Mechanisms, Reversal and Perioperative Management
- ANTIPLATELETS: ASPIRIN irreversibly inhibits COX-1, reducing thromboxane A2 for the platelet lifespan (~7-10 days); it is usually CONTINUED through most orthopaedic surgery (low bleeding risk) and especially for vascular/cardiac indications. P2Y12 inhibitors (clopidogrel, prasugrel, ticagrelor) are stopped ~5-7 days before high-bleeding-risk surgery, but DUAL antiplatelet therapy after a recent coronary STENT should NOT be interrupted without cardiology input. Reversal is by platelet transfusion and tranexamic acid.
- HEPARINS: UNFRACTIONATED HEPARIN potentiates ANTITHROMBIN to inhibit both thrombin (IIa) and factor Xa, is given IV with a short half-life, is monitored by APTT and is fully reversed by PROTAMINE (watch for heparin-induced thrombocytopenia, HIT); LOW-MOLECULAR-WEIGHT HEPARIN (e.g. enoxaparin) acts mainly on factor Xa, is given subcutaneously, is renally cleared with a longer half-life, and is only PARTIALLY reversed by protamine - LMWH is the usual agent for prophylaxis and for bridging.
- WARFARIN is a vitamin K antagonist that inhibits the vitamin-K-dependent clotting factors II, VII, IX and X (and proteins C and S), is monitored by the INR, and has a long half-life so it is typically STOPPED about 5 DAYS before elective surgery; it is reversed by VITAMIN K (which works slowly, over hours) and, for urgent reversal, by PROTHROMBIN COMPLEX CONCENTRATE (PCC) or FFP.
- DOACs (direct oral anticoagulants) are either DIRECT THROMBIN (IIa) inhibitors - DABIGATRAN, reversed by IDARUCIZUMAB - or DIRECT FACTOR Xa inhibitors - RIVAROXABAN, APIXABAN, EDOXABAN, reversed by ANDEXANET ALFA (or PCC if unavailable); they have a relatively short half-life and are RENALLY cleared (most for dabigatran), so they are stopped ~1-3 DAYS before surgery depending on the drug, bleeding risk and renal function, and - importantly - they do NOT require heparin BRIDGING.
- The perioperative decision balances the patient's THROMBOTIC risk (the reason for anticoagulation - e.g. atrial fibrillation, mechanical heart valve, recent VTE or coronary stent) against the BLEEDING risk of the surgery: BRIDGING with LMWH is reserved for HIGH thrombotic risk on WARFARIN (e.g. mechanical valve, recent VTE/AF with high CHA2DS2-VASc) and is NOT used for DOACs; neuraxial anaesthesia requires strict timing to avoid spinal haematoma, and anticoagulation is resumed once haemostasis is secure.
- For URGENT surgery (e.g. a HIP FRACTURE, where operating within ~24-48 h reduces mortality) the principle is not to delay excessively: aspirin/clopidogrel generally do NOT need stopping (use TXA +/- platelets if bleeding); WARFARIN is reversed early with VITAMIN K (PCC if truly emergent) to allow surgery; DOACs are stopped and, if surgery cannot wait, reversed with the specific antidote or PCC; LMWH bridging is generally not indicated when surgery is early and anticoagulation is restarted promptly.
- “Warfarin = II/VII/IX/X (INR; reverse vitamin K slow / PCC fast); heparin = antithrombin -> IIa+Xa (APTT; protamine); LMWH = anti-Xa (renal; partial protamine).
- “DOACs: dabigatran = direct IIa (reverse idarucizumab); rivaroxaban/apixaban/edoxaban = direct Xa (reverse andexanet alfa/PCC). Renally cleared, short half-life - NO bridging needed.
- “Balance thrombotic vs bleeding risk; bridge only HIGH-risk warfarin patients; hip fracture - don't delay (reverse warfarin with vitamin K; continue aspirin).
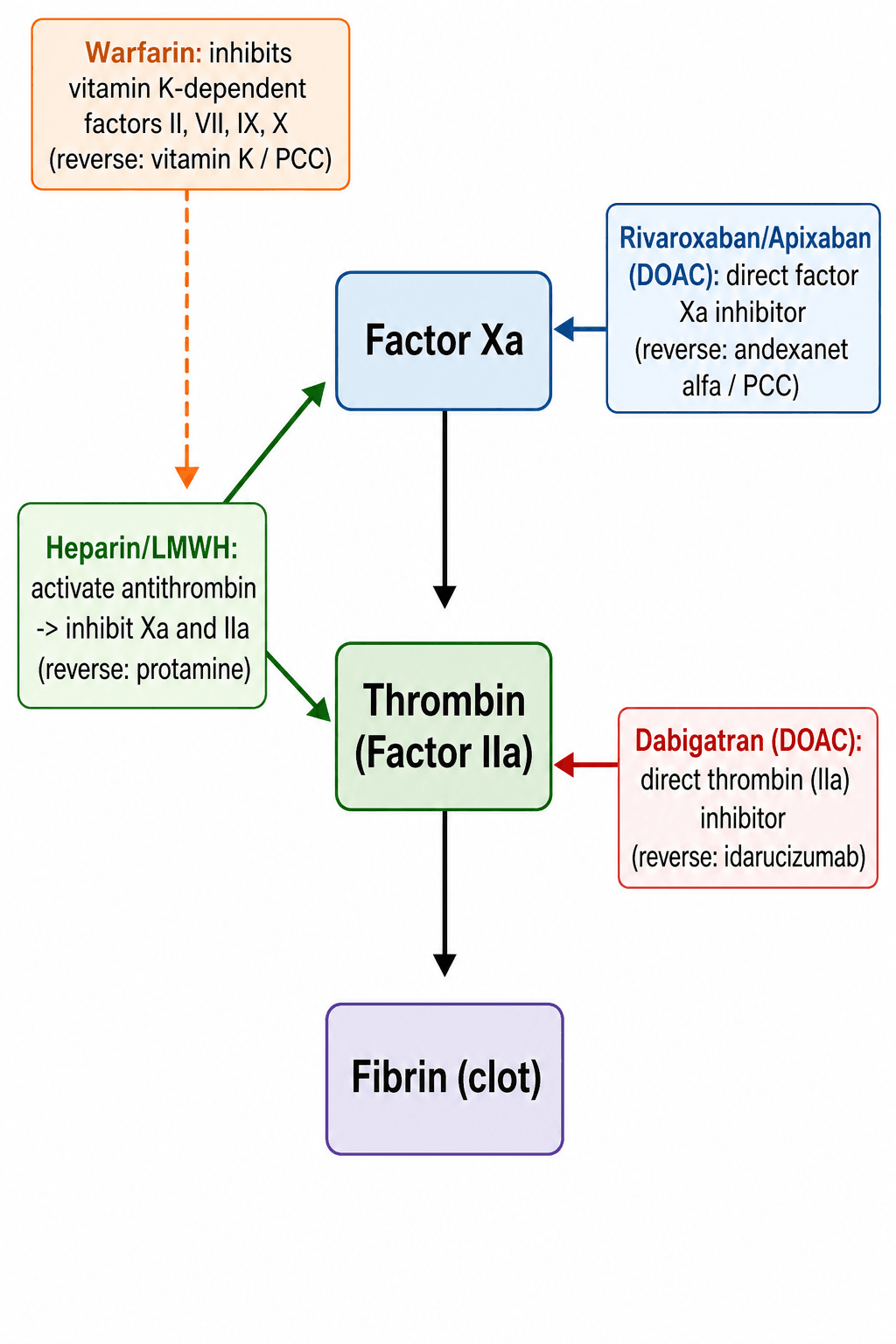
Warfarin -> II/VII/IX/X; heparin -> antithrombin (IIa+Xa); dabigatran -> thrombin (IIa); rivaroxaban/apixaban -> factor Xa.
Warfarin -> vitamin K / PCC; heparin -> protamine; dabigatran -> idarucizumab; Xa inhibitors -> andexanet alfa / PCC; antiplatelets -> platelets / TXA.
The Drug Classes & Their Targets
The antithrombotic drugs act at different points in haemostasis. Antiplatelets prevent platelet activation/ aggregation: aspirin irreversibly inhibits COX-1 (reducing thromboxane A2), and the P2Y12 inhibitors (clopidogrel, prasugrel, ticagrelor) block the platelet ADP receptor. The anticoagulants act on the clotting cascade: unfractionated heparin potentiates antithrombin to inhibit both thrombin (IIa) and factor Xa; LMWH acts mainly on factor Xa; warfarin inhibits the vitamin-K-dependent factors II, VII, IX, X; and the DOACs directly inhibit a single factor - dabigatran inhibits thrombin (IIa) while rivaroxaban, apixaban and edoxaban inhibit factor Xa. Knowing each target also tells you the monitoring (heparin - APTT; warfarin - INR; DOACs - none routinely) and the reversal agent.
| Drug | Target | Monitor | Reversal |
|---|
Perioperative Management
- Balance the risks: weigh the patient's thrombotic risk (why they are anticoagulated - AF with high CHA2DS2-VASc, mechanical valve, recent VTE, recent coronary stent) against the bleeding risk of the operation.
- Aspirin: usually continue through orthopaedic surgery (especially for cardiac/vascular indications).
- P2Y12 inhibitors: stop ~5-7 days before high-bleed surgery, but do NOT interrupt dual antiplatelet therapy after a recent stent without cardiology input.
- Warfarin: stop ~5 days before elective surgery (check INR normalises); BRIDGE with LMWH only for HIGH thrombotic risk (mechanical valve, recent VTE); restart post-op when haemostasis is secure.
- DOACs: stop 1-3 days before surgery (longer for dabigatran with renal impairment) - NO heparin bridging needed because of their short half-life; restart when haemostasis allows.
- Neuraxial anaesthesia: follow strict timing rules off all agents to avoid a spinal/epidural haematoma.
A hip fracture should be operated on early (within ~24-48 hours) to reduce mortality, so anticoagulation must be managed promptly rather than by simply waiting. Aspirin and clopidogrel generally do not need stopping - use tranexamic acid and, rarely, platelet transfusion if bleeding. WARFARIN should be reversed early with vitamin K (PCC reserved for the truly emergent case) so surgery can proceed within ~24 hours, and it is resumed afterwards. DOACs are stopped and, if surgery cannot wait, reversed with the specific antidote (idarucizumab/andexanet) or PCC, accounting for renal function. LMWH bridging is generally not indicated when surgery is early and anticoagulation is restarted promptly. Always involve haematology/ anaesthesia for complex cases.
Evidence & Key Studies
Perioperative management of patients receiving non-vitamin K antagonist oral anticoagulants (DOACs)
- DOACs are direct thrombin inhibitors (dabigatran) or direct factor Xa inhibitors (rivaroxaban, apixaban, edoxaban); high-bleed surgery is generally safe ~2 days after stopping (longer for dabigatran with renal impairment), and neuraxial anaesthesia ~3 days after.
- DOACs do NOT require preoperative heparin bridging.
- For emergent surgery, use specific reversal agents - idarucizumab for dabigatran and andexanet alfa for the Xa inhibitors - or prothrombin complex concentrate if unavailable.
Management of proximal femur fractures in patients on antiplatelet and anticoagulant therapy
- Aspirin and clopidogrel (alone or combined) do NOT need stopping before hip-fracture surgery; bleeding is managed with antifibrinolytics and, rarely, platelet concentrate.
- Warfarin is reversed early with vitamin K (PCC reserved for extreme cases) to allow surgery within 24 hours; DOACs are stopped 24-48 hours pre-op, with antidote or PCC in extreme cases.
- LMWH bridging is not indicated with early surgery and prompt restart, except for extreme thrombotic risk.
According to PubMed, the DOAC mechanisms, cessation timing, no-bridging rule and specific reversal agents come from the cited Kim review, and the practical hip-fracture management (continue antiplatelets, reverse warfarin with vitamin K, stop/reverse DOACs, avoid routine bridging) from the cited Steno review. The mechanisms, monitoring and reversal of heparin/warfarin and the thrombotic-versus-bleeding-risk framework are standard, well-established pharmacology. (See also our Thromboprophylaxis, DVT Diagnosis/Treatment and Preoperative Optimisation topics.)
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the mechanism and reversal of the main anticoagulants, and how you would manage an elective arthroplasty patient on each.”
“A patient on warfarin (or a DOAC) presents with a hip fracture. How do you manage the anticoagulation?”
Mnemonics & Memory Aids
WHO-D
Hook:WHO-D: Warfarin, Heparin, Oral antiplatelets, DOACs.
REVERSE
Hook:REVERSE: protamine (heparin), vitamin K/PCC (warfarin), idarucizumab (dabigatran), andexanet (Xa).
Mechanisms
- Aspirin: COX-1 (irreversible); P2Y12 inhibitors: ADP receptor
- Heparin: antithrombin -> IIa+Xa; LMWH: mainly Xa; warfarin: II/VII/IX/X
- DOACs: dabigatran -> IIa; rivaroxaban/apixaban/edoxaban -> Xa
Monitoring & reversal
- Heparin = APTT (protamine); warfarin = INR (vitamin K slow / PCC fast)
- Dabigatran -> idarucizumab; Xa inhibitors -> andexanet alfa / PCC
- Antiplatelets -> platelets / TXA
Elective surgery
- Continue aspirin; stop P2Y12 ~5-7 days (not after recent stent)
- Warfarin: stop ~5 days; bridge LMWH only if HIGH thrombotic risk
- DOACs: stop 1-3 days (renal-adjusted); NO bridging; neuraxial timing rules
Hip fracture (urgent)
- Operate early (24-48h); don't just wait for anticoagulation to clear
- Warfarin: reverse with vitamin K (PCC if emergent); DOAC: stop +/- antidote/PCC
- Continue aspirin/clopidogrel (TXA if bleeding); no routine bridging