Proximal and middle phalanx fractures of the digits
- Rotational malunion is the most functionally limiting deformity
- Check for scissoring - all fingers should point to scaphoid tubercle when flexed
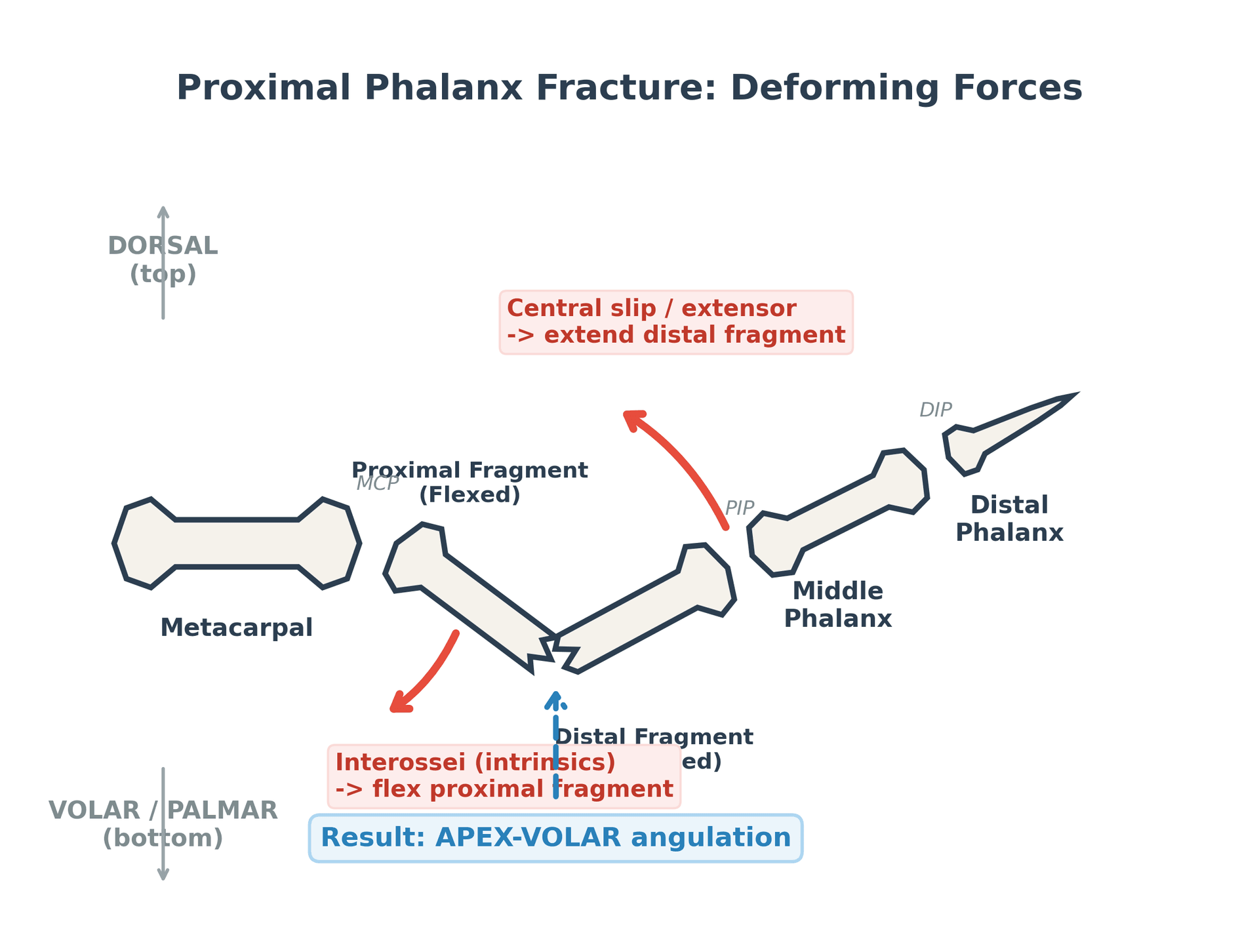
- PP apex volar angulation from intrinsic pull on proximal fragment
- MP angulation varies - proximal apex volar (central slip), distal apex dorsal (FDS)
- “Stable fractures: buddy tape + early motion
- “Unstable: K-wires, screws, or plate fixation
- “Unicondylar fractures often need ORIF to prevent angular deformity
- “Stiffness is the enemy - mobilize early when fixation stable
Phalangeal Fractures
All fingertips should point to SCAPHOID TUBERCLE when flexed. Look for SCISSORING of digits. Even 5 degrees rotation = 1.5cm overlap at fingertip. Rotational malunion is FUNCTIONALLY DEVASTATING.
Apex volar angulation at PP (intrinsics pull proximal fragment). Variable angulation at MP (FDS vs central slip). Less angulation tolerated in index/long (more visible). More tolerated in ring/small (compensatory CMC motion).
Overview
Overview
Phalangeal fractures are among the most common upper extremity injuries, representing approximately 10% of all fractures. The proximal phalanx (PP) and middle phalanx (MP) present distinct management challenges due to the complex interplay of tendons, ligaments, and muscles surrounding each bone. Understanding the deforming forces acting on these fractures is essential for appropriate reduction and stable fixation.
The primary goal of treatment is to restore anatomic alignment, particularly rotation, while allowing early mobilization to prevent the stiffness that is the major cause of poor outcomes in these injuries. Even minor rotational malalignment can result in significant functional impairment, with scissoring of digits during grip and pinch activities. The hand surgeon's mantra "stable fracture, mobile joint" encapsulates the treatment philosophy.
Classification is based on bone involved (PP vs MP), location (base, shaft, neck, head), and fracture pattern (transverse, oblique, spiral, comminuted). Each combination has specific biomechanical implications that guide treatment selection.
Anatomy and Biomechanics
Anatomy and Biomechanics
Proximal Phalanx Anatomy
- Broadest at base, tapers distally
- Biconcave base articulates with MC head
- Bicondylar head articulates with MP base
- Rectangular cross-section (makes plating easier)
- Extensor mechanism dorsal (conjoined lateral bands)
- FDP tendon volar (in sheath)
- Interossei insert on base (volar to axis)
- Lumbricals cross volar to MCP joint
- Deforming Force
- Interossei
- Result
- Flexion
- Deforming Force
- Central slip + lateral bands
- Result
- Extension
- Deforming Force
- Apex volar angulation
- Result
Middle Phalanx Anatomy
- Shortest phalanx
- Base biconcave, head bicondylar
- More tubular than PP
- Central slip inserts on dorsal base
- FDS splits and inserts on volar-lateral shaft
- FDP passes between FDS slips
- Lateral bands converge to form terminal tendon
- Proximal Pull
- Central slip (extension)
- Distal Pull
- FDS (flexion)
- Apex Direction
- Apex volar
- Proximal Pull
- FDS (flexion)
- Distal Pull
- Terminal tendon (extension)
- Apex Direction
- Apex dorsal
Vascular Supply
Digital Arteries:
- Proper digital arteries run along volar-lateral aspect
- Nutrient arteries enter volar cortex
- Periosteal stripping affects blood supply
Key Anatomical Points for Surgery
- Dorsal approach between extensor and lateral bands
- Avoid vincular system volarly
- Protect digital nerves at lateral aspect
- Lateral approach (between NV bundle and extensor)
- Dorsal approach (beneath extensor)
- Avoid volar plating (tendon adhesions)
Classification
Classification
Proximal Phalanx
- Characteristics
- Often intra-articular
- Treatment Considerations
- May need ORIF for articular
- Characteristics
- Strong deforming forces
- Treatment Considerations
- K-wire or plate
- Characteristics
- Condylar fractures
- Treatment Considerations
- Often need ORIF
- Characteristics
- Unicondylar/bicondylar
- Treatment Considerations
- ORIF for congruency
Middle Phalanx
- Characteristics
- Often pilon-type
- Treatment Considerations
- May need external fixation
- Characteristics
- FDS insertion affects apex
- Treatment Considerations
- Variable angulation
- Characteristics
- Rare
- Treatment Considerations
- Reduction important
- Characteristics
- Often associated with DIP injury
- Treatment Considerations
- Rare
AO/OTA Classification (Overview)
- A: Extra-articular
- B: Partial articular
- C: Complete articular
PIP Fracture-Dislocations and Condylar Fracture Stability
PIP Fracture-Dislocations and Condylar Fracture Stability
Two intra-articular patterns are tested far more often than their frequency would suggest because the management decision hinges on a single principle of articular stability. They deserve separate treatment from the diaphyseal fractures above.
Dorsal PIP Fracture-Dislocation
The commonest PIP fracture-dislocation is dorsal: a hyperextension/axial-load injury fractures the volar lip of the middle phalanx base (the volar plate attachment) and the head of the proximal phalanx rides dorsally. Stability - and therefore treatment - is determined by how much of the middle phalanx base articular surface is involved, because the volar lip and collateral ligament origins are what keep the joint reduced.
- Stability
- Stable - reduces and stays congruent in modest flexion
- Management
- Closed reduction + dorsal extension-block splinting, progressively extending; early motion
- Stability
- Tenuous / potentially unstable - may subluxate as the joint extends
- Management
- Extension-block splinting if congruent through useful arc; otherwise ORIF (screws / fragment fixation)
- Stability
- Unstable - cannot hold a congruent reduction
- Management
- Reconstruction: hemi-hamate (osteochondral) autograft arthroplasty, volar plate arthroplasty, or dynamic/force-couple external fixation
On the true lateral, look for loss of the smooth congruent PIP joint line - a dorsal "V" sign (the dorsal joint space gaps open while the volar space narrows) signals dorsal subluxation and an unstable fracture-dislocation, even when the AP looks acceptable. A truly concentric reduction must be confirmed on a lateral, not an oblique.
A volar PIP fracture-dislocation is much rarer but important because it is associated with central slip disruption (risk of a boutonnière deformity) and is often irreducible if the head buttonholes through the extensor mechanism.
Condylar (Unicondylar and Bicondylar) Fractures
Phalangeal head condylar fractures are intra-articular and inherently unstable because the attached collateral ligament continuously pulls the fragment. The examinable trap is that a "nondisplaced" unicondylar fracture is deceptively dangerous: a high proportion displace late if splinted (in the classic series the majority of nondisplaced fractures treated by splinting alone displaced, and single-K-wire fixation often failed).
Treat unicondylar fractures as unstable. Even genuinely nondisplaced fractures need either fixation or, if managed closed, very close (e.g. weekly) radiographic surveillance so late displacement is caught early. Displaced unicondylar fractures need ORIF with multiple K-wires or interfragmentary screws - a single K-wire gives poor rotational control and commonly redisplaces. Bicondylar fractures require restoration of the articular surface with a mini-condylar plate, accepting the higher stiffness cost of that exposure.
Clinical Presentation
Clinical Presentation
History
- Direct blow (crush injury)
- Axial load (ball-handling sports)
- Twisting injury (spiral fractures)
- Fall on outstretched hand
- Industrial accidents
- Hand dominance
- Occupation
- Sports/activities
- Previous hand injuries
- Time since injury
Physical Examination
- Swelling (localized vs diffuse)
- Deformity (angulation, shortening)
- Rotational malalignment
- Skin integrity (open fracture?)
- Nail bed alignment
- Semiflexion cascade: All fingertips should converge toward scaphoid tubercle
- Full flexion: Check for scissoring/overlap
- Finger extension: Assess nail plate alignment
- Compare to contralateral hand
- Point tenderness at fracture site
- Assess for crepitus (gentle)
- Evaluate stability
- Digital sensation (radial and ulnar aspects)
- Capillary refill
- Allen test for digital arteries
- FDP function (DIP flexion)
- FDS function (isolated PIP flexion)
- Extensor function
- Note if pain limits assessment
Associated Injuries
- Tendon avulsions (mallet, jersey finger)
- Ligament injuries (collateral, volar plate)
- Nerve injuries (digital nerve laceration)
- Vascular injuries (in open fractures)
- Nail bed injuries
Differential Diagnosis
The painful, swollen, deformed finger has several mimics. The key discriminators are the presence of a cortical break on radiographs, the location of maximal tenderness, and whether the deformity is correctable.
- Typical History
- Axial load, twist or crush
- Key Examination
- Point tenderness over shaft, possible scissoring
- Radiograph / Discriminator
- Cortical break; assess rotation and angulation
- Typical History
- Hyperextension or axial load
- Key Examination
- Visible joint deformity, springy block to motion
- Radiograph / Discriminator
- Loss of joint congruity without a shaft fracture
- Typical History
- Forced hyperextension (ball sport)
- Key Examination
- Volar PIP tenderness, dorsal instability
- Radiograph / Discriminator
- Small volar lip fragment at middle phalanx base
- Typical History
- Forced flexion (mallet) or hyperextension on grip (jersey)
- Key Examination
- Loss of active DIP extension or FDP flexion
- Radiograph / Discriminator
- Bony avulsion at distal phalanx base or none
- Typical History
- Lateral stress to finger
- Key Examination
- Tenderness over collateral, pain on lateral stress
- Radiograph / Discriminator
- Normal or small avulsion fleck; no shaft break
- Typical History
- Low-energy injury, may be trivial
- Key Examination
- Often little soft-tissue reaction
- Radiograph / Discriminator
- Lytic expansile lesion, typically proximal phalanx
Investigations
Investigations
Radiographic Assessment
- PA (posteroanterior): Fracture pattern, shortening
- True lateral: Angulation, displacement
- Oblique: Rotational assessment, condylar fractures
- Fracture location (base/shaft/neck/head)
- Fracture pattern (transverse/oblique/spiral)
- Angulation (degree and apex direction)
- Shortening
- Articular involvement
- Bone quality

CT Imaging
- Articular fractures (condylar, pilon)
- Complex comminuted patterns
- Surgical planning
- Unclear fracture pattern on XR
- 3D reconstruction
- Fragment number and size
- Articular surface assessment
- Guide surgical approach
MRI (Limited Role)
- Suspected ligament injury
- Occult fractures
- Tendon pathology
- Not routine for fractures
Ultrasound
- Dynamic tendon assessment
- Soft tissue masses
- Guided injections
Management Algorithm
Management Algorithm
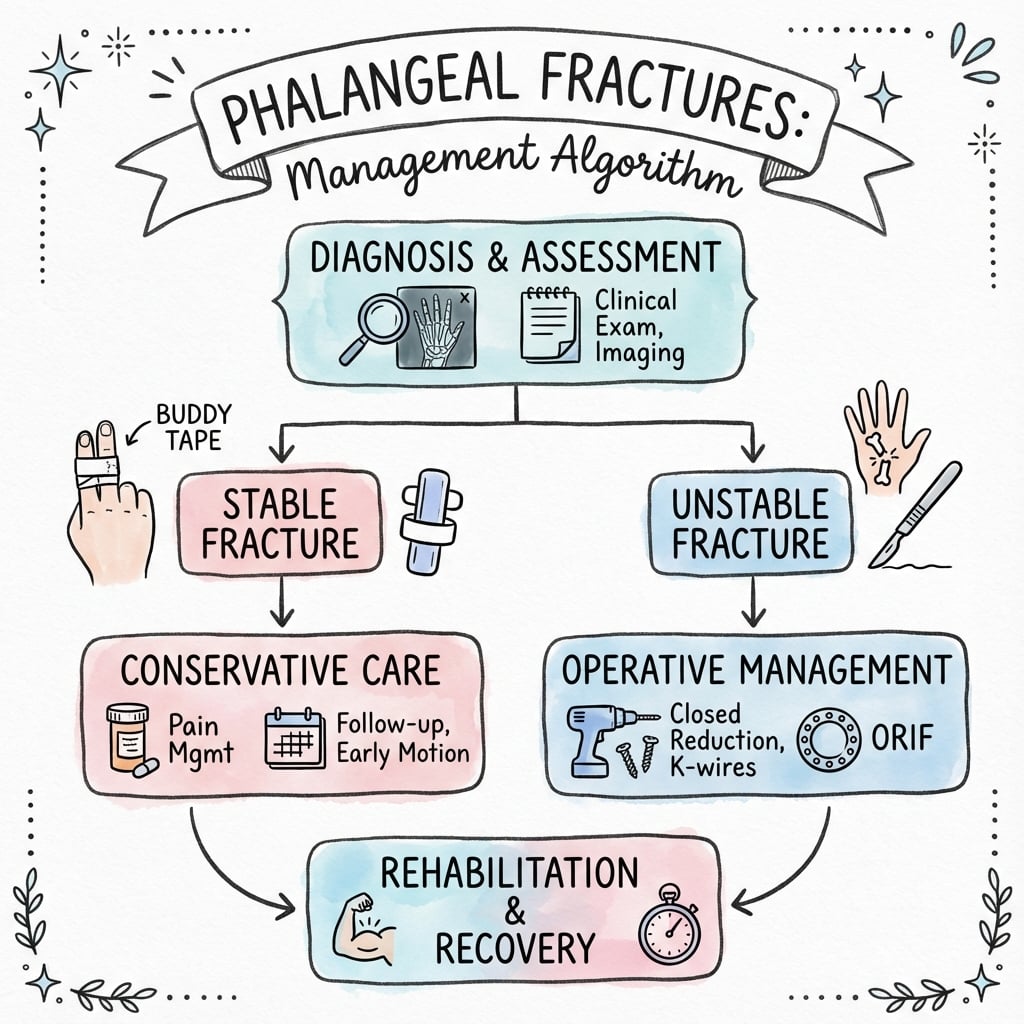
Non-Operative Treatment
- Stable, non-displaced fractures
- Acceptable alignment maintained
- No rotational deformity
- Patient compliance expected
- Tape affected finger to adjacent finger
- Provides stability through adjacent digit
- Allows early motion
- Ideal for stable fractures
- For base fractures with dorsal angulation
- MCP in 70-90 degrees flexion
- Prevents dorsal displacement
- Custom molded
- Immobilizes fracture
- Allows motion of unaffected joints
- Immobilization: 3-4 weeks
- Begin ROM exercises early when stable
- Buddy tape for protection 4-6 weeks total
- Hand therapy referral for optimal outcomes
Early mobilization when fracture stable prevents stiffness complications.
Surgical Technique
Surgical Technique
Cross K-Wire Pattern (Most Stable)
- Setup: Fluoroscopy, mini C-arm, 0.045" or 0.062" K-wires
- Reduction: Achieve closed reduction, hold with reduction forceps
- First wire: Insert dorsal-lateral, aim distal-medial, cross fracture site
- Second wire: Insert dorsal-medial, aim distal-lateral, cross first wire
- Check: PA and lateral fluoroscopy for reduction and wire position
- Finish: Cut and bend wires outside skin, apply dressing
Intramedullary Bouquet Technique
- Used for transverse fractures
- Multiple 0.028" K-wires inserted retrograde from fracture site
- Drive across fracture into proximal fragment
- Provides rotational and angular stability
- Wires buried beneath skin
Advantage: Wires buried beneath skin, reducing pin site infection risk compared to percutaneous technique.
Complications
Complications
Early Complications
- Rotational most significant
- May require revision fixation
- Prevention better than treatment
- Higher risk with open fractures
- Pin site infection with K-wires
- Deep infection rare with proper technique
- Digital nerve during approach
- Vascular compromise (rare)
- Screw loosening
- K-wire migration
- Plate failure in comminuted fractures
Late Complications
- MOST COMMON complication
- Affects PIP joint primarily
- Results from:
- Prolonged immobilization
- Tendon adhesions
- Capsular contracture
- Prevention: early motion
- Rotational most functionally significant
- Angulation may be tolerated
- May require corrective osteotomy
- Uncommon in phalanges
- Risk factors: comminution, infection, motion at fracture
- Treatment: bone graft + rigid fixation
- After articular fractures
- Risk proportional to articular incongruity
- May need arthrodesis
- Common after dorsal surgery
- Extensor lag or flexion loss
- May need tenolysis
- Common in first year
- Usually improves
Comparison of Complication Risk
- K-wire
- High
- Screw
- N/A
- Plate
- N/A
- K-wire
- Low-Mod
- Screw
- Low
- Plate
- Moderate
- K-wire
- Low
- Screw
- Low
- Plate
- Higher
- K-wire
- Common
- Screw
- Rare
- Plate
- Sometimes
Postoperative Care
Postoperative Care
Week 0-1: Protection Phase
- Wound healing
- Control edema
- Protect fixation
- Splint protection (volar slab with MCP in flexion)
- Hand elevation above heart level
- Ice therapy 20 minutes every 2 hours
- Digital ROM exercises if fixation is rigid (plate/screws)
- K-wire cases: splint immobilization
- Monitor for infection (increased pain, erythema, drainage)
- Dressing change at 2-3 days
- Suture removal at 10-14 days
- Pin site care (K-wires): daily cleaning with chlorhexidine
Week 1-3: Early Motion Phase
- Prevent stiffness
- Maintain reduction
- Progress ROM
- Remove sutures at 10-14 days
- Hand therapy referral
- Active ROM exercises:
- MCP, PIP, DIP flexion/extension
- Tendon gliding exercises
- Place and hold exercises
- Avoid passive stretching initially
- Splint between exercises
- Edema control: compression glove, elevation, retrograde massage
- Continue splint protection
- Active ROM of adjacent joints
- Pin site monitoring
Week 3-6: Progressive Motion Phase
- Increase ROM
- Begin light functional use
- Remove K-wires if used
- Remove K-wires at 3-4 weeks (when fracture sticky)
- Increase frequency of ROM exercises
- Begin passive ROM (gentle)
- Dynamic splinting if stiffness developing:
- Extension turnbuckle for PIP flexion contracture
- Flexion strap for extension lag
- Light functional activities
- Buddy taping for protection
- XR at K-wire removal to confirm alignment maintained
- Check for callus formation
Week 6-12: Strengthening Phase
- Restore grip strength
- Return to function
- Maximize ROM
- Progressive strengthening exercises:
- Putty exercises (soft to firm progression)
- Gripper exercises
- Functional activities
- Sport-specific training
- Work conditioning program
- Continue ROM exercises to plateau
- Desk work: 1-2 weeks (with protection)
- Light manual work: 6-8 weeks
- Heavy manual work: 10-12 weeks
- Contact sports: 10-12 weeks (with protection initially)
Hardware Removal
- Symptomatic hardware (prominence, pain)
- Patient request
- Plate/screw removal: generally only if symptomatic
- K-wires: 3-4 weeks routine
- Screws/plates: after fracture consolidation (12+ weeks) if needed
Red Flags Requiring Review
- Increasing pain after initial improvement
- Loss of reduction on radiographs
- Signs of infection (erythema, purulent drainage, fever)
- Worsening stiffness despite therapy
- Neurovascular compromise
- Pin migration or loosening
Outcomes and Prognosis
Outcomes and Prognosis
Prognostic Factors
- Simple fracture pattern
- Anatomic reduction (especially rotation)
- Early motion achieved
- Young patient
- Single digit involved
- Comminuted fracture
- Residual rotation
- Prolonged immobilization
- Index/long finger (less CMC compensation)
- Multiple digit involvement
- Associated soft tissue injury
Expected Outcomes by Fixation
- 90% good/excellent for stable fractures
- ROM typically 80-90% of contralateral
- Minimal grip strength deficit
- 80-85% good/excellent
- Stiffness main complication
- Slight grip strength reduction
- 85-90% good/excellent
- Best ROM preservation
- Hardware issues may require removal
Return to Activity
- Timeframe
- 1-2 weeks (with splint)
- Timeframe
- 6-8 weeks
- Timeframe
- 10-12 weeks
- Timeframe
- 10-12 weeks
- Timeframe
- 3-6 months
Guidelines, Registries & Global Practice
Guidelines, Registries and Global Practice
Global Epidemiology
Phalangeal and metacarpal fractures are among the commonest skeletal injuries, accounting for approximately 10% of all fractures, with roughly a quarter occurring during sport. [Cotterell & Richard 2014; PMID 25455397] Prospective population data from a single trauma unit reported a hand fracture incidence of 3.7 per 1000 per year in men and 1.3 per 1000 per year in women, with a marked young-male predominance and gender-specific mechanisms (assault and sport in men; falls in older women). [Anakwe et al. 2010; PMID 20709710]
- Figure
- ~10%
- Source population
- Mixed (review)
- Figure
- ~25%
- Source population
- Mixed (review)
- Figure
- 3.7 per 1000 per year
- Source population
- Edinburgh trauma unit
- Figure
- 1.3 per 1000 per year
- Source population
- Edinburgh trauma unit
- Figure
- Young men; second peak in older women
- Source population
- Edinburgh trauma unit
Major Guidance, Side by Side
There is no single high-level international guideline dedicated to phalangeal fractures; practice is driven by hand-surgery society teaching, the AO Foundation principles and consistent themes across narrative reviews and one randomised trial. The areas of genuine consensus and the few areas of variation are summarised below.
- Position
- Stable fixation tailored to pattern (lag screws for long oblique/spiral, plates for transverse/comminuted), preserve soft tissue, enable early motion
- Evidence level
- Expert consensus / biomechanical
- Position
- Most extra-articular fractures with acceptable alignment and no malrotation are treated non-operatively with buddy strapping and early movement
- Evidence level
- Expert consensus
- Position
- Same principles; midlateral plating or screws where unstable; early protected motion
- Evidence level
- Expert consensus
- Position
- Anatomic reduction (rotation least tolerated), stability adequate for early mobilisation; complication rates after fixation remain variable
- Evidence level
- Level V [PMID 37704026, 24486016]
- Position
- Lateral plate-and-screw fixation gave higher total active motion and fewer complications than K-wires in unstable diaphyseal fractures
- Evidence level
- Level II [PMID 30803743]
Registry Evidence
Unlike arthroplasty, phalangeal fractures are not tracked by national joint registries (NJR, AJRR, AOANJRR, SHAR), so high-volume implant-survival data do not exist for this topic. The best comparative evidence is therefore the single randomised controlled trial above plus prospective and retrospective hand-surgery series, rather than registry output. This is an important point to make explicitly in a viva: the evidence base is dominated by Level II–IV studies.
Global Practice Variation
- Resource setting: K-wires are inexpensive, universally available and remain the workhorse in limited-resource settings; plate-and-screw systems and image intensifiers concentrate the cost and are more variably available.
- Specialty delivery: hand trauma is delivered by orthopaedic, plastic or dedicated hand surgeons depending on region, which influences thresholds for operative fixation.
- Rehabilitation access: outcomes hinge on early hand therapy; access to specialist hand therapists varies widely between and within countries and is a key determinant of the stiffness that dominates poor results.
- Consistent worldwide principle: regardless of system, malrotation is never accepted, and the goal is a stable fracture with an early-moving joint.
Mnemonics and Memory Aids
PHALANXPHALANX Fracture Assessment
Hook:Assess the whole PHALANX before deciding treatment!
SCISSORSCISSOR Test for Rotation
Hook:The SCISSOR test catches what others miss!
APEXAPEX Direction by Location
Hook:Know your APEX direction for proper reduction!
Viva Questions
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old carpenter presents with a spiral fracture of the proximal phalanx of his ring finger sustained while using a power tool. There is 20 degrees of apex volar angulation and you suspect rotational malalignment. Describe your assessment and management.”
“Explain the deforming forces acting on proximal phalanx fractures and why the apex of angulation is volar.”
“A patient presents 3 weeks after injury with a stiff PIP joint following a middle phalanx shaft fracture that was treated in a splint. The fracture is uniting. What are the causes of stiffness and how would you manage this?”
MCQ Practice Points
MCQ Practice Points
High-Yield Facts
Q: Why is rotational malalignment the most critical assessment? A: 5° rotation = 1.5cm fingertip overlap - Even minor rotation causes functional scissoring. Unlike angulation, rotation does not remodel and causes permanent impairment. All fingertips must point to the scaphoid tubercle.
Q: What is the typical deformity of a proximal phalanx fracture? A: Apex Volar - The interossei flex the proximal fragment, while the central slip extends the distal fragment. Reduction requires flexing the MCP joint to relax the intrinsics.
Q: When is lag screw fixation indicated? A: Long spiral fractures (greater than 2x bone diameter) - Requires sufficient length for 2-3 screws. Short oblique or transverse fractures require K-wires or plating as screws won't hold.
Q: what is the most common complication of phalangeal fractures? A: PIP Joint Stiffness - Risk increases significantly with immobilization greater than 3 weeks. The goal of fixation is "stable fracture, mobile joint" to allow immediate motion.
Q: Why is the volar approach avoided for phalangeal plating? A: Tendon Adhesions - The flexor tendons (FDS/FDP) are prone to adherence to the plate, causing stiffness. Lateral (preferred) or dorsal approaches are safer.
Q: How must displaced unicondylar fractures be treated? A: ORIF - These are unstable intra-articular fractures. Without fixation, the condyle displaces proximally, causing angular deformity and arthritis.
Common Exam Traps
Accepting small rotational deformity
- WRONG: "5 degrees is minor"
- RIGHT: NO rotation acceptable (5° = 1.5cm overlap)
Using lag screws for short oblique fractures
- WRONG: Screws for all oblique fractures
- RIGHT: Need length at least 2x diameter for screw purchase
Volar approach for plating
- WRONG: Direct access to fracture
- RIGHT: NEVER volar (massive tendon adhesions)
Prolonged immobilization
- WRONG: "Immobilize 6 weeks for healing"
- RIGHT: Maximum 3 weeks if possible, early motion critical
Ignoring deforming forces
- WRONG: Just reduce the fracture
- RIGHT: Must understand apex direction (PP = volar, MP = variable)
At a Glance
- Decision
- Buddy tape + early motion
- Rationale
- Low risk of displacement
- Decision
- Closed reduction or ORIF
- Rationale
- Cannot accept rotation
- Decision
- K-wires or plate
- Rationale
- High intrinsic deforming force
- Decision
- K-wires (cross-pattern)
- Rationale
- Lag screws won't hold
- Decision
- Lag screws
- Rationale
- Ideal screw purchase
- Decision
- Plate +/- bone graft
- Rationale
- Need to span comminution
- Decision
- ORIF with screws
- Rationale
- Prevent angular deformity
- Decision
- ORIF with mini-condylar plate
- Rationale
- Restore articular surface
- Decision
- Irrigation, debridement, stabilization
- Rationale
- Prevent infection
- Decision
- Consider external fixation
- Rationale
- Joint distraction helpful
Exam Cheat Sheet
Exam Day Cheat Sheet
Critical Assessment
- ROTATION - most important (check scissoring)
- All fingertips point to scaphoid tubercle in flexion
- 5 degrees rotation = 1.5cm fingertip overlap
- No rotation is acceptable
Deforming Forces
- PP: apex VOLAR (intrinsics flex proximal fragment)
- MP proximal to FDS: apex volar (central slip)
- MP distal to FDS: apex dorsal (FDS pulls)
- MCP flexion relaxes intrinsics for reduction
Fixation Selection
- Stable: buddy tape + early motion
- Transverse/short oblique: K-wires or plate
- Long spiral: lag screws (2-3 minimum)
- Comminuted: plate to bridge
Complications
- Stiffness - MOST COMMON complication
- Prevention: early motion when stable
- Malunion - rotational most significant
- Adhesions - avoid volar plating
Quick Reference: Key Numbers
- Value
- 10-15°
- Value
- 15-20°
- Value
- NONE (0°)
- Value
- 1.5cm at tip
- Value
- 3 weeks ideal
- Value
- 2 (prefer 3)
- Value
- at least 2x diameter
- Value
- 10-12 weeks
Evidence and Guidelines
Evidence Base
Epidemiology of Hand Fractures
- Prospective single-unit data on 1382 patients (1569 metacarpal and phalangeal fractures) gave a hand fracture incidence of 3.7 per 1000 per year in men and 1.3 per 1000 per year in women, with gender-specific mechanisms
Comprehensive Review - Principles of Phalangeal Fracture Care
- Across phalangeal fracture patterns the guiding principles are anatomic reduction (particularly rotation, the least-tolerated deformity), stable fixation and early postoperative mobilisation; reported complication rates after internal fixation remain variable and represent an unsolved problem
K-Wire vs Plate Fixation (Randomised Controlled Trial)
- RCT of 40 unstable proximal/middle phalangeal diaphyseal fractures: lateral titanium plate-and-screw fixation gave significantly higher total active motion and fewer complications (2 of 20) than percutaneous K-wires (5 of 20); grip strength and patient-reported scores were similar
Early Mobilisation and Treatment Principles
- Review of extra-articular metacarpal and phalangeal fractures emphasises that treatment must restore anatomy while mobilising the digital chain as early as possible in every patient, with regular follow-up to detect secondary displacement
Distal Unicondylar Fractures of the Proximal Phalanx
- Series of 38 distal unicondylar proximal phalanx fractures: 5 of 7 nondisplaced fractures treated by splinting and 4 of 10 displaced fractures fixed with a single K-wire displaced; multiple K-wire or miniscrew fixation gave the best final joint motion
Metacarpal and Phalangeal Fractures in Athletes
- Metacarpal and phalangeal fractures account for about 10% of all fractures and roughly a quarter occur during sport; evolving fixation allows early range of motion and earlier return to play, with stiffness the principal functional threat