Eccentric Load Injury | Bench Press Mechanism | Loss of Axillary Fold
- Pectoralis major has two heads: clavicular (proximal) and sternocostal (distal), forming a bilaminar tendon inserting on the lateral lip of the bicipital groove
- Mechanism is eccentric loading during bench press, especially during the eccentric (lowering) phase with the arm abducted and externally rotated
- Classic exam finding: loss of the anterior axillary fold with webbing, ecchymosis over the chest wall, and weakness of adduction and internal rotation
- Acute surgical repair within 6 weeks yields significantly better outcomes than delayed repair or conservative management for complete tears
- MRI is the gold standard for confirming diagnosis, delineating tear location, and assessing retraction
- “Loss of anterior axillary fold is pathognomonic for pectoralis major rupture
- “Tietjen Type III (complete tendon avulsion from humerus) is the most common pattern in surgical series
- “Arm in abduction and external rotation during eccentric loading is the classic mechanism
- “Surgical repair within 6 weeks gives best results; chronic tears have inferior outcomes
Pectoralis major is a bilaminar tendon. The clavicular head (anterior layer) and sternocostal head (posterior layer) twist 90 degrees before inserting on the lateral lip of the bicipital groove. The sternocostal fibres insert more proximally on the humerus. This twisting makes the inferior fibres most vulnerable during eccentric loading.
Male, 20 to 40 years, bench pressing. Sudden tearing sensation or pop during the eccentric phase. Pain over anterior chest and proximal arm. Swelling, ecchymosis spreading over chest wall and medial arm. Loss of the normal anterior axillary fold contour.
Resisted adduction and internal rotation reproduces pain and demonstrates weakness. With the arm forward-elevated, the patient attempts to adduct against resistance. Asymmetry of the anterior axillary fold is the hallmark finding. Palpate for a defect along the lateral chest wall or proximal humerus.
Refer for surgical consultation urgently for complete tears. Optimal repair window is within 6 weeks of injury. Beyond this, retraction and scarring make repair more difficult and outcomes deteriorate. Type III tears in active individuals should be repaired surgically.
- Diagnosis
- Loss of axillary fold, MRI confirms tear
- Treatment
- Urgent surgical repair within 6 weeks
- Key Pearl
- Complete tears in active patients need surgery
- Diagnosis
- Some axillary fold preserved, MRI partial
- Treatment
- Conservative or surgical based on demand
- Key Pearl
- High-demand athletes may benefit from repair
- Diagnosis
- Retracted tendon, absent axillary fold
- Treatment
- Delayed repair or reconstruction with graft
- Key Pearl
- Outcomes inferior to acute repair
BENCHPectoralis Major Rupture Mechanism
Hook:Think BENCH press for the classic mechanism of pectoralis major rupture!
Overview and Epidemiology
Pectoralis major rupture is an increasingly recognised injury, particularly among weightlifters and athletes. The incidence has risen significantly over recent decades with the growing popularity of resistance training. Despite this, the diagnosis is frequently missed or delayed in the emergency setting because the ecchymosis and swelling obscure the clinical picture. Early recognition and timely surgical repair of complete tears yield excellent functional outcomes, while delayed diagnosis leads to retraction, scarring, and inferior results.
- Demographics: Predominantly males aged 20 to 40 years
- Incidence: Increasing, parallel to rise in resistance training and anabolic steroid use
- Activity: Bench press accounts for approximately 90 percent of cases
- Side: More common on the dominant side
- Steroids: Anabolic steroid use is a recognised risk factor (tendon weakening)
- Functional loss: Weakness of shoulder adduction, flexion, and internal rotation
- Cosmetic deformity: Loss of anterior axillary fold is disfiguring
- Athletic performance: Significantly impairs pressing and throwing activities
- Psychological impact: Important in young active patients and bodybuilders
- Return to sport: Over 90 percent return after acute surgical repair
Pathophysiology
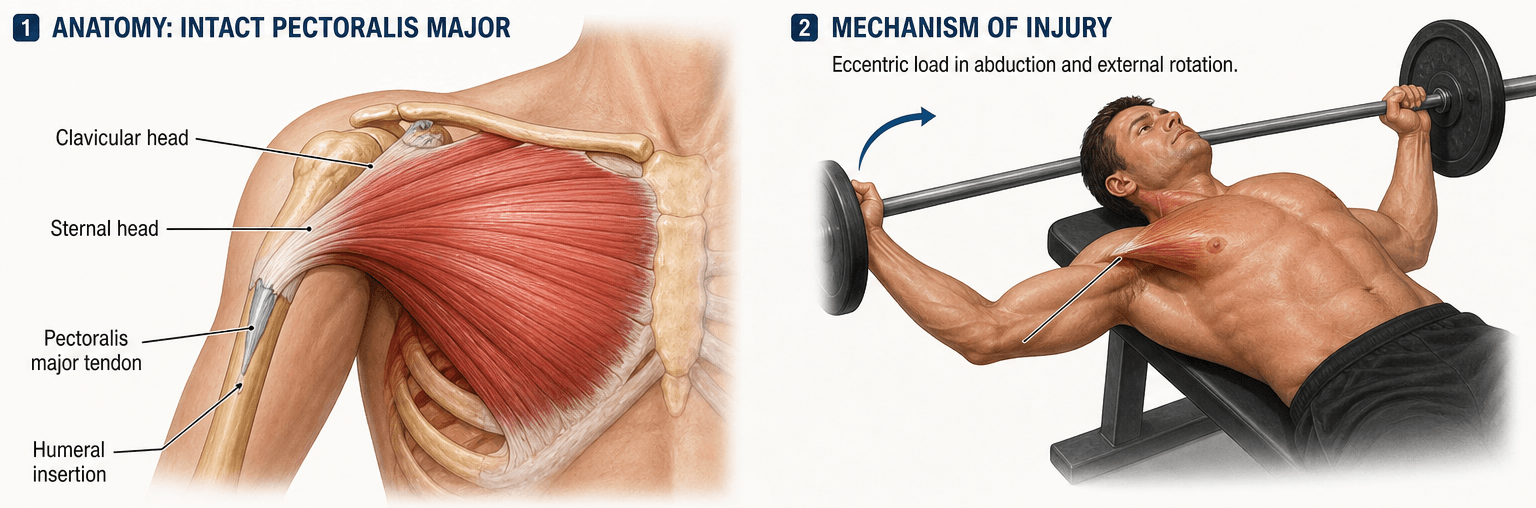
The pectoralis major is a large fan-shaped muscle originating from the medial clavicle, anterior sternum, and costal cartilages of ribs 1 through 6. The muscle converges into a bilaminar tendon that twists 90 degrees before inserting on the lateral lip of the bicipital groove of the humerus. The clavicular fibres form the anterior layer and insert more distally, while the sternocostal fibres form the posterior layer and insert more proximally. This arrangement means that during abduction and external rotation, the inferior (sternocostal) fibres are under the greatest tension, making them most vulnerable to rupture during eccentric loading.
- Origin
- Medial half of clavicle
- Insertion
- Lateral lip of bicipital groove (anterior layer, distal)
- Primary Action
- Shoulder flexion and adduction
- Origin
- Sternum and costal cartilages 1-6
- Insertion
- Lateral lip of bicipital groove (posterior layer, proximal)
- Primary Action
- Shoulder adduction and internal rotation
- Origin
- Convergence of both heads
- Insertion
- Lateral lip of bicipital groove
- Primary Action
- The twist concentrates stress on inferior fibres during eccentric loading
Loading position: Arm abducted 60 to 90 degrees and externally rotated
Phase: Eccentric (lowering) phase of bench press or similar pressing movement
Force: Maximal eccentric contraction against heavy load exceeds tendon tensile strength
Site of failure: Most commonly at the humeral insertion (tendinous avulsion)
Contributing factors: Anabolic steroid use (tendon dysplasia), inadequate warm-up, excessive load
Tendon rotation: The bilaminar tendon twists, concentrating stress
Vascular watershed: The insertion zone has a relatively poor blood supply
Mechanical disadvantage: In abduction and external rotation, the inferior fibres are maximally stretched
Steroid effect: Anabolic steroids cause tendon dysplasia (increase muscle strength faster than tendon adaptation)
Result: Complete avulsion from the humeral insertion (Tietjen Type III) is the most common pattern seen at surgery
- The strength-mismatch mechanism: AAS rapidly increase muscle mass and contractile force, but the tendon does not strengthen at the same rate - and AAS additionally cause collagen dysplasia (disorganised, stiffer, less elastic collagen fibrils with altered crimp). The result is a powerful muscle pulling on a relatively under-adapted, stiffer tendon, which fails under eccentric load - the classic AAS-user rupturing mid bench press.
- Implications for the contralateral side: because AAS act systemically, the other pectoralis (and other tendons) are also at risk - examine and counsel about the contralateral side, and be alert to a history of prior tendon ruptures.
- Implications at surgery and for outcome: AAS-associated tendon tissue is often of poorer quality, which can compromise suture purchase and is cited among the poor-prognosis factors; tissue quality should be assessed intra-operatively and fixation chosen accordingly.
- Counselling: discuss cessation of AAS, realistic expectations, and modification of maximal single-rep lifting - the underlying tendon vulnerability persists.
Exam point: AAS cause a muscle-tendon strength mismatch plus collagen dysplasia, explaining the bench-press rupture, mandating contralateral assessment and counselling on cessation, and contributing to poorer tissue quality at repair.
Classification and Types
Tietjen Classification (Modified by ElMaraghy)
- Description
- Muscle belly strain or contusion
- Clinical Features
- Pain, minimal swelling, preserved axillary fold
- Treatment
- Conservative: rest, ice, progressive rehabilitation
- Description
- Partial tear at musculotendinous junction (parsimonious)
- Clinical Features
- Weakness, some deformity, palpable defect possible
- Treatment
- Conservative for low demand; surgical for athletes
- Description
- Partial tear at musculotendinous junction (extensive)
- Clinical Features
- Significant weakness, visible deformity, ecchymosis
- Treatment
- Surgical repair recommended for active patients
- Description
- Complete tendon rupture from humeral insertion
- Clinical Features
- Complete loss of axillary fold, marked weakness, ecchymosis
- Treatment
- Surgical repair indicated; best within 6 weeks
Tietjen Type III is the most clinically significant and most commonly reported in surgical series. The ElMaraghy modification adds subtypes for partial tears based on extent.
PACTTietjen Classification
Hook:PACT = Partial, Attenuated, Complete, Timing is critical!
Clinical Assessment
- Mechanism: Eccentric loading during bench press or similar pressing movement
- Sensation: Audible or palpable pop, tearing sensation
- Pain: Sharp anterior chest or proximal arm pain, then dull ache
- Function: Immediate weakness of pressing, adduction, and internal rotation
- Timeline: Onset at time of lift, swelling and bruising develop over hours to days
- Inspect: Loss of anterior axillary fold, asymmetry compared to contralateral side
- Ecchymosis: Bruising over anterior chest wall, axilla, and medial proximal arm
- Palpate: Defect along lateral chest wall or proximal humerus; retracted muscle belly may be palpable medially
- Strength test: Weakness of resisted adduction and internal rotation with arm forward-elevated
- Webbing: The axillary fold appears flattened or concave, producing a web-like deformity
The most reliable clinical sign of pectoralis major rupture is asymmetric loss of the anterior axillary fold. With the patient standing and arms at the sides, observe the contour of the anterior axillary fold from the front. Then ask the patient to press the hands together (isometric adduction): on the affected side, the pectoralis major contracts but the axillary fold remains deficient because the tendon is discontinuous. The muscle belly may bunch up proximally. This finding, combined with a history of eccentric loading injury, is highly suggestive of complete rupture and should prompt urgent MRI and surgical referral.
"Loss of the anterior axillary fold" is taught as the hallmark of pectoralis major rupture, but relying on it alone misses an important subset:
- The fold has two contributors. The pectoralis major is bilaminar - so if the tear spares the clavicular head, an isolated sternocostal (sternal) head tear or a partial tear leaves the upper/clavicular part of the fold intact. The fold can therefore look deceptively preserved at rest, and the diagnosis is wrongly downgraded to a "strain."
- How to avoid the miss: examine dynamically and inferiorly - on resisted adduction/internal rotation, look for a thinned, low or asymmetric inferior fold and a step-off, and palpate specifically for the inferior (sternal-head) defect along the lateral chest wall/humeral insertion rather than just inspecting the gross contour. Compare side-to-side with the patient pressing the palms together.
- Have a low threshold for MRI even when the fold appears present, because the sternal head carries most of the muscle's adduction/internal-rotation power - a missed sternal-head tear still becomes a retracted chronic problem.
Exam point: an intact-looking axillary fold does not exclude rupture - an isolated sternal-head or partial tear is masked by the intact clavicular head; test resisted adduction, palpate the inferior defect, and image if in doubt.
- Key Feature
- Loss of axillary fold after bench press
- Discriminating Finding
- Ecchymosis, weakness of adduction and internal rotation
- Investigation
- MRI confirms tear location and extent
- Key Feature
- Anterior chest pain without axillary fold loss
- Discriminating Finding
- Pectoralis major intact on clinical exam
- Investigation
- MRI differentiates; rare compared to PM rupture
- Key Feature
- Popeye deformity, not axillary fold loss
- Discriminating Finding
- Ecchymosis anterior arm, not chest; biceps contour abnormal
- Investigation
- Clinical diagnosis confirmed with ultrasound or MRI
- Key Feature
- Global shoulder pain and instability
- Discriminating Finding
- Positive apprehension, not axillary fold deformity
- Investigation
- X-ray and MRI for labral injury
- Key Feature
- Pain without functional muscle deficit
- Discriminating Finding
- Intact axillary fold, normal adduction strength
- Investigation
- Chest X-ray if rib fracture suspected
Both present with anterior pain and ecchymosis after lifting. However, pectoralis major rupture causes loss of the anterior axillary fold with weakness of adduction and internal rotation, while proximal biceps rupture causes the classic Popeye deformity of the biceps belly with weakness of supination and elbow flexion. The axillary fold is preserved in biceps rupture.
Investigations
Imaging Protocol
Views: AP and axillary lateral of the shoulder
Look for: Bony avulsion fragment from the lateral bicipital groove, soft tissue swelling
Clinical correlation: Most pectoralis major ruptures are purely soft tissue and X-rays are normal. Radiographs primarily exclude other pathology.
Subtle sign: Focal loss of the normal pectoralis major soft tissue shadow on the AP view may suggest the diagnosis
Indication: All suspected pectoralis major ruptures
Protocol: T1 and T2 weighted sequences in axial, coronal, and sagittal planes. T2 fat-suppressed sequences best demonstrate the tear and fluid collection.
Findings: Discontinuity of the tendon at the humeral insertion, retraction of the muscle belly, surrounding haemorrhage and oedema, and assessment of the tear location (tendinous vs musculotendinous vs muscular)
Pre-op planning: Determines whether direct repair is feasible or graft reconstruction will be needed
Indication: Rapid bedside assessment when MRI is unavailable
Findings: Tendon discontinuity, haematoma, and retraction. Dynamic assessment possible.
Limitation: Operator-dependent, less accurate for tear extent and preoperative planning compared to MRI
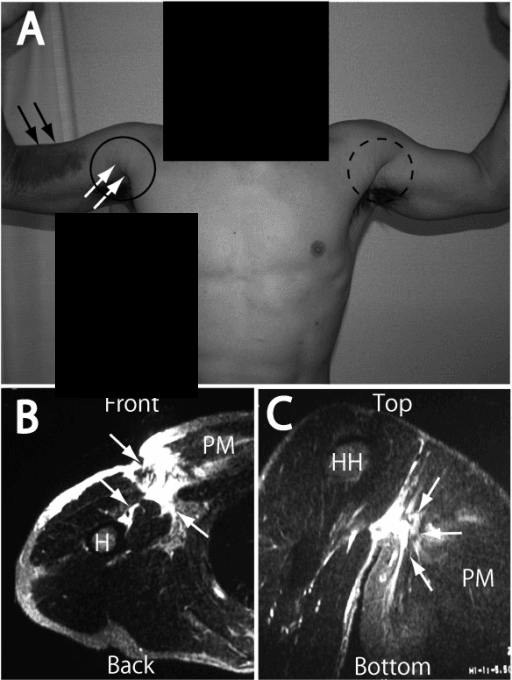
MRI is the gold standard for pectoralis major rupture because it accurately delineates the tear location, extent, and degree of retraction. Axial T2-weighted images are most useful for identifying the discontinuity at the humeral insertion. This information is essential for surgical planning: tendinous avulsions are repaired directly to bone, while musculotendinous junction tears may require different reconstruction techniques. Do not delay MRI in suspected complete tears as the surgical window is time-sensitive.
TEARClinical Diagnosis of PM Rupture
Hook:TEAR = the clinical hallmarks you need to spot pectoralis major rupture!
Management Algorithm
Acute Complete Rupture (Tietjen Type III, Under 6 Weeks)
Goal: Restore the anterior axillary fold and shoulder adduction/internal rotation power by anatomic repair of the tendon to its humeral insertion
Surgical Protocol
Timing: Ideally within 2 to 3 weeks; acceptable up to 6 weeks
Imaging: MRI to confirm tear location and retraction
Consent: Risks include infection, re-rupture, stiffness, and residual weakness
Approach: Deltopectoral incision, identify the retracted tendon edge
Preparation: Debride tendon edge to healthy tissue, mobilise the muscle from adhesions
Fixation: Transosseous sutures through bone tunnels in the lateral bicipital groove, or suture anchors (typically 3 anchors in a single-row configuration)
Arm position: Shoulder abducted 30 to 45 degrees and internally rotated to reduce tension on repair
Closure: Standard layered closure, sling immobilisation
Immobilisation: Sling for 4 to 6 weeks
Weeks 0-2: Pendular exercises, elbow, wrist, and hand ROM only
Weeks 2-4: Passive forward flexion to 90 degrees, passive external rotation to neutral
Weeks 4-6: Progress passive ROM to full, begin active-assisted exercises
Weeks 6-12: Active ROM, gentle strengthening with therabands
Weeks 12-16: Progressive resistance training, avoid heavy bench press
Weeks 16-24: Gradual return to weightlifting, start with light bench press
Return to sport: Typically 4 to 6 months post-operatively
The key technical point is anatomical repair to the lateral lip of the bicipital groove. The tendon must be secured with the arm in slight abduction and internal rotation to avoid over-tensioning. Transosseous bone tunnels and suture anchors both provide reliable fixation. Identifying the correct insertion site is essential because malposition affects the rotational mechanics of the bilaminar tendon.
Surgical Technique
Deltopectoral approach (standard)
- Beach chair or supine with bump under shoulder
- Arm free-draped to allow positioning
- Head of bed elevated 30-45 degrees
- Deltopectoral interval from clavicle to deltoid insertion
- Typically 8-12cm incision
- Can extend distally for better exposure of humeral insertion
- Identify deltopectoral interval (cephalic vein is landmark)
- Develop interval (vein usually taken laterally with deltoid)
- Retract deltoid laterally, pectoralis major medially
- Identify torn pectoralis major tendon (retracted medially)
- The tendon may be significantly retracted - require careful mobilization
- Cephalic vein: preserve or ligate if necessary
- Coracoid: landmark for orientation
- Long head biceps: medial to surgical field
- Axillary nerve: deep and inferior (safe with proper retraction)
The deltopectoral approach provides excellent visualization of the humeral insertion and allows tendon mobilization.
Complications
- Incidence
- Around 5 percent after repair
- Risk Factors
- Early return to heavy lifting, inadequate fixation
- Management
- Revision repair if tissue adequate; graft reconstruction if not
- Incidence
- Common after delayed repair
- Risk Factors
- Chronic tears, muscle atrophy, poor tissue quality
- Management
- Rehabilitation and activity modification
- Incidence
- Around 10 percent post-operative
- Risk Factors
- Prolonged immobilisation, poor rehabilitation compliance
- Management
- Physiotherapy, rarely manipulation under anaesthesia
- Incidence
- Around 1 to 2 percent
- Risk Factors
- Diabetes, smoking, prolonged tourniquet time
- Management
- Standard wound infection management; may require washout
- Incidence
- Near universal if untreated
- Risk Factors
- Complete tears managed conservatively
- Management
- Only addressed by surgical repair or reconstruction
The most important message for exam candidates is that early diagnosis and timely surgical repair prevent the complications of chronic rupture. A missed or delayed diagnosis that results in a chronic retracted tear converts a straightforward primary repair into a complex reconstruction with inferior outcomes. Always examine the axillary fold in any patient presenting with anterior chest or shoulder pain after weightlifting.
Postoperative Care and Rehabilitation
Post-surgical rehabilitation protocol:
Rehabilitation is critical to successful outcome. Protocol must balance early motion (to prevent stiffness) with protection of repair (to allow healing).
- Sling immobilization with arm in neutral rotation
- Remove sling for hygiene and gentle elbow/wrist ROM
- No active shoulder motion
- No passive stretching
- Ice and elevation for swelling control
- Focus on patient education regarding restrictions
- Begin passive ROM with therapist supervision
- Gentle pendulum exercises
- Avoid terminal external rotation and abduction (stresses repair)
- Continue sling between exercises
- No active shoulder motion yet
- Begin scapular retraction exercises (pain-free)
- Discontinue sling
- Begin active-assisted ROM in all planes
- Progress to active ROM as tolerated
- Continue to avoid combined abduction and external rotation
- Light isometrics in adduction and internal rotation
- Avoid resistance exercises
- Progressive resistance exercises
- Focus on internal rotation and adduction strengthening
- Rubber band exercises, light dumbbells
- Begin chest press with light weight (limited ROM initially)
- Gradually increase ROM and resistance
- Continue to avoid maximal external rotation
- Progressive resistance training
- Sport-specific exercises
- Can begin bench press with light-moderate weight
- Avoid maximal single-rep lifts
- Focus on proper form and controlled motion
- Most patients return to full activity by 6 months
- Gradual return to pre-injury activity levels
- May return to competitive sports after 6 months
- Return to heavy weightlifting after 6-9 months
- Permanent modification: avoid maximal single-rep bench press
- Emphasize proper warm-up and technique
- Full strength recovery may take up to 12 months
Key rehabilitation principles:
The first 6 weeks are critical for tendon-to-bone healing. Aggressive early motion can lead to repair failure. Passive ROM is safe. Active motion begins at 4-6 weeks. Resistance is delayed until 6 weeks minimum.
- 6 weeks: full passive ROM expected
- 12 weeks: full active ROM, beginning strength training
- 6 months: return to sport, near-normal strength
- 12 months: full strength recovery, unrestricted activity
- Light bench press at 3 months (50% body weight)
- Moderate bench press at 6 months (80% body weight)
- Heavy bench press after 9-12 months
- Avoid maximal single-rep attempts permanently
Outcomes and Prognosis
- Timing
- Within 6 weeks
- Expected Outcome
- Over 90 percent good to excellent results
- Return to Sport
- 4 to 6 months, high rate of return
- Timing
- 6 weeks to 3 months
- Expected Outcome
- 70 to 80 percent good results
- Return to Sport
- 6 to 9 months, some residual weakness
- Timing
- Over 3 months
- Expected Outcome
- 50 to 70 percent functional improvement
- Return to Sport
- Variable, may not return to pre-injury level
- Timing
- N/A (non-operative)
- Expected Outcome
- Pain resolves, persistent weakness and deformity
- Return to Sport
- Return to modified activity at 3 to 4 months
Best prognosis: Acute repair within 2 to 3 weeks, tendinous avulsion (Type III), anatomical repair to bone, compliant rehabilitation programme
Poor prognosis: Delayed repair beyond 6 weeks, musculotendinous junction tears, significant retraction and muscle atrophy, anabolic steroid-associated tendon dysplasia
Key threshold: 6 weeks from injury. Beyond this, tissue retraction and scarring significantly compromise repair quality and functional outcomes.
Guidelines, Registries & Global Practice
- Incidence rising worldwide in parallel with the popularity of resistance training and weightlifting
- Predominantly males aged 20 to 40, though female cases are increasingly reported
- Anabolic steroid use is a recognised risk factor, more prevalent in competitive bodybuilding communities globally
- Bench press is the most common mechanism across all regions and populations
- High-resource settings: Urgent MRI and surgical repair within 2 to 3 weeks is standard for complete tears; suture anchors widely available
- Limited-resource settings: Diagnosis may be clinical and ultrasound-based; transosseous bone tunnels are a low-cost alternative to anchors for repair
- Universal principle: Timing of repair is the most important modifiable factor regardless of setting
- Rehabilitation: Structured physiotherapy protocols are universally applicable regardless of fixation method
- Diagnosis Emphasis
- MRI gold standard; clinical exam sufficient to suspect diagnosis
- Acute Treatment
- Surgical repair for complete tears in active patients within 6 weeks
- Surgical Technique
- Suture anchors or bone tunnels to lateral bicipital groove
- Diagnosis Emphasis
- Clinical assessment of axillary fold + MRI to confirm
- Acute Treatment
- Surgical repair recommended for complete tears; conservative for partial tears in low-demand patients
- Surgical Technique
- Anatomical footprint restoration; anchors increasingly preferred
- Diagnosis Emphasis
- Imaging to define tear pattern for surgical planning
- Acute Treatment
- Early repair for complete tendon avulsions
- Surgical Technique
- Transosseous repair principles; anchors as equivalent alternative
There is no dedicated registry for pectoralis major ruptures. The evidence base consists of retrospective case series, a few prospective cohort studies, and one systematic review. No randomised controlled trial compares surgical to non-operative management, although the observational evidence strongly favours surgery for complete tears. The key exam message: the superiority of early surgical repair is supported by consistent observational evidence, and timing is the most important modifiable prognostic factor.
Controversies & Areas of Uncertainty
Both fixation methods have good published outcomes. No randomised trial has demonstrated superiority of one technique over the other. Suture anchors are more expensive but technically simpler. Bone tunnels are low-cost and equally effective. Choice is often dictated by surgeon preference and resource availability.
The optimal management of Tietjen Type II partial tears is debated. Low-demand patients may do well with conservative management, but high-demand athletes may benefit from surgical repair to maximise strength recovery. No high-quality evidence guides this decision, which must be individualised.
There are case reports of pectoralis major rupture following corticosteroid injection for shoulder pathology. The causal relationship is unproven, but caution is advised when injecting near the pectoralis major insertion in active weightlifters.
While most studies report high rates of return to sport after surgical repair, return to competitive-level bench press at pre-injury loads is less well documented. Athletes should be counselled that while the vast majority return to training, elite-level powerlifting performance may be affected.
Evidence Base and Key Trials
Rupture of the pectoralis major: a meta-analysis of 112 cases
- Meta-analysis of 112 cases demonstrating that surgical repair of pectoralis major ruptures yields superior outcomes compared to conservative management
- Patients treated with surgical repair achieved near-normal strength and returned to pre-injury activity levels
- Conservatively treated patients had persistent weakness of adduction and internal rotation
- Advocated early surgical repair for complete tears in active individuals
Ruptures of the pectoralis major muscle. An anatomic and clinical analysis.
- Anatomical study detailing the bilaminar structure of the pectoralis major tendon and its insertion on the lateral lip of the bicipital groove
- Clarified that the sternocostal fibres insert proximally and the clavicular fibres insert distally due to the 90-degree twist
- Described the mechanism of injury as eccentric loading with the arm in abduction and external rotation
- Provided the anatomical rationale for why the inferior (sternocostal) fibres are most vulnerable to rupture
Clinical considerations for the surgical treatment of pectoralis major muscle ruptures based on 60 cases: a prospective study and literature review
- Prospective study of 60 surgically treated pectoralis major ruptures demonstrating excellent functional outcomes after repair
- Surgical group demonstrated significant improvement in strength, cosmesis, and patient satisfaction
- The isokinetic strength deficit was markedly lower in the surgically treated group compared to historical conservative controls
- Recommended surgical repair for complete tears, especially in athletes and active individuals
A systematic review and comprehensive classification of pectoralis major tears
- Systematic review proposing a comprehensive classification system for pectoralis major tears based on tear location and extent
- Clarified the bilaminar tendon anatomy and its relevance to the pattern of injury and surgical repair
- Modified the Tietjen classification to include partial tear subtypes (ElMaraghy modification)
- Provided surgical guidance for anatomical footprint restoration during repair based on the classification
Treatment of Pectoralis Major Tendon Tears: A Systematic Review and Meta-analysis of Operative and Nonoperative Treatment
- Systematic review and meta-analysis pooling outcomes of surgical repair versus conservative management for pectoralis major ruptures
- Surgical repair resulted in significantly higher patient satisfaction and return-to-sport rates compared to non-operative treatment
- Acute repair (within 6 weeks) had significantly better outcomes than chronic or delayed repair
- No significant difference found between transosseous bone tunnel and suture anchor fixation techniques