High-energy carpal instability | lateral X-ray diagnosis | urgent reduction | definitive fixation
- 25% missed initially - always look at lateral wrist X-ray
- Lateral X-ray key - capitate should be colinear with radius and lunate
- Lesser arc = pure ligamentous, Greater arc = with fractures (trans-scaphoid)
- Lunate maintains contact with radius in perilunate; loses contact in lunate dislocation
- Urgent reduction - median nerve at risk in carpal tunnel
- “On lateral: look for colinearity of radius-lunate-capitate
- “Spilled teacup sign = lunate dislocates volarly (Stage IV)
- “Trans-scaphoid perilunate = greater arc injury, better prognosis than pure ligamentous
- “Acute carpal tunnel syndrome common - median nerve compression
One quarter of perilunate dislocations are missed on initial presentation. The injury is subtle on PA view. Always check the lateral - look for colinearity of radius, lunate, and capitate.
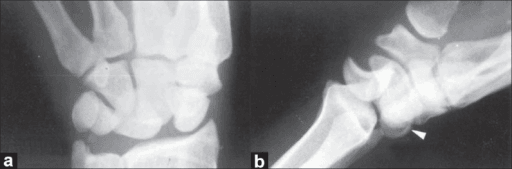
On lateral view: radius, lunate, and capitate should be colinear (like cups stacked). In perilunate dislocation, capitate is dorsal to lunate. In lunate dislocation, lunate tips volarly (spilled teacup).
Acute carpal tunnel syndrome occurs in up to 25%. The dislocated bones compress the median nerve in the carpal tunnel. Urgent reduction is required - delays risk permanent median nerve damage.
Lesser arc = pure ligamentous injury (through Mayfield stages). Greater arc = fracture through bone (trans-scaphoid perilunate most common). Greater arc injuries may have better prognosis.
- Key Finding
- Scapholunate widening, no dislocation
- Treatment
- May be isolated or progress
- Key Finding
- Capitate dorsal to lunate on lateral
- Treatment
- Urgent reduction, operative repair
- Key Finding
- Lunate volarly rotated (spilled teacup)
- Treatment
- Urgent reduction, operative repair
- Key Finding
- Greater arc with scaphoid fracture
- Treatment
- Fix scaphoid + ligament repair
- Key Finding
- Acute carpal tunnel syndrome
- Treatment
- Urgent reduction, consider CTR
- Key Finding
- Chronic dislocation
- Treatment
- Complex reconstruction required
MAYFIELDMAYFIELD - Stages of Injury
Hook:MAYFIELD stages progress from radial to ulnar, lesser to greater severity
SPILLEDSPILLED - Lunate Dislocation Sign
Hook:A SPILLED teacup = lunate dislocation (Stage IV)
Overview and Epidemiology
Perilunate dislocations are high-energy injuries representing the most severe end of the carpal instability spectrum. They are frequently missed on initial assessment, with up to 25% of cases not diagnosed at first presentation.
Mechanism of injury:
- High-energy wrist hyperextension
- Motor vehicle accidents
- Falls from height
- Industrial injuries
- Sports injuries - FOOSH with significant force
- Force transmitted through palm causes sequential ligament failure
Perilunate dislocations require significant force - these are not minor injuries. The energy required to cause sequential ligament rupture (or fracture through bone in greater arc injuries) indicates high-energy trauma. Always assess for associated injuries.
Classification:
- Lesser arc injuries: Pure ligamentous (through Mayfield stages)
- Greater arc injuries: With fractures (trans-scaphoid most common - 61%)
- Trans-scaphoid perilunate
- Trans-radial styloid perilunate
- Trans-triquetral perilunate
- Combined patterns
Anatomy and Pathomechanics
- Proximal row: Scaphoid, lunate, triquetrum (+ pisiform)
- Distal row: Trapezium, trapezoid, capitate, hamate
- Lunate: Central keystone, articulates with radius
- Capitate: Head articulates with lunate concavity
- Scapholunate (SL) ligament: Dorsal portion strongest, connects scaphoid to lunate
- Lunotriquetral (LT) ligament: Connects lunate to triquetrum
- Space of Poirier: Weak area between lunate and capitate (volar)
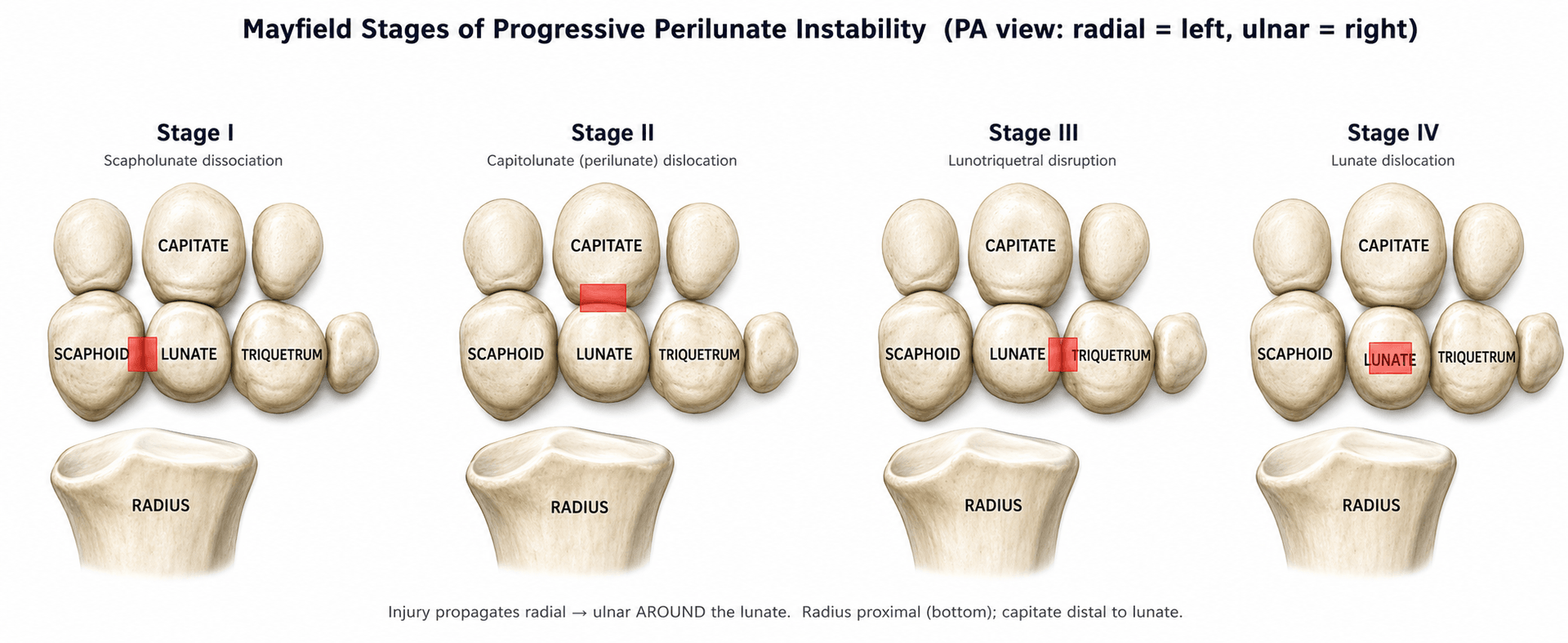
Progressive perilunar instability (Mayfield):
Mayfield Classification (Progressive Instability):
- Stage I: Scapholunate dissociation
- Stage II: Capitolunate dislocation
- Stage III: Lunotriquetral dissociation (Perilunate dislocation)
- Stage IV: Lunate dislocation (Lunate ejected volar into carpal tunnel)
- Lesser arc (pure ligamentous): Injury passes through the ligaments connecting carpal bones
- Greater arc (with fractures): Injury passes through the bones themselves
- Energy dissipated through bone fracture
- Trans-scaphoid perilunate is most common (61%)
- May have better prognosis - bone heals better than ligament
- Perilunate dislocation: Lunate maintains contact with radius; carpus displaces dorsally
- Lunate dislocation: Lunate loses contact with radius; rotates volarly into carpal tunnel
The topic refers to a "DISI pattern" without defining it, yet the lateral carpal angles are exactly what an examiner asks you to measure on the post-reduction or chronic-instability film:
- Normal angles (true lateral): scapholunate angle about 30-60 degrees (mean ~47), capitolunate angle under about 30 degrees, radiolunate angle under about 15 degrees.
- DISI (Dorsal Intercalated Segment Instability): with scapholunate dissociation the unrestrained lunate extends/dorsiflexes (and the scaphoid flexes). Hallmarks: scapholunate angle over 70 degrees, radiolunate angle over 15 degrees dorsal, increased capitolunate angle. This is the pattern that follows a perilunate/SL injury.
- VISI (Volar Intercalated Segment Instability): typically with lunotriquetral dissociation the lunate flexes/volarflexes - scapholunate angle low (under about 30 degrees) and a volar radiolunate tilt.
Why it matters: a DISI deformity on the post-reduction lateral signals inadequate reduction or unhealed SL ligament, and persistent DISI is the radiographic forerunner of chronic instability and SLAC collapse.
Exam point: state the normal SL angle (30-60 degrees) and recognise DISI (SL angle over 70 degrees, lunate dorsiflexed - the SL/perilunate sequel) versus VISI (lunate volarflexed - the LT pattern) on the true lateral.
Classification Systems
Mayfield Classification (Stages of Perilunar Instability)
- Description
- SL ligament rupture
- X-ray Finding
- SL widening (Terry Thomas)
- Description
- + Space of Poirier
- X-ray Finding
- Capitate starts to dorsally dislocate
- Description
- + LT ligament rupture
- X-ray Finding
- Complete perilunate dislocation
- Description
- + Dorsal radiocarpal
- X-ray Finding
- Lunate dislocates volarly
Injury propagates in an arc from radial to ulnar side. Stage I = SL injury alone. Stages progress as more ligaments fail. Stage III = complete perilunate. Stage IV = lunate pushed volarly into carpal tunnel.
Clinical Presentation and Assessment
Perilunate injury is usually not a subtle clinical injury; the subtlety is that the radiographs are often misread. Assessment must document mechanism, timing, median nerve function, skin condition and associated carpal fractures before and after reduction.
- Why It Matters
- Fall from height, motor vehicle crash, motorcycle injury and industrial trauma imply high-energy carpal disruption.
- Management Consequence
- Look beyond the wrist: associated limb, spine and polytrauma injuries may coexist.
- Why It Matters
- Acute injuries are usually reducible and reconstructable; delayed injuries develop contracture, chondral injury and carpal malalignment.
- Management Consequence
- Acute reduction and fixation differs from delayed reconstruction or salvage.
- Why It Matters
- The volar lunate or swollen carpal tunnel may compress the median nerve.
- Management Consequence
- Document before reduction; persistent symptoms after reduction push toward urgent carpal tunnel release.
- Why It Matters
- Manual workers need realistic counselling about grip loss, stiffness and delayed arthritis.
- Management Consequence
- Changes fixation/reconstruction expectations and return-to-work planning.
- Why It Matters
- Old SL injury, scaphoid nonunion or arthritis may change the interpretation.
- Management Consequence
- Pre-existing pathology may alter reconstruction versus salvage decisions.
- How To Examine
- Inspect for swelling, dorsal carpal prominence, volar fullness, skin puckering, open wound, bruising and finger posture.
- What It Means
- Massive swelling or skin compromise increases urgency. Volar fullness may reflect lunate displacement into the carpal tunnel.
- How To Examine
- Palpate distal radius, scaphoid, SL interval, lunate region, triquetrum, metacarpal bases and DRUJ. Avoid repeated painful stress before imaging.
- What It Means
- Localises fracture components and associated carpal/metacarpal injury.
- How To Examine
- Assess active finger flexion/extension first, then gentle wrist motion only if tolerated. Do not force a locked wrist.
- What It Means
- Finger stiffness and tendon irritation matter; a mechanical wrist block supports carpal dislocation.
- How To Examine
- Check thumb, index, middle and radial ring-finger sensation, two-point discrimination if possible, thenar power and pain with passive finger extension.
- What It Means
- Abnormal or worsening median nerve function is an emergency finding.
- How To Examine
- Capillary refill, radial/ulnar pulses, hand temperature, escalating pain and forearm compartment signs.
- What It Means
- Rare but important in high-energy trauma.
- How To Examine
- Repeat median nerve, vascular status, skin tension and radiographic alignment.
- What It Means
- Improvement supports decompression by reduction; persistent median symptoms need operative decompression.
Do not simply write "neurovascularly intact." For this injury, explicitly document median nerve symptoms, two-point discrimination where possible, thenar power and whether symptoms improve after reduction. Persistent or progressive symptoms should trigger urgent carpal tunnel release with definitive management.
LATERALLATERAL - X-ray Assessment
Hook:Use LATERAL view to diagnose - look for the three C's colinearity
Investigations
Request PA wrist, true lateral wrist and oblique wrist radiographs immediately. If the mechanism is high energy or the radiograph shows any carpal crowding, add CT of the wrist to define greater-arc fractures and plan fixation. Do not accept a poor lateral film when the diagnosis depends on sagittal carpal alignment.
- What To Check
- Trace Gilula arcs, look for SL widening, LT widening, carpal overlap, radial styloid/scaphoid/capitate/triquetral fractures and ulnar styloid injury.
- Abnormal Finding
- Broken arcs, crowded proximal carpal row or associated carpal fracture should trigger lateral review and CT.
- What To Check
- Assess whether radius, lunate and capitate are colinear. The lunate should articulate with both radius and capitate.
- Abnormal Finding
- In perilunate dislocation the capitate lies dorsal to the lunate while the lunate remains in the lunate fossa.
- What To Check
- Look for the lunate losing its normal radius relationship and rotating volarly.
- Abnormal Finding
- The classic spilled-teacup appearance represents Stage IV injury and may compress the median nerve.
- What To Check
- Look for scaphoid, triquetral, capitate, hamate or metacarpal base fracture components.
- Abnormal Finding
- Fractures convert the injury into a greater-arc pattern and change fixation.
- What To Check
- Repeat PA and lateral after closed reduction.
- Abnormal Finding
- Residual capitate-lunate malalignment means reduction is inadequate or unstable.
Gilula's lines are three smooth arcs on PA X-ray:
- Arc 1: Along proximal carpal row proximal surface
- Arc 2: Along proximal carpal row distal surface
- Arc 3: Along proximal capitate/hamate surfaces Disruption indicates carpal instability or dislocation.

- Indication
- High-energy injury, suspected greater-arc fracture, poor radiograph quality, preoperative planning or post-reduction confirmation.
- What It Changes
- Defines scaphoid, capitate, triquetral, radial styloid and articular fragments; guides fixation approach.
- Indication
- Subacute or chronic cases when ligament/cartilage viability, occult fracture or osteonecrosis is uncertain.
- What It Changes
- Rarely needed before urgent reduction; more useful when planning delayed reconstruction versus salvage.
- Indication
- Reduction assessment and intraoperative carpal alignment.
- What It Changes
- Confirms capitate-lunate reduction, SL/LT interval control and K-wire trajectory.
A PA wrist film can look deceptively acceptable. The lateral film is the safety check: if the capitate is not seated on the lunate, the wrist is not reduced.
- Distinguishing Features
- Capitate dorsal to lunate on lateral; lunate stays in radial fossa; broken Gilula arcs.
- Key Discriminator
- Lunate maintains radius contact; capitate displaced dorsally.
- Distinguishing Features
- Spilled-teacup lunate tipped volarly; loses radius contact; often acute carpal tunnel syndrome.
- Key Discriminator
- Lunate ejected volarly out of the radial fossa.
- Distinguishing Features
- Terry Thomas sign and SL angle greater than 70 degrees, but normal capitolunate colinearity on lateral.
- Key Discriminator
- No carpal dislocation - radius-lunate-capitate remain colinear.
- Distinguishing Features
- Anatomical snuffbox/scaphoid tubercle tenderness; intact Gilula arcs and carpal alignment.
- Key Discriminator
- No dislocation; carpal arcs preserved.
- Distinguishing Features
- Metaphyseal cortical break, dorsal/volar tilt; carpus moves with the distal fragment.
- Key Discriminator
- Fracture line is in the radius, not a carpal malalignment.
- Distinguishing Features
- Normal radiographs including a good lateral; tenderness without bony or carpal malalignment.
- Key Discriminator
- Diagnosis of exclusion only after an adequate lateral film.
Management

Emergency management:
- Neurovascular status (median nerve critical)
- Skin integrity
- Associated injuries
- Adequate X-rays (PA AND lateral)
- Indicated for all perilunate/lunate dislocations
- May be done in ED with sedation
- Traction + manipulation technique
- Confirm with post-reduction X-ray
- Splint wrist in neutral to slight flexion
- Re-assess median nerve function
- Arrange definitive surgical treatment
Reduction technique:
- Finger-trap traction for 10-15 minutes
- Extend wrist while applying pressure to carpus
- For lunate: direct pressure on dislocated lunate from palmar side
- Flex wrist to lock reduction
- Confirm with X-ray
- Splint in slight flexion Even with reduction, surgical treatment is almost always required.
Surgical Indications
- Essentially all perilunate/lunate dislocations
- Closed reduction alone has unacceptable outcomes
- Goals:
- Anatomic reduction
- Ligament repair
- Fracture fixation (greater arc)
- Stable fixation allowing early motion
Emergency surgery:
- Unreducible dislocation
- Median nerve symptoms persisting after reduction
- Open injury
All perilunate injuries require surgical stabilization for optimal outcomes.
Surgical Technique
- What To Do
- Supine, arm on hand table, tourniquet, image intensifier positioned for true PA and lateral wrist views.
- Key Point
- A poor lateral view intraoperatively risks accepting a malreduced capitate-lunate relationship.
- What To Do
- Mark Lister's tubercle, third/fourth compartments, carpal tunnel incision if volar approach planned, scaphoid and K-wire trajectories.
- Key Point
- Plan for both dorsal and volar access when median nerve symptoms, lunate dislocation or reduction difficulty exists.
- What To Do
- Longitudinal dorsal incision centred over the carpus. Protect dorsal sensory branches and veins. Open retinaculum as needed, mobilise EPL, perform dorsal capsulotomy.
- Key Point
- Preserve capsuloligamentous tissue that may be needed for repair.
- What To Do
- Extended carpal tunnel release when median symptoms, lunate dislocation or routine combined approach is chosen. Release transverse carpal ligament and protect median nerve.
- Key Point
- Reassess the nerve and remove compression; volar exposure also helps lunate reduction.
- What To Do
- Apply traction, derotate lunate/capitate, clear interposed capsule or tendon, restore radius-lunate-capitate colinearity.
- Key Point
- Reduction is judged on both direct view and fluoroscopy, not by feel alone.
- What To Do
- In greater-arc injuries, fix scaphoid, radial styloid, capitate or triquetral fractures with appropriate screws, wires or plates.
- Key Point
- The scaphoid usually needs stable compression fixation in trans-scaphoid perilunate injuries.
- What To Do
- Temporarily pin SL, LT and/or scaphocapitate intervals according to instability pattern.
- Key Point
- Pins protect ligament healing and prevent recurrent carpal dissociation.
- What To Do
- Repair dorsal SL and LT ligaments when tissue allows; repair capsule and dorsal intercarpal/radiocarpal structures as needed.
- Key Point
- Do not repair an unreduced carpus.
- What To Do
- Confirm PA/lateral alignment, wire position, fracture fixation and median nerve status. Close capsule/retinaculum without tendon tethering.
- Key Point
- Document post-reduction median nerve function and final alignment.
Complications
- Incidence
- Up to 50%
- Management
- Activity modification, salvage procedures
- Incidence
- 30-50%
- Management
- Reconstruction, fusion options
- Incidence
- 10-15%
- Management
- Prevention with urgent treatment
- Incidence
- 5-10%
- Management
- Revision fixation, bone graft
- Incidence
- Common
- Management
- Physiotherapy, capsular release
- Incidence
- Rare with timely treatment
- Management
- Salvage procedures
- Incidence
- 5-10%
- Management
- Early recognition, MDT treatment
- Most significant long-term complication
- Radiocarpal and midcarpal joints affected
- May progress despite initial good result
- Treatment: activity modification, fusion procedures
- SL ligament heals poorly
- May have chronic SL dissociation despite repair
- Leads to DISI pattern, SLAC wrist
- May need late reconstruction or fusion
Despite optimal treatment, post-traumatic arthritis develops in up to 50% of patients over time. Carpal instability is also common. Patients should be counseled that even with good initial treatment, long-term problems may develop.
Median nerve injury:
- Acute compression usually resolves with reduction
- Delayed treatment = higher risk of permanent deficit
- May need neurolysis or secondary procedures
The topic repeatedly invokes "SLAC wrist" and says PRC is contraindicated when the capitate head is degenerate, but never gives the staging that drives the salvage choice. The chronic SL dissociation/DISI after a perilunate injury produces a predictable arthritic cascade:
- SLAC (ScaphoLunate Advanced Collapse) stages: I = arthritis at the radial styloid-distal scaphoid; II = whole radioscaphoid joint; III = capitolunate / midcarpal joint. The radiolunate (lunate fossa) joint is characteristically spared even in advanced disease.
- SNAC (Scaphoid Nonunion Advanced Collapse) is the analogous cascade after scaphoid nonunion (relevant to the trans-scaphoid greater-arc injury), staged the same way around the nonunion.
- Why staging dictates salvage: because the radiolunate joint and the proximal capitate/lunate cartilage are the load-bearing surfaces relied on by motion-preserving salvage - PRC needs a healthy capitate head and lunate fossa (so it fails / is contraindicated once the capitolunate joint is arthritic, i.e. SLAC/SNAC III), whereas a four-corner fusion (excise scaphoid, fuse capitate-lunate-hamate-triquetrum) is preferred when the capitolunate joint is involved but the radiolunate is spared. Total wrist fusion is the end-stage/high-demand option.
Exam point: the late perilunate/SL sequel is a SLAC (or SNAC) wrist staged I-III - the radiolunate joint is spared, so PRC suits stage I-II (healthy capitate head) and four-corner fusion suits stage III (capitolunate arthritis), with total wrist fusion for pan-carpal disease.
Postoperative Care and Rehabilitation
Postoperative protocol:
- Volar splint, wrist neutral to slight flexion
- Elevation
- Finger motion immediately
- Monitor median nerve function
- Convert to removable splint
- Gentle active wrist ROM
- Continue finger exercises
- Suture removal
- X-ray to assess healing
- Consider K-wire removal (8-12 weeks)
- Progressive ROM
- Light functional activities
- K-wire removal (usually by 12 weeks)
- Progressive strengthening
- Increase ROM exercises
- CT if concerns about union
- Full strengthening program
- Grip strength recovery
- Return to work assessment
- Final outcome evaluation
Key rehabilitation principles:
- Finger motion from day 1 (prevent stiffness)
- Protected wrist motion starts at 2 weeks
- K-wires removed before aggressive ROM
- Grip strength takes 6-12 months to recover
- Long-term monitoring for arthritis
K-wires are typically left in place for 8-12 weeks to allow ligament healing. SL ligament is particularly slow to heal. Remove K-wires once adequate healing confirmed, then progress rehabilitation.
Outcomes and Prognosis
Outcome factors:
- Better Outcome
- Greater arc (trans-scaphoid)
- Worse Outcome
- Lesser arc (pure ligamentous)
- Better Outcome
- Less than 7 days
- Worse Outcome
- More than 7 days
- Better Outcome
- Anatomic
- Worse Outcome
- Residual malalignment
- Better Outcome
- None
- Worse Outcome
- Persistent median neuropathy
- Better Outcome
- Isolated
- Worse Outcome
- Multiple patterns
Prognostic considerations:
- Even with optimal treatment, outcomes are guarded
- Post-traumatic arthritis common long-term
- SL ligament rarely heals to normal
- Chronic instability may develop despite repair
- Greater arc (trans-scaphoid) may have better outcomes - bone heals better than ligament
Greater arc injuries (trans-scaphoid) may have better long-term outcomes than lesser arc (pure ligamentous). The scaphoid fracture, once healed, provides stability. In lesser arc, the SL ligament rarely heals to normal strength.
Guidelines, Registries & Global Practice
Global epidemiology (PubMed-verifiable):
- Figure
- Rare, high-energy injury pattern
- Source
- Herzberg multicentre series (PMID 8228045)
- Figure
- 25% (41 of 166)
- Source
- Herzberg 1993 (PMID 8228045)
- Figure
- 97% (palmar only 3%)
- Source
- Herzberg 1993 (PMID 8228045)
- Figure
- 61% of whole series
- Source
- Herzberg 1993 (PMID 8228045)
- Figure
- 56-80%
- Source
- Herzberg 1993 (PMID 8228045); Garcon 2022 (PMID 35609818)
- Figure
- Young adults, male predominance, high-energy MVA/fall/industrial mechanisms
- Source
- Herzberg 1993 (PMID 8228045)
There is no orthopaedic device registry that tracks perilunate dislocation outcomes, because management relies on K-wires, screws and ligament repair rather than registered implants. Arthroplasty registries (AOANJRR in Australia, NJR in England/Wales, AJRR in the USA) therefore do not capture this injury. Evidence is confined to retrospective single-centre and multicentre series; there are no randomised trials.
Side-by-side guidance and society position (global):
- Position on perilunate injury
- Carpal dislocation is a surgical emergency; urgent reduction, then open reduction, ligament repair and internal fixation in a hand unit
- Evidence level
- Expert consensus / Level IV
- Position on perilunate injury
- Open reduction and internal fixation with ligament repair is the standard of care; closed treatment alone is inadequate
- Evidence level
- Expert consensus / Level IV
- Position on perilunate injury
- Combined volar-dorsal or dorsal-only ORIF with carpal stabilisation; carpal tunnel decompression for persistent median symptoms
- Evidence level
- Expert consensus / Level IV
- Position on perilunate injury
- Emergent closed reduction followed by ORIF; scaphoid fixed with headless compression screw in trans-scaphoid patterns
- Evidence level
- Expert consensus / Level IV
Genuine debate persists over (1) dorsal-only versus combined volar-dorsal approach, (2) whether to routinely release the carpal tunnel - Garcon et al. (PMID 35609818) found median symptoms usually resolve with reduction alone - and (3) the role of dorsal spanning plates for early load-bearing. None of these is settled by Level I evidence.
Practical management across health systems: These high-energy injuries should be managed in centres with hand-surgery capability. Urgent closed reduction should be performed at the presenting centre to decompress the median nerve before transfer for definitive fixation. For any open component, antibiotic prophylaxis follows standard open-wound antimicrobial guidelines.
Be prepared to discuss Mayfield stages, X-ray interpretation (especially lateral view), lesser vs greater arc, acute carpal tunnel syndrome, and surgical approach. Understanding why 25% are missed (inadequate lateral film) is commonly tested.
MCQ Practice Points
Q: In Mayfield Stage III, which structures are disrupted? A: SL ligament + lunocapitate joint (space of Poirier) + LT ligament. This represents complete perilunate dislocation. Stage IV adds dorsal radiocarpal ligament failure with lunate dislocating volarly.
Q: What is the key X-ray finding on lateral view for perilunate vs lunate dislocation? A: In perilunate: lunate maintains contact with radius, capitate is dorsal to lunate. In lunate dislocation: lunate loses radius contact and tips volarly ("spilled teacup" sign).
Q: What percentage of perilunate dislocations are missed on initial presentation? A: 25% (approximately one quarter). This is usually due to inadequate lateral X-ray or not recognizing the abnormal carpal alignment. Always look at the lateral view for colinearity of radius-lunate-capitate.
Q: What is the difference between lesser arc and greater arc injuries? A: Lesser arc = pure ligamentous (injury through SL, lunocapitate, LT ligaments). Greater arc = with fractures (most commonly trans-scaphoid - 61%). Greater arc injuries may have better long-term prognosis as bone heals better than ligament.
Q: Why is median nerve assessment critical in perilunate dislocations? A: Acute carpal tunnel syndrome occurs in up to 25% of cases. The dislocated carpal bones compress the median nerve. This is an urgent indication for reduction - delay risks permanent nerve damage.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old man comes to your clinic referred by his GP. He fell off a motorcycle 3 weeks ago and was seen in another hospital's ED. He was told he had a 'wrist sprain' and given a splint. He has persistent pain and weakness. You obtain new X-rays. What are you looking for and what might you find?”
“A 35-year-old woman is brought to ED after a high-speed MVA. She has numbness and tingling in her thumb, index, and middle fingers. Her wrist is swollen and painful. X-rays show a lunate dislocation (Stage IV Mayfield). What is your management?”
“A 25-year-old construction worker falls from scaffolding onto his outstretched hand. X-rays show a perilunate dislocation with a scaphoid fracture through the waist. How does this change your management compared to a pure ligamentous injury?”
MAYFIELD STAGES
- Stage I: Scapholunate ligament rupture
- Stage II: + Lunocapitate (space of Poirier)
- Stage III: + Lunotriquetral (complete perilunate)
- Stage IV: + Dorsal radiocarpal → lunate dislocates volarly
KEY X-RAY FINDINGS
- LATERAL VIEW IS KEY
- Normal: radius-lunate-capitate colinear
- Perilunate: capitate dorsal, lunate maintains radius contact
- Lunate dislocation: lunate tilts volarly (spilled teacup)
LESSER VS GREATER ARC
- Lesser arc: pure ligamentous
- Greater arc: with fractures (trans-scaphoid 61%)
- Greater arc may have better prognosis
- Bone heals better than ligament
CRITICAL POINTS
- 25% missed on initial presentation
- Acute carpal tunnel syndrome in 25%
- Urgent reduction required
- Surgery almost always required
SURGICAL APPROACH
- Combined dorsal and volar approach
- Volar: CTR, visualize reduction
- Dorsal: ligament repair, K-wire fixation
- Fix scaphoid if trans-scaphoid
PROGNOSIS
- 50% develop arthritis long-term
- 30-50% chronic instability
- SL ligament rarely heals to normal
- Even optimal treatment has guarded prognosis
Evidence Base
- Loaded 32 cadaver wrists to failure, producing 13 perilunate and 2 lunate dislocations. Defined the mechanism as extension, ulnar deviation and intercarpal supination, with sequential ligament failure proceeding from radial to ulnar.
- Classified injury into four stages of progressive perilunar instability (PLI): Stage I scapholunate diastasis through to Stage IV lunate dislocation (greatest instability).
- Reduction was achieved by reversing the mechanism (intercarpal pronation, radial deviation, palmar flexion).
- Series of 166 perilunate dislocations/fracture-dislocations; the diagnosis was missed initially in 41 cases (25%). Displacement was dorsal in 97% and palmar in only 3%.
- Trans-scaphoid perilunate fracture-dislocations represented 61% of the whole series; fracture-dislocations outnumbered pure dislocations roughly two to one.
- In the 115 cases followed (mean 6 years), open injury and delayed treatment adversely affected results; post-traumatic arthritis occurred in 56% even when treated early.
- 30 patients (14 dislocations, 16 fracture-dislocations) reviewed at a mean of 18 years. Radiographic arthritis occurred in 70% of cases, yet its clinical and functional impact appeared low.
- Mean flexion-extension arc was 68%, grip strength 70% and mean Mayo wrist score 70 relative to the contralateral side.
- Six patients developed CRPS type 1; the two lowest Mayo wrist scores corresponded to the patients with the most advanced arthritis.
- Combined volar-dorsal approach in 11 perilunate dislocations/fracture-dislocations, mean 13 hours from injury to surgery, mean follow-up 30 months.
- Flexion-extension arc averaged 71% and grip strength 77% of the contralateral side; all 8 wrist fractures united and patient satisfaction was high in 9 of 11.
- No scapholunate dissociation or significant DISI persisted, although one wrist developed SLAC arthritis.
- 32 patients (7 dislocations, 25 fracture-dislocations) at mean 9.9-year follow-up; radiographic osteoarthritis in 79% and residual carpal instability in 16%.
- The magnitude of lunate displacement (injury stage) and older patient age were significant predictors of poorer long-term functional outcome and arthritis.
- Symptoms of median nerve compression generally resolved with reduction alone in this cohort.
- 45 wrists undergoing proximal row carpectomy (PRC), including chronic perilunate dislocation/fracture-dislocation, with mean 32-month follow-up.
- Active flexion-extension averaged 70 degrees with grip strength 51% of the unaffected side; pain reduced 71% at rest and 44% after strenuous activity.
- PRC is contraindicated when the capitate head or lunate fossa cartilage is degenerate.