Physiology first | Posterior ring decides stability | CT defines fixation
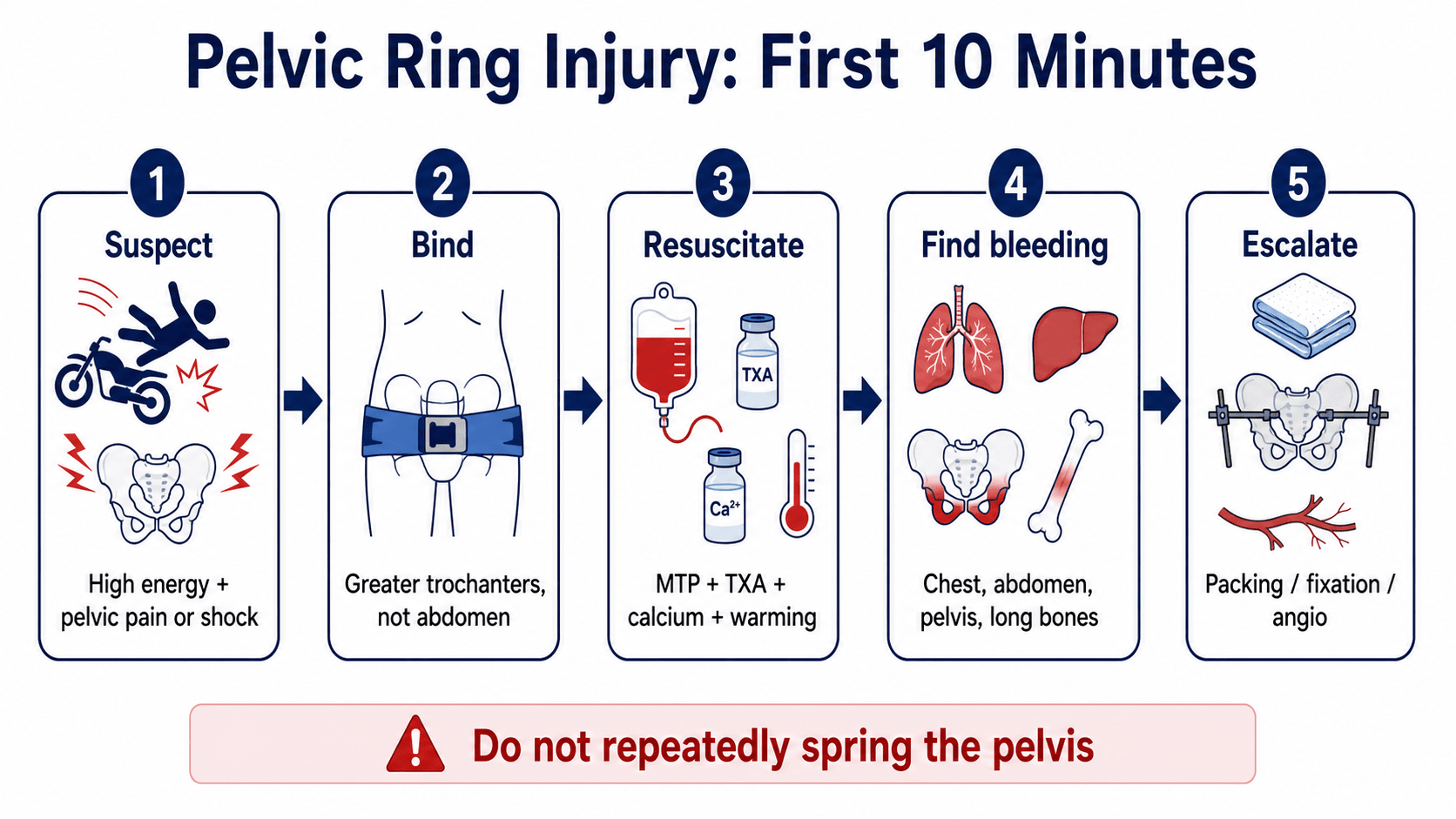
- Do not repeatedly spring the pelvis. One clinical suspicion is enough to bind and resuscitate.
- Binder position matters. It belongs over the greater trochanters, not the abdomen or iliac crests.
- The first decision is physiology. A non-responder needs haemorrhage control, not a perfect classification.
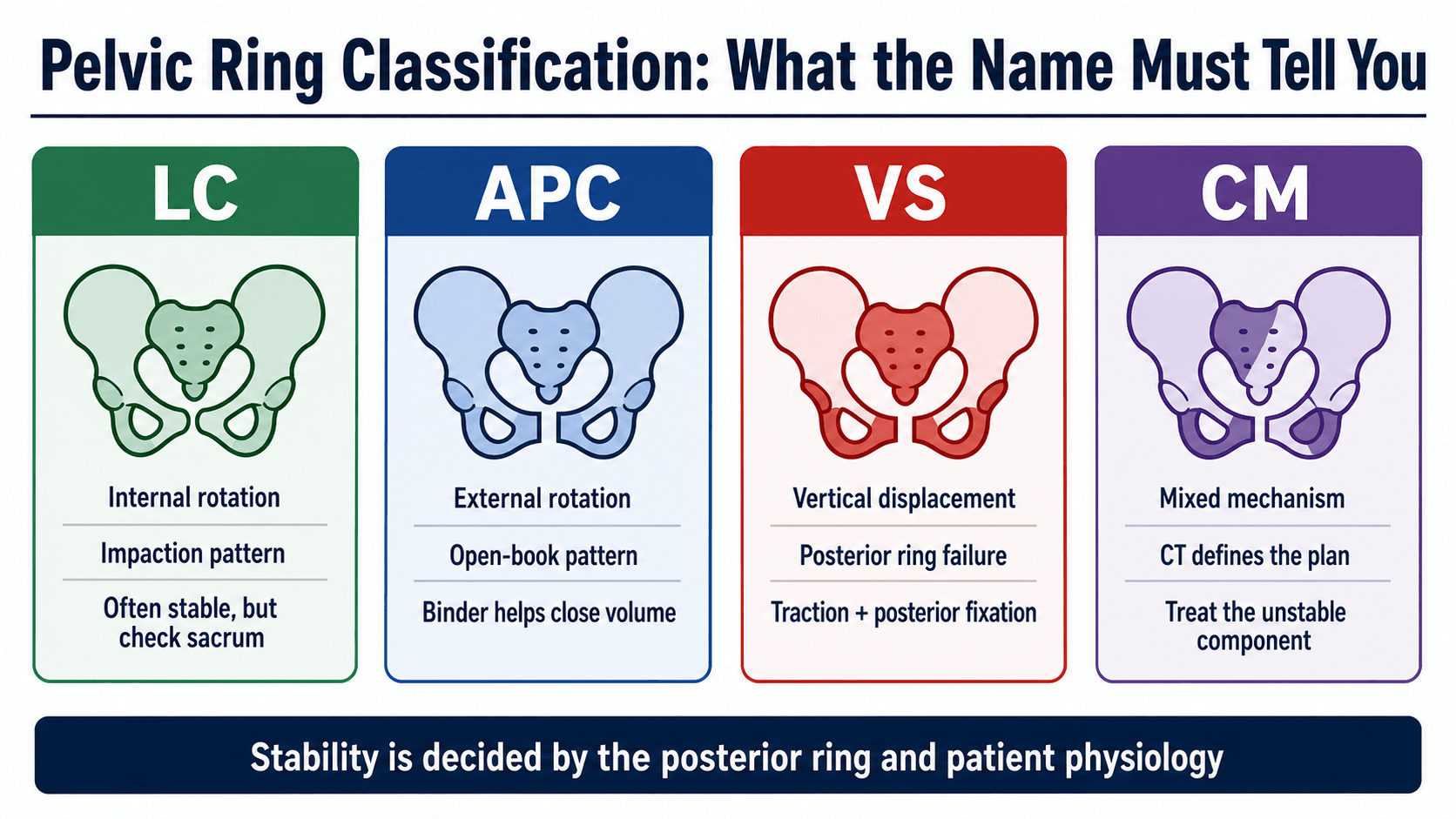
- The posterior ring decides stability. SI disruption, sacral displacement and vertical migration change fixation.
- Open pelvic fractures fail from bleeding early and sepsis later. They need multidisciplinary damage control.
- “A shocked patient with a pelvic fracture has pelvic bleeding until another major source is proven.
- “APC and vertical shear patterns are dangerous because they open pelvic volume and disrupt posterior stability.
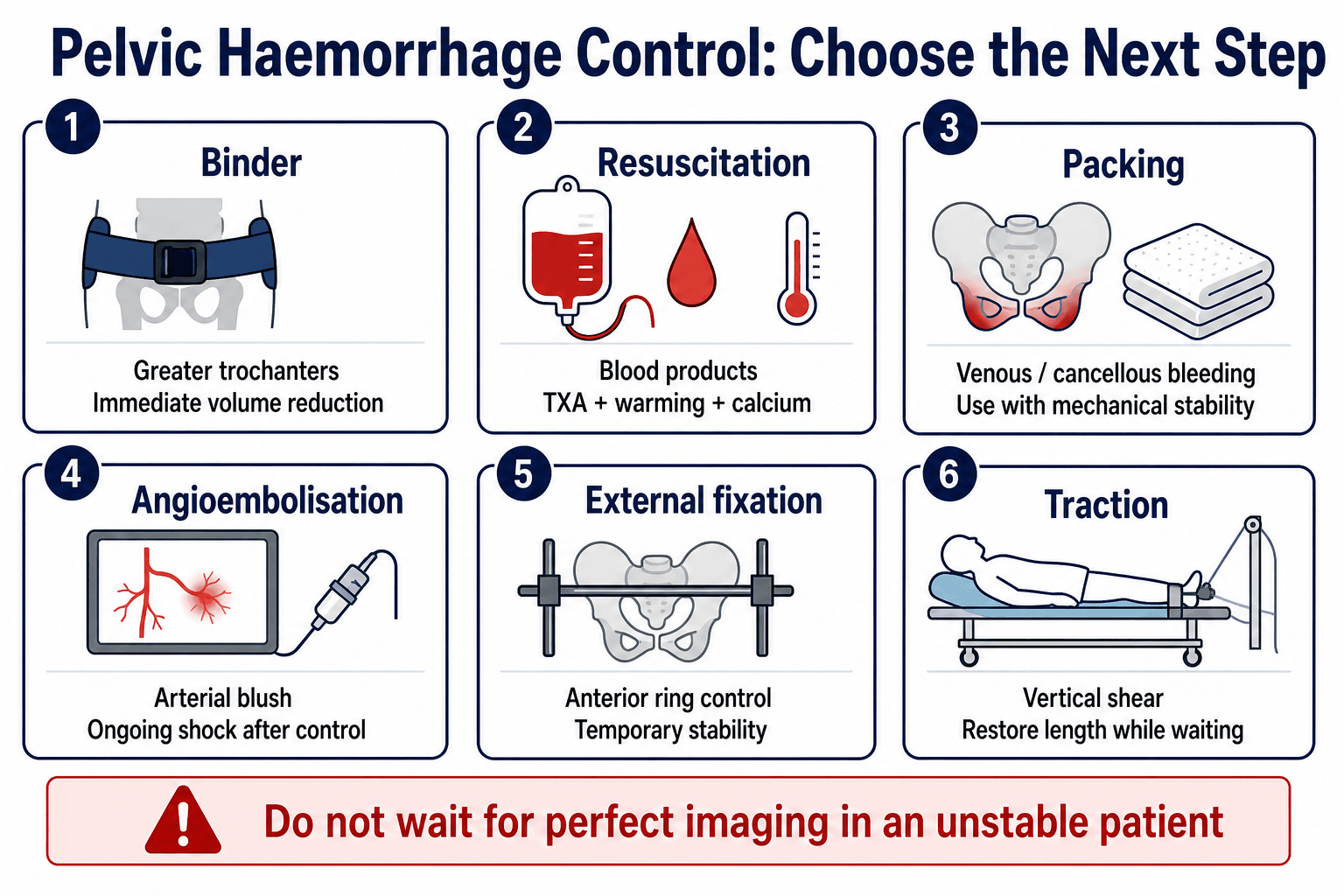
- “Angioembolisation treats arterial bleeding; it does not close pelvic volume or stabilise the posterior ring.
- “An LC-1 label is not enough. Sacral completeness, displacement, dynamic instability and ability to mobilise matter.
Do not repeatedly spring the pelvis. If the mechanism, pain pattern, deformity or physiology suggests pelvic ring injury, apply a binder over the greater trochanters and move to resuscitation.
- Finding
- Shock, falling base excess, transfusion need or non-response to resuscitation.
- Action
- Binder, blood products, senior trauma call, haemorrhage-control pathway.
- Finding
- SI widening, complete sacral fracture, posterior displacement or vertical migration.
- Action
- Posterior fixation becomes central.
- Finding
- Symphyseal opening, external rotation force, anterior SI widening.
- Action
- Binder acutely; anterior fixation with posterior assessment.
- Finding
- Rami fracture with ipsilateral sacral impaction or crescent fracture.
- Action
- Stable LC-1 mobilises; displaced or unstable LC needs fixation discussion.
- Finding
- Perineal, rectal, vaginal, scrotal, labial or major soft tissue wound.
- Action
- Antibiotics, debridement, urology or colorectal input and staged fixation.
BINDFirst Response | RINGClassification Logic | SIFTPosterior Ring Checklist |
|---|---|---|
B Binder Place over the greater trochanters. | R Rotation LC closes the ring; APC opens it. | S Sacrum Zone, fracture completeness, displacement and comminution. |
I Instability Shock means pelvic bleeding until proven otherwise. | I Instability Tile B rotates; Tile C rotates and translates. | I Ilium Crescent fragment, iliac wing fracture and posterior corridor. |
N No springing Avoid repeated pelvic stress tests. | N Neurology Sacral roots and lumbosacral trunk must be documented. | F Foramina Neural risk and screw trajectory. |
D Damage control Escalate to packing, fixation or angio when physiology demands. | G Genitourinary Meatal blood or haematuria changes catheter and imaging decisions. | T Translation Vertical or rotational displacement of the hemipelvis. |
BIND before defining the exact fracture. | Classify the ring only when it changes stability and treatment. | SIFT the CT before choosing posterior fixation. |
Overview
Pelvic ring injuries are not managed by naming the fracture first. They are managed by deciding whether the patient is bleeding, whether the posterior ring is unstable, and whether contamination or associated injuries change the sequence.
Definition
A pelvic ring injury disrupts the osteoligamentous ring formed by the sacrum, sacroiliac joints, innominate bones and symphysis pubis. Because the pelvis is a ring, a visible anterior fracture should prompt a deliberate search for a posterior fracture, SI ligament injury or occult instability.
Epidemiology
High-energy pelvic ring injuries are uncommon compared with other fractures, but they carry disproportionate risk because they occur in polytrauma and can be associated with major haemorrhage. A second important population is the older patient with osteoporotic fragility fracture, where the immediate problem is often pain, immobility and loss of independence rather than exsanguination.
Why it matters
The pelvis can bleed from cancellous bone, venous plexus and internal iliac arterial branches. Early deaths are usually haemorrhagic.
Stable injuries can mobilise. Rotational and vertical instability need mechanical control and often operative fixation.
Urethral, bladder, rectal, vaginal, neurological and Morel-Lavallee injuries change timing, fixation and complication risk.
Describe the patient first, then the fracture. A complete answer starts with haemodynamic status, binder position, associated injuries and CT-defined posterior ring stability.
Mechanism and Stability
- Mechanism
- Side impact causing internal rotation.
- Mechanical Failure
- Rami fracture plus sacral impaction or incomplete sacral fracture.
- Clinical Consequence
- Often stable, but complete sacral fractures and failure to mobilise need reassessment.
- Mechanism
- Greater lateral compression energy.
- Mechanical Failure
- Rami fracture plus ipsilateral posterior iliac crescent injury.
- Clinical Consequence
- Rotational instability may need posterior fixation.
- Mechanism
- Internal rotation on one side with contralateral external rotation.
- Mechanical Failure
- Windswept pelvis with mixed instability.
- Clinical Consequence
- Treat as unstable combined mechanism.
- Mechanism
- External rotation opening.
- Mechanical Failure
- Symphyseal opening less than 2.5 cm with intact posterior ring.
- Clinical Consequence
- Usually non-operative after posterior injury is excluded.
- Mechanism
- Further external rotation.
- Mechanical Failure
- Symphysis greater than 2.5 cm, pelvic floor disruption, anterior SI widening, posterior SI ligaments intact.
- Clinical Consequence
- Rotationally unstable; anterior fixation is usually required.
- Mechanism
- Complete external rotation disruption.
- Mechanical Failure
- Anterior and posterior SI disruption.
- Clinical Consequence
- Rotationally and vertically unstable; anterior and posterior fixation.
- Mechanism
- Axial load through limb or fall from height.
- Mechanical Failure
- Cranial migration through sacrum, SI joint or ilium.
- Clinical Consequence
- High instability; posterior fixation and length restoration are essential.



Anatomy That Changes Decisions
- Function
- Main posterior tension band and vertical stability.
- Why It Changes Management
- Complete disruption usually needs posterior fixation.
- Function
- Resist external rotation and vertical shear.
- Why It Changes Management
- Failure separates APC-1 from APC-2 and contributes to instability.
- Function
- Controls rotational opening.
- Why It Changes Management
- A symphyseal plate closes the front but cannot stabilise posterior vertical failure alone.
- Function
- Major venous and bone bleeding.
- Why It Changes Management
- Responds to binder, packing and mechanical stability.
- Function
- Arterial bleeding source.
- Why It Changes Management
- CTA blush or persistent shock may require angioembolisation.
- Function
- Motor, sensory and sphincter function.
- Why It Changes Management
- Neurology must be documented before and after reduction or screw fixation.
- Function
- Associated organ injury.
- Why It Changes Management
- Changes catheterisation, contamination control and operative sequencing.
Anterior ring displacement is often the obvious image finding. Posterior ring injury is usually the treatment-defining finding.
Classification

Young-Burgess is a mechanism classification. Its value is that it predicts direction of force, likely ligament failure, bleeding risk and initial fixation direction.
- Key Imaging
- Symphyseal diastasis less than 2.5 cm, no posterior injury.
- Stability
- Stable or minimally unstable.
- Usual Treatment Direction
- Binder if acute trauma; non-operative after posterior ring is excluded.
- Key Imaging
- Symphyseal diastasis greater than 2.5 cm, anterior SI opening, posterior SI ligaments intact.
- Stability
- Rotationally unstable, vertically stable.
- Usual Treatment Direction
- Anterior fixation with posterior assessment; external fixation may be temporary.
- Key Imaging
- Anterior and posterior SI disruption.
- Stability
- Rotationally and vertically unstable.
- Usual Treatment Direction
- Anterior and posterior fixation after resuscitation.
- Key Imaging
- Rami fracture plus ipsilateral sacral impaction or incomplete sacral fracture.
- Stability
- Often stable but variable.
- Usual Treatment Direction
- Mobilise if stable; reassess if complete sacral fracture, displacement or inability to mobilise.
- Key Imaging
- Rami fracture plus ipsilateral iliac wing crescent fracture.
- Stability
- Rotational instability possible.
- Usual Treatment Direction
- Posterior fixation if displaced, unstable or painful with mobilisation.
- Key Imaging
- Ipsilateral LC plus contralateral APC.
- Stability
- Combined instability.
- Usual Treatment Direction
- Treat unstable components; posterior control often required.
- Key Imaging
- Vertical migration through sacrum, SI joint or ilium.
- Stability
- Rotationally and vertically unstable.
- Usual Treatment Direction
- Traction, posterior fixation and anterior support as needed.

Clinical Assessment
Trauma bay priorities
- What to Look For
- Hypotension, tachycardia, transfusion need, lactate, base excess and response to binder.
- Why It Matters
- Decides CT versus urgent haemorrhage control.
- What to Look For
- Motorcycle crash, side impact, crush, fall from height, pedestrian impact or elderly low-energy fall.
- Why It Matters
- Predicts LC, APC, VS, open injury and associated trauma.
- What to Look For
- Perineal wound, scrotal or labial swelling, Morel-Lavallee lesion, degloving, rectal or vaginal blood.
- Why It Matters
- Open pelvis and soft tissue injury change antibiotics, debridement and fixation staging.
- What to Look For
- Blood at meatus, gross haematuria, inability to void, suprapubic pain.
- Why It Matters
- Retrograde urethrogram or CT cystogram may be needed before catheter strategy.
- What to Look For
- L5 weakness, foot drop, sacral sensory loss, saddle symptoms, anal tone when indicated.
- Why It Matters
- Documents lumbosacral plexus or sacral root injury and protects against missed iatrogenic change.
Examination sequence
Leg length asymmetry, rotational posture, pelvic bruising, flank bruising, open wounds, genital swelling and abdominal distension.
Do not repeatedly compress, distract or spring the pelvis. Clinical suspicion is enough to bind and image.
Binder position, distal pulses, lower-limb neurology, perineal signs, urology signs and skin condition before transfer or fixation.
Blood at the urethral meatus, perineal bruising or high suspicion of posterior urethral injury means do not blindly pass a urethral catheter. Use urethral imaging or urology input and consider suprapubic drainage.
Differential diagnosis of the painful or injured pelvis
- Distinguishing Features
- Ring disrupted at two or more points; symphysis, rami and posterior SI complex involved; instability with high-energy mechanism.
- Key Discriminator
- Posterior ring injury on CT confirms a true ring injury rather than an isolated fracture.
- Distinguishing Features
- Intra-articular hip pain, femoral head involvement, fracture lines through columns or walls on Judet views.
- Key Discriminator
- Articular surface and column involvement rather than ring discontinuity.
- Distinguishing Features
- Often low-energy in older patients; intact posterior ring; able to weight bear with pain.
- Key Discriminator
- CT shows no posterior ring injury; treat as a stable anterior-only injury.
- Distinguishing Features
- Low-energy or atraumatic in osteoporotic bone; insidious sacral or buttock pain; honda sign on bone scan or oedema on MRI.
- Key Discriminator
- Stress or insufficiency pattern in fragile bone without a clear high-energy event.
- Distinguishing Features
- Groin pain, shortened externally rotated limb, fracture at femoral neck or trochanter.
- Key Discriminator
- Injury is in the femur, not the ring; pelvis is intact.
- Distinguishing Features
- Fixed posture, locked hip, femoral head out of acetabulum on imaging.
- Key Discriminator
- Joint dislocation rather than osseous ring failure.
Imaging

- Best Question
- Is the pelvic ring obviously disrupted?
- Treatment-Changing Findings
- Symphyseal diastasis, rami fracture, SI widening, sacral asymmetry, iliac wing injury.
- Best Question
- Is there AP translation or rotational deformity?
- Treatment-Changing Findings
- Internal or external rotation, hemipelvis overlap, posterior displacement.
- Best Question
- Is there vertical displacement?
- Treatment-Changing Findings
- Sacral fracture, cranial migration, foraminal involvement.
- Best Question
- What is the posterior injury?
- Treatment-Changing Findings
- Complete sacral fracture, crescent fracture, SI disruption, comminution, dysmorphism and fixation corridor.
- Best Question
- Is there arterial bleeding?
- Treatment-Changing Findings
- Contrast blush, expanding haematoma or arterial cut-off.
- Best Question
- Is there bladder or urethral injury?
- Treatment-Changing Findings
- Extraperitoneal or intraperitoneal bladder leak, posterior urethral disruption.
- Why It Matters
- Posterior tension band injury.
- Decision
- Posterior fixation likely.
- Why It Matters
- Higher instability than sacral impaction alone.
- Decision
- Assess displacement, pain and dynamic stability.
- Why It Matters
- Reduced inherent stability and screw purchase.
- Decision
- Fixation strategy must match bone corridor and displacement.
- Why It Matters
- Posterior iliac injury with SI joint component.
- Decision
- Percutaneous or open posterior fixation depending morphology.
- Why It Matters
- Alters iliosacral screw safe zone.
- Decision
- Use careful inlet, outlet, lateral views or navigation.
- Why It Matters
- Soft tissue envelope at risk.
- Decision
- May delay or alter approach and implant choice.
The topic repeatedly says "sacral zone" and "complete sacral fracture" without giving the Denis classification, which is exactly what links the fracture line to neurological risk:
- Zone I (alar, lateral to the foramina) - the commonest zone; neurological injury is uncommon (roughly 6 percent), but an upward-driven ala can trap the L5 nerve root against the L5 transverse process.
- Zone II (transforaminal, through the neural foramina) - intermediate neurological risk (roughly 28 percent), typically L5, S1 or S2 radiculopathy; vertical shear through this zone is unstable.
- Zone III (central, involving the spinal canal) - the highest neurological risk (roughly 57 percent), characteristically bowel, bladder and sexual dysfunction (cauda equina) from canal compromise.
Practical use: the zone predicts both the deficit to examine for (document perianal sensation, anal tone and sphincter/voiding function, especially in Zone III) and the fixation corridor - foraminal comminution (Zone II) and canal involvement (Zone III) change iliosacral screw safety and may mandate decompression.
Exam point: classify every sacral fracture by Denis zone (I alar, II transforaminal, III central) and quote the rising neurological risk (about 6, 28 and 57 percent) - Zone III with cauda equina symptoms is the one that may need decompression, not just stabilisation.
A pubic rami fracture is rarely the whole injury in high-energy trauma. If pain, mechanism or displacement suggests more, the posterior ring needs CT assessment.
Management
The key decision is response to resuscitation
A non-responder remains shocked despite binder, blood products and correction of reversible trauma physiology.
Management direction
- Confirm binder over the greater trochanters.
- Continue balanced transfusion, warming, calcium replacement and coagulopathy correction.
- Exclude immediately treatable thoracic, abdominal and extremity bleeding.
- If pelvic venous or cancellous bleeding is likely, proceed to urgent preperitoneal packing with mechanical stability.
- If arterial bleeding is suspected, persistent or demonstrated by CTA, use angioembolisation when physiology and access permit.
- Do not let CT delay haemorrhage control in a crashing patient.
- Best Use
- Immediate pelvic volume reduction in suspected unstable injury.
- Limitations and Pitfalls
- Must be over greater trochanters; prolonged use can cause skin injury; may mask instability on imaging.
- Best Use
- Temporary anterior control in APC, VS or combined injuries.
- Limitations and Pitfalls
- Poor control of posterior vertical instability if used alone.
- Best Use
- Rapid tamponade of venous plexus and cancellous bleeding.
- Limitations and Pitfalls
- Needs mechanical stability; does not reliably treat major arterial bleeding.
- Best Use
- Arterial blush or persistent arterial bleeding.
- Limitations and Pitfalls
- Does not close pelvic volume; may be delayed by access and patient physiology.
- Best Use
- Selected posterior ring compression in expert hands.
- Limitations and Pitfalls
- Unsafe in comminuted sacral fractures or unfamiliar settings.
- Best Use
- Bridge for selected exsanguinating infra-diaphragmatic haemorrhage.
- Limitations and Pitfalls
- Requires expertise and is not definitive pelvic treatment.
The scanner is not a resuscitation strategy. A non-responder with suspected pelvic bleeding needs haemorrhage control, not prolonged diagnostic sequencing.
Definitive Treatment
- Usual Treatment
- Non-operative after posterior injury is excluded.
- Decision Details
- Analgesia, mobilisation and follow-up imaging if symptoms or displacement suggest more.
- Usual Treatment
- Anterior ring fixation.
- Decision Details
- Symphyseal plate is common; external fixation may be temporary or selected definitive care. Add posterior fixation if SI instability persists.
- Usual Treatment
- Anterior and posterior fixation.
- Decision Details
- Posterior SI disruption makes anterior-only fixation inadequate.
- Usual Treatment
- Non-operative.
- Decision Details
- Analgesia, early mobilisation, protected weight bearing as needed, repeat imaging if unable to mobilise.
- Usual Treatment
- Selective fixation.
- Decision Details
- Complete sacral fracture, displacement, stress instability or failure to mobilise supports fixation discussion.
- Usual Treatment
- Posterior fixation if displaced or unstable.
- Decision Details
- Percutaneous screw fixation or open reduction depending crescent fragment morphology.
- Usual Treatment
- Posterior fixation plus anterior support.
- Decision Details
- Restore length and posterior reduction; anterior fixation supports rotational control.
- Usual Treatment
- Damage control then staged reconstruction.
- Decision Details
- Avoid definitive implants through contaminated or devitalised tissue if staging is safer.
- Usual Treatment
- Selective minimally invasive stabilisation.
- Decision Details
- Balance posterior ring injury, pain, frailty, medical risk and baseline function.
Appropriate for stable patterns. It must still include analgesia, mobilisation plan, VTE prevention, repeat imaging when symptoms demand it, and treatment of osteoporosis in fragility injuries.
Indicated for unstable patterns, unacceptable displacement, failure of mobilisation in selected injuries, open fracture needs and associated injuries that require surgical control.
Surgical Technique
This section describes practical operative principles. Exact implants and sequence depend on patient physiology, fracture morphology, local trauma resources and surgeon experience.
Indication: suspected unstable pelvic ring injury during early resuscitation.
Technique
- Place the binder centred over the greater trochanters.
- Do not place it over the abdomen or iliac crests.
- Internally rotate and tape the legs only if it helps reduction and does not compromise other injuries.
- Reassess skin, abdomen access, distal perfusion and imaging interpretation.
- Transition to fixation or another haemorrhage-control strategy as soon as clinically appropriate.
Pitfalls: high binder position, prolonged pressure injury, masking instability on CT, and failure to escalate when shock persists.
A distinct pattern the iliosacral-screw discussion above does not cover: spinopelvic dissociation, where the spine is mechanically separated from the pelvis.
- Pattern: bilateral vertical (transforaminal) sacral fractures connected by a transverse fracture, producing a U-, H-, lambda- or T-shaped sacrum. The classic mechanism is an axial load (fall/jump from height), hence the association with calcaneal and thoracolumbar fractures.
- Why it is dangerous: the upper sacrum/spine flexes forward on the lower sacrum/pelvis, causing kyphotic sacral deformity and canal narrowing with a high rate of cauda equina / sacral root injury (often Denis Zone III). It is frequently missed because the AP pelvis looks deceptively intact - look for a "paradoxical inlet" appearance of the upper sacrum on the AP film and confirm with CT/sagittal reconstructions.
- Management: it is a posterior tension-band failure that iliosacral screws alone may not control. Highly displaced or kyphotic patterns, and those with progressive neurology, are stabilised with lumbopelvic ("triangular") fixation (pedicle screws into L5/sacrum connected to iliac screws), with sacral laminectomy/decompression if there is cauda equina compromise.
Exam point: a bilateral-vertical-plus-transverse (U-shaped) sacral fracture is spinopelvic dissociation - suspect it from a paradoxical inlet on the AP film and an axial-load mechanism, examine for cauda equina, and stabilise unstable/kyphotic patterns with lumbopelvic (triangular) fixation, decompressing when there is neural compromise.
Associated Injuries
- Clues
- Blood at meatus, perineal bruising, inability to void, high suspicion in APC injury.
- Action
- Retrograde urethrogram before urethral catheter; early urology input.
- Clues
- Gross haematuria, suprapubic pain, pelvic fracture with urinary symptoms.
- Action
- CT cystogram; intraperitoneal rupture usually needs repair.
- Clues
- Perineal wound, blood on examination, open fracture contamination.
- Action
- Antibiotics, debridement, colorectal or gynaecology input, diversion when indicated.
- Clues
- Foot drop, sensory change, sphincter symptoms, sacral fracture.
- Action
- Document early, correlate with CT/MRI and counsel prognosis.
- Clues
- Fluctuant degloving, abrasions, swelling over trochanter or pelvis.
- Action
- Recognise before fixation; drainage or debridement may be needed.
- Clues
- Intra-articular extension, hip instability, femoral head injury.
- Action
- Plan pelvic ring reduction and acetabular reconstruction sequence carefully.
Open Pelvic Fracture
An open pelvic fracture combines haemorrhage, contamination, soft tissue loss, urogenital injury and possible rectal or vaginal injury. Early death is usually bleeding; later death is often sepsis and organ failure.
Binder or external stability, blood products, antibiotics, tetanus prophylaxis, wound control and senior multidisciplinary coordination.
Examine the perineum, rectum and vagina. Faecal diversion is considered for rectal injury or major perineal contamination.
Temporary stability is often needed early. Definitive internal fixation should respect the contaminated zone and soft tissue viability.
Delayed haemorrhage control, missed rectal injury, inadequate debridement, pelvic sepsis and poorly planned implants through contaminated tissue.
Complications
- Complication
- Exsanguination, coagulopathy, hypothermia and acidosis.
- Prevention or Response
- Binder, blood products, warming, calcium, packing, fixation or angio pathway.
- Complication
- Missed urethral or bladder injury.
- Prevention or Response
- Look for meatal blood and haematuria; use urethrogram or cystogram appropriately.
- Complication
- Neurological injury.
- Prevention or Response
- Document before and after reduction and posterior fixation.
- Complication
- Pelvic infection or sepsis.
- Prevention or Response
- Debridement, contamination control, planned re-look and careful fixation staging.
- Complication
- Loss of reduction or implant failure.
- Prevention or Response
- Match fixation strength to posterior instability and weight-bearing plan.
- Complication
- Malunion, nonunion and chronic posterior pelvic pain.
- Prevention or Response
- Anatomical reduction of unstable patterns and follow-up imaging.
- Complication
- Sexual dysfunction, bladder dysfunction and neuropathic pain.
- Prevention or Response
- Screen actively and involve urology, pain and rehabilitation services when needed.
Postoperative Care
- Plan
- Base on posterior ring stability, fixation strength, bone quality and associated injuries.
- Reason
- One rule does not fit LC-1, APC-2, APC-3 and VS injuries.
- Plan
- Repeat lower-limb and perineal neurological examination after reduction or fixation.
- Reason
- New deficit may indicate screw, reduction or haematoma problem.
- Plan
- Inspect binder pressure areas, pin sites, Morel-Lavallee lesions and open fracture wounds.
- Reason
- Soft tissue failure drives infection and delayed reconstruction.
- Plan
- Use mechanical and pharmacological prophylaxis when bleeding risk allows.
- Reason
- Pelvic trauma has high thromboembolic risk.
- Plan
- Early sitting, transfers, chest care and progressive mobilisation with physiotherapy.
- Reason
- Outcome depends on whole-trauma rehabilitation, not only radiographic union.
- Plan
- Osteoporosis treatment, falls assessment and geriatric rehabilitation.
- Reason
- Prevents recurrent fractures and loss of independence.
Outcomes and Prognosis
Early haemorrhage control, accurate posterior reduction, stable fixation, recognised urology and neurology issues, and effective rehabilitation.
Open pelvic fracture, prolonged shock, pelvic sepsis, vertical instability, neurological injury, severe associated trauma and malunion.
Guidelines, Registries & Global Practice
Global epidemiology
Pelvic ring injuries account for a small share of all fractures but a disproportionate share of trauma deaths because they cluster in polytrauma. Haemodynamically unstable patterns carry the highest early mortality.
A bimodal pattern is seen worldwide: young patients after road traffic and fall-from-height trauma, and older patients with low-energy fragility fractures whose incidence is rising with ageing populations.
Genitourinary, neurological, rectal and major vascular injuries are common in high-energy patterns and drive long-term morbidity beyond the skeletal injury.
Side-by-side guidance
- Emphasis
- Physiology-driven algorithm integrating haemodynamics, ring anatomy and associated injuries.
- Practical Point
- Classifies by stability and bleeding risk; supports packing, angio and REBOA in defined roles.
- Emphasis
- Anatomical fracture classification and corridor-based fixation planning.
- Practical Point
- Tile/AO and OTA coding guide implant choice and posterior screw safety.
- Emphasis
- Time-critical pathway, early binder, CT in the stable patient and specialist referral.
- Practical Point
- Defines responsibilities, transfer standards and documentation in the major trauma network.
- Emphasis
- Evidence-based haemorrhage-control choices including angioembolisation and packing.
- Practical Point
- Supports early mechanical stabilisation and source-directed bleeding control.
- Emphasis
- Separate pathway for osteoporotic pelvic injury centred on mobility and bone health.
- Practical Point
- Mobilisation failure and posterior instability shift care toward minimally invasive fixation.
Registry and resource-setting notes
Trauma registries and major trauma audit (for example national trauma networks and the European and North American trauma databases) consistently link organised trauma systems and early haemorrhage control with lower pelvic-trauma mortality. Implant and fixation registries are less mature for pelvic fixation than for arthroplasty.
Access to CT angiography, interventional radiology, navigation for iliosacral screws, blood-bank major haemorrhage protocols and a multidisciplinary trauma team supports rapid source-directed control.
Where angiography and navigation are unavailable, the binder, external fixation, preperitoneal packing and fluoroscopy-guided fixation become the mainstays. Early transfer to a higher-level centre is often the decisive step.
Older patients need osteoporosis treatment, falls assessment, rehabilitation planning and review of baseline mobility as part of fracture care, regardless of country.
Controversies and Areas of Uncertainty
- One View
- Packing controls dominant venous and cancellous bleeding rapidly and needs no angio suite.
- Opposing View
- Angioembolisation targets arterial bleeding directly and avoids a laparotomy.
- Practical Position
- Driven by local resources, bleeding source and physiology; many trauma systems pack the crashing patient and reserve angio for arterial blush or ongoing bleeding.
- One View
- Demonstrable rotational instability favours stabilisation for faster pain-free mobilisation.
- Opposing View
- Minimally displaced LC-1 with complete sacral fracture can do well nonoperatively.
- Practical Position
- Decide on displacement, dynamic stability and ability to mobilise rather than on the fracture line alone.
- One View
- Reveals occult instability missed on static imaging and changes operative decisions.
- Opposing View
- Adds an anaesthetic and is operator-dependent and not universally available.
- Practical Position
- Useful in equivocal incomplete posterior injuries when the static scan does not settle stability.
- One View
- Bridges selected exsanguinating patients to definitive control.
- Opposing View
- Evidence on survival benefit is limited and it carries access and ischaemia risks.
- Practical Position
- Reserve for expert centres as a temporising adjunct, never as definitive pelvic treatment.
- One View
- Symphyseal plating gives rigid anterior control.
- Opposing View
- Anterior external fixation or INFIX avoids an open anterior approach in compromised soft tissue.
- Practical Position
- Match implant to soft tissue envelope, contamination and posterior stability needs.
Common Pitfalls
A binder around the abdomen does not close the pelvic ring. It must sit over the greater trochanters.
A symphyseal plate does not solve posterior SI disruption or vertical shear.
A non-responder needs haemorrhage control. CT is useful only when the patient can tolerate it.
LC-1 includes a spectrum. Complete sacral fracture, displacement or failure to mobilise changes the discussion.
Blood at the meatus is a urethral injury warning. Do not pass a urethral catheter blindly.
Morel-Lavallee lesions and open wounds can dictate timing, approach and infection risk.
MCQ Practice Points
Q: What is the first orthopaedic action in a shocked patient with an open-book pelvis? A: Apply a pelvic binder over the greater trochanters while major haemorrhage resuscitation is activated.
Q: What is the safe catheter plan when there is blood at the urethral meatus? A: Do not pass a urethral catheter blindly; perform urethral assessment and involve urology.
Q: Why is anterior fixation alone inadequate for APC-3 or vertical shear injury? A: The posterior ring is disrupted, so posterior fixation is needed for mechanical control.
- Best Answer Direction
- Binder, blood products and haemorrhage control.
- Trap
- CT first in a non-responder.
- Best Answer Direction
- Retrograde urethrogram or urology-guided drainage.
- Trap
- Blind catheterisation.
- Best Answer Direction
- Think APC-2 or worse and assess posterior SI joint.
- Trap
- Calling every open book APC-1.
- Best Answer Direction
- Posterior fixation and length restoration.
- Trap
- External fixator alone.
- Best Answer Direction
- Reassess posterior ring and instability.
- Trap
- Assuming all LC-1 injuries are benign.
- Best Answer Direction
- Antibiotics, debridement, contamination control and staged fixation.
- Trap
- Treating it as a closed pelvic fracture.
Applied Scenarios
Practise clinical reasoning and management decisions out loud
“A motorcyclist arrives hypotensive. AP pelvis shows symphyseal diastasis and SI widening.”
“An older patient has pubic rami fractures on X-ray and severe posterior pelvic pain. They cannot mobilise despite analgesia.”
“A patient with pelvic ring injury has blood at the urethral meatus during trauma survey.”
“CT shows cranial migration of the left hemipelvis through a sacral fracture with anterior rami fractures.”
First moves
- Suspect after high-energy mechanism, shock, pelvic pain or deformity.
- Binder over greater trochanters.
- Major haemorrhage protocol, warming, calcium and senior trauma escalation.
- Do not repeatedly spring the pelvis.
Classify
- LC: internal rotation; ask if posterior sacral injury is stable.
- APC: external rotation; symphyseal diastasis greater than 2.5 cm suggests APC-2 or worse.
- VS: vertical migration; posterior fixation is central.
- Tile B rotates; Tile C rotates and translates.
Treat bleeding
- Binder and stability reduce pelvic volume.
- Packing targets venous and cancellous bleeding.
- Angioembolisation targets arterial bleeding.
- A non-responder should not wait for perfect imaging.
Fixation logic
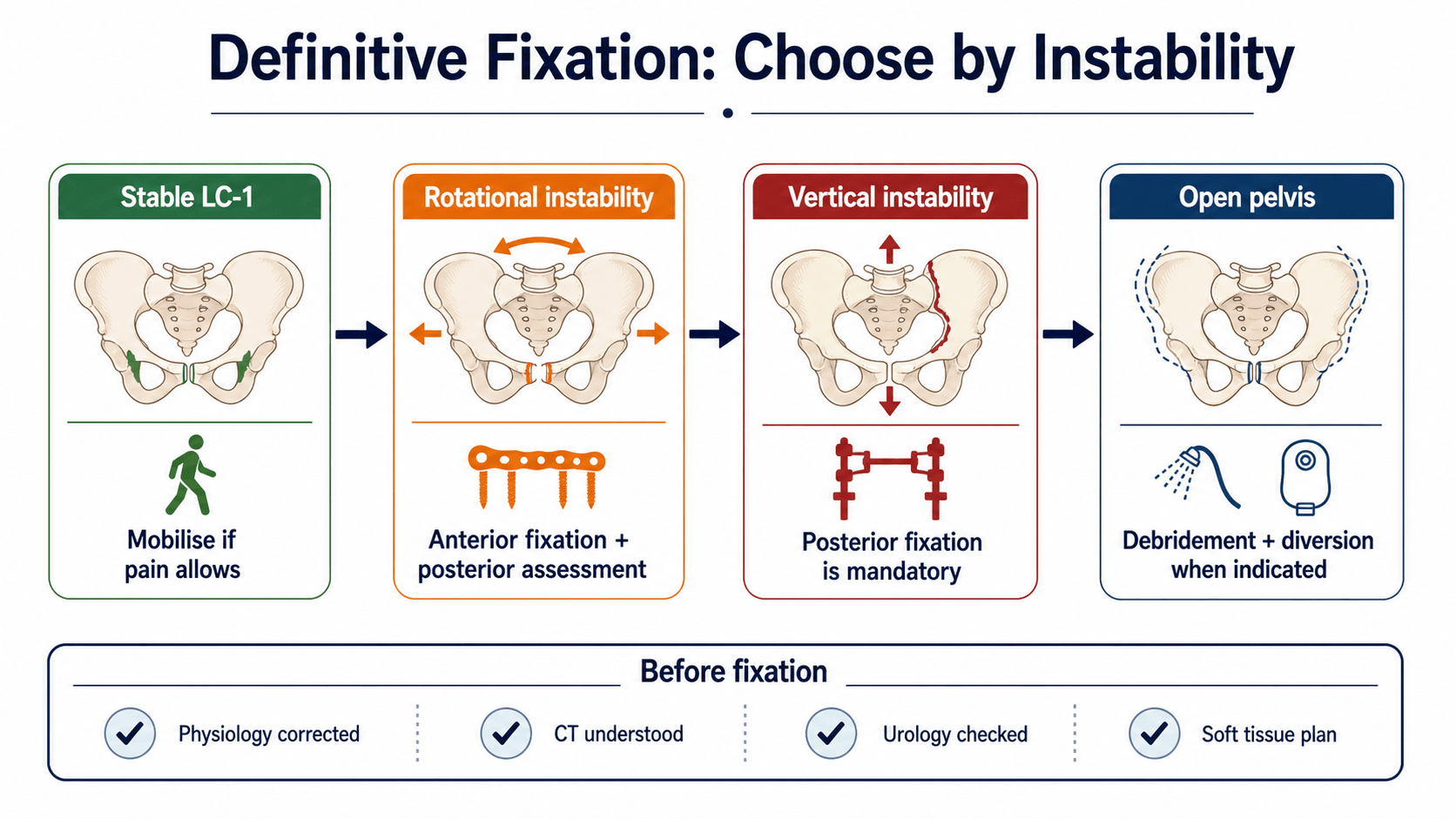
- Stable LC-1: mobilise and reassess if pain prevents function.
- APC-2: anterior fixation with posterior assessment.
- APC-3 and vertical shear: posterior fixation is essential.
- Open pelvis: staged multidisciplinary damage control.
Must not miss
- Urethral injury: blood at meatus.
- Bladder injury: gross haematuria.
- Open pelvis: perineal, rectal or vaginal wound.
- Neurology: L5, sacral roots and perineal sensation.
Evidence Signals
WSES Pelvic Trauma Classification and Guidelines
- Management must be multidisciplinary and based on the patient's physiology and the anatomy of the injury, not on a single classification.
- Haemodynamic status, mechanical ring instability and associated injuries are integrated into a unified treatment algorithm spanning binder, external fixation, preperitoneal packing, angioembolisation and REBOA.
Preperitoneal Pelvic Packing for Haemodynamically Unstable Fractures
- In 28 consecutive shocked patients (mean ED systolic blood pressure 77 mmHg, mean ISS 55) a preperitoneal packing plus external fixation protocol significantly reduced transfusion in the 24 hours after surgery (12 versus 6 units).
- No patient died of acute blood loss, and only 1 of the first 4 routinely angiographed patients required embolisation, supporting venous bleeding as the dominant source.
Examination Under Anaesthesia for Occult Instability
- Dynamic stress fluoroscopy under anaesthesia revealed occult instability in 50% of presumed APC-1 and 35% of presumed LC-1 injuries, reclassifying many to operative patterns.
- The authors proposed LC-1a and LC-1b subgroups to capture the dynamic instability missed on static imaging.