Metastatic Disease | Mirels Score | Prophylactic Fixation | Workup First
- Workup First: Never fix a pathological fracture without knowing the primary (unless impending emergency). Biopsy track might spread tumor.
- BLT with a Kosher Pickle: Breast, Lung, Thyroid, Kidney, Prostate (Most common bone mets).
- Renal/Thyroid tumors: Highly vascular & Radio-resistant. Pre-op embolization often needed.
- Survival Estimate: Fixation should outlast the patient's life expectancy (durable construct).
- Fixation Logic: Fixation spans the whole bone (prevent new fractures). Cement augmentation improves stability.
- “Always ask about constitutional symptoms (weight loss, night sweats)
- “Solitary lesion greater than 40y is Mets/Myeloma until proven otherwise
- “Solitary lesion less than 20y is Primary Bone Tumor until proven otherwise
- “Do not nail a primary bone sarcoma (contaminates whole compartment)
Biopsy Trap: If the primary is unknown, DO NOT perform internal fixation. You must stage and biopsy first. An inappropriate nail can upstage a sarcoma to Stage IV or necessitate amputation.
Renal & Thyroid: These metastases are significantly vascular. Pre-operative embolization is mandatory to prevent exsanguination on the table.
Know it cold: Site, Pain, Lesion Type, Size. This is the gold standard answer for "When to operate prophylactically".
Span the Bone: Disease can progress elsewhere. Use a long IM nail or long plate to protect the entire humerus, not just the lesion.
- Fracture Status
- None (Impending)
- Primary Known
- Yes
- Treatment
- Radiotherapy
- Fracture Status
- Impending
- Primary Known
- Yes
- Treatment
- Prophylactic Nail/Plate
- Fracture Status
- Complete
- Primary Known
- Yes
- Treatment
- Acute Fixation + Post-op RT
- Fracture Status
- Any
- Primary Known
- NO (Unknown)
- Treatment
- Workup first (Biopsy)
BLT-KPCommon Bone Metastases
Hook:BLT with a Kosher Pickle for lunch.
SPLSMirels Score Components
Hook:Some People Like Statistics.
CRABMultiple Myeloma Features
Hook:Beware the CRAB in patients over 40 with back pain.
Overview
Pathological fractures of the humerus occur when bone weakened by disease (cystic, metabolic, or neoplastic) fails under physiological loads. In adults over 40, metastatic disease and myeloma are the overwhelming causes. The humerus is the second most common site for long bone metastases (after femur).

Incidence:
- Bone is the 3rd most common site of metastatic disease.
- Humerus involvement: 20% of bone mets.
- Increasing due to improved cancer survival rates.
Survival (Median):
- Prostate/Breast: Years (24-36 months).
- Renal/Thyroid: Intermediate (12 months).
- Lung: Short (less than 6 months).
- Fixation must be durable enough for expected survival.
Anatomy and Pathophysiology
Pathophysiology of Metastasis
- Tumor emboli deposit in vascular marrow (Red marrow).
- Batson's Plexus (low pressure venous system) facilitates spread.
- Cytokines (RANKL/PTHrP) stimulate osteoclasts.
- Lytic: Lung, Renal, Thyroid, Breast (mixed), Myeloma. Bone destruction leads to Fracture.
- Blastic: Prostate, Breast (mixed). Bone formation leads to Brittle bone.
Lytic lesions are more prone to fracture and harder to fix.
Classification
Mirels Scoring System
Used to predict fracture risk in impending pathological fractures.
- Score 1
- Upper Limb
- Score 2
- Lower Limb
- Score 3
- Peritrochanteric
- Score 1
- Mild
- Score 2
- Moderate
- Score 3
- Functional
- Score 1
- Blastic
- Score 2
- Mixed
- Score 3
- Lytic
- Score 1
- Less than 1/3
- Score 2
- 1/3 - 2/3
- Score 3
- Greater than 2/3
Score Calculation: Sum of all 4 variables. Minimum 4, Maximum 12.
- Fracture Risk
- 0-4%
- Recommendation
- Radiotherapy / Observation
- Fracture Risk
- 15%
- Recommendation
- Clinical Judgement
- Fracture Risk
- 33%
- Recommendation
- Prophylactic Fixation
Mirels score applies to metastatic disease in long bones. It does NOT apply to primary bone tumors or spinal metastases.
History
Key Questions:
- Known history of cancer?
- Constitutional symptoms: Weight loss, night sweat, fatigue.
- Pain history: Mechanical ( fracture) vs Biological (night pain).
- Functional demand.
Night pain typically indicates active tumor.
Examination
- Soft tissue mass? (Sarcoma concern).
- Previous mastectomy scars?
- Thyroid enlargement?
- Radial nerve commonly involved in humeral shaft fractures.
- Check Lymph nodes (Axillary/Supraclavicular).
Examination focuses on finding a primary source.
Investigations
Imaging & Staging
- "Moth-eaten" or "Permeative" appearance.
- Cortical destruction.
- Pathological fracture (transverse, minimal trauma).
- Chest/Abdomen/Pelvis (Staging).
- Defines bone stick remaining.
- Identifies other skeletal metastases.
- Solitary vs Multiple (Prognostic).
Complete staging is mandatory.
Differential Diagnosis
A destructive humeral lesion in an adult is metastasis or myeloma until proven otherwise, but the differential changes dramatically with age and imaging. Distinguishing these before any fixation is the single most important decision.
- Typical Age
- Over 40
- Imaging Clue
- Multiple lytic/mixed lesions, moth-eaten
- Key Discriminator
- Known primary or constitutional symptoms
- Typical Age
- Over 50
- Imaging Clue
- Punched-out lytic lesions, cold on bone scan
- Key Discriminator
- Positive SPEP/free light chains, CRAB features
- Typical Age
- Under 30 (or any age)
- Imaging Clue
- Aggressive periosteal reaction, soft-tissue mass
- Key Discriminator
- Solitary aggressive lesion, no primary on staging
- Typical Age
- Any
- Imaging Clue
- Permeative lesion, large soft-tissue component
- Key Discriminator
- Tissue diagnosis; often radiosensitive
- Typical Age
- Under 30
- Imaging Clue
- Well-defined, non-aggressive margin
- Key Discriminator
- No cortical breach, no soft-tissue mass
The decisive distinction is metastasis/myeloma (fix it) versus primary bone sarcoma (do NOT touch it without an oncology MDT). When the primary is unknown, treat every solitary lesion as a potential sarcoma until staging and biopsy say otherwise.
Management Algorithm
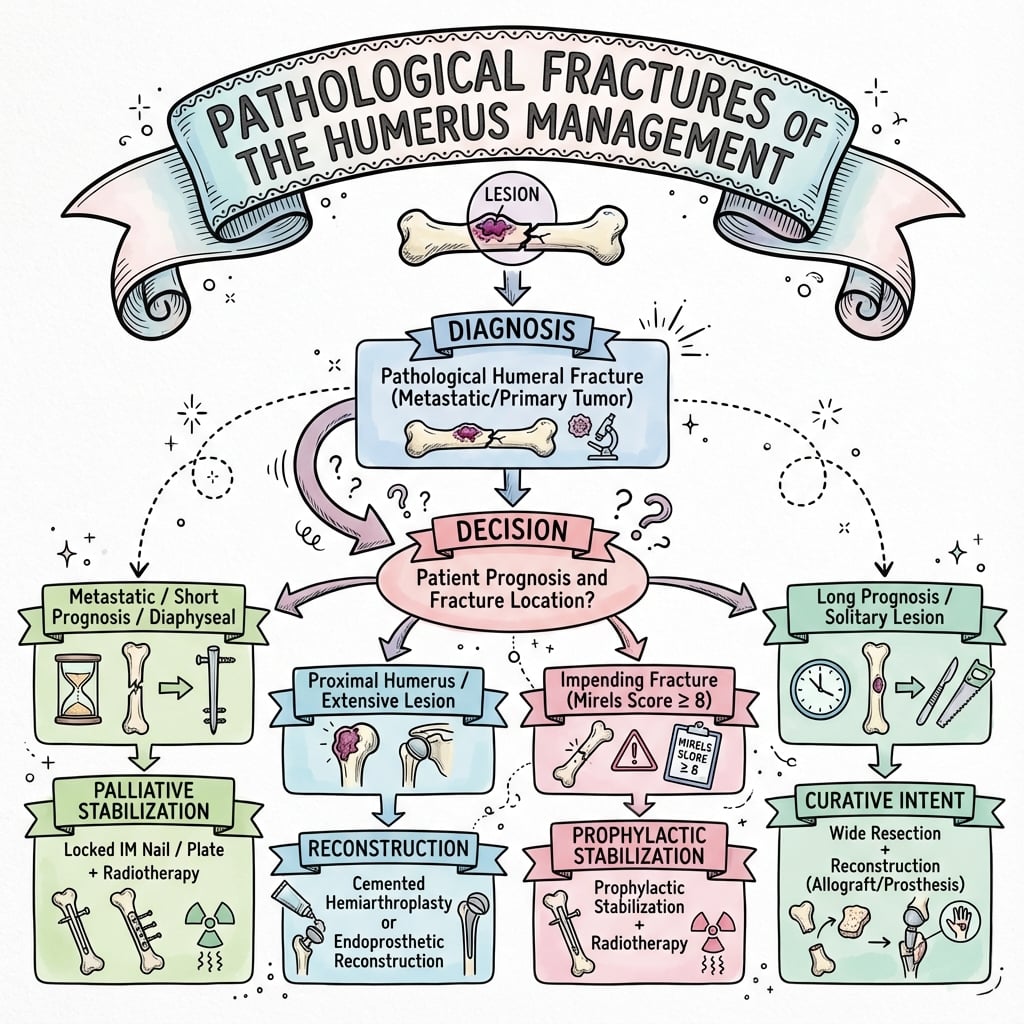
Treatment Decision Making
- Low Mirels score (less than 8).
- Terminally ill (Life expectancy less than 6 weeks).
- Non-displaced fracture in severe comorbidities.
- Radiosensitive tumor (Myeloma/Lymphoma/Small Cell Lung).
- Radiotherapy (RT).
- Functional bracing.
- Bisphosphonates.
Pain relief is the primary goal.
Surgical Technique
Fixation Strategy
- Load sharing device.
- Prophylactic or Acute.
- Reaming: Careful! Can spread tumor or cause fat embolism.
- Locking: Static locking (proximal and distal). Or Cement screw augmentation.
Minimally invasive, preserves soft tissue, immediate stability.
The Radial Nerve: The Humerus-Specific Pitfall
The examination section flags that "the radial nerve is commonly involved in humeral shaft fractures" and the cheat sheet warns against "ignoring the radial nerve in percutaneous nailing," but the humerus's signature neurovascular structure deserves development — it is what makes fixing a pathological humerus different from any other long bone.
Three reasons it matters here:
- A pre-existing palsy. A pathological shaft lesion at the spiral groove (or the fracture through it) can cause a radial nerve palsy from tumour infiltration, compression or the fracture itself. Document active wrist, finger and thumb extension and first-dorsal-web-space sensation before any intervention — this is both planning and medicolegal protection.
- Iatrogenic risk. The nerve runs in the spiral groove on the posterolateral shaft and is at risk during open plating (particularly posterior approaches and distal-third exposure), during percutaneous or distal interlocking screw placement, and from retraction — all made harder when tumour distorts the normal anatomy.
- Approach choice. Plan the construct around the nerve: an antegrade intramedullary nail avoids open dissection over the nerve along the shaft (but distal interlocking screws still endanger it — place them with the nerve in mind, open if necessary), whereas open plating mandates identifying and protecting the radial nerve, and a posterior approach requires formally exposing it.
Document radial nerve function (wrist/finger/thumb extension, first-web sensation) before any fixation of a pathological humerus. The nerve lies in the spiral groove and is threatened by the tumour, the fracture, open plating and distal interlocking — identify and protect it, and never be left explaining a post-operative palsy you never checked for pre-operatively.
Complications
Potential Complications
Local Recurrence: If RT is not given post-op, tumor continues to grow and destroys fixation. Hardware failure is inevitable if patient survives long enough.
Intra-operative Hemorrhage: Especially Renal Cell/Thyroid. Embolize pre-op!
Radiation Effect: RT inhibits bone healing. Pathological fractures often rely on the hardware for life (union is not guaranteed).
Fat/Tumor Embolism: Reaming increases intramedullary pressure. Vent the canal or use unreamed nails in high-risk pulmonary patients.
Postoperative Care
Rehabilitation Protocol
- Sling for comfort.
- Immediate use: Construct should allow weight bearing (as tolerated).
- No restrictions usually (construct must be strictly stable).
- Radiotherapy planning begins (once wound dry).
- Bisphosphonate therapy (Zoledronic acid / Denosumab).
- Surveillance for hardware failure.
- Systemic therapy for underlying disease.
Post-operative Radiotherapy to the Whole Implant
The topic states throughout that post-operative radiotherapy follows fixation, that it should cover "the whole implant," and that "if RT is not given, the tumour continues to grow and destroys the fixation" — the rationale and its orthopaedic consequences deserve to be assembled, because it is a stock examiner question after "how would you fix it?"
Why irradiate, and why the whole bone. Surgery for metastatic disease is palliative and deliberately leaves tumour behind. Post-operative radiotherapy to the entire instrumented field controls the residual and microscopic disease along the canal and around the implant; irradiating only the original lesion risks progression elsewhere along the instrumented bone that would ultimately destroy the construct. This is the reason both for spanning the whole bone surgically and for radiating the whole implant.
Timing. Radiotherapy is started once the wound has healed (commonly around 2 to 3 weeks post-operatively) to avoid wound-healing complications.
The double-edged effect on bone. Radiotherapy impairs osteoblast function and bone healing, so a pathological fracture fixed in irradiated tumour bone may never unite. The corollary defines the whole philosophy of this operation: the construct must be durable enough to outlast the patient independent of bony union — mechanical durability, not biological healing, is the goal (the basis of the Capanna and Katagiri prognosis-matched approach). Antiresorptive therapy (a bisphosphonate or denosumab) complements radiotherapy in reducing skeletal-related events. (Detailed radiotherapy dose/fractionation is developed in the radiotherapy for musculoskeletal tumours topic.)
After fixation, give post-operative radiotherapy to the entire implant/bone (once the wound has healed) to sterilise residual tumour along the construct and stop it destroying the fixation. But radiotherapy also blocks bone healing, so the metalwork — not union — must carry the limb for life: build a construct durable enough to outlast the patient.
Outcomes
Prognosis
- Pain Relief: Excellent (80-90% improvement) after fixation.
- Function: Restoration of ability to feed/groom.
- Ambulatory: Upper limb fixation allows use of walking aids.
- Hardware Failure: 5-10%, usually due to disease progression or long survival.
Guidelines, Registries & Global Practice
Global epidemiology: Bone is the third most common site of metastatic disease after lung and liver, and the humerus is the second most common long bone affected after the femur (around 20% of long-bone metastases). Breast, lung, thyroid, renal and prostate cancers account for the overwhelming majority. Rising cancer survival worldwide is increasing the absolute burden of skeletal metastases.
- Position on Metastatic Bone Disease
- Endorse Mirels and Harrington criteria; durable fixation that spans the bone, with postoperative radiotherapy to the whole implant
- Position on Metastatic Bone Disease
- British Orthopaedic Oncology Society guidance: discuss all suspected bone tumours with a specialist centre before fixation; biopsy unknown primaries first
- Position on Metastatic Bone Disease
- Metastatic spinal cord compression pathway emphasises urgent imaging and surgery for instability (mirrors Patchell principle)
- Position on Metastatic Bone Disease
- Load-sharing intramedullary fixation or cement-augmented plating; whole-bone protection
- Position on Metastatic Bone Disease
- Multidisciplinary tumour board, prognosis-adapted reconstruction (simple fixation vs endoprosthesis)
National sarcoma and bone-tumour registries (e.g. EMSOS in Europe) and arthroplasty registries (NJR, AOANJRR) track endoprosthetic survival for proximal humeral replacement. Implant survival is generally limited by patient survival rather than mechanical failure in this palliative population.
- Well-resourced settings: Routine pre-operative embolisation for renal/thyroid metastases, ready access to modular endoprostheses, denosumab/zoledronic acid, and same-admission radiotherapy planning.
- Limited-resource settings: Reliance on conventional nails and bone cement; embolisation and endoprostheses may be unavailable, shifting practice toward plate-and-cement constructs and external bracing; antiresorptive therapy access is variable.
A universal principle across all settings: never fix a destructive bone lesion of unknown origin without staging and, where indicated, biopsy.
Controversies & Areas of Uncertainty
Mirels has high sensitivity but low specificity, so a score of 9 or more over-predicts fracture and may lead to over-treatment. A score of 8 remains a clinical-judgement grey zone where functional demand and prognosis drive the decision.
No randomised data favours intramedullary nailing over locked plating with cement augmentation for the humeral shaft. Nail protects the whole bone; plate allows debulking and direct lesion control. Choice is lesion-location and surgeon dependent.
Whether to ream remains debated. Reaming improves nail fit but raises intramedullary pressure and theoretical tumour/fat embolism risk; many advocate venting or unreamed nails in patients with poor pulmonary reserve.
For a solitary metastasis from a favourable primary, the balance between palliative fixation and wide resection with endoprosthetic reconstruction is unsettled and should be an oncology MDT decision based on prognosis.
MCQ Practice
Self-Assessment Questions
Q: Which factor is weighted most heavily (highest score) in the Mirels scoring system for "Site"?
- A) Humerus
- B) Radius
- C) Femoral Shaft
- D) Peritrochanteric region
- E) Tibia
A: D - The Peritrochanteric region is assigned a score of 3 due to the high biomechanical loads and consequences of failure. Upper limb is 1, Lower limb (shaft) is 2.
Q: What is the most common source of bone metastasis in women?
- A) Lung
- B) Thyroid
- C) Breast
- D) Kidney
- E) Cervix
A: C - Breast cancer is the most common source of bone metastases in women (about 70%). Prostate is most common in men.
Q: Which primary tumor gives rise to highly vascular bone metastases requiring pre-operative embolization?
- A) Breast
- B) Prostate
- C) Renal Cell Carcinoma
- D) Lung
- E) Melanoma
A: C - Renal Cell and Thyroid carcinomas are classically highly vascular. Pre-operative embolization is recommended to control bleeding.
Q: A Mirels score of 10 indicates:
- A) Low risk of fracture (less than 4%)
- B) Moderate risk, Observation indicated
- C) High risk, Prophylactic fixation indicated
- D) Imminent death
- E) Need for amputation
A: C - A score of 9 or greater indicates a high risk of fracture (greater than 33%) and is the threshold for recommending prophylactic fixation.
Q: Internal fixation of a pathological fracture is potentially contraindicated if:
- A) The patient has multiple metastases
- B) The primary tumor is unknown (solitary lesion)
- C) The Mirels score is 12
- D) The fracture is displaced
- E) The patient is on bisphosphonate therapy
A: B - If the primary is unknown and the lesion is solitary, internal fixation (nailing) is contraindicated until a primary bone sarcoma is ruled out via biopsy/staging, to avoid compartment contamination.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“You are called to ED for a 60-year-old male with a solitary lytic lesion of the humerus and a fracture. He has no history of cancer. What is your plan?”
“Describe the Mirels Score and how you use it.”
“How do you manage a pathological humerus fracture from Renal Cell Carcinoma?”
Key Facts
- Causes: Breast, Lung, Thyroid, Kidney, Prostate
- Threshold: Mirels score greater than 9
- Trap: Solitary lesion (Unknown primary) = STOP
- Vascular: Renal/Thyroid (Embolize)
- Fixation: Durable (Nail or Cemented Plate)
- Survival: Fixation must last longer than the patient
Mirels Score (SPLS)
- Site (Upper/Lower/Troch)
- Pain (Mild/Mod/Func)
- Lesion (Blastic/Mixed/Lytic)
- Size (less than 1/3, 1/3-2/3, greater than 2/3)
Surgical Steps
- Positioning (Beach chair/Supine)
- Approach (Deltopectoral/Split)
- Biopsy (If needed, frozen section)
- Reaming (Gentle/Unreamed if pulmonary risk)
- Nail Insertion (Span whole bone)
- Cement Augmentation (If proximal/distal voids)
- Closure (Layered)
Common Pitfalls
- Nailing a primary sarcoma
- Missing hypercalcemia
- Underestimating bleeding in Renal mets
- Inadequate fixation length (Must span bone)
- Ignoring radial nerve in percutaneous nailing
Examiner Favorites
- Calculate Mirels for this X-ray...
- Workup of solitary lesion
- Role of radiotherapy vs surgery
- Mechanism of bisphosphonates
- What to do if fixation fails?
Evidence Base
Key Studies
Mirels - Scoring System for Impending Fractures
- Retrospective analysis of 78 irradiated metastatic long-bone lesions (27 fractured, 51 did not)
- Four weighted variables: site, pain, lesion type, size (range 4-12)
- Mean score 7 in non-fracture group vs 10 in fracture group; risk rises progressively above 7
- Lesions scoring 7 or lower safely irradiated; 8 or higher recommended for prophylactic fixation
Capanna & Campanacci - Appendicular Metastasis Treatment
- Comprehensive framework for surgical treatment of appendicular skeletal metastases
- Stratifies fixation by life expectancy and solitary vs multiple disease
- Promotes durable load-bearing constructs (cement augmentation, endoprosthesis) over biological union
- Solitary metastasis from favourable primaries (renal, thyroid) considered for wide resection
Katagiri et al. - Prognostic Scoring
- 350 patients with skeletal metastases; Cox model identified 5 survival factors
- Factors: primary site, poor performance status (ECOG 3-4), visceral/cerebral mets, prior chemotherapy, multiple bone mets
- Score 6 or more: 31% survival at 6 months, 11% at 1 year; score 2 or less: 98% at 6 months, 89% at 1 year
- Guides choice between simple palliative fixation and durable reconstruction
Patchell et al. - Surgery + Radiation vs Radiation
- Randomised trial (n=101) in metastatic spinal cord compression; principle applies to mechanical instability generally
- Surgery plus RT vs RT alone: 84% vs 57% able to walk after treatment (OR 6.2, p=0.001)
- Surgery group retained ambulation far longer (median 122 vs 13 days) and needed fewer steroids/opioids
- Trial stopped early at interim analysis for surgical superiority
Harrington - Criteria for Prophylactic Fixation
- Established the classic indications for prophylactic fixation of lytic metastatic lesions
- Lesion 2.5 cm or larger in size
- Destruction of 50% or more of the cortex
- Persistent local pain with loading despite adequate radiotherapy
Arpornsuksant et al. - Local Progression After IM Nailing
- 122 patients with long-bone metastases (humerus 27%) treated by intramedullary nail
- Cumulative local tumour progression only 4.9% at 12 months; reoperation in 2%
- Renal cell carcinoma (OR 5.1) and older age were the only factors linked to progression
- No survival difference between those with and without local progression