Comminuted Intra-Articular | Thumb MC Base | 3+ Fragments | Worse Prognosis
- Rolando = COMMINUTED (3+ fragments) vs Bennett = 2-part - classic exam distinction
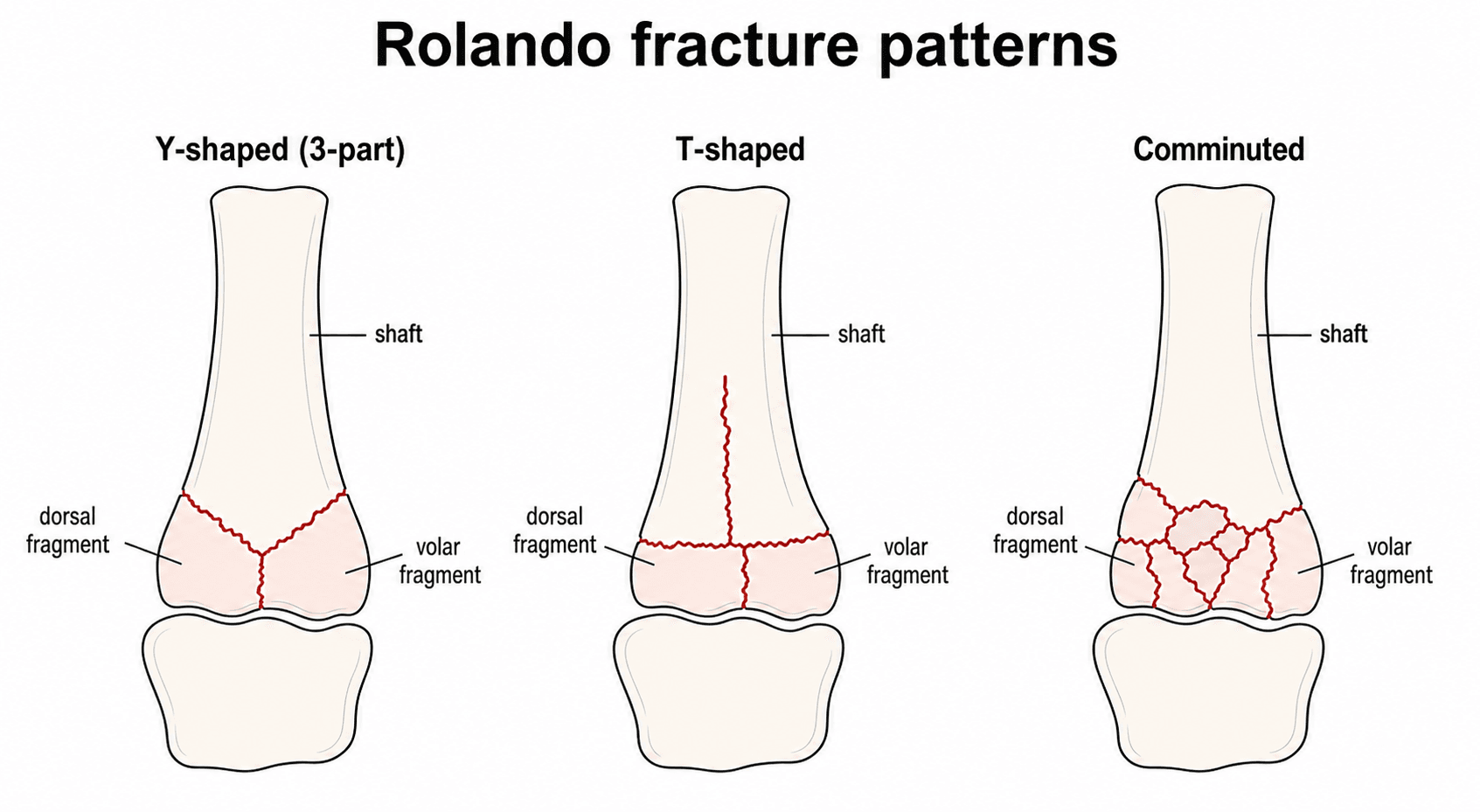
- Y-shaped or T-shaped pattern with dorsal and volar fragments
- WORSE prognosis than Bennett's due to greater articular cartilage damage
- Treatment depends on fragment size: ORIF for large, external fixation for small
- “Bennett = 2-part (Binary), Rolando = 3+ parts (comminuted) - know this cold
- “CT scan ESSENTIAL for surgical planning - count fragments, assess impaction
- “High arthritis rate (40-50%) even with anatomic reduction
- “CMC arthrodesis is the ultimate salvage procedure for post-traumatic arthritis
Rolando's Fractures
TWO-PART fracture-subluxation. Volar-ulnar fragment stays (AOL intact). Shaft subluxates dorsally (APL pull). Generally GOOD prognosis if reduced.
COMMINUTED fracture (3+ fragments). Y-shaped or T-shaped pattern. More articular damage and impaction. WORSE prognosis despite treatment.
Overview and Epidemiology
Overview
Rolando's fracture, first described by Silvio Rolando in 1910, is a comminuted intra-articular fracture of the first metacarpal base involving the carpometacarpal (CMC) joint. Unlike the two-part Bennett's fracture, Rolando's fracture involves three or more fragments and typically demonstrates a Y-shaped or T-shaped fracture pattern. This comminuted nature results in greater articular surface disruption and a higher incidence of post-traumatic arthritis despite optimal treatment.
The injury represents approximately 15-20% of thumb metacarpal base fractures and occurs through a similar mechanism to Bennett's fracture - axial load applied to a partially flexed thumb. The comminuted pattern makes surgical reconstruction challenging, often requiring ORIF with miniature plates and screws, external fixation with ligamentotaxis, or a combination of techniques. Even with anatomic reduction, the prognosis remains guarded due to the cartilage damage sustained at the time of injury.
Understanding the distinction between Bennett's and Rolando's fractures is essential for orthopaedic examination success, as this represents a classic comparison question testing knowledge of thumb base injury patterns.
Anatomy and Biomechanics
Anatomy and Biomechanics
Thumb CMC Joint Anatomy
The anatomy is identical to that described for Bennett's fractures, but the understanding of articular loading is crucial for Rolando's:
Joint Characteristics:
- Saddle-shaped (biconcave-biconvex) articulation
- Allows flexion-extension, abduction-adduction, opposition
- High functional demands with pinch and grip
- Articular cartilage approximately 1-2mm thick
- 40% of hand function depends on thumb
Ligamentous Stabilizers:
- Role in Rolando's
- Often disrupted with volar fragment
- Role in Rolando's
- May be attached to dorsal fragment
- Role in Rolando's
- Contributes to instability
- Role in Rolando's
- Usually intact
Vascular Supply:
- Princeps pollicis artery (from radial artery)
- First dorsal metacarpal artery
- Both at risk during surgical approach
Fracture Mechanics
- High-energy axial load on partially flexed thumb
- Greater force than Bennett's (higher energy injury)
- Punching, falls, sporting injuries, MVA
- Force exceeds articular tolerance causing comminution
- Volar-ulnar fragment (like Bennett's)
- Dorsal-radial fragment
- Metacarpal shaft (may subluxate)
- Horizontal articular split
- Vertical fracture into shaft
- Similar treatment principles
- Multiple small articular fragments
- Central impaction common
- Most challenging pattern
Deforming Forces (Same as Bennett's)
- Inserts on dorsal base of MC1
- Pulls shaft proximally, radially, and dorsally
- Major deforming force
- Pulls shaft ulnarly
- Contributes to shortening
- Extension and radial deviation force
Classification Systems
Classification
Traditional Rolando Classification
Type 1: Y-Shaped (Three-Part)
- Most common Rolando pattern
- Volar fragment, dorsal fragment, shaft
- Amenable to ORIF if fragments adequate size
Type 2: T-Shaped
- Transverse articular component
- Vertical shaft component
- Similar fixation principles
Type 3: Comminuted
- Multiple small fragments
- Central impaction often present
- May require external fixation
The Y-shaped pattern is most common and offers the best opportunity for anatomic reconstruction.
Clinical Presentation
Clinical Presentation
History
- Higher energy than typical Bennett's
- Axial load with metacarpal impact on trapezium
- Punching injury (often with missed punch)
- Fall onto extended thumb
- Sporting injuries (skiing, contact sports)
- Motor vehicle accidents
- Severe pain at thumb base
- Significant swelling
- Inability to use thumb
- Obvious deformity may be present
- May report "crunching" at time of injury
Physical Examination
- Marked swelling at thenar eminence
- Ecchymosis extending to palm
- Thumb appears shortened
- Possible angular deformity
- Skin integrity assessment (open fracture?)
- Exquisite tenderness at CMC joint
- Crepitus with gentle manipulation
- Assess for associated injuries
- Digital sensation (radial and ulnar thumb)
- Capillary refill
- Radial artery palpation at snuffbox
- Other metacarpal fractures
- Carpal bone injuries
- Ligamentous injuries
Differentiating Features from Bennett's
- Bennett's
- Lower
- Rolando's
- Higher
- Bennett's
- Moderate
- Rolando's
- Severe
- Bennett's
- Minimal
- Rolando's
- Marked
- Bennett's
- Subtle
- Rolando's
- Often obvious
- Bennett's
- 2 fragments
- Rolando's
- 3+ fragments
Differential Diagnosis of the Painful, Swollen Thumb Base
- Key Distinguishing Feature
- Comminuted intra-articular base fracture, 3+ fragments, Y/T pattern with articular impaction
- Confirming Investigation
- PA/lateral/Roberts XR; CT to count fragments
- Key Distinguishing Feature
- Two-part intra-articular fracture; volar-ulnar fragment retained, shaft subluxates dorsally
- Confirming Investigation
- XR (true lateral shows subluxation)
- Key Distinguishing Feature
- Transverse/oblique fracture that spares the CMC joint
- Confirming Investigation
- XR - fracture line proximal but extra-articular
- Key Distinguishing Feature
- Tenderness over trapezium, pain on axial thumb load; base of MC1 intact
- Confirming Investigation
- Roberts/Bett views; CT for occult fracture
- Key Distinguishing Feature
- Gross instability without fracture fragment; AOL/dorsoradial ligament rupture
- Confirming Investigation
- Stress XR; little or no bony fragment
- Key Distinguishing Feature
- Older patient, chronic symptoms, positive grind test, joint-space narrowing not acute fracture
- Confirming Investigation
- XR shows degenerative change, not acute fragments
- Key Distinguishing Feature
- Anatomical snuffbox tenderness, pain on axial thumb load referred radially
- Confirming Investigation
- Scaphoid-series XR; MRI/CT if occult
Investigations
Investigations
Radiographic Assessment
- PA View: Shows Y or T pattern
- True Lateral: Assesses subluxation
- Roberts View: Hyperpronated thumb AP
- Oblique Views: Additional fragment detail
- Multiple fracture lines through articular surface
- Y-shaped or T-shaped configuration
- Central impaction may be visible
- Metacarpal shaft shortening
- CMC joint widening or subluxation
CT Imaging (Essential for Surgical Planning)
- All Rolando's fractures being considered for surgery
- Assessment of fragment number and size
- Evaluation of articular impaction
- 3D reconstruction for surgical planning
- Number of fragments
- Size of each fragment
- Degree of articular impaction
- Metaphyseal bone loss
- Fragment displacement
- Visualize fracture pattern
- Plan surgical approach
- Assess fragment orientation
- Guide implant selection
MRI (Rarely Indicated)
- Associated ligament injury assessment
- Not routine for acute fracture
- May help assess chronic instability
Imaging Atlas


Management Algorithm

Management
Treatment Goals
- Anatomic articular reduction when possible
- Stable fixation allowing early motion
- Restore thumb length and alignment
- Preserve CMC joint motion
- Minimize post-traumatic arthritis
Non-Operative Treatment
- Non-displaced or minimally displaced
- Elderly, low-demand patients
- Severe comorbidities precluding surgery
- Patient preference after informed consent
- Closed reduction under fluoroscopy
- Thumb spica cast/splint
- Serial radiographs weekly for 3 weeks
- Total immobilization 6 weeks
- High rate of displacement
- Difficult to maintain reduction
- Poor outcomes with articular step
- Most require surgical intervention
Non-operative treatment is rarely successful for true Rolando's fractures due to the comminuted pattern.
Surgical Technique
Surgical Technique
ORIF with Mini-Plate and Screws
Best For: Y-shaped or T-shaped with adequate fragment size
- Volar-radial or dorsal exposure (based on fragment location)
- Identify and protect neurovascular structures
- Reduce articular fragments under direct visualization
- Provisional K-wire fixation to hold reduction
- Apply mini-plate (T-plate, L-plate, or straight)
- Lag screws for articular fragments if possible
- Confirm reduction fluoroscopically
- 2.0mm or 2.4mm mini-fragment plates
- 1.5mm or 2.0mm screws
- Combination plate and K-wires
Anatomic articular reduction is the primary goal. Use provisional K-wires to hold reduction before definitive plating. Confirm reduction with intraoperative fluoroscopy in multiple planes.
Complications
Complications
Early Complications
- Most significant early complication
- Articular step leads to arthritis
- May require revision surgery
- Pin site infection (5-10% with ex-fix)
- Deep infection rare with ORIF
- Treat early, consider hardware removal
- Small screws may strip
- K-wires may migrate
- Plate loosening possible
- Common without stable fixation
- Close radiographic follow-up essential
- May need revision surgery
Late Complications
- Most significant long-term complication
- 40-50% incidence (higher than Bennett's)
- Occurs even with anatomic reduction
- Due to cartilage damage at injury
- May require CMC arthrodesis
- Common, especially with prolonged immobilization
- May limit opposition and grip
- Hand therapy essential
- May need capsular release
- From ligament damage
- May contribute to arthritis
- Ligament reconstruction rarely successful
- Results from inadequate reduction
- Altered thumb mechanics
- Accelerates degenerative change
- Reduced pinch strength
- Reduced grip strength
- Usually improves over 12 months
- May be permanent
Comparison with Bennett's Complications
- Bennett's
- 20-30%
- Rolando's
- 40-50%
- Bennett's
- Common
- Rolando's
- More common
- Bennett's
- Moderate
- Rolando's
- Higher
- Bennett's
- Rare
- Rolando's
- More common
Postoperative Care
Postoperative Care
Timeline
- Timeframe
- Weeks 0-2
- Focus
- Strict immobilization, edema control
- Timeframe
- Weeks 2-6
- Focus
- Gentle ROM if stable fixation
- Timeframe
- Weeks 6-12
- Focus
- Progressive strengthening
- Timeframe
- 12+ weeks
- Focus
- Full activity as tolerated
Immobilization Protocol
- Thumb spica splint initially
- Convert to removable splint at 2-4 weeks (if stable fixation)
- External fixator typically remains 6 weeks
- K-wire removal at 4-6 weeks
- Daily cleaning with normal saline
- Monitor for infection signs
- No submersion in water
- Patient education on warning signs
Proper immobilization protects the reduction while allowing soft tissue healing.
Outcomes and Prognosis
Outcomes and Prognosis
Prognostic Factors
- Y-shaped pattern (not comminuted)
- Anatomic reduction achieved
- Large fragments amenable to fixation
- Young patient
- Early surgical treatment
- Compliant with rehabilitation
- Highly comminuted pattern
- Central articular impaction
- Small multiple fragments
- Cartilage damage visible at surgery
- Delayed treatment
- Open fracture
- Associated soft tissue injury
Expected Outcomes
- 60-70% good/excellent results
- Anatomic reduction critical
- Early arthritis in 30-40%
- 40-50% satisfactory results
- Expect some articular incongruity
- Higher fusion rate ultimately
Functional Outcomes
- 70-80% of contralateral at 1 year
- May continue to improve to 2 years
- Rarely returns to 100%
- 60-75% of contralateral
- More affected than grip
- Impacts fine motor tasks
- Variable loss of motion
- Opposition usually preserved
- May lose terminal extension/flexion
Long-Term Follow-Up
- Annual radiographs for 5 years
- Monitor for arthritis progression
- Assess functional limitations
- Consider salvage procedure timing
- Symptomatic post-traumatic arthritis
- Failed conservative measures
- Limiting function and quality of life
- CMC arthrodesis (most common)
- Trapezium excision arthroplasty
- Total joint arthroplasty (limited role)
Guidelines, Registries & Global Practice
Guidelines, Registries & Global Practice
Thumb metacarpal base fractures are uncommon but functionally important. Metacarpal and phalangeal fractures together account for a large share of all hand fractures, yet the thumb is involved in only a small minority of tubular-bone hand fractures in large epidemiological series (Stanton, Dias and Burke reviewed 701 tubular-bone hand fractures and found the thumb was rarely involved, with intra-articular base fractures being almost universally displaced). Rolando fractures are the comminuted, three-or-more-fragment subset of intra-articular thumb base fractures and are the least common but most difficult of the recognised patterns.
Global Epidemiology
- Evidence
- Thumb rarely involved; only 10% of intra-articular hand fractures completely undisplaced
- Source
- Stanton et al., 701 fractures
- Evidence
- CMC fracture-dislocations are the commonest thumb injury in high-energy crashes (e.g. motorcycle)
- Source
- Alexander et al., trauma series
- Evidence
- Least common but most comminuted intra-articular base pattern
- Source
- Younis et al. review
- Evidence
- Young males predominate after axial-load/punch and fall mechanisms
- Source
- Pooled series
Guideline & Consensus Positions (Side by Side)
No single national society publishes a Rolando-specific guideline; recommendations are drawn from AO Foundation principles, society reviews, and trauma standards. The recommendations converge internationally.
- Position on intra-articular thumb base fractures
- Articular step greater than 1mm warrants reduction; stable fixation to allow early motion; lag-screw/plate for large fragments, bridging/external fixation for comminution
- Evidence level
- Expert consensus / principle-based
- Position on intra-articular thumb base fractures
- Displaced intra-articular hand fractures should be referred to a hand/specialist service; CT where surgical planning needed
- Evidence level
- Standard of care (consensus)
- Position on intra-articular thumb base fractures
- No dedicated guideline; supports anatomic reduction of displaced intra-articular fractures and early therapy referral
- Evidence level
- Consensus / expert opinion
- Position on intra-articular thumb base fractures
- Surgery for displaced patterns; ligamentotaxis-based fixation for comminution; counsel on arthritis risk
- Evidence level
- Level IV-V evidence
Registry & Comparative Evidence
There is no dedicated joint registry for thumb-base fractures (registries cover arthroplasty, not fracture fixation). The strongest comparative evidence is therefore from cohort series:
- Reduction quality, not implant choice, drives outcome. In Bennett fractures, ORIF and closed transarticular pinning gave equivalent clinical and radiographic results at a mean 7-year follow-up (Lutz et al.) — the principle generalises to Rolando fixation selection.
- Ligamentotaxis works for comminution. Dynamic external fixation restored joint space and motion in small Rolando series (El-Sharkawy et al.).
- Salvage is reliable. Trapeziometacarpal arthrodesis achieves ~96% fusion with improved pinch/grip in the post-traumatic setting (Talsania et al.).
Practice Variation
- High-resource settings: routine CT/3D planning, locking mini-fragment systems, and arthroscopic-assisted reduction in selected centres.
- Limited-resource settings: closed reduction with percutaneous K-wire or simple external fixation predominates; outcomes remain acceptable where length and alignment are restored.
- Threshold for surgery is broadly consistent worldwide (articular step greater than 1-2mm, instability, or displacement), reflecting shared AO-derived principles rather than divergent national policy.
Mnemonics and Memory Aids
ROLANDOROLANDO for Fracture Features
Hook:ROLANDO = multiple pieces Rolling Around in the joint!
Y vs BY vs B for Pattern
Hook:Y has 3 branches (comminuted), B has 2 bumps (2-part)
COMMINUTEDCOMMINUTED Treatment
Hook:When it's COMMINUTED, you need to think CREATIVELY!
Viva Questions
Viva Scenarios
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old male punches a wall and presents with severe thumb base pain. X-rays show a Y-shaped fracture of the first metacarpal base with 3mm articular step. How do you differentiate this from Bennett's fracture and what is your management?”
“Describe the surgical options for a highly comminuted Rolando's fracture where the fragments are too small to fix with screws.”
“A patient returns 18 months after ORIF of a Rolando's fracture with progressive thumb pain, stiffness, and weakness. X-rays show joint space narrowing. What are your options?”
MCQ Practice Points
MCQ Practice Points
Q: What is the key distinguishing feature between a Bennett's fracture and a Rolando's fracture?
A: Number of fragments - Bennett's is a two-part fracture-subluxation, while Rolando's is a comminuted fracture with 3 or more fragments. Both are intra-articular thumb metacarpal base fractures, but Rolando's has a worse prognosis due to greater articular damage.
Q: What is the typical fracture pattern seen in a Rolando's fracture on radiograph?
A: Y-shaped or T-shaped pattern with three main fragments: a volar fragment, a dorsal fragment, and the metacarpal shaft. Central articular impaction may also be present. The Y-shaped pattern is most common and offers the best opportunity for anatomic reconstruction.
Q: What is the most important imaging study for surgical planning in Rolando's fracture?
A: CT scan with 3D reconstruction is essential for surgical planning. It allows accurate assessment of fragment number, fragment size, degree of articular impaction, and helps guide fixation strategy. Plain radiographs are insufficient for surgical planning.
Q: A patient has a highly comminuted Rolando's fracture with multiple small articular fragments. What is the preferred treatment?
A: External fixation with ligamentotaxis is preferred when fragments are too small for screw fixation. Pins are placed in MC1 shaft and trapezium/MC2, then distraction is applied to restore length and achieve indirect reduction through ligamentotaxis. Limited percutaneous K-wires may supplement.
Q: What is the expected arthritis rate following a Rolando's fracture, even with anatomic reduction?
A: 40-50% develop post-traumatic arthritis (compared to 20-30% for Bennett's fractures). This higher rate occurs because the cartilage damage at the time of injury cannot be reversed, even with perfect reduction. Patients should be counseled about this expected outcome.
Q: What is the gold standard salvage procedure for symptomatic post-traumatic arthritis following a Rolando's fracture?
A: CMC arthrodesis (fusion) is the gold standard salvage, particularly for young, active patients. The thumb is fused in functional position: 40° palmar abduction, 20° radial abduction, and 15° pronation. This provides reliable pain relief with acceptable functional outcome.
At a Glance
Rolando's fracture is a comminuted intra-articular fracture of the thumb metacarpal base with 3+ fragments (vs Bennett's 2-part). Typically Y-shaped or T-shaped with dorsal and volar fragments and central articular impaction. Worse prognosis than Bennett's due to greater articular damage - arthritis rate 40-50% even with anatomic reduction. CT scan is essential for surgical planning. Treatment depends on fragment size: ORIF with plate/screws for large reconstructable fragments; external fixation with ligamentotaxis for highly comminuted injuries. CMC arthrodesis is the salvage procedure for post-traumatic arthritis.
- Decision
- ORIF with screws/plate
- Rationale
- Reducible fragments allow stable fixation
- Decision
- Plate fixation preferred
- Rationale
- Need stable construct for articular reduction
- Decision
- External fixation with ligamentotaxis
- Rationale
- Cannot fix each fragment individually
- Decision
- Bone graft augmentation
- Rationale
- Fill void after fragment elevation
- Decision
- CMC arthrodesis
- Rationale
- Salvage procedure for symptomatic arthritis
- Decision
- Conservative or early fusion
- Rationale
- Balance surgical risk vs benefit
- Decision
- Elevate, graft + K-wires
- Rationale
- Restore articular congruity
- Decision
- Extended plate fixation
- Rationale
- May need longer plate for length
Exam Cheat Sheet
Exam Day Cheat Sheet
Definition
- COMMINUTED intra-articular fracture of thumb MC base
- 3 or more fragments (vs Bennett's = 2 parts)
- Y-shaped or T-shaped pattern typically
- Described by Silvio Rolando in 1910
Key Differences from Bennetts
- Bennett = 2-part, Rolando = comminuted (3+)
- Higher energy injury mechanism
- More articular cartilage damage
- Worse prognosis (40-50% vs 20-30% arthritis)
Imaging
- XR: Y-shaped or T-shaped pattern
- CT essential for surgical planning
- Count fragments, assess impaction
- 3D reconstruction helpful
Treatment Options
- Y-shaped (large fragments): ORIF with plate/screws
- Comminuted (small fragments): External fixation
- Combined approach for complex patterns
- K-wires for intermediate patterns
Surgical Approach
- Wagner (volar-radial) for volar fragments
- Dorsal for dorsal fragments
- Mini-plates: 2.0mm or 2.4mm
- External fixator: MC1 to trapezium/MC2
Outcomes
- Y-shaped: 60-70% good/excellent
- Comminuted: 40-50% satisfactory
- Arthritis rate: 40-50%
- Salvage: CMC arthrodesis
Quick Reference: Key Numbers
- Value
- 15-20%
- Value
- 3 (vs 2 for Bennett's)
- Value
- 40-50%
- Value
- 60-70%
- Value
- 70-80%
- Value
- 6 weeks
- Value
- 12-16 weeks
Bennett's vs Rolando's Summary
- Bennett's
- 2
- Rolando's
- 3+
- Bennett's
- Volar-ulnar + shaft
- Rolando's
- Y or T-shaped
- Bennett's
- Lower
- Rolando's
- Higher
- Bennett's
- K-wires usually
- Rolando's
- Plate/Ex-fix often
- Bennett's
- 20-30%
- Rolando's
- 40-50%
- Bennett's
- Better
- Rolando's
- Worse
- Bennett's
- Rare
- Rolando's
- More common
Evidence Base
Evidence Base
Contemporary Review: Anatomy, Classification and Management of Thumb Base Fractures
- Narrative review confirming that stable extra-articular fractures respond to closed reduction and casting, whereas displaced intra-articular Bennett, Rolando and highly comminuted fractures generally require surgery
- Rolando and comminuted patterns are inherently unstable and often need advanced techniques such as locking plates, external fixation or arthroscopic-assisted reduction
- Anatomical reduction is emphasised as paramount to limit joint incongruity, instability and post-traumatic arthritis
Dynamic External Fixation for Rolando Fracture
- Small case series (7 patients) treating the Y- or T-shaped Rolando fracture with a modified dynamic external fixator restoring joint space through ligamentotaxis
- Reported excellent range of motion and power grip with restoration of joint space and patients pain-free by 3 months
- No patient developed arthritic changes over the (short) follow-up period
Closed Reduction and Intermetacarpal K-wire Fixation
- Series of 25 unstable first metacarpal base fractures (including 3 Rolando and 7 Bennett) treated by closed reduction and percutaneous intermetacarpal Kirschner wires
- Fixation was stable with no secondary displacement and union at a mean of 32 days
- One of three Rolando patients had grip loss greater than 20 percent, illustrating the comminuted pattern's poorer functional reserve
ORIF versus Closed Pinning for Bennett Fracture (Reduction-Quality Principle)
- Comparative study of 32 Bennett fractures treated by ORIF versus closed transarticular K-wiring at a mean 7-year follow-up
- Treatment method did not influence clinical outcome or prevalence of radiological post-traumatic arthritis
- Percutaneous wiring carried a higher rate of first metacarpal adduction deformity from loss of reduction
Trapeziometacarpal Arthrodesis as Salvage
- Series of 72 thumbs undergoing trapeziometacarpal arthrodesis, a procedure classically favoured for young active males in the post-traumatic setting
- Fusion rate 95.8 percent using continuous-compression nitinol staples and autograft
- Key pinch improved from 6.7 to 9.3 kg and grip from 33.7 to 41.1 kg, with 94 percent patient satisfaction