Metaphyseal Infection | Hematogenous Spread
- Pathophysiology: Hematogenous seeding of the metaphysis (slow flow in venous sinusoids).
- Pathogen: S. aureus is #1. Kingella kingae in under 4yo. Salmonella in Sickle Cell.
- Diagnosis: MRI is most sensitive/specific early. X-rays normal for 10-14 days.
- Treatment: Antibiotics are mainstay. Surgery (Drilling/Decompression) if abscess or no response.
- Complications: Chronic OM, Growth arrest, Septic arthritis (transphyseal spread in neonates).
- “Infection starts in the METAPHYSIS (vascular loop slowing).
- “X-rays are negative early (need 30-50% bone loss to see lysis).
- “CRP is the best marker for monitoring response.
- “Treatment is 90% Medical (Antibiotics), 10% Surgical (Abscess).
X-ray Lags. X-rays are normal for the first 2 weeks. Do not rule out OM based on a normal X-ray. Get MRI.
Intra-articular Metaphysis. Metaphyses inside cartilage (proximal femur, distal humerus, proximal radius, distal fibula) can breach into the joint → Septic Arthritis.
Neonates. Vessels cross the physis in infants under 18 months. OM can spread to epiphysis and joint easily.
Weak Bone. Infection weakens bone. Protect weight-bearing during treatment.
At a Glance
| Feature | Acute OM | Chronic OM |
|---|---|---|
| Duration | less than 2 weeks | greater than 6 weeks |
| Bone Viability | Ischemia reversible | Sequestrum (Dead bone) |
| Pathology | Pus / Inflammation | Sequestrum / Involucrum |
| Treatment | Antibiotics (+/- Decompression) | Surgical Debridement essential |
| Biofilm | Immature | Mature / Established |
SLOWPathophysiology
Hook:Why metaphysis? Slow flow.
KINGSPathogens
Hook:Know the bugs.
S-I-B-CChronic OM Features
Hook:The terminology of chronic OM.
CAFEIV to Oral Switch Criteria
Hook:Ready for oral when you can go to the CAFE!
Overview and Epidemiology
Definition: Acute infection of bone, typically involving the metaphysis of long bones in children, usually arising by haematogenous spread.
Epidemiology:
- Incidence: Roughly 1 in 5,000 to 1 in 10,000 children per year in high-income settings; higher in some low-resource regions. More common than septic arthritis.
- Age: Roughly half of cases occur under 5 years. Boys affected more than girls (about 2:1).
- Sites: Lower limb predominates (distal femur, proximal/distal tibia) — fast-growing, well-vascularised metaphyses.
- Pathogens: S. aureus predominant in older children. Kingella kingae is the leading organism in children aged 6 to 48 months when PCR is used. Group B Streptococcus and E. coli in neonates; Salmonella in sickle cell disease.
Pathophysiology (Hematogenous):
- Bacteremia: Transient bacteremia (e.g., from teeth, skin, gut).
- Seeding: Bacteria lodge in the Metaphyseal Vascular Loops.
- Why? Blood flow slows down in hairpin loops, allowing bacteria to settle.
- Why Metaphysis? Reticuloendothelial system is deficient here.
- Proliferation: Bacteria proliferate → Inflammation → Pus.
- Pressure: Intra-osseous pressure rises → Ischemia of bone.
- Spread:
- Subperiosteal abscess: Pus breaks through cortex (children have loose periosteum).
- Joint: If metaphysis is intra-articular (Hip, Shoulder, Elbow, Ankle).
- Medullary canal.
Pathophysiology and Mechanisms
Metaphyseal Anatomy
The metaphysis of pediatric long bones is the primary site of infection due to its unique vascular architecture.
- Vascular Loops: Nutrient arteries terminate in hairpin capillary loops near the physis.
- Slow Flow: Blood flow slows significantly in these loops, allowing bacteria to settle.
- Physis: The growth plate (physis) usually acts as a barrier to the spread of infection into the epiphysis.
- Periosteum: In children, the periosteum is thick but loosely attached. Pus can easily lift it, forming a subperiosteal abscess.
Intra-articular Metaphyses
In four specific locations, the joint capsule inserts distal to the metaphysis (or proximal in femur/humerus terms), meaning the metaphysis is intracapsular.
- Proximal Femur (Hip Joint)
- Proximal Radius (Elbow Joint)
- Distal Humerus (Elbow Joint)
- Distal Fibula (Ankle Joint)
Infection here can rupture directly into the joint, causing Septic Arthritis.
Classification Systems
- Acute (less than 2 weeks): Inflammation. No sequestrum yet. Antibiotics +/- washout.
- Subacute (2-6 weeks): Brodie's Abscess. Indolent.
- Chronic (greater than 6 weeks): Sequestrum (dead bone) & Involucrum (new bone).
Classification guides duration of antibiotic therapy.
Clinical Assessment
History:
- Pain: Focal limb pain.
- Limp/Pseudoparalysis: Refusal to use limb.
- Fever: Often febrile (but not always).
- History: Recent trauma (minor) often reported (red herring or localizes bacteria).
Physical Examination:
- Tenderness: FOCAL bony tenderness (Metaphysis).
- Swelling: Soft tissue swelling / Erythema (late sign).
- ROM: Joint range often preserved (vs Septic Arthritis) unless pararticular or sympathetic effusion.
- Systemic: Signs of sepsis.
Differential Diagnosis
| Condition | Distinguishing Features | Key Investigation |
|---|---|---|
| Septic arthritis | Joint held flexed, marked pain on ANY passive movement, effusion | Joint aspiration (WCC over 50,000), MRI |
| Transient synovitis | Afebrile/low fever, normal-near-normal CRP, recent viral URTI, settles in days | Kocher criteria, normal inflammatory markers |
| Ewing sarcoma / leukaemia | Diaphyseal, lamellated periosteal reaction, night pain, cytopenias, weight loss | MRI, biopsy, blood film, LDH |
| Chronic non-bacterial osteomyelitis (CRMO) | Multifocal, recurrent, sterile cultures, clavicle/metaphyses, no true sepsis | Whole-body MRI, biopsy excluding infection |
| Pyomyositis / cellulitis | Soft-tissue focus, normal underlying bone marrow on MRI | MRI (soft-tissue vs marrow signal) |
| Trauma / occult fracture | Clear mechanism, normal inflammatory markers | Radiograph; MRI if uncertain |
Investigations
Labs:
- WBC: Elevated (neutrophilia).
- CRP/ESR: Elevated. CRP rises first and best for monitoring.
- Blood Cultures: POSITIVE in 40-50%. CRITICAL STEP.
Imaging:
-
X-ray:
- Early (less than 2 weeks): Normal or soft tissue swelling.
- Late: Periosteal reaction, Lytic lesions (need 30-50% bone loss).
-
MRI (Test of Choice):
- High sensitivity (greater than 90%) and specificity.
- Shows Marrow Edema (T2 bright, T1 dark).
- Shows Subperiosteal Abscess.
- Shows associated Septic Arthritis.
-
Ultrasound: Can show subperiosteal abscess (fluid under periosteum).
-
Bone Scan: If MRI unavailable or multifocal suspicion.
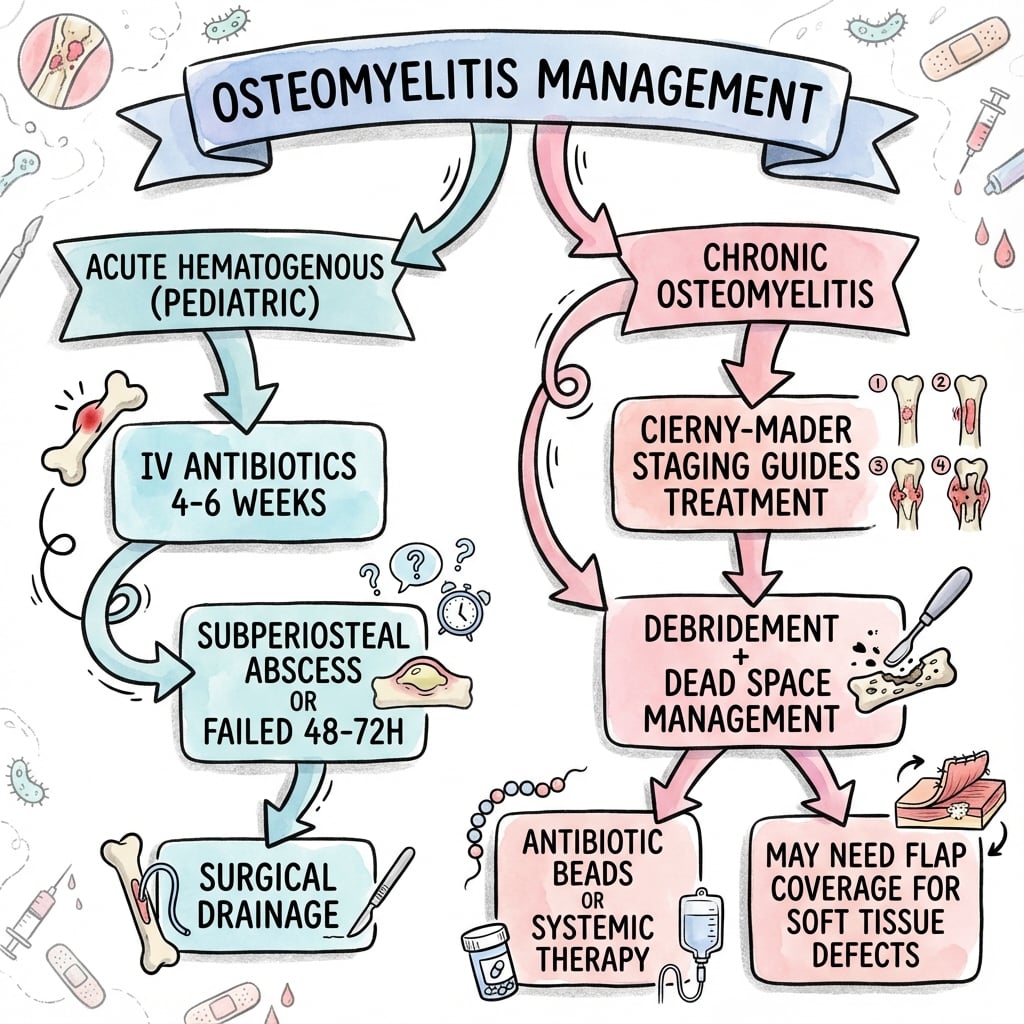
Management Algorithm
Surgical Technique
Cortical Window / Drilling
- Locate: Use fluoro to locate metaphyseal focus.
- Incision: Directly over maximal tenderness/abscess.
- Periosteum: Incise periosteum (often releases pus from subperiosteal abscess).
- Drill: 2.0mm or 3.2mm drill holes into metaphysis.
- Window: Create small cortical window if needed to evacuate intramedullary pus.
- Irrigate: Copious washout.
- Culture: Swab pus, bone biopsy.
- Closure: Loose closure over drain.
Decompress the "boil inside the bone".
Complications
| Complication | Mechanism | Management |
|---|---|---|
| Chronic Osteomyelitis | Inadequate Rx, Sequestrum | Debridement + Long Abx |
| Growth Arrest | Physis damage | Epiphysiodesis / Reconstruction |
| Septic Arthritis | Proximity / Transphyseal | Joint Washout |
| Pathologic Fracture | Bone cleaning/weakening | Cast / Fixation |
| DVT | Inflammation + Immobility | Anticoagulation |
Pelvic Osteomyelitis: Specifically tricky. Often presents as deep hip/abdominal pain. MRI essential. May need prolonged antibiotics.
Postoperative Care
- Antibiotics: Guided by culture sensitivities. Monitor CRP weekly.
- Immobilization: Splint/Cast for comfort and to prevent pathologic fracture.
- PICC Line: For long-term IV (if oral not suitable/available).
- Follow-up: X-rays to ensure healing, monitor growth.
Outcomes
- Uncomplicated: Excellent prognosis with antibiotics.
- MRSA: More aggressive, higher DVT risk, often needs surgery.
- Chronic OM: Difficult to eradicate. Recurrence common.
Evidence Base
Short-Course Antibiotics (Landmark RCT)
- 131 culture-positive children randomised to 20 vs 30 days of clindamycin or first-generation cephalosporin (first 2-4 days IV).
- S. aureus caused 89% of cases, all methicillin-susceptible; 24% had no surgery.
- Both groups recovered fully (only 1 mild sequela per arm) when CRP normalised within 7-10 days.
Simplified Treatment & CRP Monitoring
- Prospective RCT of 50 children with acute S. aureus osteomyelitis, early IV-to-oral switch (mostly within 4 days).
- CRP normalised within a median of 9 days; ESR took a median of 29 days.
- No failures or long-term sequelae; serum bactericidal titres added nothing.
Kingella kingae Epidemiology (PCR Era)
- 217 children with suspected osteoarticular infection; organism identified in 63.6% using culture plus PCR.
- K. kingae caused 87.7% of confirmed infections in children aged 6-48 months, exceeding S. aureus.
- S. aureus remained dominant (78.2%) in children over 4 years.
Oropharyngeal PCR for Kingella
- Prospective study of 123 children aged 6-48 months with atraumatic osteoarticular complaints.
- Oropharyngeal swab PCR for K. kingae had sensitivity 100% and specificity 90.5% for K. kingae osteoarticular infection.
- A non-invasive swab can predict K. kingae as the cause.
Mimic: Chronic Non-Bacterial Osteomyelitis (CRMO)
- CRMO (chronic recurrent multifocal osteomyelitis) is a sterile autoinflammatory mimic of bacterial OM in children.
- Whole-body MRI detects multifocal lesions at typical sites and clinically silent lesions.
- Imaging plus clinical features can avoid biopsy when infection and malignancy are excluded.
PIDS/IDSA Guideline (Diagnosis & Management)
- First multidisciplinary PIDS/IDSA GRADE-based guideline on acute haematogenous osteomyelitis in children (2021).
- Recommends MRI as the preferred imaging, blood cultures and image-guided/operative sampling, and prompt empirical antibiotics covering local S. aureus resistance.
- Supports early IV-to-oral transition and total courses of about 3-4 weeks in uncomplicated, responding cases.
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do you manage?”
“What is happening and what do you do?”
“List them and explain.”
MCQ Practice Points
Q: Where does hematogenous osteomyelitis start? A: In the Metaphysis. Specifically in the slow-flowing venous sinusoidal loops.
Q: How long before X-ray changes are visible in acute OM? A: 10-14 days. Need 30-50% bone mineral loss to see changes.
Q: What is an Involucrum? A: New bone formation (sheath) surrounding the dead bone (sequestrum) in chronic osteomyelitis.
Q: What unique pathogen causes OM in Sickle Cell patients? A: Salmonella (though S. aureus is still common/more common, Salmonella is the unique association).
Q: When is surgery indicated in acute OM? A: 1) Abscess formation (subperiosteal/intra-osseous), 2) Failure to respond to antibiotics (48-72h), 3) Sequestrum, 4) Associated septic arthritis.
Controversies and Areas of Uncertainty
Landmark RCTs support total courses near 3 weeks for uncomplicated, responding disease, yet many units still treat for 4-6 weeks. Optimal duration in MRSA, neonates and complicated cases is unresolved.
Early switch (within days) is safe with high-bioavailability oral agents and a falling CRP, but exact thresholds differ between guidelines and there is no universal CRP cut-off.
MRI is the most sensitive test but access, cost and the frequent need for sedation/anaesthesia in young children limit universal early use; some centres treat clinically with ultrasound and markers.
Most acute OM resolves on antibiotics alone. The threshold for drilling/decompression (especially for small intraosseous collections) and the value of "source control" without a drainable abscess remain debated.
Guidelines, Registries & Global Practice
Global epidemiology
- Incidence roughly 1 in 5,000 to 1 in 10,000 children/year in high-income settings; higher burden and later presentation (more chronic OM) in low-resource regions.
- Kingella kingae predominates in children 6-48 months in PCR-equipped centres; S. aureus predominates in older children worldwide. CA-MRSA proportion varies sharply by region and drives empirical choices.
| Body | Imaging | Antibiotic Approach |
|---|---|---|
| PIDS / IDSA (US, 2021) | MRI preferred; culture/PCR sampling stressed | Empirical cover by local resistance; early IV-to-oral; ~3-4 weeks total if responding |
| BSAC / UK practice (BOA-aligned) | MRI gold standard; ultrasound for subperiosteal collections | Short IV then oral; flucloxacillin first-line where MSSA dominant |
| European (ESPID-informed) | MRI; supports short-course strategy (Peltola data) | Total course as short as ~20 days in uncomplicated MSSA disease |
| Limited-resource settings | Radiograph +/- ultrasound; MRI often unavailable | Longer empirical IV courses; higher surgical/source-control role due to late presentation |
Practice variation (high- vs limited-resource)
- High-resource: MRI-led diagnosis, PCR microbiology, early IV-to-oral switch, outpatient/ambulatory IV (e.g. PICC) where oral not feasible, short total courses.
- Limited-resource: later presentation, more chronic OM and sequestra, greater reliance on radiographs/ultrasound and surgical debridement, longer parenteral therapy.
- Registries: no dedicated paediatric OM implant registry; surveillance comes from national paediatric infection networks and antimicrobial-resistance programmes that track local S. aureus/MRSA rates guiding empirical therapy.
Key Features
- Metaphyseal start
- Slow flow loops
- S. aureus #1
- Start Abx after CX
Imaging
- X-ray normal early (10-14 days for changes)
- MRI Gold Standard (95% sensitivity)
- Marrow edema = Early sign
- Subperiosteal abscess = Surgical drainage
- US useful for soft tissue/abscess
Chronic Terms
- Sequestrum (Dead)
- Involucrum (New)
- Cloaca (Drain)
- Brodie's (Abscess)
Intra-articular
- Prox Femur
- Dist Humerus
- Prox Radius
- Dist Fibula