Posterior Tibial Avulsion | Posterior Approach | Screw or Suture Fixation
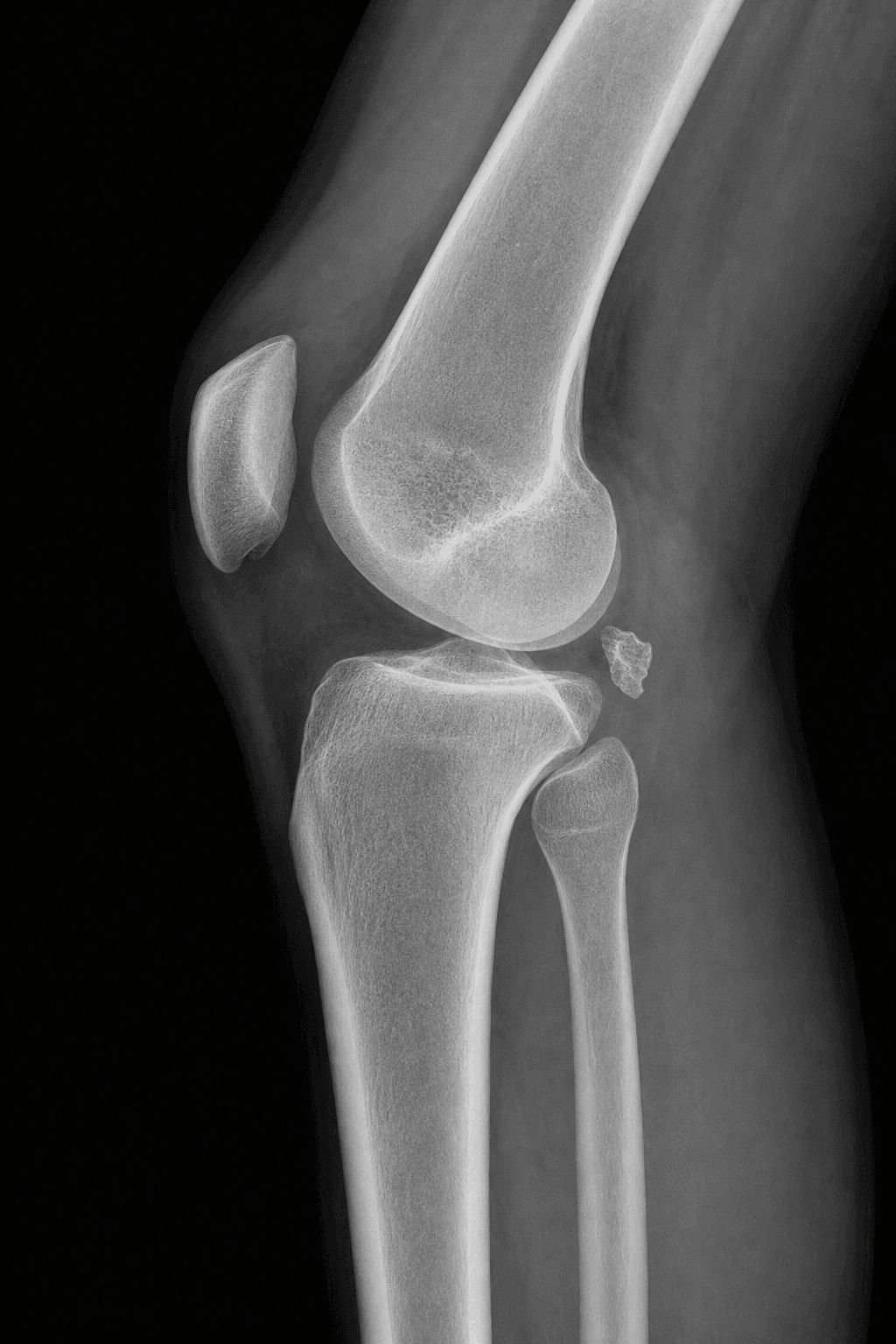
- PCL avulsion fracture = PCL avulses from posterior tibia with bone fragment (better prognosis than midsubstance tear)
- Posterior approach - patient prone, popliteal vessels at risk, must protect neurovascular bundle
- Optimal timing: Within 3 weeks - earlier fixation has better outcomes (85-95% good results)
- Fixation options: Screw (large fragment) or suture anchors (small fragment) - both achieve excellent outcomes
- Advantage over reconstruction: Bony healing is faster and more reliable than ligament reconstruction
- “PCL avulsion fracture = PCL avulses from posterior tibia with bone fragment - better prognosis than midsubstance tear
- “Posterior approach with patient prone - popliteal artery at risk, must protect neurovascular bundle
- “Optimal timing within 3 weeks - earlier fixation achieves 85-95% good results
- “Screw fixation for large fragments, suture anchors for small fragments - both excellent outcomes
PCL avulsion fracture has better prognosis than midsubstance PCL tear. Bony healing is faster and more reliable than ligament reconstruction. 85-95% good results with proper fixation. Always attempt fixation if fragment is adequate.
Posterior approach with patient prone - popliteal artery and tibial nerve at risk. Must protect neurovascular bundle. Use posterior midline or posteromedial approach. Identify vessels before any dissection.
Within 3 weeks for best outcomes - earlier fixation achieves 85-95% good results. Delayed fixation (over 6 weeks) may require reconstruction instead of fixation. Timing is critical for success.
Screw fixation (large fragment) or suture anchors (small fragment) - both achieve excellent outcomes. Screw provides compression, suture anchors for small or comminuted fragments. Choose based on fragment size.
- Timing
- Within 3 weeks
- Fixation Method
- Screw fixation
- Outcome
- 85-95% good results
- Timing
- Within 3 weeks
- Fixation Method
- Suture anchors
- Outcome
- 85-95% good results
- Timing
- Within 3 weeks
- Fixation Method
- Suture anchors
- Outcome
- 80-90% good results
- Timing
- Over 6 weeks
- Fixation Method
- May need reconstruction
- Outcome
- 60-80% good results
Overview and Epidemiology
PCL avulsion fractures occur when the PCL avulses from its insertion on the posterior tibia, taking a bone fragment with it. This is better than midsubstance PCL tears because bony healing is faster and more reliable than ligament reconstruction. Treatment involves surgical fixation via posterior approach.
Mechanism of Injury
Dashboard injury (classic mechanism):
- Motor vehicle accident: Knee strikes dashboard with knee flexed
- Posterior force: Posteriorly directed force on proximal tibia
- PCL avulses: PCL insertion on posterior tibia avulses with bone fragment
- High energy: Usually high-energy trauma
Other mechanisms:
- Hyperflexion: Extreme knee flexion
- Direct trauma: Posterior blow to proximal tibia
- Fall: Landing on flexed knee
The PCL inserts on the posterior tibia, 1-1.5cm below the joint line. When excessive posterior force is applied, the PCL avulses from the tibia, taking a bone fragment with it.
PCL avulsion fracture has better prognosis than midsubstance PCL tear. Bony healing is faster and more reliable than ligament reconstruction. 85-95% good results with proper fixation vs 60-80% for midsubstance tears. Always attempt fixation if fragment is adequate.
Epidemiology
- Incidence: 5-10% of PCL injuries
- Age: Peak 20-40 years (trauma population)
- Gender: Male predominance (3:1 ratio)
- Laterality: Usually unilateral
- Associated injuries: PLC injury (20-30%), ACL injury (10-15%), meniscal tears (10-20%)
Anatomy and Pathophysiology
PCL Anatomy
The posterior cruciate ligament (PCL):
- Origin: Posteromedial lateral femoral condyle (intercondylar notch)
- Insertion: Posterior tibia, 1-1.5cm below joint line (posterior intercondylar area)
- Two bundles: Anterolateral (AL) and posteromedial (PM)
- Blood supply: Middle genicular artery
- Function: Primary restraint to posterior tibial translation (95% at 90 degrees flexion)
PCL insertion site:
- Location: Posterior tibia, 1-1.5cm below joint line
- Size: 1-2cm area
- Relationship: Close to popliteal artery (separated by popliteus muscle)
- Bone quality: Good cancellous bone for fixation
Pathophysiology
Avulsion mechanism:
- Posterior force: Excessive posterior force on proximal tibia
- PCL tension: PCL experiences excessive tension
- Bone weaker than ligament: In some cases, bone-ligament interface fails
- Avulsion: PCL avulses from tibia with bone fragment
Why avulsion is better:
- Bony healing: Faster and more reliable than ligament healing
- Anatomic: Can restore native PCL insertion
- Outcomes: 85-95% good results vs 60-80% for midsubstance tears
- Timing: Earlier fixation has better outcomes
Fragment characteristics:
- Size: Usually 1-2cm (varies)
- Location: Posterior tibia, PCL insertion site
- Quality: Usually good bone quality
- Displacement: Usually displaced posteriorly
Popliteal artery lies directly posterior to the tibia, separated by only the popliteus muscle. During posterior approach, the neurovascular bundle must be carefully protected. Tethering at the soleal arch makes it vulnerable to injury with posterior displacement.
Classification Systems
Fragment Size Classification
Large fragment (over 1cm):
- Usually single fragment
- Good bone quality
- Treatment: Screw fixation (compression)
- Outcomes: 85-95% good results
Small fragment (under 1cm):
- May be single or multiple fragments
- Treatment: Suture anchors
- Outcomes: 85-95% good results
Comminuted:
- Multiple fragments
- May be difficult to fix
- Treatment: Suture anchors or reconstruction
- Outcomes: 80-90% good results
Fragment size determines fixation method and predicts outcomes.
Clinical Assessment
History
Mechanism: Dashboard injury (classic)
- Motor vehicle accident (knee strikes dashboard)
- Posterior force on proximal tibia
- High-energy trauma
Symptoms:
- Immediate pain and swelling
- Inability to bear weight
- Knee "giving way" (instability)
- Posterior knee pain
Physical Examination
Inspection:
- Knee effusion (hemarthrosis)
- Antalgic gait
- Knee held in slight flexion
Palpation:
- Tenderness over posterior knee
- Posterior tibial step-off (abnormal - normal is 1cm anterior)
Range of Motion:
- Limited flexion (pain, effusion)
- Limited extension (pain, effusion)
Ligament Testing:
- Posterior drawer: Positive (posterior translation) - most sensitive
- Posterior sag sign: Positive (tibia sags posteriorly)
- Quadriceps active test: Positive (tibia reduces with quadriceps contraction)
- Dial test: May be positive (if PLC injured)
Posterior drawer test is most sensitive for PCL injury - assess posterior tibial translation and endpoint quality. Normal tibial step-off is 1cm anterior to femoral condyle. PCL injury causes posterior translation.
Associated Injuries
- PLC injury: 20-30% (posterolateral corner)
- ACL injury: 10-15%
- Meniscal tears: 10-20%
- Bone bruises: Anterior tibia, anterior femur (kissing contusion pattern)
Differential Diagnosis
- Key Distinguishing Feature
- Posterior drawer/sag with bony fragment at posterior tibial insertion
- Confirming Investigation
- Lateral radiograph + CT (fragment, displacement)
- Key Distinguishing Feature
- Posterior sag/drawer but no bony fragment
- Confirming Investigation
- MRI (discontinuous PCL fibres, no avulsed bone)
- Key Distinguishing Feature
- Increased external rotation (dial test) at 30 degrees, varus laxity
- Confirming Investigation
- MRI; stress radiographs; examine before attributing all laxity to PCL
- Key Distinguishing Feature
- Lateral capsular/anterolateral fragment, not posterior insertion
- Confirming Investigation
- AP radiograph + CT
- Key Distinguishing Feature
- Gross instability, dimple sign, vascular compromise
- Confirming Investigation
- Urgent ABI/CT angiography - exclude before elective fixation
- Key Distinguishing Feature
- Tibial spine/physeal avulsion rather than PCL insertion
- Confirming Investigation
- Radiograph + MRI to define physis
Investigations
Standard X-ray Protocol
Views: AP and lateral knee.
Key findings:
- PCL avulsion fragment: Visible on lateral view (posterior tibia)
- Fragment size: Assess size and displacement
- Posterior tibial step-off: Abnormal (normal is 1cm anterior)
- Associated fractures: Tibial plateau, femoral condyle
Lateral view is critical - shows fragment and posterior displacement.
Associated Bony Avulsion Signs
The posterior tibial fragment is the diagnostic lesion, but two secondary avulsion signs on plain films flag the concomitant injuries that change the operation. Both are easily confused with the classic (lateral, ACL-associated) Segond fracture listed in the differential above, so they are worth learning as a set.
Reverse Segond Fracture
- What it is: a small cortical avulsion off the medial tibial plateau margin, at the attachment of the deep medial collateral ligament / medial capsule — the mirror image of the classic lateral Segond fleck.
- Why it matters: the reverse Segond is strongly associated with PCL injury and a medial meniscus tear, whereas the classic lateral Segond signals ACL injury. Spotting a medial-margin fleck on the AP film should trigger a deliberate search for the posterior tibial PCL avulsion and MRI assessment of the medial meniscus.
- Mechanism: valgus with external rotation, distinct from the posterior-drawer dashboard mechanism of the isolated PCL fragment, but often part of the same high-energy event.
Arcuate (Fibular Styloid) Sign
- An avulsion fleck off the fibular styloid at the arcuate-complex insertion signals a posterolateral corner (PLC) injury, which co-exists with PCL injury in a meaningful minority of cases.
- Full PLC evaluation and reconstruction is owned by the dedicated posterolateral-corner-injuries topic; here the teaching point is that a tiny fibular-head fleck alongside a posterior tibial fragment means "not an isolated PCL avulsion — look for combined instability."
A medial tibial-plateau fleck (reverse Segond) points to PCL plus medial meniscus injury; a fibular-styloid fleck (arcuate sign) points to a posterolateral corner injury. Either finding converts an apparently isolated PCL bony avulsion into a combined injury that alters the surgical plan — always inspect the medial plateau margin and the fibular styloid before assuming the lesion is isolated.
PCL AVULSIONPCL Avulsion Fracture Features
Hook:PCL AVULSION: Posterior approach, Critical timing (3 weeks), Large fragment = screw, Anchors for small, Vessels at risk, Under 3 weeks optimal, Ligament better than midsubstance, Screw or suture both good, Identify vessels first, Outcomes 85-95%, Non-weight bearing 6 weeks!
Management Algorithm
Management Pathway
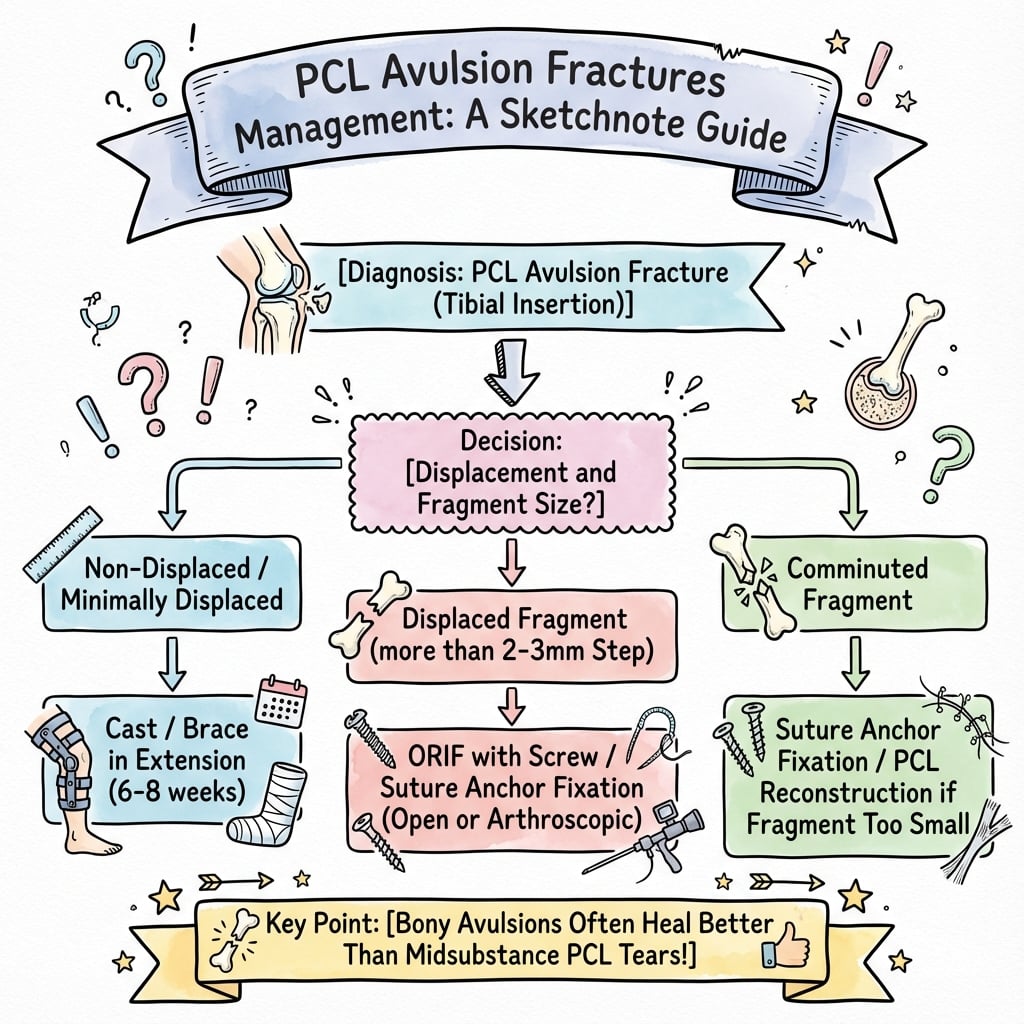
PCL Avulsion Fracture Management
Determine fragment size, displacement, and timing. Assess for associated injuries (PLC, ACL, meniscus). Plan surgical approach.
Optimal timing. Posterior approach, reduce fragment, fix with screw (large) or suture anchors (small). Excellent outcomes (85-95% good results).
May still be fixable. Attempt fixation if fragment mobile. May need reconstruction if fixed. Good outcomes (75-85%).
Fragment usually fixed. May require PCL reconstruction instead of fixation. Outcomes lower (60-80%).
Surgical Technique
Posterior Approach Technique
Patient Positioning:
- Prone on standard operating table
- Tourniquet on thigh (may deflate for exposure)
- Contralateral leg abducted
- Image intensifier positioned
Incision:
- Posterior midline or posteromedial approach
- 8-10cm incision
- Full-thickness flaps
Exposure:
- Identify neurovascular bundle first (popliteal artery, tibial nerve)
- Protect with vessel loops
- Retract medially or laterally
- Expose posterior tibia
- Identify PCL avulsion fragment
Critical: Popliteal artery at risk - must identify and protect before any dissection.
Popliteal artery lies directly posterior to the tibia, separated by only the popliteus muscle. During posterior approach, identify and protect the neurovascular bundle before any dissection. Use vessel loops to retract. Avoid excessive retraction. The artery is vulnerable to injury with posterior displacement.
Named Posterior Approaches & the Safe Interval
The guidelines table above names the "Burks / Trickey" open posterior approach, but the operative point examiners are really testing is how the popliteal neurovascular bundle is kept out of harm's way — that is a matter of which interval you choose, not just where the skin incision runs.
The Approaches by Name
- Trickey posterior (midline) approach: a lazy-S popliteal incision giving direct access to the posterior capsule. Because it crosses the popliteal fossa, it requires formal identification and mobilisation of the popliteal vessels and tibial nerve, so it is generally reserved for combined injuries needing wide exposure.
- Burks–Schaffer posteromedial approach: a more medial incision that uses the interval between the medial head of gastrocnemius and semimembranosus, avoiding the midline popliteal dissection.
- Lobenhoffer / posteromedial inverted-L approach: a widely used modern variant giving the same posteromedial window onto the PCL facet of the posterior tibia.
The Safe Interval (the high-yield principle)
The posteromedial approaches share one protective manoeuvre: develop the plane medial to the medial head of gastrocnemius, then retract that muscle belly laterally. The retracted medial gastrocnemius then sits as a muscular shield between the operative field and the popliteal artery, vein and tibial nerve, so the posterior tibial fragment can be reduced and fixed without dissecting directly onto the vessels. This is precisely why a posteromedial route is generally preferred over a direct midline popliteal dissection for the isolated tibial avulsion.
For the isolated posterior tibial PCL avulsion, the posteromedial approach (Burks–Schaffer / Lobenhoffer) is favoured: enter medial to the medial head of gastrocnemius and retract it laterally so the muscle shields the popliteal neurovascular bundle. A midline (Trickey) popliteal approach works but exposes the vessels directly and is usually reserved for combined injuries requiring wider access.
POSTERIORPosterior Approach Steps
Hook:POSTERIOR approach: Prone position, Open approach, Safely identify vessels, Tibial fragment exposure, Expose posterior tibia, Reduce fragment, Internal fixation, Outcomes excellent, Repair PCL!
Complications
- Incidence
- Less than 5%
- Risk Factors
- Inadequate exposure, excessive retraction
- Prevention/Management
- Identify vessels first, protect with vessel loops
- Incidence
- 5-10%
- Risk Factors
- Inadequate fixation, poor reduction
- Prevention/Management
- Secure fixation, good bone apposition
- Incidence
- 10-15%
- Risk Factors
- Malreduction, inadequate fixation
- Prevention/Management
- Anatomic reduction, secure fixation
- Incidence
- 5-10%
- Risk Factors
- Prolonged immobilization
- Prevention/Management
- Early ROM (2-4 weeks)
- Incidence
- 5-10%
- Risk Factors
- Prominent hardware
- Prevention/Management
- Countersink screws, use suture anchors if prominent
Neurovascular Injury
Less than 5% incidence:
- Cause: Inadequate exposure, excessive retraction, direct injury
- Prevention: Identify popliteal artery and tibial nerve first, protect with vessel loops, avoid excessive retraction
- Management: Immediate vascular surgery consultation if arterial injury
Nonunion
5-10% incidence:
- Cause: Inadequate fixation, poor reduction, fragment devascularization
- Prevention: Secure fixation, good bone apposition, proper timing
- Management: Revision fixation with bone graft if needed
Residual Laxity
10-15% incidence:
- Cause: Malreduction, inadequate fixation, fragment resorption
- Prevention: Anatomic reduction, secure fixation
- Management: Revision fixation if symptomatic, PCL reconstruction if needed
RISKSComplications
Hook:RISKS: Retraction injury to vessels, Inadequate fixation causes nonunion, Stiffness from immobilization, Killer curve not applicable (avulsion), Stiffness prevention with early ROM!
Postoperative Care
Immediate Postoperative
- Immobilization: Hinged knee brace locked in extension (4-6 weeks)
- Weight bearing: Non-weight bearing initially (4-6 weeks)
- ROM: Begin passive ROM at 2-4 weeks (unlock brace)
- PT: Quadriceps sets, straight leg raises (immediate)
Rehabilitation Protocol
Weeks 0-2:
- Brace locked in extension
- Non-weight bearing
- Quadriceps sets, straight leg raises
- Ice and elevation
Weeks 2-4:
- Unlock brace for passive ROM (0-90 degrees)
- Continue non-weight bearing
- Stationary bike (when ROM allows)
- Continue quadriceps strengthening
Weeks 4-6:
- Progressive weight bearing (partial to full)
- Full passive ROM
- Continue quadriceps strengthening
- Balance and proprioception
Weeks 6-12:
- Full weight bearing
- Progressive strengthening
- Sport-specific training
- Return to sport (when strength and ROM normal)
Return to Sport
Criteria:
- Full ROM (equal to contralateral)
- Quadriceps strength greater than 90% of contralateral
- No instability (negative posterior drawer)
- Functional testing passed
Timeline: Usually 6-9 months postoperatively.
Outcomes and Prognosis
Overall Outcomes
Surgical fixation outcomes:
- Success rate: 85-95% (excellent with proper technique and timing)
- Functional outcomes: 80-85% return to pre-injury level
- Complications: 10-15% (nonunion, residual laxity, stiffness)
Timing effects:
- Acute (under 3 weeks): 85-95% good results
- Subacute (3-6 weeks): 75-85% good results
- Chronic (over 6 weeks): 60-80% good results (may need reconstruction)
Functional Outcomes
Return to sport:
- Timeline: 6-9 months postoperatively
- Rate: 80-85% return to pre-injury level
- Factors: Age, sport level, rehabilitation compliance, timing of fixation
Functional testing:
- Quadriceps strength: 90%+ of contralateral
- No instability (negative posterior drawer)
- Full ROM
Long-Term Prognosis
Residual laxity:
- 10-15% have some residual posterior laxity
- Usually asymptomatic (does not affect function)
- May require revision if symptomatic
Arthritis risk:
- Low risk with proper treatment (less than 5% at 10 years)
- Higher risk with malreduction or persistent instability
- Proper reduction and fixation minimize risk
Factors Affecting Outcomes
Positive factors:
- Early fixation (within 3 weeks)
- Anatomic reduction
- Secure fixation
- Complete rehabilitation
Negative factors:
- Delayed fixation (over 6 weeks)
- Malreduction
- Inadequate fixation
- Incomplete rehabilitation
Prevention and Return to Sport
Prevention
Primary prevention:
- Proper seatbelt use (prevents dashboard injury)
- Airbag deployment
- Safe driving practices
- Protective equipment in sports
Secondary prevention (after injury):
- Complete rehabilitation before return to sport
- Continued strength and conditioning
- Gradual return to activity
Return to Sport Criteria
Clinical:
- Full ROM (equal to contralateral)
- Quadriceps strength greater than 90% of contralateral
- No effusion
- No instability (negative posterior drawer)
Functional:
- Single-leg hop test (greater than 90% of contralateral)
- Agility testing passed
- Sport-specific drills completed
Timeline: Usually 6-9 months postoperatively, depending on sport and level.
Guidelines, Registries & Global Practice
Global Epidemiology
- PCL injuries account for roughly 3-20% of acute knee ligament injuries; isolated bony tibial avulsions are a small subset.
- In pooled series, motor vehicle and motorcycle trauma cause the majority of tibial-sided avulsions (around 68% in the largest systematic review, with motorcycle crashes dominant in many Asian cohorts).
- High-energy mechanisms drive a male predominance and a 20-40 year peak. In limited-resource and high-motorcycle-density regions the absolute burden is higher.
Side-by-Side Guidance
- Position on Operative Fixation
- Surgical fixation for displaced bony avulsions; repair favoured over reconstruction when fragment adequate
- Approach Emphasis
- Arthroscopic or open, surgeon-dependent
- Position on Operative Fixation
- Reduce and fix displaced fragments; protect neurovascular structures
- Approach Emphasis
- Open posterior or arthroscopic in specialist centres
- Position on Operative Fixation
- Anatomic reduction and stable fixation (lag screw for large fragment) with early protected motion
- Approach Emphasis
- Open posterior (Burks/Trickey) approach detailed
- Position on Operative Fixation
- No single mandated technique; emphasis on stability and addressing concomitant injury
- Approach Emphasis
- Arthroscopic suture-button techniques increasingly favoured
There is no high-level guideline mandating a single technique. Consensus across societies is: displaced fragments should be reduced and stably fixed, repair is preferred over reconstruction when a fixable fragment exists, and concomitant ligament/meniscal injury must be addressed.
Registry & Resource Notes
- No dedicated arthroplasty-style registry tracks PCL avulsion fixation; evidence is limited to Level II RCTs and Level IV series/systematic reviews.
- High-resource settings: increasing use of arthroscopic suture-button/suture-bridge fixation to avoid open popliteal dissection, despite longer operative time and higher cost (Sundararajan RCT).
- Limited-resource settings: open posterior screw or staple fixation remains the workhorse - faster, cheaper, and not dependent on advanced arthroscopic instrumentation.
A high-yield global viva topic. Be ready to discuss: bony avulsion is repairable (favour fixation over reconstruction), the dashboard/high-energy mechanism, prone open posterior versus arthroscopic fixation (equivalent functional outcomes - Hooper, Sundararajan, Song), the popliteal artery at risk, and screw-for-large versus suture-for-small/comminuted fragment selection. Arthrofibrosis is the commonest complication.
Controversies & Areas of Uncertainty
The biggest live debate. A Level II RCT (Sundararajan 2020) and two systematic reviews (Hooper 2017, Song 2018) show equivalent functional outcomes. Arthroscopy avoids open popliteal dissection but is longer, costlier, and carried the only popliteal artery injury and both non-unions in the RCT. No clear winner - surgeon expertise and fragment morphology decide.
Lag screw (large solid fragment), suture/suture-bridge or suture-button (small/comminuted), and staple have all shown good results. Biomechanically, suture fixation is equivalent to a screw at time zero (Sasaki 2007). No construct is proven superior in clinical trials.
Early anatomic fixation is widely advocated, but the precise window is not defined by high-level evidence. Chronic/malunited fragments may need takedown, bone grafting or reconstruction; the threshold for abandoning fixation in favour of reconstruction is opinion-based.
Whether minimally/non-displaced bony avulsions can be managed non-operatively (brace in extension) versus prophylactic fixation is unresolved - reasonable conservative trials exist, but displacement and instability lower the threshold to operate.
MCQ Practice Points
Q: Why do PCL avulsion fractures have better prognosis than midsubstance PCL tears? A: Bony healing is faster and more reliable - PCL avulsion fractures achieve 85-95% good results with proper fixation vs 60-80% for midsubstance tears. Bony healing is more predictable than ligament reconstruction.
Q: What is the optimal timing for PCL avulsion fracture fixation? A: Within 3 weeks - Earlier fixation achieves 85-95% good results. Delayed fixation (over 6 weeks) has lower success rate (60-80%) and may require reconstruction instead of fixation.
Q: What is the surgical approach for PCL avulsion fracture fixation? A: Posterior approach with patient prone - Popliteal artery and tibial nerve at risk. Must identify and protect neurovascular bundle before any dissection. Use vessel loops to retract.
Q: What fixation method is used for large PCL avulsion fragments (over 1cm)? A: Screw fixation - Provides compression across fracture. For small fragments (under 1cm) or comminuted, use suture anchors. Both achieve excellent outcomes (85-95% good results).
Q: What structure is at risk during posterior approach for PCL avulsion fracture? A: Popliteal artery - Lies directly posterior to the tibia, separated by only the popliteus muscle. Must identify and protect before any dissection. Injury risk is less than 5% with proper technique.
Q: What are the outcomes of PCL avulsion fracture fixation? A: 85-95% good results with proper technique and timing (within 3 weeks). Better than midsubstance PCL tears (60-80%). Bony healing is faster and more reliable than ligament reconstruction.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 30-year-old man presents to ED after a motor vehicle accident. He was the driver and his knee struck the dashboard. He has a swollen, painful knee and cannot bear weight. Examination shows positive posterior drawer test and posterior sag sign. X-ray shows a PCL avulsion fracture with a 1.5cm fragment displaced posteriorly.”
“A 35-year-old athlete presents 2 weeks after a high-energy knee injury. He has persistent instability and cannot return to sport. Examination shows positive posterior drawer and posterior sag. CT scan shows a comminuted PCL avulsion fracture with multiple small fragments (largest 8mm).”
“An examiner shows you a lateral radiograph and a CT of a displaced single-fragment PCL tibial avulsion in a 28-year-old motorcyclist. MRI shows an associated lateral meniscal tear. The examiner asks: 'Would you fix this open or arthroscopically, and what does the evidence say?'”
Key Anatomy
- PCL insertion: Posterior tibia, 1-1.5cm below joint line
- Popliteal artery: Directly posterior to tibia, separated by popliteus muscle
- PCL function: Primary restraint to posterior tibial translation (95% at 90° flexion)
- Two bundles: Anterolateral (AL) and posteromedial (PM)
Classification
- By fragment size: Large (over 1cm) = screw, Small (under 1cm) = suture anchors
- By displacement: Minimal (under 2mm), Moderate (2-5mm), Severe (over 5mm)
- By timing: Acute (under 3 weeks), Subacute (3-6 weeks), Chronic (over 6 weeks)
- Comminuted: Multiple fragments - use suture anchors (2-3), not screw fixation
Treatment Algorithm
- Acute (under 3 weeks): Surgical fixation (screw or suture anchors) - 85-95% good results
- Subacute (3-6 weeks): Attempt fixation if mobile - 75-85% good results
- Chronic (over 6 weeks): May need reconstruction - 60-80% good results
- Timing is critical - earlier fixation has better outcomes
Surgical Pearls
- Posterior approach with patient prone
- Identify popliteal artery and tibial nerve first (critical for safety)
- Screw fixation for large fragments (compression), suture anchors for small
- Optimal timing within 3 weeks for best outcomes
Complications
- Neurovascular injury: Less than 5% (prevent by identifying vessels first)
- Nonunion: 5-10% (prevent with secure fixation, good apposition)
- Residual laxity: 10-15% (prevent with anatomic reduction)
- Stiffness: 5-10% (prevent with early ROM at 2-4 weeks)
Evidence Base
Open vs Arthroscopic Fixation - Systematic Review (637 patients)
- MVA caused 68.4% of injuries (motorcycle 59% of those) - confirms dashboard/high-energy mechanism
- Open and arthroscopic fixation give comparable validated outcome scores
- Arthrofibrosis is the most common complication for both approaches
ARIF vs ORIF - Randomised Controlled Trial
- Functional outcomes equivalent between open screw and arthroscopic suture fixation
- ORIF was faster, cheaper and had fewer complications in this trial
- The single popliteal artery injury occurred during the arthroscopic technique
Open vs Arthroscopic - Pooled Systematic Review (308 patients)
- Both approaches achieve good clinical outcomes and radiological union
- Residual side-to-side laxity 0-5 mm in both groups
- No clear superiority of one fixation strategy over the other
All-Arthroscopic High-Strength Suture Fixation
- Arthroscopic suture fixation suitable for small or comminuted fragments not amenable to a screw
- Large Lysholm/IKDC gains with restoration of posterior stability (KT-3000 1.1 mm)
- Avoids open popliteal dissection and a second hardware-removal procedure
Open Screw vs Arthroscopic Suture - Cadaveric Biomechanics
- Arthroscopic suture fixation is biomechanically equivalent to open screw fixation at time zero
- No difference in posterior displacement or construct stiffness
- Provides rationale for suture techniques that avoid popliteal fossa exposure
Open Staple Fixation - Stress Radiograph Outcomes
- Staple fixation is a simple, reliable alternative for the bony avulsion fragment
- Stress radiography confirmed restoration of posterior stability vs contralateral knee
- All fractures united without implant migration