The Salter-Harris Classification
- SALTR Mnemonic: Slip, Above, Lower (Through), Ram, Ruin (Crush).
- Type II is Most Common: Fracture through physis with metaphyseal fragment (Thurston-Holland).
- Type III/IV are Intra-Articular: Require anatomical reduction.
- Type V is a Crush Injury: Often diagnosed retrospectively by growth arrest.
- Distal Femur is High Risk: Accounts for 60-70% of leg length discrepancy from growth arrest.
- “Know the Salter-Harris classification perfectly
- “Understand which types require ORIF
- “Know the high-risk physes (Distal Femur, Proximal Tibia)
- “Recognize growth arrest patterns (Bar, Complete)
The Distal Femoral Physis is HIGH RISK.
- It contributes 70% of femoral length and 35% of total leg length.
- Even minor physeal damage can cause significant leg length discrepancy.
- Angular deformity (varus/valgus) is also common.
- Any Salter-Harris injury to the distal femur should be treated with respect and followed long-term for growth disturbance.
- Fracture Line
- Physis only
- Prognosis
- Good
- Treatment
- Casting
- Fracture Line
- Physis + Metaphysis
- Prognosis
- Good
- Treatment
- Reduction + Casting
- Fracture Line
- Physis + Epiphysis
- Prognosis
- Fair (intra-articular)
- Treatment
- ORIF
- Fracture Line
- All three layers
- Prognosis
- Poor (high arrest risk)
- Treatment
- ORIF
- Fracture Line
- Crush injury
- Prognosis
- Very Poor (often missed)
- Treatment
- Monitor for arrest
SALTRSALTR Mnemonic
Hook:SALTR - The classic mnemonic.
DPDDHigh-Risk Physes
Hook:DPD - Distal Femur is Priority, but Distal Tibia is tricky.
Overview/Epidemiology
Physeal Injuries are fractures involving the growth plate (physis).
- Epidemiology:
- Account for 15-30% of all pediatric fractures.
- Boys are more commonly affected (2:1).
- Peak incidence during the adolescent growth spurt ("closing physes are vulnerable physes").
- Anatomical Weakness:
- The physis is weaker than bone, ligaments, and tendons in children.
- In adults, the same mechanism would cause a ligament sprain or dislocation.
- In children, it causes a physeal fracture.
Anatomy and Pathomechanics
Physeal Anatomy The physis has distinct zones (from epiphysis to metaphysis):
- Reserve Zone (Resting Zone): Storage of nutrients. Germinal cells.
- Proliferative Zone: Chondrocyte replication (columns of cells).
- Hypertrophic Zone: Chondrocyte enlargement. Weakest zone - fractures propagate here.
- Zone of Provisional Calcification: Chondrocytes undergo apoptosis, matrix calcifies.
- Primary Spongiosa: New woven bone formation.
Fracture Propagation
- Fractures typically propagate through the hypertrophic zone (Type I, II).
- This zone is weak because the chondrocytes are dying, and the matrix is transitioning.
- The germinal cells (Reserve and Proliferative zones) are typically preserved, allowing continued growth.
- In Type III, IV, and V injuries, the germinal layers are disrupted, leading to growth arrest.
Ring of LaCroix and Perichondral Ring
- These structures provide peripheral stability to the physis.
- Injury to these (e.g., in severe Type I) can contribute to instability and arrest.
Classification Systems
Salter-Harris Classification (1963)
The gold standard.
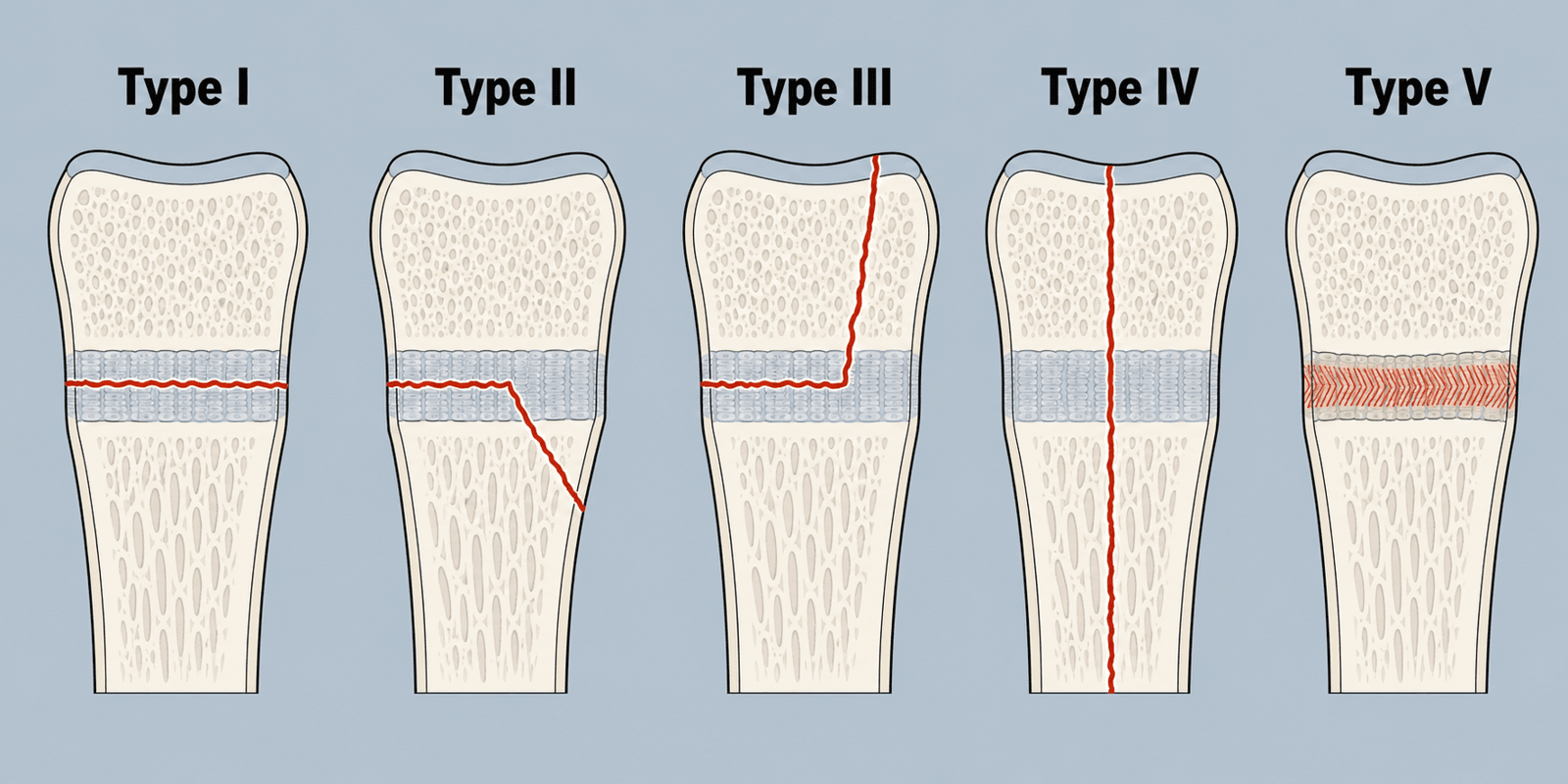
Type I: Fracture through the physis only. No metaphyseal or epiphyseal fragment. Often occult on X-ray (diagnosed by point tenderness over the physis).
Type II: Fracture through the physis with extension into the metaphysis. The metaphyseal fragment is called the Thurston-Holland fragment. Most common (75%).
Type III: Fracture through the physis with extension into the epiphysis. Intra-articular. Requires anatomical reduction.
Type IV: Fracture crosses all three layers (metaphysis, physis, epiphysis). Highest risk of growth arrest. Requires ORIF.
Type V: Crush injury to the physis. Often missed on initial X-rays. Diagnosed retrospectively when growth arrest is identified.

Clinical Assessment
- Mechanism: Fall? Twisting? Direct blow?
- Location of Pain: Point tenderness over the physis is the key finding.
- Swelling: May be minimal in Type I.
- Inspection: Swelling, deformity, ecchymosis.
- Palpation: Point tenderness over the physis = physeal injury until proven otherwise (even if X-ray is negative).
- ROM: May be limited by pain.
- Neurovascular: Document status (especially for displaced fractures).
Investigations
- X-ray (AP and Lateral): Standard. May be normal in Type I or V.
- Comparison Views: Of the contralateral (uninjured) side can be helpful for subtle widening.
- MRI: If X-ray is negative but clinical suspicion is high. Shows physeal edema.
- Useful for complex intra-articular fractures (Type III, IV) to map the fracture and plan surgery.
- 3D reconstruction is helpful.
Differential Diagnosis
The key clinical scenario is a skeletally immature child with periarticular pain and a normal or equivocal radiograph. Because the physis is the weakest link, what would be a sprain in an adult is usually a Type I physeal fracture in a child.
- Discriminating Feature
- Point tenderness exactly over the physis after acute injury
- Confirmatory Test
- Clinical; MRI if doubt
- Action
- Immobilise and treat as a fracture
- Discriminating Feature
- Tenderness over the ligament, not the physis; uncommon pre-maturity
- Confirmatory Test
- MRI / stress views
- Action
- Functional rehab once fracture excluded
- Discriminating Feature
- Insidious overuse pain, no single trauma
- Confirmatory Test
- MRI or bone scan
- Action
- Activity modification
- Discriminating Feature
- Fever, refusal to bear weight, raised CRP/ESR
- Confirmatory Test
- Bloods, aspiration, MRI
- Action
- Urgent — antibiotics +/- washout
- Discriminating Feature
- Night pain, mass, systemic symptoms, metaphyseal lesion
- Confirmatory Test
- Radiograph + MRI, refer
- Action
- Do not biopsy — refer to tumour unit
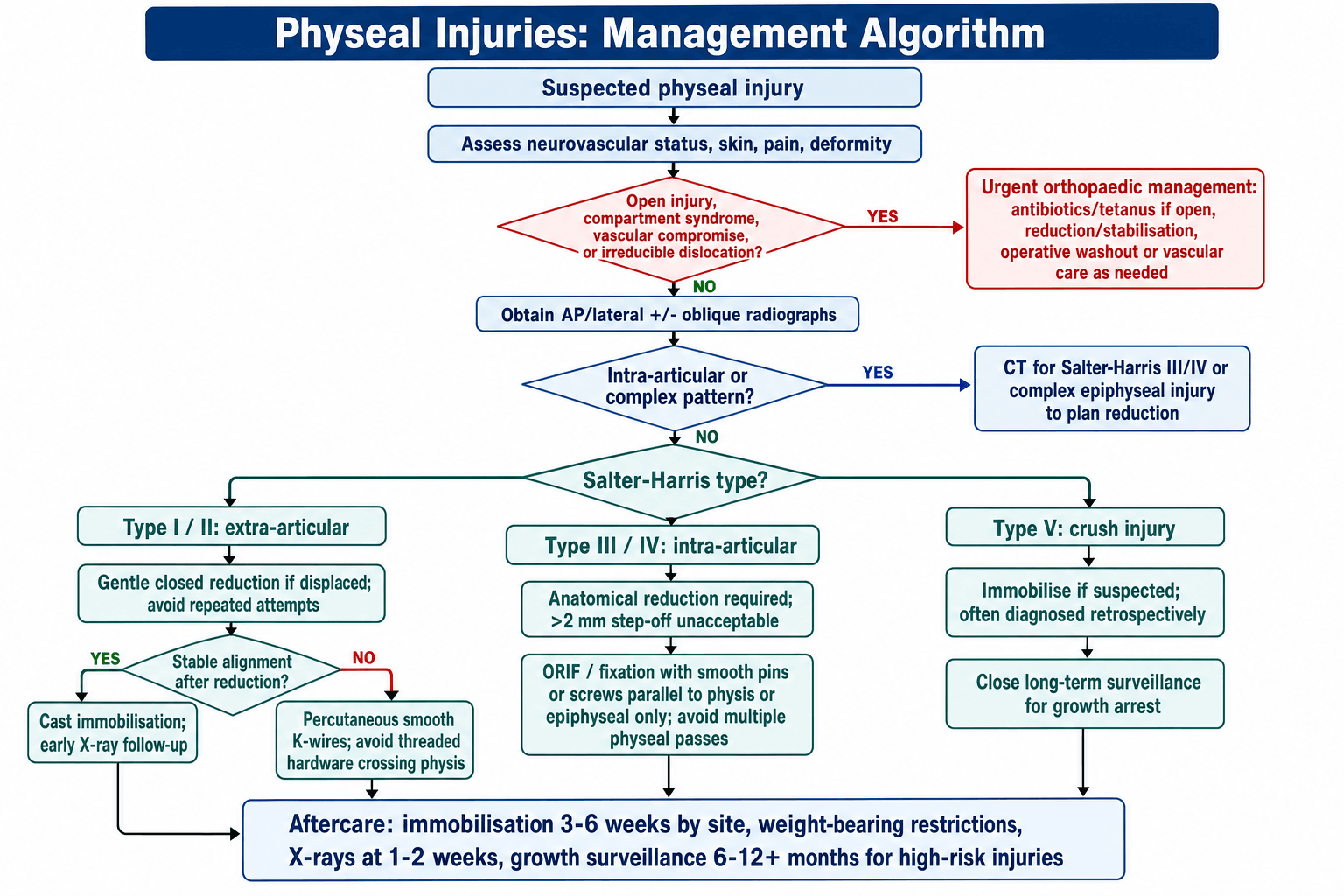
Management Algorithm
Type I and II (Extra-Articular)
- Closed Reduction and Casting is the mainstay.
- Gentle manipulation. Avoid repeated reduction attempts (damages physis).
- If stable: Cast immobilization.
- If unstable after reduction: Consider percutaneous pinning (smooth K-wires that do not cross the physis).
- Do NOT cross the physis with threaded hardware (exception: very localized Type IV with screw well away from the rest of the physis).
Surgical Techniques
Percutaneous K-Wire Fixation
Indications: Unstable Type I/II after reduction, or Type III/IV after open reduction.
Technique: Closed or open reduction under fluoroscopic guidance. Pass smooth K-wires, avoiding crossing the physis if possible. For Type III/IV, place pins through the epiphysis, parallel to the physis. Bury or leave percutaneous. Immobilize in cast and remove pins at 3-4 weeks.
Key Technical Points When performing ORIF for physeal injuries, the surgeon must balance the need for rigid fixation against the risk of iatrogenic physeal damage. The following principles guide technique selection:
- Use the smallest effective implants.
- Place hardware parallel to the physis when possible.
- If screws must cross the physis, use small diameter (less than 4.0mm) and remove early.
- Minimize soft tissue stripping to preserve blood supply.
Reduction Maneuvers by Type
- Type I: Gentle traction and reduction. Avoid aggressive manipulation.
- Type II: Reverse the mechanism (e.g., apex posterior = flex and apply posterior force). Use the Thurston-Holland fragment as a guide.
- Type III/IV: Open reduction to visualize the articular surface. The physis cannot be adequately assessed closed.
Postoperative Immobilization
- Long leg cast for lower limb physeal injuries.
- Above elbow cast for upper limb physeal injuries.
- Duration: 4-6 weeks for most injuries, longer for distal femur.
Complications
- Rate
- Variable (1-10% Type II, up to 50% Type IV)
- Prevention/Management
- Anatomical reduction. Avoid physis damage.
- Rate
- Common with partial arrest
- Prevention/Management
- Bar excision if less than 50% physis affected, osteotomy if complete.
- Rate
- Depends on site and age
- Prevention/Management
- Epiphysiodesis or lengthening depending on discrepancy.
- Rate
- Rare (except specific sites like femoral head)
- Prevention/Management
- Gentle reduction. Minimize soft tissue stripping.
- Rate
- Very Rare
- Prevention/Management
- Good blood supply in children.
Harris (Park-Harris) Growth-Arrest Lines
This topic repeatedly mandates "follow-up radiographs to screen for growth disturbance" and "surveillance to maturity" — the radiographic tool that makes that surveillance work is the Harris line (Park-Harris growth-arrest line), which can flag a physeal bar early, before deformity is established.
- What it is. After any insult that transiently slows the physis (a fracture, serious illness, chemotherapy), growth briefly stops then resumes, laying down a transverse dense (sclerotic) line in the metaphysis parallel to the physis — a "footprint" of where the physis sat at the time of the insult.
- How to read it for arrest:
- A symmetric line that is parallel to the physis and moves away from it with subsequent growth means the physis has resumed normal, even growth — reassuring, no bar.
- A line that is NOT parallel — converging on or tethered to one point of the physis means that point has stopped growing while the rest continues; the line points toward the physeal bar. This is the early radiographic signature of a partial arrest, often visible before any clinical angulation.
- Why it matters. It operationalises the "surveillance to maturity" recommended throughout: a Harris line running parallel and moving away reassures, whereas one converging on a focal area flags a forming bar and prompts MRI mapping and early intervention — while the discrepancy or angulation is still small and correctable.

Q: On a follow-up radiograph after a physeal fracture, what does a Harris line tell you? A: A transverse metaphyseal line parallel to the physis and moving away from it confirms resumed symmetric growth (no bar). A line that is asymmetric and converges on a point of the physis points to a forming bar at that site — the earliest radiographic warning of partial growth arrest, before deformity appears.
Postoperative Care
- Immobilization: Cast or splint for 3-6 weeks depending on location.
- Weight Bearing: Usually non-weight bearing initially for lower limb injuries.
- Follow-up: X-rays at 1-2 weeks to confirm alignment, then at 6-12 months to screen for growth disturbance.
- Long-Term Surveillance: Any patient with a SH III, IV, or high-risk location (distal femur) should be followed for at least 1 year for growth arrest.
Rehabilitation Protocol
Phase 1: Immobilization (0-4 weeks)
- Cast or splint immobilization.
- Non-weight bearing for lower limb injuries.
- Gentle ROM of uninvolved joints.
Phase 2: Early Mobilization (4-6 weeks)
- Cast removal if healed.
- Progressive weight bearing.
- Gentle ROM exercises.
Phase 3: Strengthening (6-12 weeks)
- Progressive strengthening.
- Proprioception and balance.
- Return to activities.
Long-Term
- Follow-up X-rays at 6-12 months to screen for growth disturbance.
Why Physeal Shape Modifies the Prognosis (Beyond the SH Type)
The Salter-Harris type predicts prognosis because a fracture through the flat hypertrophic zone spares the germinal (reserve and proliferative) cells — but this topic repeatedly notes the distal femur is "worst regardless of type", with even a Type II there carrying a 30-50% arrest risk. The reason is that the SH type is not the whole story: the three-dimensional shape of the physis matters.
- A flat physis (e.g. distal radius) fractures cleanly and transversely through the hypertrophic zone in a Type I/II, leaving the germinal layers intact — hence the excellent prognosis and rare arrest.
- An undulating, interdigitated physis — the distal femur is the extreme, with prominent mamillary processes and a wavy contour that anchors it to the epiphysis — cannot fail through a single clean plane. A shear injury tears across the germinal layers even in a nominally "safe" Type I or II, which is why the distal femur behaves worse than its SH type predicts and why even a non-displaced Type II there is followed to maturity.
- The practical corollary: counsel and follow up by site as well as SH type. A Type II distal radius is benign; an identical Type II at the distal femur is a high-arrest injury. (The distal-femur-specific management is developed in the distal-femoral-physeal-injuries topic.)
Q: Why does a Salter-Harris II of the distal femur carry a far higher arrest risk than a Salter-Harris II of the distal radius? A: Because the distal femoral physis is highly undulating/interdigitated (mamillary processes), a shear injury crosses the germinal layers even in a Type I/II, whereas the flat distal radial physis fractures cleanly through the hypertrophic zone and spares them. Prognosis depends on physeal geometry and site, not the SH type alone.
ASTRFactors Affecting Prognosis
Hook:ASTR - Assess these factors for prognosis.
Outcomes/Prognosis
- Type I/II: Generally excellent. Growth arrest is rare (less than 2% for Type II).
- Type III/IV: Fair to poor if malreduced. Good if anatomically reduced. Arrest rate 10-50%.
- Type V: Poor. Often missed initially. Growth arrest is common.
- Site Matters: Distal femur has the worst outcomes regardless of type.
Guidelines, Registries & Global Practice
Global epidemiology
- Physeal fractures account for 15-30% of all paediatric fractures; the Olmsted County population study (Peterson 1994) gives an incidence of ~279/100,000 person-years, male:female 2:1, peaking in 11-12-year-old girls and 14-year-old boys.
- Salter-Harris Type II is the commonest type (about half of cases); the distal radius and phalanges are the commonest sites.
Where society guidance converges (no major disagreement)
- AAOS / POSNA (US)
- Anatomical reduction, fixation parallel to physis
- BOA-BOAST / NICE (UK)
- Anatomical reduction; specialist paediatric input
- AO Foundation / EFORT (Europe)
- Anatomical joint and physis restoration
- AAOS / POSNA (US)
- Smooth wires preferred; remove early
- BOA-BOAST / NICE (UK)
- Avoid threaded transphyseal fixation in young children
- AO Foundation / EFORT (Europe)
- Epiphyseal/metaphyseal fixation; spare the physis
- AAOS / POSNA (US)
- Until growth disturbance excluded / maturity for high-risk
- BOA-BOAST / NICE (UK)
- Safeguard against missed arrest; clear follow-up pathway
- AO Foundation / EFORT (Europe)
- Follow high-risk physes to maturity
- There is no Salter-Harris-specific national clinical guideline from AAOS, NICE or AO; practice is consensus- and evidence-based rather than protocolised, and the principles above are essentially universal.
Registry note
- Paediatric physeal injuries are not tracked by the major arthroplasty registries (NJR, AJRR, AOANJRR, SHAR). Outcome data derive from institutional series (e.g. Arkader for the distal femur, Barmada for the distal tibia) rather than registries.
High- vs limited-resource practice variation
- Well-resourced settings: ready MRI/CT for occult or complex injuries, low-dose EOS for limb-length surveillance, navigation/fluoroscopy for bar excision, and tension-band (guided-growth) plating for angular correction.
- Limited-resource settings: reliance on plain radiographs and clinical follow-up, closed reduction and casting as the default, and later presentation of established deformity managed by osteotomy. The core principle — gentle anatomical reduction and avoidance of physeal injury — is achievable anywhere.
- Surveillance: any child with an SH III/IV, a high-risk physis (distal femur, proximal tibia) or a suspected Type V should be followed for at least 1-2 years, or to maturity for the highest-risk injuries.
Deep Dive: Hardware and the Physis
Can you cross the physis with hardware?
- Smooth K-wires: Yes. They cause minimal localized damage. Remove early (3-4 weeks).
- Threaded screws: Avoid if possible. They create a "tether" that can cause asymmetric growth (angular deformity).
- Exception: In Type IV fractures, a single 4.0mm screw placed perpendicular to the fracture line (crossing the physis) may be acceptable if placed centrally and only one or two small holes are made. The risk is lower than leaving a malreduced fracture.
Key Principle The bigger the physis (younger the child, more growth remaining), the more cautious you must be about crossing it.
Deep Dive: Physeal Bar Excision
What is a Physeal Bar?
- A bridge of bone that forms across the injured physis, tethering growth.
- Can be central (causes shortening only) or peripheral (causes angular deformity).
Indications for Bar Excision
- Bar less than 50% of physis width.
- At least 2 years (or 2cm) of growth remaining.
- Angular deformity that is progressive.
Technique
- Preoperative MRI to map the bar.
- Approach based on bar location.
- Excise the bar under fluoroscopy and direct vision.
- Interpose fat graft or PMMA (to prevent bar reformation).
- Consider concurrent osteotomy if significant angular deformity.
Outcomes
- Restoration of growth in 50-80% of cases.
- Better results with smaller bars and more growth remaining.
Parent's Guide: Understanding Physeal Injuries
What is a Growth Plate? A growth plate is a layer of cartilage near the end of a bone where growth occurs. Children's bones grow from these areas until they reach skeletal maturity (around age 14-16 for girls, 16-18 for boys).
What happens if the growth plate is injured? Most growth plate injuries heal completely without any problems. However, in some cases, the injury can damage the cells responsible for growth, leading to:
- Shorter limb: If growth slows or stops.
- Crooked limb: If one part of the growth plate is damaged but the rest keeps growing.
How is it treated?
- Most injuries are treated with a cast.
- Some injuries (especially those that go into the joint) may require surgery to realign the bones.
What are the warning signs? Your doctor will want to see your child for follow-up X-rays. Call them if you notice:
- One leg looking shorter than the other.
- A limb that seems to be growing crooked.
Long-term outlook Most children do very well. Your doctor may want to monitor your child with X-rays over the next 1-2 years to ensure the growth plate is healing normally.
Controversies & Areas of Uncertainty
- Open vs closed reduction of gapped SH I/II fractures. Barmada showed a residual physeal gap (over 3 mm) is associated with a 60% closure rate and entrapped periosteum. Whether routine open removal of interposed periosteum actually lowers arrest remains unproven — it is biologically logical but not supported by randomised data.
- Crossing the physis with hardware. It is widely taught that smooth wires are safe and threaded screws are not, yet small (under 7% of physeal area), centrally placed, briefly retained screws are used routinely without measurable arrest. The true safe threshold is extrapolated from animal work, not human trials.
- Routine MRI/CT after closed reduction. Advanced imaging detects gaps and early bars earlier, but Thawrani showed CT does not improve classification reliability and rarely changes the decision. Cost, radiation (CT) and sedation needs argue against routine use; reserve for surgical planning.
- Prophylactic contralateral epiphysiodesis timing. For an established distal-femoral arrest, the trade-off between accepting limb-length discrepancy, contralateral epiphysiodesis, bar excision and lengthening is individualised; multiplier-method timing carries inherent prediction error.
- The "transitional" distal tibia. Whether a 2 mm step-off threshold for Tillaux/triplane fractures (derived from adult articular data) is the correct cut-off in a near-closed physis with little remaining growth is debated; some accept slightly more in the oldest adolescents.
MCQ Practice Points
Q: Which Salter-Harris type is most common? A: Type II (75% of physeal fractures). Fracture through physis with a metaphyseal (Thurston-Holland) fragment.
Q: Which Salter-Harris type has the worst prognosis for growth arrest? A: Type IV and V. Type IV crosses all layers. Type V is a crush injury.
Q: Which zone of the physis is the weakest? A: Hypertrophic zone. This is where Type I and II fractures propagate.
Q: What is the maximum acceptable step-off for a Salter-Harris Type III or IV fracture? A: 2mm. Greater than 2mm requires ORIF.
Q: Can threaded screws be placed across the physis? A: Avoid if possible. Threaded hardware creates a tether causing asymmetric growth. Use smooth K-wires and remove early (3-4 weeks).
Q: What is the significance of the distal femoral physis? A: High risk location. Contributes 70% of femoral growth and 35% of leg length. Even Type II injuries have 30-50% arrest risk.
Self-Assessment Quiz
Additional Self-Assessment Questions
Specific Physeal Injuries by Location
Distal Radius
- Most common pediatric physeal injury.
- Usually Type I or II. Excellent prognosis.
- Growth arrest is rare (less than 5%).
- Treatment: Closed reduction and casting.
Distal Femur
- High-risk injury. 70% of femoral growth from this physis.
- Growth disturbance in 30-50% of cases.
- Even Type II can lead to significant LLD or angular deformity.
- Requires close long-term follow-up.
Proximal Tibia
- Also high-risk. Contributes 55% of tibial growth.
- Risk of popliteal artery injury (tethered by genicular branches).
- Always perform thorough vascular examination.
Distal Tibia
- Transitional fractures (Tillaux, Triplane) occur as physis is closing.
- Type III (Tillaux) and Type IV (Triplane) are common patterns.
- Require anatomical reduction if displaced.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“9-year-old with ankle pain after a twisting injury. X-ray is normal. Point tenderness over the distal fibular physis.”
“12-year-old with a Salter-Harris Type IV fracture of the distal tibia. 3mm of articular step-off on CT.”
“8-year-old presents 1 year after a Salter-Harris II distal femur fracture. Now has 2cm of LLD and progressive valgus.”
“5-year-old with a lawnmower injury to the foot. Significant soft tissue loss over the lateral malleolus and visible physis.”
CLASSIFICATION
- I: Physis only
- II: + Metaphysis (Most Common)
- III: + Epiphysis (Intra-art)
- IV: All Three (Worst)
ANATOMY
- Hypertrophic Zone (Weakest)
- Reserve Zone (Germinal)
- Perichondral Ring (Stability)
- Thurston-Holland (Type II)
HIGH RISK SITES
- Distal Femur (70% growth)
- Proximal Tibia
- Distal Tibia (Tillaux)
- Type IV Anywhere
TREATMENT
- I/II: Cast
- III/IV: ORIF (greater than 2mm)
- V: Monitor
- Avoid crossing physis
Evidence Base
- Original five-type classification based on the anatomy of the fracture line and its relation to the germinal layers
- Prognosis worsens from Type I to Type V as the proliferative/reserve zones become involved
- Established that crushing injury (Type V) carries the worst prognosis
- 850 children sustained 951 physeal fractures over 10 years; incidence 279/100,000 person-years
- Male:female ratio 2:1; peak in 11-12-year-old girls and 14-year-old boys
- Phalanges of the fingers were the commonest site (37%); Salter-Harris II was the commonest type (54%)
- Proposed a classification with anatomic, epidemiologic and prognostic basis after review of all prior systems
- Added previously unclassified patterns including metaphyseal-only and transverse-physis injuries
- Type VI (perichondral/periosteal ring injury, e.g. lawnmower) carries high peripheral-bar risk
- 27% of 92 distal tibial physeal fractures developed premature physeal closure
- A residual physeal gap over 3 mm after reduction raised closure to 60% vs 17% with no gap
- Quality of reduction — not initial displacement, attempts or method — predicted closure; entrapped periosteum was found in gapped SH I/II fractures
- Adding CT to radiographs did NOT improve interobserver reliability of Salter-Harris classification (kappa fell from 0.67 to 0.57)
- Surgeons rated CT most useful for planning screw placement (56%), not for the treatment decision
- CT changed the management plan in only about one fifth of complex cases
- 43 bar excisions in 35 patients; bone bridge replaced with a free fat transplant
- Most operations restored growth and corrected or prevented deformity; benefit was questionable in 7
- Age, bar location and bar size determined both the indication and the result
Additional Evidence
- 73 distal femoral physeal fractures across 2 Level I centres; overall complication rate 40%, growth arrest most frequent
- Salter-Harris grade and displacement (48.8% vs 26.6% complications) were significant predictors of outcome
- Complications were higher when hardware violated the physis (65% vs 30%)
- Reinforces that CT is for operative planning of Type III/IV patterns, not routine grading
- Interobserver reliability of SH grading remained only moderate even with CT
- Displacement measurement was highly reproducible on both radiograph and CT