastases bleed heavily and carry higher local progression risk after nailing. The roles of preoperative embolisation and of resection/endoprosthesis versus simple fixation are debated and depend on local resources.
MCQ Practice Points
Q: What Mirels' score indicates prophylactic fixation? A: Score ≥8 - Mirels' score ≥8 = prophylactic fixation recommended. Score ≥9 = 33% fracture risk within 6 months, ≥10 = 50% risk. Components: Site (1-3), Pain (1-3), Lesion (1-3), Size (1-3).
Q: What is the minimum life expectancy for surgery to be beneficial in pathological fractures? A: 3-6 months - Surgery beneficial if life expectancy over 3-6 months. Use Katagiri or PATHFx score to estimate. If under 3 months, consider non-operative (palliative care).
Q: What are the key surgical principles for pathological fractures? A: Fix normal bone to normal bone, bypass lesion by ≥2 cortical diameters, cement augmentation for lytic lesions, construct must outlast patient - IMN for diaphyseal, arthroplasty for periarticular. Allow immediate weight bearing.
Q: What are the most common primary tumors metastasizing to bone? A: Breast, Lung, Prostate, Kidney, Thyroid (BLT with Kosher Pickle - BL P K T) - Breast most common. Lytic: lung, kidney, thyroid. Blastic: prostate. Mixed: breast.
Q: What is the postoperative radiation protocol for pathological fractures? A: Commonly 30 Gy in 10 fractions, around 2-3 weeks postop - Adjuvant radiotherapy independently improves and maintains functional status and reduces reoperations to the treated site (Townsend). Coordinate with radiation oncology.
Q: What is the nonunion rate in pathological fractures? A: Common (radiotherapy impairs bony healing) - but not problematic if construct stable. Durable fixation matters more than biological healing; radiographic nonunion is acceptable if the patient is comfortable and functional.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 60-year-old woman with known breast cancer and bone metastases presents with increasing right thigh pain. She has difficulty walking due to pain. X-ray shows a large lytic lesion in the femoral shaft involving 70% of the cortex. The lesion is in the lower limb, and she has moderate pain that affects her activities.”
“A 65-year-old man with known prostate cancer and multiple bone metastases presents after a fall. He has a complete pathological fracture through the proximal femur with femoral head and neck involvement. He is otherwise healthy and ambulatory. CT shows blastic metastases throughout skeleton but no visceral metastases.”
“A 45-year-old previously well man presents with 3 months of progressive thigh pain and a limp. There is no history of cancer. AP and lateral radiographs show a single destructive lesion in the proximal femoral diaphysis with cortical destruction, a hint of periosteal reaction and an associated soft-tissue shadow. The on-call team asks whether they should book him for an intramedullary nail.”
Key Concepts
- Pathological fracture = fracture through abnormal bone weakened by disease
- Treatment is palliative (not curative) - restore function, relieve pain, improve quality of life
- Most common primaries: Breast, Lung, Prostate, Kidney, Thyroid (BLT K P)
- Lytic: lung, kidney, thyroid, breast. Blastic: prostate. Mixed: breast
Mirels' Score
- Site: Upper limb 1, Lower limb 2, Peritrochanteric 3
- Pain: Mild 1, Moderate 2, Functional 3
- Lesion: Blastic 1, Mixed 2, Lytic 3
- Size: Under 1/3 cortex 1, 1/3-2/3 is 2, over 2/3 is 3
- Score ≥8 = prophylactic fixation, ≥9 = 33% risk, ≥10 = 50% risk
Treatment Algorithm
- Life expectancy over 3-6 months = surgery beneficial (use Katagiri or PATHFx score)
- Mirels' score ≥8 (impending) or complete fracture = surgical fixation
- Diaphyseal lesion: IMN + cement augmentation
- Periarticular lesion: Arthroplasty (cemented) with long stem
Surgical Pearls
- Fix normal bone to normal bone
- Bypass lesion by ≥2 cortical diameters (4x bone diameter)
- Cement augmentation for lytic lesions (40-80g PMMA)
- Long implant (proximal to distal metaphysis)
- Allow immediate weight bearing
Complications
- Nonunion common (not problematic if construct stable)
- Reoperation for fixation failure ~6% (prevent with adequate bypass, cement)
- Local progression ~5% at 12 months (higher in renal cell; reduced by radiotherapy)
- Embolic complications ~12% with long intramedullary implants
Evidence Base
Mirels' Score (Original Description)
- Components: Site (1-3), Pain (1-3), Lesion type (1-3), Size (1-3); range 4-12
- Mean score 7 in non-fracture group vs 10 in fracture group
- Score 8 or higher = prophylactic fixation recommended before irradiation
Revised Katagiri Prognostic Scoring System
- Six weighted factors; primary lesion, visceral/cerebral mets and abnormal labs carry the largest weight
- Score 7 or higher: 27% survival at 6 months, 6% at 1 year
- Score 3 or lower: 91% survival at 1 year, 78% at 2 years
PATHFx External Validation
- AUC 0.80-0.83 for 3-, 6- and 12-month survival predictions
- Validated across Western and Asian cohorts - generalisable decision-support tool
- Best used to guide surgical decisions at 3, 6 and 12 months rather than 1 month
Surgical Principles (Prophylactic Fixation)
- More than 50% cortical destruction (or a proximal femoral lesion over 2.5 cm) = high fracture risk
- Prophylactic fixation prevents secondary fracture and its high non-union risk
- Augment fixation with debulking plus methylmethacrylate to restore load-sharing and improve radiotherapy efficacy
Postoperative Radiotherapy After Stabilisation
- Postoperative radiotherapy independently predicted good functional status (53% vs 11.5%)
- Fewer reoperations to the treated site with adjuvant radiotherapy
- Median survival 12.4 vs 3.3 months (likely partly selection bias)
Length of Fixation and Reoperation Risk
- Reoperation for symptomatic failure 6.3% with a bone-protecting (long-implant) strategy
- New disease distant from the index lesion in only 1 of 96 bones
- Embolic-type complications from long implants (12.5%) must be weighed against reoperation risk
Local Progression After Intramedullary Nailing
- Local progression around the nail was low (4.9% at 12 months)
- Only 2% underwent reoperation for local progression
- Renal cell carcinoma carries higher progression risk - consider resection/alternative reconstruction