Intra-articular fractures of the distal tibia (Tibial Plafond)
- Soft Tissue is King: Respect the envelope. Do not plate through swollen skin.
- Staged Protocol: 1. ExFix (Span) to 2. CT Scan (Plan) to 3. ORIF (Fix) when swelling subsides (10-21 days).
- 3 Columns: Fixation strategy relies on rebuilding the Anterolateral, Anteromedial, and Posterior columns.
- Syndesmosis: Often intact in Pilon (unlike rotational ankle fractures) because the force is axial.
- “Varus vs Valgus: Determines which column failed in tension vs compression.
- “Open Fractures: High rate due to thin medial skin cover.
- “Compartment Syndrome: Always check calcaneal compartment.
Operating through blistered or swollen skin guarantees wound breakdown and infection. Wrinkle Sign is mandatory before definitive surgery.
Can occur in the foot or leg. Pain out of proportion? Pain on passive toe stretch?
Check the lumbar spine (L1) and calcaneus (Lover's Triad) due to axial load mechanism.
Check deep peroneal nerve (sensation 1st web space) and dorsalis pedis pulse before and after reduction.
- Timing
- Immediate
- Treatment
- **Spanning ExFix**
- Rationale
- Restore length, allow soft tissue recovery.
- Timing
- Day 1-14
- Treatment
- **WAIT** (Elevate)
- Rationale
- Operating now = Infection/Dehiscence.
- Timing
- Day 14-21
- Treatment
- **Definitive ORIF**
- Rationale
- Soft tissue can tolerate incision.
- Timing
- Any
- Treatment
- **Circular Frame / Fusion**
- Rationale
- Reconstruction not possible or poor bone stock.
MAPThe Columns (Y-configuration)
Hook:Draw a MAP of the articular surface.
Overview and Epidemiology
A Pilon (French for "Pestle") fracture is an intra-articular fracture of the distal tibia metaphysis involving the weight-bearing dome (plafond). It typically results from high-energy axial loading.
- 1-10% of lower extremity fractures.
- Bimodal:
- Young males: High energy (fall from height, MVA).
- Elderly females: Low energy (rotational ankle fracture variant).
- Associations:
- Open fracture (20-25%).
- Fibula fracture (75-85%).
- Polytrauma.
Anatomy
- Tibial Plafond: The weight-bearing articular surface. It is wider anteriorly than posteriorly (trapezoidal).
- Three Pillars (AO Concept):
- Medial Column: Medial malleolus and anteromedial cortex.
- Lateral Column: Anterolateral tibia (Chaput tubercle).
- Posterior Column: Posterior malleolus (Volkmann).
- Fibula: Acts as a lateral buttress. If fractured, it indicates significant instability.
- Subcutaneous: The anteromedial face of the tibia is strictly subcutaneous with no muscle cover. This is the "danger zone" for wound breakdown.
- Fascial Compartments:
- Anterior (Deep Peroneal N, Anterior Tibial A).
- Lateral (Superficial Peroneal N).
- Posterior (Tibial N, Posterior Tibial A).
- Deep Posterior.
- Knowledge of vascular supply is critical for incision planning.
- Anteromedial approach: Safe zone, supplied by Saphenous/Posterior Tibial branches? No, risky.
- Anterolateral approach: Supplied by Anterior Tibial artery (perforators).
- Bridge: The skin bridge between an anterolateral and posteromedial incision must be at least 7cm.
Blood Supply Details
- Anterior Tibial Artery: Becomes the Dorsalis Pedis. Main supply to anterior compartment structures. Perforators supply the anterolateral skin.
- Posterior Tibial Artery: Main supply to the medial ankle and deep posterior compartment. The medial malleolar artery (branch) is at risk during medial approaches.
- Peroneal Artery: Supplies the lateral compartment. Branches contribute to the syndesmotic region.
- Watershed Zone: The anteromedial tibial skin is a "watershed" area between the anterior and posterior tibial angiosomes, making it highly susceptible to necrosis.
Ligamentous Anatomy
- Syndesmosis: AITFL, PITFL, Transverse ligament, Interosseous membrane. Unlike rotational ankle fractures, the syndesmosis is often intact in axial Pilon because the force is vertical, not rotational.
- Deltoid Ligament (Medial): Deep and superficial components. Important for medial stability. Assess for injury by palpating the medial gutter.
- Spring Ligament (Calcaneonavicular): Supports the talar head. Can be injured in high-energy Pilon variants with significant foot injury extension.
Classification Systems
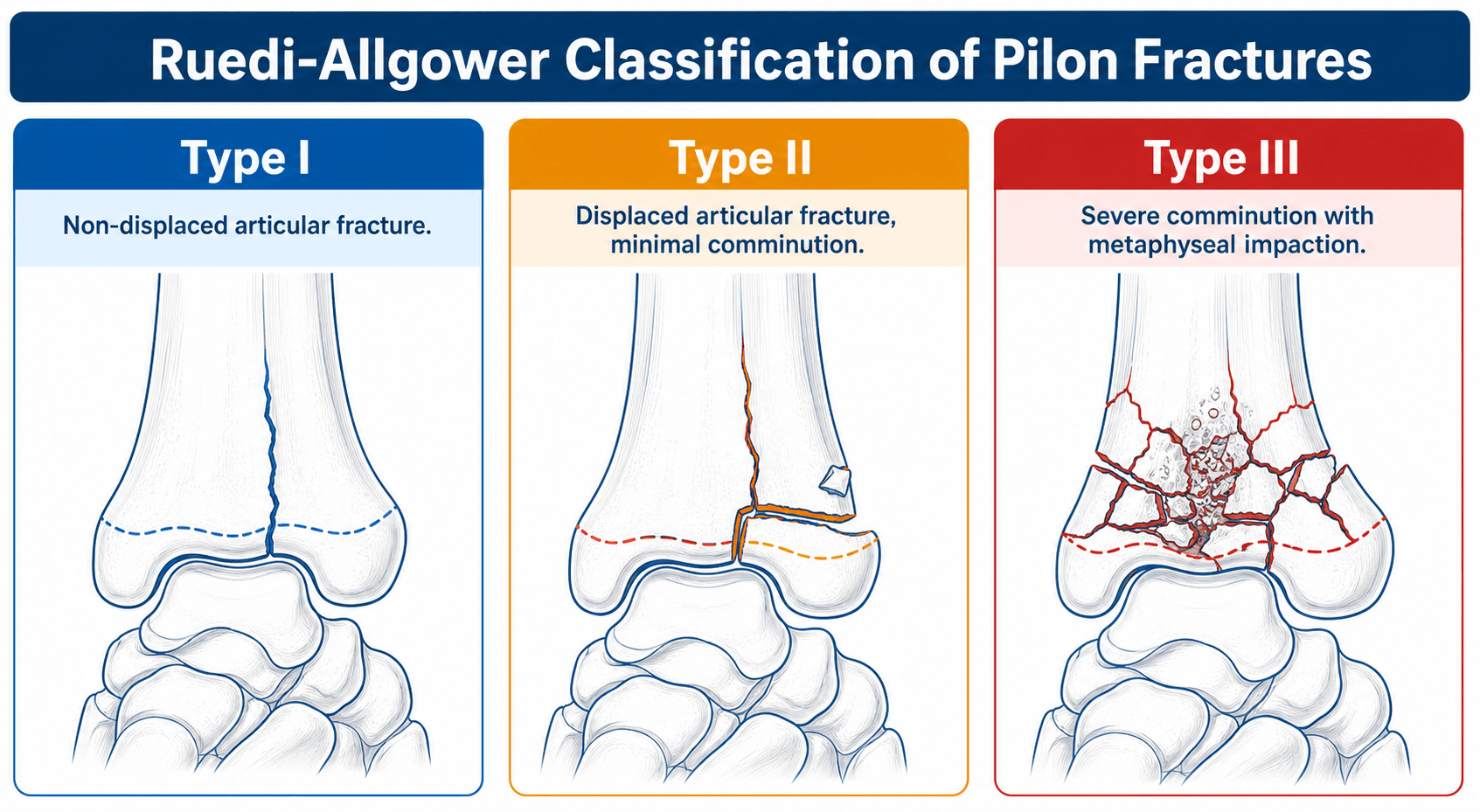
Based on displacement and comminution.
- Type I: Intra-articular, non-displaced.
- Type II: Displaced, but articular fragments are recognizable and congruous (implying standard ORIF feasible).
- Type III: Displaced with metaphyseal impaction and articular comminution (The "Explosion" fracture).
S-D-CRuedi-Allgower Classification
Hook:Simple to Displaced to Comminuted.
Grading the Soft-Tissue Injury: the Tscherne Classification
"Soft tissue is King" runs through this topic and dictates the timing of every step — the formal way to grade the closed soft-tissue injury is the Tscherne classification.
- Why grade it. The staged protocol is driven by the state of the soft-tissue envelope, not the bone; a formal grade communicates severity, guides timing, and predicts wound complications.
- Tscherne grades of the CLOSED injury:
- Grade 0 — negligible soft-tissue injury; simple fracture from an indirect force.
- Grade I — superficial abrasion or contusion from fragment pressure within; mild-to-moderate fracture.
- Grade II — deep contaminated abrasion with local skin and muscle contusion and impending compartment syndrome; a more severe, often direct-force fracture.
- Grade III — extensive skin contusion or crushing, severe muscle damage, subcutaneous degloving, and overt compartment syndrome or arterial injury.
- How it maps to management. Higher Tscherne grades mean a longer wait behind the spanning fixator and a higher threshold for open incisions; the clinical signs this topic already uses — fracture blisters (clear vs haemorrhagic), swelling and the wrinkle sign — are how you track the envelope back to a safe (low) grade before definitive ORIF.
- Open injuries are graded separately by Gustilo-Anderson (developed in the open-fracture topic); Tscherne specifically grades the CLOSED soft-tissue injury that governs most pilon timing.
Q: What system grades the closed soft-tissue injury that dictates pilon timing, and why does it matter? A: The Tscherne classification (Grade 0-III) of the closed soft-tissue injury. Because pilon timing is driven by the envelope, a higher grade (deep contusion, degloving, impending/overt compartment syndrome) means a longer wait behind the spanning fixator; the wrinkle sign and blister epithelialisation signal the envelope has recovered enough for definitive ORIF. Open injuries are graded by Gustilo-Anderson instead.
Clinical Assessment
- Mechanism (Fall from height vs Twisting).
- Smoking status (Critical for wound healing prognosis).
- Diabetes/Neuropathy.
- Inspection: Look for open wounds (medial side), tenting of skin, fracture blisters.
- Clear fluid blisters: Epidermal injury. Can operate through (carefully).
- Hemorrhagic blisters: Dermal/Subdermal injury. Do NOT incise. Wait for epithelialization.
- Neurovascular: Pulses and Sensation.
- Compartments: Pain with passive extension of toes? (Leg and Foot).
Systematic Examination
- Deformity - Varus/Valgus, Shortening.
- Skin - Open wounds, Tenting, Blisters, Degree of swelling.
- Foot position - External rotation (suggests PER)?
- Tenderness - Entire tibia, Ankle mortise, Medial malleolus, Fibula.
- Compartments - Tense? (Anterior and Deep Posterior at highest risk).
- Pulses - DP and PT. Document pre- and post-reduction.
- Do NOT attempt active motion if clearly fractured.
- Assess passive motion gently to evaluate joint stability.
- Deep Peroneal N: Sensation in 1st web space. EHL motor function.
- Tibial N: Sensation on plantar foot. FHL motor function.
- Document meticulously - Neurologic injury may occur from swelling or compartment syndrome.
All high-energy Pilon fractures are at risk. Monitor pain out of proportion, pain with passive toe stretch. Consider prophylactic fasciotomy if swelling severe.
Investigations
Plain X-rays:
- Views: Ankle AP, Lateral, Mortise. Full Tib/Fib. Foot views (Calcaneus).
- Findings:
- Articular step-off.
- Varus/Valgus angulation.
- Talus impaction into tibia.
- Fibula fracture level.
Reading the CT: Fracture Mapping and the Primary Fracture Patterns
The topic makes the post-fixator CT mandatory and uses the "Mercedes Benz" three-column sign — here is how to actually map the fragments and the recognised primary patterns.
- Map the fragments after ligamentotaxis. The CT is taken after the spanning fixator has restored length, which pulls the major fragments apart and makes them readable. On the axial cut the classic "Mercedes Benz" (Y) sign separates the three constant fragments — anterolateral (Tillaux-Chaput), medial, and posterior (Volkmann); the sagittal cut shows posterior-fragment size and impaction, and the coronal cut shows varus/valgus and central die-punch impaction.
- Primary fracture-line families (Topliss). High-energy pilon fractures cluster into a sagittal family and a coronal family of fracture lines, with comminution and impaction usually maximal at the anterolateral or anteromedial plafond depending on foot position at impact (dorsiflexion drives the anterior fragment, plantarflexion the posterior). Recognising the family tells you which column to buttress and which approach to use.
- The die-punch fragment. A central, impacted osteochondral fragment driven up into the metaphysis must be disimpacted, reduced to the articular frame, and its void bone-grafted - leaving it impacted guarantees articular incongruity.
- The "double contour" sign. On the plain AP/mortise, a doubled subchondral line ("double contour / double density") betrays an impacted or rotationally malreduced articular fragment - a warning of residual incongruity that should prompt CT correlation and correction.
Q: You have the post-fixator CT - what are you looking for and how does it change the operation? A: Map the three constant fragments on the axial "Mercedes Benz" Y (anterolateral Chaput, medial, posterior Volkmann), size the posterior fragment on sagittal, and read varus/valgus and central die-punch impaction on coronal. Identify the Topliss sagittal- vs coronal-family line to choose the column to buttress and the approach; disimpact and bone-graft any die-punch fragment. A "double contour" on plain films flags an impacted/malrotated fragment to correct.
Differential Diagnosis
- Mechanism
- Axial load (talus driven into tibia)
- Key Distinguishing Feature
- Intra-articular comminution + metaphyseal impaction; syndesmosis often intact
- Implication
- Staged management, guarded prognosis
- Mechanism
- Rotational / torsional
- Key Distinguishing Feature
- Malleolar fracture lines without plafond impaction; syndesmosis often disrupted
- Implication
- Often early single-stage ORIF, good prognosis
- Mechanism
- Bending / axial
- Key Distinguishing Feature
- Fracture spares the articular surface
- Implication
- Nail or plate; better outcome than true pilon
- Mechanism
- Axial + dorsiflexion
- Key Distinguishing Feature
- Body/neck of talus involved; talar dome AVN risk
- Implication
- Different fixation, AVN surveillance
- Mechanism
- Axial load at the knee
- Key Distinguishing Feature
- Proximal (not distal) articular surface; check both ends in fall-from-height
- Implication
- Screen the ipsilateral limb and spine
Management Algorithm
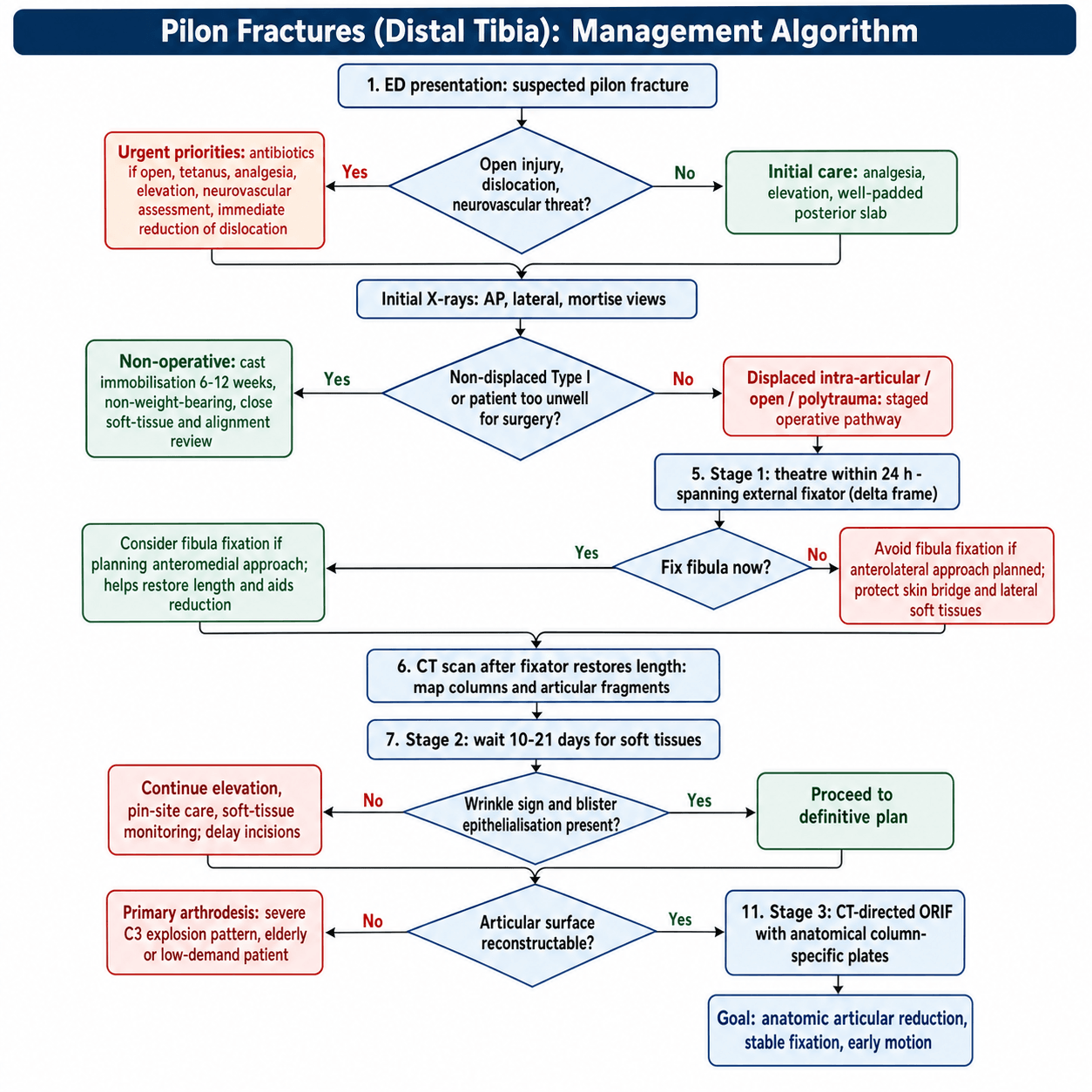
The Gold Standard: Span, Scan, Plan.

-
Stage 0 (ED Presentation):
- Action: Immediate reduction of dislocation.
- Splint: Well-padded posterior slab.
- Imaging: X-rays (AP/Lat/Mortise).
- Medication: Analgesia, Elevation, Antibiotics (if open).
-
Stage 1 (Theatre < 24hrs):
- Action: Application of Spanning External Fixator (Delta Frame).
- Fibula: Fixation of fibula is controversial.
- Pros: Restores length, aids reduction.
- Cons: Increases lateral wound complications.
- Decision: Fix if planning anteromedial approach. Avoid if planning anterolateral approach (skin bridge issues).
- CT Scan: Obtain CT only AFTER the fixator has pulled the fracture out to length.
-
Stage 2 (The Wait):
- Duration: Typically 10-21 days.
- Goal: Resolution of soft tissue edema.
- Sign: "Wrinkle Sign" (skin wrinkles when pinched) and epithelialization of fracture blisters.
-
Stage 3 (Definitive Fixation):
- Action: ORIF with anatomical specific plates.
- Approach: Dictated by the CT scan (Column concept).
Surgical Techniques
- Interval: Between Tibialis Anterior and Tibia (No true internervous plane).
- Indication: Fixation of Medial Column + Posterior Column (indirectly).
- Risk: Saphenous vein/nerve. Skin breakdown (watershed area).
- Interval: Between Peroneus Tertius and Extensor Hallucis Longus (or Tib Ant).
- Indication: Fixation of Anterolateral fragment (Chaput) + Lateral column. Allows visualization of joint surface.
- Risk: Superficial Peroneal Nerve (seen in subcut fat).
- Benefit: Better muscle coverage over plate than medial side.
- Interval: Between Peroneus Brevis and FHL.
- Indication: Fixation of Posterior Malleolus (Volkmann).
- Timing: Can be done acutely or staged.
Span, Scan, PlanSurgical Strategy
Hook:Don't rush in. Span it, Scan it, then Plan it.
Complications
- Wound Dehiscence / Infection (10-30%):
- Highest rate in orthopaedic trauma.
- Deep infection often requires free flap coverage or amputation.
- Post-Traumatic Arthritis (50%+):
- Almost inevitable in Type III injuries.
- Correlates with quality of reduction (less than 2mm stepoff).
- Treatment: Ankle Arthrodesis or Arthroplasty (in elderly).
- Nonunion (5-10%):
- Metaphyseal junction nonunion.
- Malunion:
- Varus malunion common.
- Stiffness:
- Arthrofibrosis from prolonged immobilization.
- Chronic Pain:
- CRPS type symptoms.
Hardware Complications
- Hardware Failure (Plate Breakage):
- Risk factors: Early weight bearing, Severe comminution, Poor reduction.
- Management: Plate out, Bone graft, Re-plate. Consider IM nail.
- Prominent Hardware:
- Due to thin soft tissue over anteromedial tibia.
- Management: Remove once union achieved (6-12 months post-op).
- Screw Irritation:
- Periarticular screws can cause synovitis if protruding into joint.
- Remove prominent screws.
Deep Venous Thrombosis (DVT)
- Risk: High due to lower limb trauma, NWB, immobilization.
- Prophylaxis: LMWH or Aspirin. Decision based on bleeding risk and institutional protocol.
- Diagnosis: Clinical suspicion (calf swelling, pain). Duplex US.
- Treatment: Anticoagulation.
Stiffness (Near Universal)
- Cause: Intra-articular scarring, cartilage damage, prolonged immobilization.
- Prevalence: Loss of 10-20 degrees dorsiflexion is common.
- Impact: Affects gait (requires greater knee flexion).
- Management: Early ROM exercises. Aggressive physiotherapy. MUA rarely helpful.
Checklist for Complications:
- Wound Healing:
- The anteromedial skin is precarious.
- Vacuum dressings (PICO) often used prophylactically.
- Any necrosis must be debrided early and covered (Flap).
- Stiffness:
- Ankle stiffness is universal.
- Loss of dorsiflexion is most debilitating.
- Infection:
- Deep infection rate is 5-15% in closed fractures, higher in open.
- Staph aureus is most common pathogen.
- Management: Debridement, retention of hardware (if stable) or removal (if loose) + antibiotics.
- CRPS (Complex Regional Pain Syndrome):
- Vitamin C 500mg daily proposed for prevention (controversial evidence but low harm).
Postoperative Care
- Weeks 0-2 (Wound Check):
- Splint in neutral.
- Strict elevation.
- NWB.
- Ensure wound healing before motion.
- Weeks 2-6 (Motion):
- Start active ankle pumping (Dorsiflexion/Plantarflexion).
- No inversion/eversion (stresses columns).
- Removable boot.
- Weeks 6-12 (Loading):
- Start partial weight bearing (proprioception).
- Progress to full weight bearing by 12 weeks if X-rays show union.
Outcomes/Prognosis
- Return to Work: Average 12 months.
- Make it clear: "Your ankle will never be normal again." (Manage expectations).
- Score: AOFAS scores typically 70-80/100.
- Arthrodesis Rate: 10-20% require fusion within 5-10 years.
Guidelines, Registries & Global Practice
Global epidemiology:
- Pilon fractures represent roughly 1-10% of lower-limb fractures and under 1% of all fractures worldwide.
- Bimodal distribution: high-energy axial loading in young males (falls from height, road traffic, occupational) and lower-energy rotational variants in older, often osteoporotic patients.
- Associated fibular fracture in 75-85% and open injury in 20-30% of high-energy patterns; incidence is rising with motorisation in low- and middle-income regions.
Side-by-side guidance (where societies differ in emphasis):
- Core Position
- Two-stage protocol: spanning external fixation then delayed staged ORIF once soft tissues recover; column-based reduction strategy.
- Core Position
- Open fractures: prompt IV antibiotics, combined ortho-plastic care, definitive skeletal and soft-tissue cover within 72h (often single-stage fix-and-flap at a specialist centre).
- Core Position
- Endorses staged management; mandatory CT after spanning fixation for articular planning; reduction quality emphasised as outcome driver.
- Core Position
- Recognises circular (Ilizarov / hexapod) fixation as a valid definitive alternative, especially with poor soft tissues or in limited-resource settings.
Registry & evidence notes:
- No implant registry tracks pilon plates the way arthroplasty registries track joints; outcome evidence comes from trauma cohorts and trials (Wyrsch, Sirkin, Pollak above).
- Anatomically pre-contoured locking plates are now standard in high-resource settings; large cohorts (e.g. circular-frame series) confirm high union rates with frames where plating is contraindicated.
High- vs Limited-Resource Practice Variation
- Well-resourced centres: Two-stage ORIF with CT planning, pre-contoured locking plates, ortho-plastic flap cover, prophylactic negative-pressure dressings.
- Limited-resource / remote settings: Definitive circular or hybrid external fixation is often preferred - it avoids implant cost, allows weight-bearing, and tolerates a compromised soft-tissue envelope. Where a peripheral hospital cannot offer definitive care, the principle is span and stabilise, then refer: apply a spanning external fixator (even a simple unilateral frame), give analgesia, elevate, document neurovascular and compartment status, give antibiotics and tetanus cover for open injuries, and transfer to a major trauma centre with CT and reconstructive capability.
Consent & Documentation (universal)
- Counsel every patient on the high complication burden: wound breakdown, infection, near-universal stiffness, post-traumatic arthritis and possible future arthrodesis, plus the alternatives (non-operative care, circular frame, primary fusion).
- Document neurovascular and compartment status before and after any reduction, antibiotic timing for open injuries, and clear return instructions for wound review and compartment-syndrome warning signs.
Controversies & Areas of Uncertainty
- Fibula fixation: Restores length and lateral column but adds a lateral incision and can lock in malreduction or compromise the skin bridge. Fix when planning a medial-based approach or when length is otherwise unrecoverable; consider leaving it when an anterolateral approach is planned.
- Definitive ORIF vs definitive circular frame: No high-quality trial proves superiority of one over the other for severe patterns. Frames avoid wound complications and allow loading but carry pin-site issues and patient burden. Choice is driven by soft tissues, comorbidities, surgeon expertise and resources.
- Optimal timing of ORIF: "Wait for the wrinkle sign" (typically 10-21 days) is widely taught, but the precise safe window is not standardised and depends on the individual soft-tissue response rather than a fixed day count.
- Four-column theory - must every column be fixed? A long-term cohort (Bakan 2023, Injury) found no functional or radiological difference between fully and partly supported columns in 43-C fractures, challenging the dogma that every fractured column needs its own implant.
- Primary arthrodesis vs reconstruction in non-reconstructable 43-C3 / elderly low-demand patients: arthrodesis trades motion for a durable, single-procedure outcome; the threshold for choosing it remains a matter of judgement.
- Early weight-bearing: Permitted with stable circular frames; after plate ORIF it remains cautious and is not yet supported by robust comparative data.
- Adjuncts of uncertain benefit: Prophylactic negative-pressure wound therapy over incisions and vitamin C for CRPS prevention have plausible mechanisms but limited high-level evidence.
MCQ Practice Points
Q: Which column of the distal tibia typically includes the Tillaux-Chaput tubercle? A: Anterolateral Column.
Q: What is the 'Mercedes Benz Sign' on CT axial view? A: The confluence of fracture lines separating the Medial, Anterolateral, and Posterior fragments.
Q: What is the most common long-term complication of Type III Pilon fractures? A: Post-traumatic Osteoarthritis (PTOA).
Q: What is the minimum skin bridge required between anteromedial and anterolateral incisions? A: 7 cm. Less than this risks necrosis of the skin bridge.
Q: Which nerve is at risk during an Anterolateral approach? A: Superficial Peroneal Nerve (runs in subcutaneous fat layer).
Q: What is the staged protocol for Pilon fractures? A: Span (ExFix) → Scan (CT after reduction) → Plan (Choose approach based on fragments) → Fix (Wait for Wrinkle Sign, then ORIF). Definitive surgery typically at 10-21 days.
Q: What is the infection rate for open Pilon fractures? A: 10-15% deep infection rate, despite staged protocol. Requires early debridement, antibiotics, and often free flap coverage for Grade IIIB.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 40-year-old male presents with a Grade 3B open Pilon fracture 6 hours after a motorbike crash. Soft tissue loss medial side.”
“Referral tells you: 'It's just an ankle fracture, can you admit?' You see the X-ray is a comminuted Pilon.”
“An 82-year-old female, multiple comorbidities (NIDDM, CAD), presents with a Type C3 Pilon fracture after a fall from standing. Swelling is significant.”
Key Concepts
- Axial Load Mechanism
- Soft Tissue dictates timing
- Span, Scan, Plan
- 3 Column Fixation
Emergency Steps
- Reduce
- Spanning ExFix (Delta)
- CT Scan
- Elevate x 14 days
X-ray Signs
- Articular step-off
- Metaphyseal impaction
- Mercedes Benz Sign (Axial CT)
- Double Contour sign
Complications
- Wound Breakdown (Disaster)
- Infection
- Arthritis (Inevitable?)
- Varus Malunion
Evidence
ORIF vs External Fixation (Landmark RCT)
- Randomized prospective study of 39 tibial plafond fractures (17 type III, 10 open).
- ORIF group had 15 complications in 7 patients vs 4 complications in the external fixation group; complications after ORIF were more severe.
- Three amputations, all in the ORIF group.
- No significant difference in clinical score or radiographic osteoarthritis between groups; all type II/III fractures developed some OA.
Staged Protocol for Soft-Tissue Management
- 56 fractures: immediate fibular ORIF plus spanning external fixator, then delayed plating once swelling subsided (mean 12.7 days closed, 14 days open).
- Closed fractures: all wounds healed; 17% partial-thickness necrosis treated non-operatively; one late osteomyelitis (3.4%).
- Open fractures: two deep infections (10.5%), including one below-knee amputation.
- No skin grafts, rotation flaps or free transfers required for the surgical wounds.