Surface Low-Grade Cartilage Malignancy
- PERIOSTEAL (juxtacortical) CHONDROSARCOMA is a rare malignant CARTILAGE tumour arising on the bone SURFACE (from the periosteum/cortex) rather than within the medullary cavity; it most often involves the METAPHYSIS of the long bones of the extremities. In the largest single-centre series (Rizzoli, n = 55; median age 37, 62% male, median size 7.5 cm) only 42% were grade 1 - 49% were grade 2, 5% grade 3 and 4% dedifferentiated - so 'low-grade' in practice means 'grade 1 OR 2'.
- Behaviour is indolent but not benign. Over a median 137 months in 54 followed patients there were 4 local recurrences (7.4%) and 6 lung metastases (11.1%); ALL SIX who metastasised DIED OF DISEASE, while 46 (85%) were alive without disease. Neither grade nor any other clinical or morphological parameter was statistically associated with overall or disease-free survival - so you cannot reassure a patient on the basis of a grade 1 biopsy.
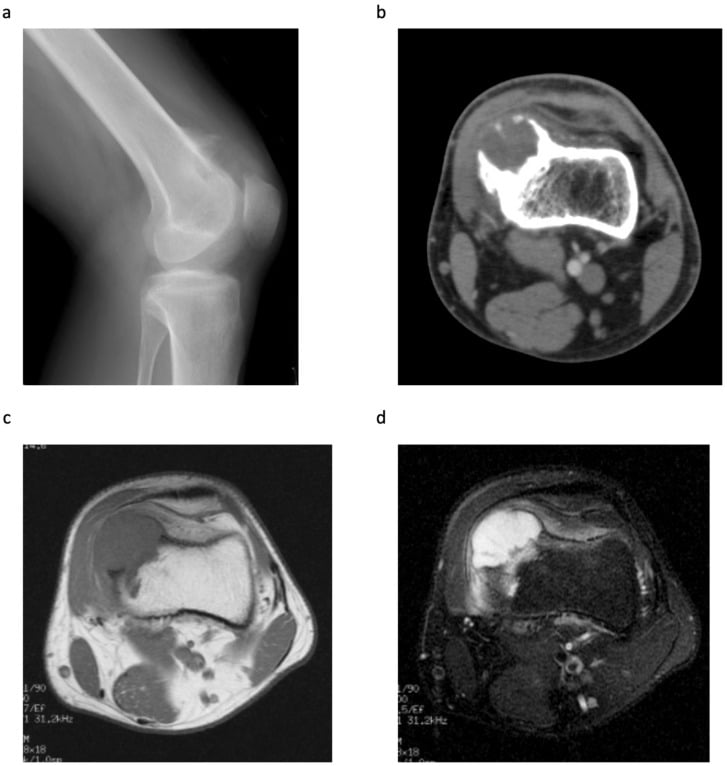
- A proportion of periosteal chondrosarcomas harbour IDH1 mutations (as in other cartilage tumours), which can support the diagnosis on molecular testing; the lesion shows a chondroid (cartilage) matrix on imaging, with cortical scalloping/thickening and a surface soft-tissue mass.
- The key DIFFERENTIAL is from the benign PERIOSTEAL CHONDROMA (a small, benign surface cartilage tumour, usually a few centimetres) and from PERIOSTEAL (surface) OSTEOSARCOMA - distinction rests on size and aggressiveness, the matrix (chondroid in chondrosarcoma vs osteoid in osteosarcoma), and the histological grade; a periosteal chondroma that is large or aggressive should raise concern for chondrosarcoma.
- DIAGNOSIS requires imaging (radiograph/CT for the chondroid matrix and cortical changes, MRI for extent) and a properly PLANNED BIOPSY read at a specialist centre, with staging where indicated; as with all bone sarcomas, an unplanned excision must be avoided.
- MANAGEMENT is adequate surgical EXCISION, and cartilage tumours are relatively CHEMO/RADIO-RESISTANT, so surgery is the mainstay. Know the caveat the literature's own headline hides: the Rizzoli authors conclude that periosteal chondrosarcoma 'can be adequately treated with marginal excision', but in their own cohort the margin was WIDE OR RADICAL in 38 of 54 (70.4%) and marginal in only 9 (16.7%), with 7 (12.9%) intralesional - so the good survival was achieved predominantly under WIDE margins, and 'marginal is enough' is an inference from a small subgroup, not a tested comparison.
- “Periosteal chondrosarcoma = rare SURFACE (juxtacortical) malignant cartilage tumour, usually LOW-grade, at the METAPHYSIS of long bones. Chondroid matrix; cortical scalloping; IDH1 in a proportion.
- “Rizzoli n = 55: 42% grade 1, 49% grade 2. At median 137 months - 4 local recurrences (7.4%), 6 lung metastases (11.1%), all six dead of disease; 85% alive without disease. NO parameter, grade included, predicted survival.
- “Differential: benign periosteal chondroma (small) vs surface osteosarcoma (osteoid matrix). Treatment = adequate EXCISION; chemo/radio-resistant. The 'marginal excision is adequate' conclusion comes from a cohort in which 70.4% actually had WIDE/radical margins.
A surface (juxtacortical) cartilage lesion at the metaphysis of a long bone, with chondroid matrix and cortical changes = periosteal chondrosarcoma (usually low-grade, good prognosis).
Benign periosteal chondroma (small) vs periosteal chondrosarcoma (larger/aggressive) vs surface osteosarcoma (osteoid matrix). Grade on a planned biopsy.
Imaging: Periosteal Chondroma versus Periosteal Chondrosarcoma
- Size. A periosteal chondroma is small - usually under about 3 cm. A periosteal chondrosarcoma is larger (typically over 5 cm; median 7.5 cm across the 55-case Rizzoli series).
- Cortical response. The chondroma produces a well-defined, saucer-shaped cortical defect (scalloping) with a sclerotic rim and a solid periosteal buttress at its margins. The chondrosarcoma produces more aggressive/irregular cortical scalloping and thickening, sometimes frank cortical destruction, and a larger, bulkier soft-tissue mass.
- Matrix. Both show chondroid ring-and-arc mineralisation on radiograph/CT; more extensive, irregular mineralisation and a larger soft-tissue component favour the chondrosarcoma. MRI (lobulated high T2 signal from the hyaline cartilage) shows the true extent.
- Marrow. Both are surface lesions and typically spare the medullary cavity; any medullary permeation is worrying.
- Bottom line. The two overlap radiographically, so larger size, aggressive cortical change and a soft-tissue mass raise suspicion for chondrosarcoma - but the grade and definitive diagnosis are settled on a planned biopsy at a sarcoma unit.
Q: How do you distinguish a periosteal chondroma from a periosteal chondrosarcoma on imaging?
A: Both are surface cartilage lesions with a chondroid (ring-and-arc) matrix and cortical scalloping, but a periosteal chondroma is small (usually under about 3 cm), with a well-defined saucerised cortical defect, a sclerotic rim and a solid periosteal buttress, and no significant soft-tissue mass; a periosteal chondrosarcoma is larger (typically over 5 cm), with more aggressive or irregular cortical scalloping/thickening and a bulkier soft-tissue mass. They overlap, so size, aggressive cortical change and a soft-tissue mass raise suspicion - but grade and diagnosis are settled on a planned biopsy.
The IDH1 / IDH2 Mutation
- What they are. IDH1 and IDH2 encode isocitrate dehydrogenase. In cartilage tumours they carry heterozygous gain-of-function point mutations (classically at IDH1 codon 132) that make the enzyme produce the oncometabolite 2-hydroxyglutarate (2-HG), which dysregulates DNA and histone methylation and drives abnormal chondrogenesis.
- Where they occur. IDH1/IDH2 mutations are found in about half of conventional central chondrosarcomas and enchondromas, in the enchondromatoses (Ollier disease and Maffucci syndrome), and in roughly a third of the periosteal chondrosarcomas in which mutational analysis was technically feasible - note that qualifier, since it means the true mutation rate in the whole cohort is unknown, and a negative result therefore never excludes the diagnosis.
- Why it matters. Detecting an IDH mutation helps confirm that a lesion is a cartilage tumour and helps distinguish it from IDH-wild-type mimics - notably chondroblastic osteosarcoma and chordoma. IDH is also a therapeutic target (IDH inhibitors are in use/trials for IDH-mutant tumours), though surgery remains the mainstay for chondrosarcoma.
Q: What is the IDH1 mutation and why is it useful in periosteal chondrosarcoma?
A: IDH1 (and IDH2) encode isocitrate dehydrogenase; heterozygous gain-of-function mutations (classically IDH1 codon 132) make the enzyme produce the oncometabolite 2-hydroxyglutarate, dysregulating methylation and driving chondrogenesis. They occur in about half of conventional cartilage tumours and the enchondromatoses (Ollier/Maffucci) and in around a third of periosteal chondrosarcomas. Detecting the mutation helps confirm a cartilage tumour and distinguish it from IDH-wild-type mimics (chondroblastic osteosarcoma, chordoma); IDH inhibitors are an emerging therapy, but surgery remains the mainstay.
Features, Differential & Management
Periosteal chondrosarcoma is a rare surface (juxtacortical) malignant cartilage tumour, arising on the bone surface, usually at the metaphysis of a long bone, and the great majority are low/intermediate grade with indolent behaviour and a good prognosis. It shows a chondroid matrix with cortical scalloping/ buttressing, and a proportion carry IDH1 mutations. It must be distinguished from the benign periosteal chondroma (small) and from surface osteosarcoma (osteoid matrix). Diagnosis uses imaging plus a planned biopsy at a specialist centre; management is adequate excision - and, as cartilage tumours are chemo/radio-resistant, surgery is the mainstay. Read the prognosis honestly: in the largest series (n = 55) 11% developed lung metastases and every one of those patients died of disease, and no parameter - grade included - predicted who they would be.
- Nature
- Benign
- Key features
- Small (usually a few cm) surface cartilage tumour; saucerised cortex
- Nature
- Malignant (usually low-grade)
- Key features
- Larger, metaphyseal, chondroid matrix, cortical scalloping; IDH1 in a proportion
- Nature
- Malignant (intermediate-grade)
- Key features
- Diaphyseal, chondroblastic but osteoid-producing
Periosteal chondrosarcoma is, in the great majority of cases, a grade 1-2 surface malignancy that behaves indolently and is cured by adequate surgical excision, and because cartilage tumours are relatively resistant to chemotherapy and radiotherapy, surgery is the mainstay. Do not let the published headline talk you into a smaller operation than the evidence supports: the series that concluded marginal excision is adequate achieved its results with wide or radical margins in 70.4% of patients, and its own analysis found no clinical or pathological parameter that predicted survival - so grade cannot be used to justify accepting a close margin. The pitfalls are diagnostic. A benign periosteal chondroma that is large or behaves aggressively should raise concern for chondrosarcoma, and a surface lesion that produces osteoid is a surface osteosarcoma, not a chondrosarcoma - so the diagnosis and grade must be established on a properly planned biopsy read at a specialist centre, with appropriate imaging and staging, before definitive surgery. As with all bone sarcomas, an unplanned excision of an undiagnosed surface mass compromises the eventual oncological result.
Mnemonics & Memory Aids
CHONDRAL
Hook:CHONDRAL: Cartilage matrix, differential (chondroma/sarcoma/osteosarcoma), Often low-grade, Near metaphysis, Diagnose+grade, Resect to a clear margin, chemo/radio-resistant.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“How do you approach a surface cartilage lesion at the metaphysis of the femur reported as a possible periosteal chondrosarcoma?”
What it is
- Rare surface (juxtacortical) malignant cartilage tumour
- Usually low/intermediate grade; metaphysis of long bones
- Chondroid matrix + cortical scalloping; IDH1 in a proportion
Behaviour & differential
- Rizzoli n = 55, median follow-up 137 months: 7.4% local recurrence, 11.1% lung metastasis, all six metastatic patients dead; 85% alive without disease
- No clinical or pathological parameter - grade included - predicted survival
- Differential: benign periosteal chondroma (small); surface osteosarcoma (osteoid)
Management
- Planned biopsy + grade at a sarcoma unit; stage as indicated
- Adequate excision aiming at a clear margin; 70.4% of the published series had wide/radical margins
- 'Marginal excision is adequate' is a conclusion, not a tested comparison - no trial of margin width exists
- Cartilage tumours chemo/radio-resistant - surgery is the mainstay
Evidence & Key Studies
Periosteal chondrosarcoma: a case series with survivorship analysis
- 55 periosteal chondrosarcomas from a single Italian referral centre (Rizzoli), retrospective. Median age 37 years, 62% male, median tumour size 7.5 cm; the great majority involved the metaphysis of long bones of the extremities. Grade: 23 (42%) grade 1, 27 (49%) grade 2, 3 (5%) grade 3, 2 (4%) dedifferentiated.
- Surgery: 30 subtotal resection, 22 tangential resection, 3 amputation. Margins (reported in 54): wide/radical 38 (70.4%), marginal 9 (16.7%), intralesional 7 (12.9%) - so the cohort behind the 'marginal is adequate' conclusion was predominantly widely resected.
- Outcome at median 137 months in 54 followed patients: 4 local recurrences (7.4%), 6 lung metastases (11.1%). All six who metastasised died of disease; 2 died of unrelated causes; 46 (85%) alive without disease. Heterozygous IDH1 codon 132 mutations in a third of the cases in which analysis was feasible.
- Neither overall nor disease-free survival was statistically associated with any clinical or pathological parameter considered - including grade. Limitations: single centre, retrospective, no comparison of margin strategies, and event numbers (4 and 6) far too small to power the prognostic analysis, so 'no predictor' means underpowered rather than proven absent.
This is the sentence most likely to be quoted back at you, and the one most likely to be misused. It is the authors' conclusion, not their protocol. Their 54 margin-reported patients were resected wide or radical in 70.4%, marginal in 16.7% and intralesional in 12.9% - there was no comparison of one margin strategy against another, and with only 4 recurrences and 6 metastases the study had no power to detect a difference if one existed. The defensible answer in a viva is: periosteal chondrosarcoma behaves indolently enough that a planned marginal excision achieving a clear margin may suffice for a small grade 1 lesion at a sarcoma unit, but the published survival was obtained mostly under wide margins, and since no parameter - grade included - predicted which patients would metastasise and die, the burden of proof sits with the surgeon proposing the smaller resection.
Every figure quoted above - n = 55, median age 37, 62% male, median size 7.5 cm, the grade distribution, the operation and margin counts, the 4 local recurrences and 6 fatal lung metastases at median 137 months, the IDH1 codon 132 rate, and the absence of any surviving prognostic parameter - comes from the cited Pacheco series (DOI). The distinction from benign periosteal chondroma and from surface osteosarcoma, the chemo/radio-resistance of cartilage tumours, and the biopsy/staging principles are standard, well-established teaching. No randomised or comparative trial of margin width exists in this tumour, and no validated surveillance interval or risk score has been published for it.