Ulnar collateral ligament injury of thumb MCP joint
- Stener lesion: UCL flips over adductor aponeurosis - blocks healing
- Stress test: greater than 30° absolute laxity OR greater than 15° vs contralateral side
- Complete tear with Stener lesion MUST have surgical repair
- Test in extension (assesses proper collateral) AND flexion (accessory collateral)
- “Gamekeeper's (chronic) vs Skier's (acute) - both UCL injuries
- “Always compare to contralateral side for stress testing
- “MRI or ultrasound can identify Stener lesion preoperatively
- “No endpoint on stress test = complete tear
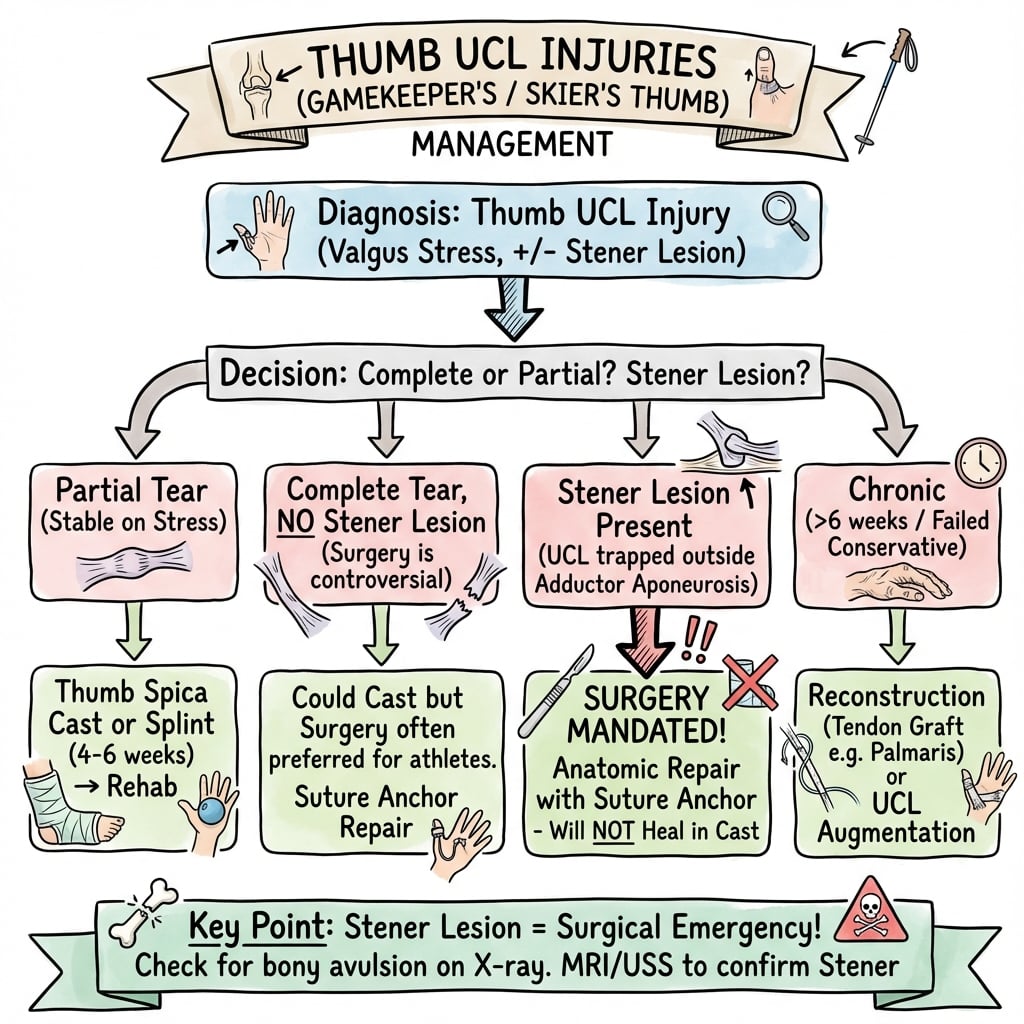
Thumb UCL Injuries (Gamekeeper's/Skier's Thumb)
UCL flips SUPERFICIAL to adductor aponeurosis. Ligament cannot reach its insertion site. Will NEVER heal with conservative treatment. MUST have surgical repair.
Palpable mass at ulnar MCP (rolled-up ligament). Greater than 30° laxity on stress testing. No firm endpoint on valgus stress. MRI or ultrasound confirms displaced UCL.
Overview
Overview
Injury to the ulnar collateral ligament (UCL) of the thumb metacarpophalangeal (MCP) joint is one of the most common ligamentous injuries of the hand. The injury occurs when a valgus (radially directed) force is applied to the thumb, stretching or rupturing the UCL complex. Historically termed "Gamekeeper's thumb" due to its prevalence among Scottish gamekeepers who broke the necks of rabbits (causing chronic UCL attenuation), the acute traumatic variant is now commonly called "Skier's thumb" given its high incidence in skiing injuries from pole strap falls.
The critical clinical concept is the Stener lesion, occurring in approximately 70% of complete UCL tears. In this pathological configuration, the torn UCL displaces to lie superficial to the adductor pollicis aponeurosis, which then interposes between the ligament and its insertion site on the proximal phalanx. This anatomical configuration prevents the ligament from healing to bone, even with prolonged immobilization, making surgical intervention mandatory for complete functional recovery.
Understanding the anatomy, clinical examination, stress testing technique, and recognition of the Stener lesion is essential for orthopaedic examination success and appropriate clinical management.
Anatomy and Biomechanics
Anatomy and Biomechanics
Thumb MCP Joint Anatomy
- Condyloid joint (biaxial)
- Primary motion: flexion-extension
- Secondary: abduction-adduction, rotation
- Less constrained than finger MCP joints
- Origin: Ulnar condyle of metacarpal head
- Insertion: Volar-ulnar base of proximal phalanx
- Two components:
- Proper collateral ligament (PCL): Taut in flexion
- Accessory collateral ligament (ACL): Taut in extension
- Origin
- Dorsal MC head
- Insertion
- Volar PP base
- Taut Position
- Flexion
- Origin
- Volar MC head
- Insertion
- Volar plate
- Taut Position
- Extension
- Origin: Third metacarpal, capitate, trapezoid
- Insertion: Proximal phalanx ulnar sesamoid
- Aponeurosis lies SUPERFICIAL to UCL insertion
- Critical in Stener lesion pathoanatomy
- Attaches to accessory collateral
- Provides additional stability
Mechanism of Injury
- Forced valgus (radial deviation) stress
- Thumb caught in ski pole strap during fall
- Ball-handling sports (football, basketball)
- Fall onto outstretched thumb
- Motor vehicle accidents
- Repetitive valgus stress
- Occupational (originally gamekeepers)
- Gradual ligament attenuation
- Progressive instability
Stener Lesion Mechanics
- Forced valgus stress causes UCL rupture
- Ligament tears from proximal phalanx insertion
- MCP joint subluxates briefly
- As joint reduces, UCL flips over adductor aponeurosis
- Aponeurosis now lies BETWEEN ligament and bone
- Healing impossible without surgical relocation
- Approximately 70% of complete UCL ruptures
- Higher with greater initial displacement
- Cannot be definitively diagnosed clinically
Classification
Classification
Clinical Grading (Heyman Classification)
- Ligament stretched but intact
- Less than 15° laxity
- Firm endpoint on stress testing
- Treatment: Conservative
- Some fibers torn
- 15-30° laxity
- Soft but present endpoint
- Treatment: Usually conservative
- Complete ligament rupture
- Greater than 30° laxity OR greater than 15° vs contralateral
- No firm endpoint
- Treatment: Surgical (especially if Stener)
This classification guides initial treatment decisions.
Clinical Presentation
Clinical Presentation
History
- Fall onto abducted thumb
- Skiing fall with pole strap
- Ball sports (thumb caught during catch)
- Motor vehicle accident
- Manual labor injury
- Pain at ulnar aspect of thumb MCP
- Swelling over thenar region
- Weakness with pinch grip
- Instability sensation with key pinch
- Difficulty with fine motor tasks
Physical Examination
- Swelling at ulnar MCP joint
- Ecchymosis over ulnar thumb
- May see angular deformity in severe cases
- Tenderness at UCL insertion (volar-ulnar PP base)
- Palpable mass at ulnar MCP = Stener lesion sign
- Rolled-up ligament sitting superficial to aponeurosis
- Highly specific but not sensitive
- Usually full ROM (pain-limited)
- Compare to contralateral side
Stress Testing (Critical Examination)
Proper Technique:
- Anesthesia: Local infiltration or digital block if needed
- Stabilize: Hold metacarpal firmly with one hand
- Test in Extension: Valgus stress (assesses accessory collateral)
- Test in 30° Flexion: Valgus stress (assesses proper collateral)
- Evaluate:
- Degree of laxity (in degrees)
- Quality of endpoint (firm vs soft)
- Compare: ALWAYS compare to contralateral thumb
Stress Test Interpretation:
- Interpretation
- Grade I sprain
- Management
- Conservative
- Interpretation
- Partial tear (II)
- Management
- Conservative
- Interpretation
- Complete tear (III)
- Management
- Consider surgery
- Interpretation
- Complete tear (III)
- Management
- Consider surgery
- Interpretation
- Complete tear (III)
- Management
- Likely Stener
Cautions:
- Avoid forceful repeated testing (may convert partial to complete)
- X-ray BEFORE stress testing to exclude fracture
- If avulsion fracture present, stress testing contraindicated
Special Tests
- Key pinch: Thumb to side of index finger
- Compare to contralateral side
- Reduced with UCL insufficiency
- Writing
- Buttoning
- Turning key
- Jar opening
Differential Diagnosis
Several conditions mimic an ulnar-sided thumb injury. The discriminating features below help avoid the common trap of attributing all base-of-thumb pain to a UCL tear.
- 1
- Ulnar MCP tenderness, valgus laxity, weak key pinch; palpable mass if Stener
- 1
- Radial-sided MCP pain and varus laxity; much less common; Stener-like RCL rare
- 1
- Pain at thumb base/CMC, positive grind test, radiographic CMC changes - not MCP
- 1
- Radial wrist/first-dorsal-compartment pain, positive Finkelstein, no MCP laxity
- 1
- Intra-articular fracture of thumb metacarpal base on X-ray; bony, not ligamentous
- 1
- Hyperextension mechanism, volar tenderness, no ulnar valgus laxity
- 1
- Catching/locking at thumb IP/MCP, A1 pulley nodule, no instability
- 1
- Anatomical snuffbox tenderness, axial load pain, distinct from MCP injury
The thumb's radial collateral ligament is the under-recognised counterpart to the UCL and is genuinely examinable:
- Far less common than UCL injury (roughly a 1:4 ratio), caused by a forced ADDuction (ulnar-deviation) force - the mirror of the abduction force that tears the UCL.
- Presents with radial-sided MCP pain/swelling and varus laxity on stress testing, often with volar and ulnar subluxation/rotation of the proximal phalanx (the metacarpal head becomes prominent dorsoradially) and a weak pinch.
- A true Stener-type lesion is rare on the radial side, because the abductor/extensor expansion is broader and less discrete than the adductor aponeurosis - so the displaced-ligament mechanical block that defines the UCL Stener lesion is much less of a feature; RCL tears more often retract or avulse without that interposition.
- Management mirrors the UCL: immobilise partial/stable tears, repair (suture anchor) complete or displaced tears, and reconstruct chronic/irreparable cases. Always stress both sides of the MCP so a radial injury is not missed while you focus on the ulnar side.
Investigations
Investigations
Radiographic Assessment
- PA thumb: Shows bony avulsion if present
- Lateral thumb: Subluxation assessment
- Oblique thumb: Additional fragment visualization
- Some advocate stress radiographs
- Risk of displacing partial tears
- MRI preferred if diagnosis uncertain
- Bony avulsion: Fragment at proximal phalanx base
- Stener lesion sign: Proximally displaced fragment
- Subluxation: Radial deviation of PP on MC
MRI Imaging
- Equivocal clinical examination
- Identify Stener lesion preoperatively
- Assess associated injuries
- Differentiate partial from complete tear
- Low signal on all sequences
- Smooth contour from MC to PP
- Discontinuous UCL
- Ligament displaced proximal and superficial
- "Yo-yo on a string" appearance
- Interposition of adductor aponeurosis visible
- Thickening and increased signal within ligament
- Ligament continuity maintained
Ultrasound
- Dynamic assessment
- Stress testing visualization
- Cost-effective
- No radiation
- Identify displaced ligament
- Can visualize Stener lesion
- Operator-dependent
- Becoming more popular
CT (Limited Role)
- Mainly for complex avulsion fractures
- Surgical planning if ORIF needed
- 3D reconstruction for fragment assessment
Management
Management Algorithm
Non-Operative Treatment
Indications:
- Grade I and II injuries (partial tears)
- Complete tear WITHOUT Stener lesion
- Less than 30° absolute laxity
- Less than 15° difference vs contralateral
- Firm endpoint on stress testing
- Non-displaced avulsion fractures
Protocol:
Acute Phase (0-2 weeks):
- Thumb spica cast or splint
- MCP in 20-30° flexion
- IP joint free
- Elevation and ice
Immobilization Phase (2-6 weeks):
- Thumb spica immobilization total 4-6 weeks
- May convert to removable splint at 4 weeks
- Serial clinical assessment
Rehabilitation Phase (6-12 weeks):
- Gentle ROM exercises
- Progressive strengthening
- Splinting for sport/heavy activities
- Return to full activity 10-12 weeks
Expected Outcomes:
- 90% success with appropriate selection
- Must exclude Stener lesion
- Full strength recovery expected
Non-operative treatment succeeds when Stener lesion is excluded.
Surgical Technique
Surgical Technique: UCL Repair
Preoperative Setup
- Supine on operating table
- Arm on hand table
- Tourniquet on upper arm
- General anesthesia OR
- Regional block (axillary/supraclavicular)
- Local infiltration often added
- 2.0-2.4mm suture anchors (typically 1-2)
- Or equipment for transosseous sutures
- Fine hand instruments
- Loupe magnification (2.5x-3.5x)
Proper setup ensures efficient surgical technique.
Beyond the standard suture-anchor repair above, the modern refinement is suture-tape "internal brace" augmentation - a strong, low-profile non-absorbable tape anchored in the metacarpal head and the proximal phalanx base, spanning the repaired UCL like a check-rein. Its purpose is not to replace the biological repair but to protect it:
- The tape carries valgus load while the native ligament heals, so the construct is immediately more stable.
- This permits an accelerated rehabilitation protocol - earlier protected motion and earlier return to sport - which is why it is popular in athletes (return-to-play rates remain very high).
- It can also augment a reconstruction or a tenuous repair in poor-quality tissue.
Caveats: it adds hardware and cost, over-tensioning the tape can over-constrain and stiffen the MCP, and it does not substitute for correctly relocating a Stener lesion deep to the adductor aponeurosis. The examinable point is the concept of "ligament repair + internal brace = earlier motion," not the brand.
Complications
Complications
Early Complications
- Infection (rare)
- Hematoma
- Wound dehiscence
- Dorsal sensory branches of radial nerve
- Numbness over dorsal thumb
- Usually neuropraxia, recovers
- Suture anchor pullout
- Avulsion fragment refracture
- May need revision
Late Complications
- Most significant complication
- From missed Stener or inadequate repair
- May need reconstruction
- Common after prolonged immobilization
- Hand therapy essential
- Usually resolves with time
- Uncommon with anatomic repair
- More common after chronic instability
- May need arthrodesis
- Pinch strength deficit
- Usually improves over 6-12 months
- May be permanent in chronic cases
- Common in first year
- Usually improves with time
Comparison: Acute vs Chronic Results
- Acute Repair
- 90-95%
- Chronic Reconstruction
- 70-80%
- Acute Repair
- Expected
- Chronic Reconstruction
- Often reduced
- Acute Repair
- Usually full
- Chronic Reconstruction
- May be limited
- Acute Repair
- Low
- Chronic Reconstruction
- Moderate
Postoperative Care
Postoperative Care
Immediate Postoperative Period (Day 0-14)
- Thumb spica splint maintained continuously
- Keep clean and dry
- Elevation above heart level for first 48-72 hours
- Ice packs around splint (avoid getting splint wet)
- First dressing change at 48-72 hours
- Inspect for hematoma, infection
- Redress with clean dressings
- Suture removal at 10-14 days
- Expect moderate pain first 24-48 hours
- Paracetamol 1g four times daily
- Ibuprofen 400mg three times daily (if no contraindications)
- Short course opioids if needed (3-5 days maximum)
- Excessive pain (concern for compartment syndrome - rare)
- Numbness in radial nerve distribution (expected, monitor)
- Signs of infection (increasing pain, fever, drainage)
Phase 1: Protected Immobilization (Week 2-6)
- Continue thumb spica splint full-time
- May convert to removable splint at week 4 (surgeon preference)
- Maintain MCP in 20-30° flexion
- IP joint should remain free - encourage active IP flexion/extension
- Adjacent finger ROM exercises
- Transition to removable thumb spica splint
- Remove only for gentle washing
- NO stress to repair site
- Begin very gentle active ROM (if permitted by surgeon)
- Continue IP joint exercises
- No lifting, gripping, pinching
- Shower with waterproof cover
- Desk work acceptable with splint on
- No driving
Phase 2: Early Mobilization (Week 6-8)
- Remove splint for exercises 3-4 times daily
- Gentle active MCP flexion/extension
- NO passive stretching
- NO valgus stress
- Therapist-supervised if possible
- Thumb opposition to each fingertip
- Gentle fist making (light grip)
- Tabletop slide exercises
- Tendon gliding exercises
- Continue splint between exercise sessions
- Night splinting continues
- Splint for any potentially stressful activities
- Light activities of daily living
- Computer work
- Writing
- Avoid sports, heavy lifting
Phase 3: Strengthening (Week 8-12)
- Gradual increase in grip activities
- Putty exercises (soft → medium → firm)
- Pinch strengthening exercises
- Key pinch, tip pinch, lateral pinch
- Progress resistance as tolerated
- Achieve full active ROM
- MCP flexion 50-60°
- Full extension to neutral or near-neutral
- No extension lag acceptable
- Simulate work/sport-specific activities
- Graded return to daily tasks
- May use taping for support during activities
- Continue night splinting for protection
- Return to most activities of daily living
- May begin light recreational activities
- No contact sports yet
- Gradual return to manual work
Phase 4: Return to Full Activity (Week 12+)
- Pain-free ROM
- Strength at least 80% of contralateral side
- No instability on stress testing
- Patient confidence in stability
- Surgeon clearance
- Gradual return to sport protocol
- May need protective taping or brace initially
- Position-specific training for athletes
- Full clearance usually 3-4 months post-op
- Most patients achieve full recovery by 4-6 months
- Strength may continue improving up to 12 months
- Annual review recommended first year
- Monitor for late instability or arthritis
Rehabilitation Milestones Summary
- Milestones
- Wound healing, suture removal
- Splinting
- Full-time rigid spica
- Milestones
- IP motion, protected healing
- Splinting
- Full-time (may convert to removable)
- Milestones
- Gentle active ROM, light ADLs
- Splinting
- Part-time, night splinting
- Milestones
- Strengthening, functional tasks
- Splinting
- Night only, taping for activities
- Milestones
- Return to sport, full activities
- Splinting
- As needed for sport
Red Flags Requiring Immediate Review
- Sudden increase in pain
- Loss of motion after initial gains
- Recurrent instability sensation
- Signs of infection
- Persistent weakness at 3 months
- Donor site problems (if graft used)
Outcomes and Prognosis
Outcomes and Prognosis
Acute Repair Outcomes
Success Rates:
- Overall success rate: 90-95% with appropriate patient selection
- Return to full activities: 85-90%
- Patient satisfaction: Greater than 90%
Functional Outcomes:
- 1
- 85-95% recovery
- 1
- 90-100% recovery
- 1
- Near-full to full ROM
- 1
- Less than 10° laxity vs contralateral
- 1
- 3-4 months
- 1
- 3-4 months
- 1
- 4-6 months
Key Factors for Success:
- Early recognition and treatment (less than 3 weeks optimal)
- Accurate diagnosis of Stener lesion
- Secure anatomic repair
- Protected rehabilitation protocol
- Patient compliance with restrictions
Chronic Reconstruction Outcomes
- Good to excellent results: 70-80%
- Return to previous level of activity: 60-70%
- Revision surgery rate: 10-15%
- Pinch strength typically 70-85% of contralateral
- May have persistent mild instability
- Slight loss of motion common (10-15° MCP flexion deficit)
- Occasional weather-related discomfort
Comparison: Acute vs Chronic Treatment
- Acute Repair
- 90-95%
- Chronic Reconstruction
- 70-80%
- Acute Repair
- 85-95%
- Chronic Reconstruction
- 70-85%
- Acute Repair
- Full
- Chronic Reconstruction
- Often slight deficit
- Acute Repair
- 3-4 months
- Chronic Reconstruction
- 4-6 months
- Acute Repair
- Less than 5%
- Chronic Reconstruction
- 10-15%
Conservative Treatment Outcomes
- Success rate: 85-90% (partial tears without Stener)
- Full recovery expected with compliant immobilization
- Failure rate: 10-15% (may have missed Stener)
- Initial laxity greater than 25° (even if less than 30°)
- Soft or absent endpoint
- Palpable mass suggesting Stener
- High-demand occupation or sport
Sport-Specific Return
Return to Sport Timeline:
- Typical Return
- 8-12 weeks
- Considerations
- May return with taping
- Typical Return
- 12-16 weeks
- Considerations
- Ensure full strength, consider bracing
- Typical Return
- 12-16 weeks
- Considerations
- Higher reinjury risk, protective equipment
- Typical Return
- 16-20 weeks
- Considerations
- High stress on thumb, gradual progression
Reinjury Risk:
- Overall reinjury rate: 5-10%
- Higher in contact sports (10-15%)
- Reduced with protective taping/bracing
- Most reinjuries occur in first year
Long-Term Outcomes (5+ Years)
- Post-traumatic MCP arthritis: 10-20% at 10 years
- Higher risk factors:
- Intra-articular fracture component
- Chronic instability before treatment
- Delayed diagnosis greater than 6 weeks
- Mild weather-related discomfort: 20-30%
- Cold intolerance: 15-20%
- Rare persistent numbness (radial nerve): 5-10%
- Clinically significant instability: Less than 5% (with proper repair)
- Overall revision rate: Less than 10%
- Most common reason: Persistent instability
- Salvage options: Reconstruction or arthrodesis
Prognostic Factors
- Age under 40 years
- Acute injury (less than 3 weeks)
- Early surgical repair
- Secure anatomic repair
- Compliant rehabilitation
- No articular damage
- Chronic injury (greater than 12 weeks)
- Multiple previous injuries
- Poor tissue quality
- Non-compliance with rehabilitation
- Heavy manual labor or contact sport
- Smoking (impairs healing)
Patient Counseling Points
- Full recovery takes 4-6 months minimum
- May have mild aching in cold weather long-term
- Small area of numbness common (usually improves)
- Excellent stability expected with proper treatment
- Arthritis risk present but low (10-20% long-term)
- May need protective taping for high-risk sports
- Avoid activities stressing valgus force in first year
- Gradual return to full activities essential
- Listen to symptoms during return to sport
Guidelines, Registries & Global Practice
Guidelines, Registries and Global Practice
Global Epidemiology
The thumb UCL is the most frequently injured ligament at the base of the thumb. A 2025 systematic review reported that UCL injuries account for approximately 86% of all base-of-thumb injuries (Assefa 2025, PMID 40741552). Acute "skier's thumb" remains one of the commonest upper-limb injuries in alpine sports, while ball-handling and contact sports (AFL, rugby codes, basketball, American football) generate a year-round burden. The Stener lesion complicates a substantial proportion of complete tears; modern radiographic series put the displaced-fleck (high-grade) subgroup at around 7.5% of all UCL presentations (Daryoush 2025, PMID 39831878).
Guideline and Society Positions (Side-by-Side)
There is no single high-level clinical-practice guideline (CPG) specific to thumb UCL injury; practice is driven by hand-society consensus and systematic-review evidence. The table summarises the prevailing position of major bodies.
- Position on complete tear / Stener
- Surgical repair for complete tear with Stener or gross instability; conservative for partial tears with firm endpoint
- Preferred imaging
- Ultrasound or MRI; plain film first to exclude avulsion
- Evidence basis
- Society consensus + Level I-III reviews
- Position on complete tear / Stener
- Same operative threshold; ultrasound increasingly first-line in hand units
- Preferred imaging
- Ultrasound-led pathway, MRI for equivocal cases
- Evidence basis
- Consensus + meta-analysis
- Position on complete tear / Stener
- Repair complete/displaced tears; reconstruction or arthrodesis for chronic/irreparable
- Preferred imaging
- MRI or high-resolution ultrasound
- Evidence basis
- Consensus + systematic review
- Position on complete tear / Stener
- Acute primary/suture-anchor repair; ORIF for displaced bony avulsion; reconstruction when chronic
- Preferred imaging
- Stress views/CT for bony avulsion
- Evidence basis
- Technique consensus
Registry and High-Level Evidence
Thumb UCL repair is a soft-tissue procedure and is not captured by arthroplasty joint registries (AOANJRR / NJR / AJRR), so registry survivorship data do not exist. The best population-level evidence is therefore from pooled systematic reviews:
- Population
- 616 thumbs, 24 studies
- Headline result
- Stable thumb: primary repair 95%, suture-anchor 95%, reconstruction 81%
- Population
- 311 athletes
- Headline result
- Return-to-play 98.1%; complication rate 10.3%
- Population
- 593 injuries, 17 studies
- Headline result
- Ultrasound for Stener: sensitivity 0.96, specificity 0.90
Practice Variation
International practice varies chiefly in first-line imaging (ultrasound-led in many UK/European hand units versus MRI in many North American centres) and in fixation choice (transition from transosseous sutures to suture anchors, and now suture-tape internal-brace augmentation enabling earlier motion). The threshold for surgery is more consistent: complete tear with a Stener lesion, gross instability, no firm endpoint, or a displaced bony avulsion.
Mnemonics and Memory Aids
STENERSTENER for Lesion Features
Hook:The STENER lesion STands ENtirely in the way of healing!
STRESSUCL Stress Test Protocol
Hook:STRESS test: compare to other Side!
GAMESGAMES for Gamekeeper's
Hook:GAMES: Scottish gamekeepers played 'games' with rabbit necks!
Viva Scenarios
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old female presents after falling while skiing. She has pain and swelling at the base of her thumb on the ulnar side. Describe your assessment and management.”
“Explain the anatomy of the Stener lesion and why it prevents healing.”
“A patient presents 3 months after a thumb injury with persistent instability and weak pinch. What are your options?”
MCQ Practice Points
MCQ Practice Points
High-Yield Exam Facts
Q: What is the Stener lesion and why does it mandate surgery? A: UCL displaced superficial to adductor aponeurosis - Occurs in ~70% of complete tears. The aponeurosis creates a mechanical block preventing ligament-to-bone contact, making healing impossible without surgical reduction.
Q: What are the stress test thresholds for complete UCL tear? A: Greater than 30° absolute laxity OR greater than 15° difference - Must test in BOTH extension (accessory collateral) AND flexion (proper collateral). No firm endpoint is the most specific sign.
Q: What is the difference between Gamekeeper's and Skier's thumb? A: Mechanism and Chronicity - Gamekeeper's is chronic attrition (historic rabbit neck breaking), Skier's is acute trauma (pole strap). Both affect the UCL of the thumb MCP.
Q: What are the absolute indications for UCL surgery? A: Stener lesion, greater than 30° laxity, no endpoint, displaced avulsion (greater than 2mm) - Any evidence of complete tear or Stener lesion requires repair as these do not heal with immobilization.
Q: How does timing affect UCL treatment options? A: Acute (less than 3 weeks) = Repair; Chronic (greater than 6 weeks) = Reconstruction - Primary repair success drops significantly after 3-4 weeks due to tissue retraction. Chronic cases require tendon graft.
Q: Which UCL component is tight in flexion? A: Proper Collateral Ligament - Taut in flexion (test at 30°). Accessory collateral is taut in extension. Stener lesion occurs when UCL flips superficial to adductor aponeurosis.
- Gamekeeper's thumb = chronic (repetitive injury from rabbit neck breaking)
- Skier's thumb = acute (traumatic fall with pole strap)
- Both refer to same anatomic injury (UCL of thumb MCP)
- UCL inserts on volar-ulnar base of proximal phalanx
- Proper collateral: dorsal origin, taut in flexion
- Accessory collateral: volar origin, taut in extension
- Adductor aponeurosis runs superficial to UCL insertion
- Acute repair: less than 3 weeks (best results)
- Subacute: 3-6 weeks (repair still possible)
- Chronic: greater than 6 weeks (reconstruction usually needed)
- Conservative: thumb spica 4-6 weeks
- Return to sport: 12-16 weeks post-op
- Acute repair success: 90-95%
- Chronic reconstruction success: 70-80%
- Conservative treatment (partial tears): 85-90%
- Pinch strength recovery: 85-95% after acute repair
- Long-term arthritis risk: 10-20% at 10 years
- RCL injury (radial collateral) - much less common than UCL
- IP joint instability - different entity
- De Quervain's tenosynovitis - radial wrist pain, not MCP
- CMC joint arthritis - base of thumb, not MCP
- Trigger thumb - different pathology
- X-ray to exclude bony avulsion (mandatory before stress testing)
- MRI: 100% sensitivity for Stener lesion
- Ultrasound: dynamic assessment possible, operator-dependent
- Stress radiographs controversial (risk converting partial to complete)
- Approach: chevron or curvilinear incision over ulnar MCP
- Must protect dorsal sensory branches of radial nerve
- Incise adductor aponeurosis to access UCL
- Fixation: suture anchors (2.0-2.4mm) most common
- Alternative: transosseous sutures through bone tunnels
- Graft for reconstruction: palmaris longus first choice
- Most common: temporary numbness (radial nerve branches)
- Most significant: chronic instability (from missed Stener)
- Late complication: post-traumatic arthritis (10-20%)
- Surgical: nerve injury, infection, anchor pullout
Common Exam Scenarios
Scenario 1: Acute Injury with Stener
- Young skier, fall with pole strap
- Palpable mass, greater than 30° laxity, no endpoint
- Management: Surgical repair with suture anchors
- Key teaching point: Stener lesion cannot heal conservatively
Scenario 2: Partial Tear vs Complete
- Patient with 25° laxity, 10° vs contralateral, firm endpoint
- Management: Conservative with thumb spica 4-6 weeks
- Key teaching point: Firm endpoint suggests partial tear
Scenario 3: Chronic Presentation
- 3-month history, persistent instability, weak pinch
- Management: Ligament reconstruction with tendon graft
- Key teaching point: Greater than 6 weeks = primary repair usually not possible
Scenario 4: Bony Avulsion
- X-ray shows 3mm displaced avulsion fragment
- Management: ORIF with mini-screw or K-wire
- Key teaching point: Greater than 2mm displacement = operative indication
At a Glance
- Decision
- Thumb spica 4-6 weeks
- Rationale
- Heals with immobilization
- Decision
- Consider conservative vs surgery
- Rationale
- May heal if stable
- Decision
- Surgical repair
- Rationale
- Cannot heal - blocked by aponeurosis
- Decision
- Likely surgical
- Rationale
- High suspicion for complete tear
- Decision
- Likely surgical
- Rationale
- Even if less than 30° absolute
- Decision
- Depends on displacement
- Rationale
- Fix if displaced greater than 2mm
- Decision
- Ligament reconstruction
- Rationale
- Primary repair often not possible
- Decision
- ORIF + ligament repair
- Rationale
- Address both components
Exam Cheat Sheet
Exam Day Cheat Sheet
Terminology
- Gamekeeper's thumb = chronic (repetitive attrition)
- Skier's thumb = acute (traumatic)
- Both = UCL injury of thumb MCP joint
- Stener lesion = UCL superficial to adductor aponeurosis
Anatomy
- Proper UCL: taut in flexion
- Accessory UCL: taut in extension
- Test BOTH positions for complete assessment
- Adductor aponeurosis lies superficial to UCL insertion
Stress Testing
- Greater than 30 degrees absolute laxity = complete tear
- Greater than 15 degrees vs contralateral = complete tear
- No firm endpoint = complete tear
- ALWAYS compare to other side
Treatment
- Partial tear: thumb spica 4-6 weeks
- Complete with Stener: surgical repair mandatory
- Acute repair: suture anchors to proximal phalanx
- Chronic (over 6 weeks): ligament reconstruction
Outcomes
- Acute repair: 90-95% success
- Chronic reconstruction: 70-80% success
- Early treatment is key
- Missed Stener = poor outcome
Quick Reference: Key Numbers
- Value
- ~70% of complete tears
- Value
- greater than 30°
- Value
- greater than 15°
- Value
- 4-6 weeks
- Value
- 90-95%
- Value
- 70-80%
- Value
- 10-12 weeks
Stress Test Algorithm
Stress Test in Extension AND Flexion
Compare to Contralateral Side
- Complete tear suspected
- MRI for Stener lesion
- Surgical repair likely needed
- Partial tear likely
- Conservative treatment
- Thumb spica 4-6 weeks
Evidence and Guidelines
Evidence Base
The Stener Lesion - Pathoanatomy and Defining Concept
- The Stener lesion, first described by Bertil Stener in 1962, is a displaced UCL tear in which the adductor pollicis aponeurosis becomes interposed between the retracted ligament and its insertion, mechanically preventing natural healing
- Recognition mandates surgical repair or reconstruction; the same interposition mechanism (Stener-like lesions) can occur at other hand, knee and foot ligaments
The Displaced Fleck Sign - Plain-Film Predictor of Stener Lesion
- In 228 patients, a 'displaced fleck sign' (avulsion fragment from the ulnar proximal phalanx base displaced proximal to the MCP joint line) was present in 7.5% with excellent interobserver reliability (kappa 0.94)
- The sign had a positive predictive value of 100% for a Grade III rupture and 94.1% for a Stener lesion - all positive cases were grossly unstable with no endpoint
Ultrasound Diagnostic Accuracy - Meta-analysis
- Bivariate meta-analysis of 17 studies (593 UCL injuries): for the Stener lesion, ultrasound pooled sensitivity 0.96 (95% CI 0.89-0.99) and specificity 0.90 (95% CI 0.81-0.94), AUC 0.98
- For complete ruptures without a Stener lesion, sensitivity 0.82 and specificity 0.94
Surgical Technique and Timing - Meta-analysis (614 patients)
- 24 studies, 616 thumbs (primary repair 146, suture-anchor repair 371, reconstruction 99); the commonest surgical indication was lack of a firm endpoint on stress testing
- Stable thumbs: primary repair 95%, suture-anchor repair 95%, reconstruction 81%; return to unrestricted activity 96% / 93% / 84% respectively, with no clinically meaningful difference in pain, grip, pinch or QuickDASH
Chronic UCL Injury - Surgical Management Review
- Systematic review of 11 studies (245 thumbs) with chronic UCL injury: direct repair, free tendon-graft reconstruction and arthrodesis all gave favourable patient-reported outcomes
- Direct repair can be performed safely beyond 2 months from injury; arthrodesis is reserved for heavy manual labourers or established osteoarthrosis
Return to Play After Surgical Repair in Athletes
- Systematic review of 311 athletes: aggregate return-to-play rate 98.1% with no measurable detriment to post-injury performance and a 10.3% complication rate
- Technique has trended toward suture anchors and suture-tape (internal brace) augmentation, permitting earlier motion protocols
Functional Outcomes Across Diverse Populations - Systematic Review
- UCL injuries account for approximately 86% of all injuries at the base of the thumb; 12 studies (335 patients, follow-up 6 months to 15 years) confirmed surgery as the gold standard for complete tears
- Suture-anchor repair, tendon-graft reconstruction and internal-brace augmentation consistently restored strength, reduced pain and gave high satisfaction; athlete return-to-sport reached 98.1%, often within 5-8 weeks