Extra Digit Formation
Polydactyly Types
Critical Must-Knows
- Preaxial: Thumb duplication - use Wassel classification (I-VII).
- Postaxial: Small finger - Type A (well-formed) vs Type B (rudimentary).
- Wassel IV: Most common thumb type - duplicated proximal phalanx.
- Bilhaut-Cloquet: Combine two equally hypoplastic thumbs into one (Wassel I/II).
- Retain the more functional digit: Usually the ulnar thumb.
Clinical Pearls
- "Wassel IV = Most common thumb duplication
- "Postaxial more common in African descent
- "Type B postaxial can ligate in nursery
- "Bilhaut-Cloquet for equal hypoplastic thumbs
- "Reconstruct collateral ligaments - critical
Clinical Imaging
Imaging Gallery




Wassel Classification - KNOW THIS
Wassel classification for thumb duplication (Roman numerals I-VII):
- Based on level of bifurcation from DISTAL to PROXIMAL
- Odd numbers = bifid (shared element)
- Even numbers = duplicated (separate elements)
- Wassel IV (duplicated proximal phalanx) is MOST COMMON
- Wassel VII is triphalangeal thumb component
At a Glance
Polydactyly is congenital duplication of digits, classified as preaxial (thumb/radial), postaxial (small finger/ulnar), or central. Preaxial is more common in Caucasians; postaxial is common in African descent (1:300). For thumb duplication, the Wassel classification (I-VII) is essential: odd numbers indicate bifid elements, even numbers indicate duplicated elements. Wassel IV (duplicated proximal phalanx) is most common. Surgery at 12-18 months: retain the more functional digit (usually ulnar thumb) and reconstruct collateral ligaments. Postaxial Type B (rudimentary) can be ligated in nursery; Type A requires formal excision.
Polydactyly Quick Decision Guide
| Type | Features | Surgery Timing | Key Surgical Point |
|---|---|---|---|
| Duplicated proximal phalanx | 12-18 months | Reconstruct collateral ligaments | |
| Well-formed digit with bone | 12-18 months | Formal surgical excision | |
| Rudimentary/pedunculated | Nursery ligation OR 6-12mo formal | Neuroma risk with ligation | |
| Two equally hypoplastic thumbs | 12-18 months | Bilhaut-Cloquet procedure |
WASSEL CWASSEL Classification Memory
| W | Wassel IV Most common type (43%) |
| A | Articulation Level determines type |
| S | Shared = Odd I, III, V are bifid |
| S | Separate = Even II, IV, VI are duplicated |
| E | Excise hypoplastic Retain better thumb |
| L | Ligaments Reconstruct collaterals |
| W | Wassel IV Most common type (43%) | S | Shared = Odd I, III, V are bifid | E | Excise hypoplastic Retain better thumb |
| A | Articulation Level determines type | S | Separate = Even II, IV, VI are duplicated | L | Ligaments Reconstruct collaterals |
Hook:WASSEL: Wassel IV most common, Articulation level determines type, Shared (odd) vs Separate (even), Excise hypoplastic, reconstruct Ligaments
EVEN WODD vs EVEN Wassel Types
| O | Odd numbers I, III, V = BIFID (shared) |
| E | Even numbers II, IV, VI = DUPLICATED (separate) |
| O | Odd numbers I, III, V = BIFID (shared) |
| E | Even numbers II, IV, VI = DUPLICATED (separate) |
Hook:ODD = bIfId (shared element), EVEN = sEparatE (duplicated)
THUMB STHUMB Selection for Retention
| T | Thenar muscles Better bulk = better thumb |
| H | Heavier/Larger Bigger thumb usually retained |
| U | Ulnar Usually the better thumb |
| M | Motion Better active movement |
| B | Better FPL Flexor insertion critical |
| T | Thenar muscles Better bulk = better thumb | M | Motion Better active movement |
| H | Heavier/Larger Bigger thumb usually retained | B | Better FPL Flexor insertion critical |
| U | Ulnar Usually the better thumb |
Hook:THUMB: The ulnar thumb is usually retained - Thenar bulk, Heavier, Ulnar, Motion, Better FPL
Overview and Epidemiology
Polydactyly is the congenital duplication of digits, one of the most common congenital hand anomalies.
Epidemiology
- Overall Incidence: 1-2 per 1,000 live births
- Preaxial (Thumb): More common in Caucasians and Asians
- Postaxial (Small Finger): 10x more common in African descent (1:300)
- Central: Rare (1:100,000)
Genetics and Inheritance
- Postaxial: Often autosomal dominant with variable penetrance
- Preaxial: Usually sporadic, can be autosomal dominant
- Associated Syndromes: Holt-Oram, Ellis-van Creveld, trisomy 13
Embryology
- Develops during limb bud formation (4-8 weeks gestation)
- Sonic Hedgehog (SHH) signalling pathway involved
- Zone of Polarising Activity (ZPA) regulates digit formation
- Duplication from abnormal signalling in limb bud
Pathophysiology
Polydactyly is a disorder of anterior-posterior (radial-ulnar) axis patterning in the developing limb bud, not a mechanical splitting of a normal digit.
Molecular Basis
- SHH-ZPA axis: The zone of polarising activity at the posterior (ulnar) limb-bud margin secretes Sonic Hedgehog (SHH), establishing the radial-ulnar gradient that specifies digit identity and number.
- ZRS dysregulation: SHH expression is controlled by a distant cis-regulatory element, the ZPA regulatory sequence (ZRS) within intron 5 of LMBR1 at 7q36.3. Point mutations or copy-number gains of the ZRS cause ectopic anterior (radial) SHH activity, producing preaxial polydactyly and triphalangeal thumb.
- GLI3 and the SHH-GLI axis: Loss-of-function in GLI3 (a downstream SHH effector and repressor) underlies postaxial and central polydactyly, including Greig and Pallister-Hall syndromes.
- HOXD13: Expansion/mutation produces synpolydactyly (central duplication fused with syndactyly).
From Signal to Phenotype
- Ectopic or excess SHH activity expands the digit field, generating a supernumerary ray.
- The level at which the supernumerary skeletal element separates (distal phalanx to metacarpal) determines the Wassel type for the thumb.
- Shared versus separate elements (bifid vs duplicated) reflect how early in ray condensation the duplication occurred.
- Because the duplicated ray shares tendons, ligaments and neurovascular structures with the dominant ray, neither thumb is fully normal, which is why simple ablation without soft-tissue rebalancing fails.
Inheritance Correlate
- Isolated postaxial Type B is typically autosomal dominant with variable penetrance (often GLI3-related).
- Preaxial duplication is usually sporadic, but ZRS-related forms (triphalangeal thumb-polysyndactyly) are autosomal dominant.
Anatomy and Biomechanics
Thumb Anatomy
- Unique Features: Thumb has 2 phalanges (vs 3 in fingers)
- Triphalangeal Thumb: Wassel VII has 3 phalanges - abnormal
- FPL Insertion: Critical for thumb function - inserts on distal phalanx
- Thenar Muscles: APB, FPB, OP provide thumb opposition
Key Anatomical Considerations in Thumb Duplication
- Metacarpal: May be single (Wassel I-V) or duplicated (Wassel VI)
- Growth Plates: Preserve physis during surgery to maintain growth
- Collateral Ligaments: Essential for joint stability - MUST reconstruct
- Neurovascular Bundle: Each thumb has its own digital nerves/arteries
Biomechanics of the Thumb
- Opposition: Unique to thumb - enables pinch grip
- Stability: UCL and RCL provide MCP joint stability
- Angular Deformity: Occurs if asymmetric ligament support
- Growth: Unequal growth can cause progressive deformity
Postaxial Anatomy
- Small Finger UCL: Critical for power grip
- Hypothenar Muscles: ADM, FDM, ODM provide small finger function
- Type A: Has articulation with 5th metacarpal
- Type B: Minimal bone - mainly skin bridge
Classification Systems
Wassel Classification (I-VII)
Principle: Higher number = more proximal duplication
Wassel Classification - Thumb Duplication
| Type | Level of Bifurcation | Frequency |
|---|---|---|
| Bifid distal phalanx (shared) | Rare (2%) | |
| Duplicated distal phalanx | 15% | |
| Bifid proximal phalanx (shared) | Rare (6%) | |
| Duplicated proximal phalanx | MOST COMMON (43%) | |
| Bifid metacarpal (shared) | Uncommon (10%) | |
| Duplicated metacarpal | Rare (4%) | |
| Triphalangeal thumb component | Rare (20%) |
Remember:
- Odd numbers = Bifid (shared element)
- Even numbers = Duplicated (separate elements)
- Wassel IV is the EXAM answer for most common type
The Wassel classification provides a systematic approach to describing thumb duplication patterns.
Wassel IV - Most Common
Wassel IV represents duplicated proximal phalanx - meaning two complete proximal phalanges articulating with a single metacarpal. This occurs in 43% of thumb duplications. The ulnar thumb is usually more functional (better FPL insertion) and is retained, while the radial thumb (often more hypoplastic) is excised.
Clinical Assessment
History
- Family history: Especially for postaxial (autosomal dominant)
- Pregnancy history: Maternal diabetes, teratogens
- Syndromic features: Cardiac, renal anomalies
- Functional concerns: Parents' goals, cosmetic concerns
Physical Examination
Inspection
- Location: Preaxial, postaxial, central
- Size: Well-formed vs rudimentary
- Skin bridge width (Type B)
- Associated syndactyly
Function
- Active movement of each thumb
- Thenar muscle bulk
- Stability assessment
- Grip pattern
Associated Features
- Cardiac murmur (Holt-Oram)
- Syndactyly (central)
- Other limb anomalies
- Facial dysmorphism
Key Examination Points for Thumb Duplication
- Which thumb is dominant? (usually ulnar)
- FPL insertion: Which thumb has better flexor function?
- Thenar muscles: Which side has better bulk?
- Stability: MCP and IP joint stability
- Size comparison: Often radial thumb is hypoplastic
Investigations
Imaging
- X-ray: Essential for surgical planning
- Level of bifurcation/duplication
- Bony anatomy of each digit
- Joint articulation
- Metacarpal morphology
When to Consider Further Investigation
- Cardiac echo: Holt-Oram syndrome (radial anomalies + ASD/VSD)
- Renal ultrasound: Associated GU anomalies
- Genetic testing: If syndromic features
Associated Syndromes
Syndromes with Polydactyly
| Syndrome | Polydactyly Type | Key Features |
|---|---|---|
| Preaxial | Radial dysplasia, ASD/VSD | |
| Postaxial | Short stature, cardiac defects | |
| Postaxial | Multiple malformations, poor prognosis | |
| Postaxial | Obesity, retinitis pigmentosa, renal |
Differential Diagnosis
Not every extra or broad digit is a simple duplication. The following entities must be distinguished because they change the operation and the counselling.
Distinguishing Polydactyly from Mimics
| Condition | Key Distinguishing Feature | Why It Matters |
|---|---|---|
| Two thumb skeletal elements sharing or duplicating at one level | Standard excision-plus-reconstruction | |
| Three phalanges in the thumb ray (extra middle phalanx), often delta-shaped | May coexist with duplication (Wassel VII); needs wedge/middle-phalanx excision, not simple ablation | |
| Central duplication fused within a syndactyly (HOXD13) | Shared tendons/neurovascular structures; staged complex reconstruction | |
| One enlarged digit, not a duplicate (lipofibromatous/PIK3CA overgrowth) | Debulking or epiphysiodesis, not duplication surgery | |
| Multiple symmetrical fingers, no thumb, duplicated ulna | Pollicisation and digit reduction, a wholly different plan | |
| Type A has bone and a true joint; Type B is a skin pedicle | Type A always needs formal excision; only true Type B is amenable to ligation |
Management Algorithm
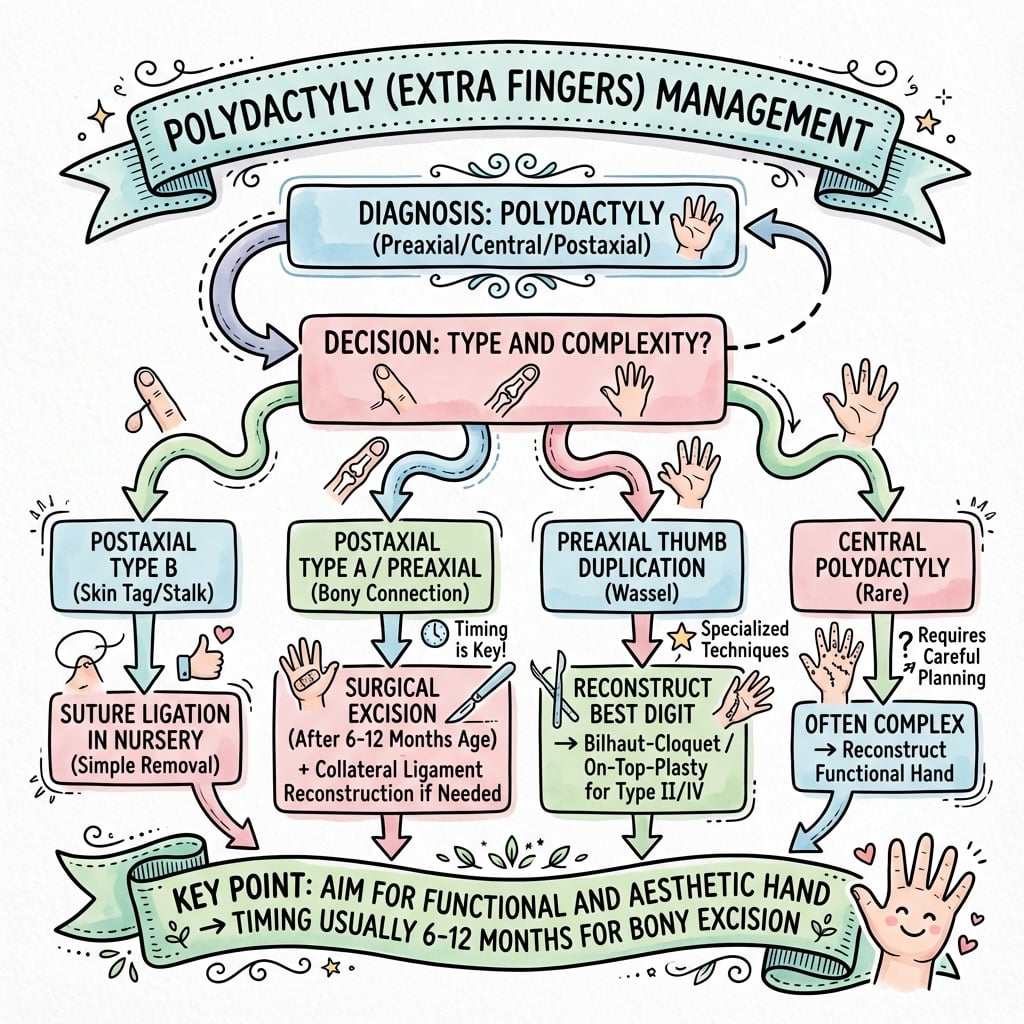
Management Decision Tree
Step 1: Identify Type
- Preaxial (thumb) → Wassel classification
- Postaxial (small finger) → Type A vs Type B
- Central → Complex reconstruction planning
Step 2: Timing Decision
- Preaxial: 12-18 months (optimal)
- Postaxial Type A: 12-18 months
- Postaxial Type B: Nursery ligation vs 6-12 months formal excision
Step 3: Surgical Planning
- Assess which digit to retain (preaxial)
- Plan incision design
- Anticipate need for ligament/tendon reconstruction
- Consider Bilhaut-Cloquet if both thumbs equally hypoplastic
The management approach is individualized based on type and functional considerations.
Surgical Technique
Thumb Duplication Surgery
Surgical Technique:
- Racquet incision around hypoplastic thumb
- Identify and preserve neurovascular bundle to retained thumb
- Detach collateral ligament from hypoplastic thumb
- Detach FPL/EPL if inserting on hypoplastic thumb
- Excise hypoplastic thumb with its metacarpal portion if needed
- Reconstruct collateral ligament to retained thumb
- Transfer/balance tendons
- Correct any angular deformity
Special Cases:
- Bilhaut-Cloquet: Combine two equally hypoplastic thumbs
- Used for Wassel I/II with equal thumbs
- Create one thumb from nail, bone, and soft tissue of both
The key to successful surgery is meticulous soft tissue reconstruction.
Critical Surgical Pearls
Must reconstruct collateral ligaments - failure to do so results in an unstable thumb. Always check joint stability intraoperatively after reconstruction. Consider osteotomy if angular deformity persists after ligament reconstruction.
EXCISE - SEXCISE - Surgical Principles
| E | Evaluate Assess which thumb is dominant |
| X | X-ray Confirm level of duplication |
| C | Collateral Reconstruct ligaments |
| I | Intrinsics Transfer thenar muscles |
| S | Stability Check joint stability |
| E | Epiphysis Preserve growth plate |
| E | Evaluate Assess which thumb is dominant | C | Collateral Reconstruct ligaments | S | Stability Check joint stability |
| X | X-ray Confirm level of duplication | I | Intrinsics Transfer thenar muscles | E | Epiphysis Preserve growth plate |
Hook:EXCISE: Evaluate dominance, X-ray, Collateral ligament repair, Intrinsic transfer, Stability check, Epiphysis preservation
Complications
Early Complications
- Wound infection: 1-2% incidence
- Flap necrosis: Avoid excessive tension
- Nerve injury: Digital nerve at risk
- Vascular compromise: Ensure perfusion intraoperatively
Late Complications
Joint Instability
Most Common Complication
- Inadequate ligament reconstruction
- Angular deformity progression
- Requires revision surgery
- Prevention: meticulous technique
Angular Deformity
Progressive Malalignment
- Growth-related
- Asymmetric growth plate injury
- May need corrective osteotomy
- Monitor during growth
Nail Deformity
Cosmetic Issue
- Bilhaut-Cloquet: central ridge
- Small/hypoplastic nail
- May need nail bed reconstruction
- Usually cosmetic only
Revision Surgery Requirements
- 15-20% may need secondary procedures
- Collateral ligament reconstruction most common
- Corrective osteotomy for angular deformity
- Tendon rebalancing
- Web space deepening
Postoperative Care and Rehabilitation
Immediate Postoperative (0-2 weeks)
- Splinting: Thumb spica or volar splint
- Wound care: Keep clean and dry
- Elevation: Reduce swelling
- Pain management: Paracetamol typically sufficient
Early Phase (2-6 weeks)
- Suture removal: 2 weeks postoperatively
- Splint weaning: Gradual reduction
- Gentle ROM: Passive then active
- Monitor for: Infection, stiffness
Late Phase (6 weeks to 6 months)
- Full ROM exercises: Encourage normal use
- Strengthening: Age-appropriate activities
- Monitor growth: Assess for angular deformity
- Occupational therapy: If functional concerns
Long-term Follow-up
- Monitor through growth: Annual assessments until skeletal maturity
- Assess stability: Check ligament integrity
- Functional assessment: Pinch, grip strength
- Consider revision: If progressive deformity or instability
Outcomes and Prognosis
Expected Outcomes
Thumb Duplication:
- Good functional outcomes in most cases
- Some residual instability common
- May have slightly smaller thumb than normal side
- May need secondary procedures (15-20%)
Postaxial Polydactyly:
- Excellent outcomes with proper technique
- Type B ligation: Risk of neuroma, bump
- Type A excision: Low complication rate
Prognostic Factors
Factors Affecting Outcome
| Factor | Good Prognosis | Poor Prognosis |
|---|---|---|
| Simple duplication | Complex with bone involvement | |
| Ligament reconstruction done | Ligaments not reconstructed | |
| 12-18 months | Delayed beyond 24 months | |
| Pediatric hand specialist | General surgeon |
Patient Satisfaction
- High satisfaction rates overall
- Cosmetic concerns more common than functional
- Realistic expectations important
- Secondary procedures may be needed
Controversies and Areas of Uncertainty
These are common viva escalation points. Take a position but acknowledge the evidence is limited.
- Nursery suture ligation vs formal excision (Type B postaxial): Ligation is convenient and avoids anaesthesia, but the systematic-review signal favours excision, with reported complication rates as high as 23.5% (residual bump, neuroma) for ligation versus around 3% for excision. Surgical-clip application is a middle ground for narrow-based digits. There is no high-level randomised evidence, so practice varies by resource setting and surgeon preference.
- Management of near-symmetric Wassel IV thumbs: When the two thumbs are nearly equal in size, simple excision-plus-reconstruction yields worse JSSH outcomes. Whether Bilhaut-Cloquet, combination (on-top plasty) procedures, or accepting a smaller thumb is best remains debated; the symmetry index is an emerging predictive tool rather than a validated decision rule.
- Bilhaut-Cloquet vs its modifications: The classic procedure reliably creates a stable, wide thumb but is criticised for IP joint stiffness (it crosses the physis), a central nail ridge and a broad appearance. Modified Bilhaut, neurovascular island-flap pulp/nail augmentation and combination techniques aim to mitigate these, but comparative evidence is sparse.
- Limitations of the Wassel classification: It poorly captures the immature epiphysis, triphalangeal components and soft-tissue anatomy. The OMT framework addresses categorisation but the thumb-specific Wassel scheme persists for surgical planning; intra- and inter-observer reliability of subtypes is imperfect.
- Optimal timing: 12-18 months is conventional but not evidence-mandated; some centres operate slightly earlier for technical convenience or later where access is constrained, with no clear functional penalty within the first few years.
Evidence Base
- Original classification of the duplicate thumb based on level of skeletal duplication
- Seven types described from distal (bifid distal phalanx) to proximal (duplicated metacarpal), with the triphalangeal variant designated Type VII
- Type IV (duplication at the metacarpophalangeal level) reported as the most common pattern
- Provided the anatomical framework that still underpins surgical planning
- Editorial synthesis of contemporary thumb duplication classification and terminology
- Highlights limitations of the original Wassel scheme, particularly misclassification of the immature epiphysis and failure to capture soft-tissue and triphalangeal variants
- Supports integration of duplication within the Oberg-Manske-Tonkin (OMT) framework adopted by the IFSSH
- Reinforces that classification should guide, not replace, individualised soft-tissue assessment
- Comprehensive review of radial (preaxial) polydactyly genetics, classification and surgery
- Confirms Wassel as the universal classification and notes misclassification of the immature epiphysis as its key limitation
- Defines three surgical objectives: thumb alignment, stability and acceptable aesthetic appearance
- Identifies the Tada score and the JSSH assessment system as validated functional outcome measures
- Forty-seven radial polydactylies reviewed with JSSH scores at mean 4.6 years
- All fair or poor outcomes (score under 17) occurred in Wassel type IV thumbs
- Symmetry of the two thumbs (symmetric index) was the only independent predictor of outcome in type IV
- A symmetric index over 0.74 predicted greater risk of a fair or poor result
- PRISMA systematic review of suture ligation versus surgical excision for postaxial (ulnar) polydactyly
- Ten studies met inclusion criteria from 900 screened, with substantial heterogeneity
- Largest cohort reported a complication rate of 23.5% for suture ligation versus 3% for surgical excision
- Residual remnants and neuromas were the principal ligation complications
- Retrospective review of 231 hands (132 newborns) with Type B postaxial polydactyly treated by surgical clip application
- No wound complications recorded with minimum two-year follow-up
- Only 7 percent required later scar revision
- Clip application performed at the bedside or outpatient setting as a low-cost alternative
- Six-year literature review of congenital upper-limb differences
- Confirms the Oberg-Manske-Tonkin (OMT) classification, endorsed by the IFSSH, as the current standard framework
- Notes ongoing refinement as genetic and embryonic understanding improves
- Emphasises good peer relationships and adaptability in affected children
- Reports a 7q36.3 microduplication encompassing the ZRS, the long-range cis-regulator of SHH
- Associated with triphalangeal thumb-polysyndactyly syndrome (preaxial polydactyly with duplicated distal phalanx and hallux duplication)
- Confirms that copy-number gain of the ZRS dysregulates SHH expression in the zone of polarising activity (ZPA)
- A coincident 22q11.21 deletion accounted for the associated congenital heart disease
Viva Scenarios
Use these scenarios to practise clinical reasoning and management decisions
Wassel IV Thumb Duplication
"10-month-old child presents with bilateral thumb duplication. X-rays show Wassel IV bilaterally. Parents ask about treatment. What is your management?"
Postaxial Polydactyly - Type Selection
"Newborn of African descent has bilateral pedunculated extra digits on ulnar side of hands. Midwife asks about suture ligation in nursery. What is your advice?"
Bilhaut-Cloquet Indication
"6-month-old with Wassel I thumb duplication - two equally small thumbs with bifid distal phalanx. Neither appears adequate alone. What are your options?"
MCQ Practice Points
Most Common Wassel Type
Q: A 1-year-old child presents with bilateral thumb duplication. What is the most common Wassel classification type?
A: Wassel Type IV (duplicated proximal phalanx) - occurs in 43% of thumb duplications. Remember: even numbers = duplicated (separate elements), odd numbers = bifid (shared elements). Wassel IV has two complete proximal phalanges articulating with a single metacarpal.
Postaxial Polydactyly Epidemiology
Q: What is the incidence of postaxial polydactyly in people of African descent, and what is the inheritance pattern?
A: 1 in 300 in African descent (compared to 1 in 3,000 in Caucasians). Inheritance is typically autosomal dominant with variable penetrance. It is 10 times more common than in other populations.
Surgical Timing for Polydactyly
Q: What is the optimal timing for surgical correction of preaxial (thumb) polydactyly and why?
A: 12-18 months is optimal. This timing allows adequate size for surgical manipulation, is performed before functional hand patterns are established, and occurs before the child's memory of surgery. Operating too early (less than 6 months) makes surgery technically difficult due to small structures.
Critical Surgical Step
Q: What is the most critical step in thumb duplication surgery that, if omitted, leads to the most common complication?
A: Reconstruction of the collateral ligaments. Failure to reconstruct the radial or ulnar collateral ligament from the excised thumb to the retained thumb results in joint instability - the most common complication requiring revision surgery.
Bilhaut-Cloquet Indication
Q: What is the indication for the Bilhaut-Cloquet procedure, and what is the main disadvantage?
A: Indicated for Wassel Type I or II with two equally hypoplastic thumbs where neither is adequate alone. The main disadvantage is IP joint stiffness because the procedure crosses the physis. Also expect a central nail ridge deformity and wide thumb appearance.
Postaxial Type B Controversy
Q: A newborn has a rudimentary pedunculated extra digit (Type B postaxial polydactyly). What are the two management options and their respective risks?
A: (1) Suture ligation in nursery (traditional): Risks include incomplete removal, neuroma formation, and unsightly bump/scar. (2) Formal surgical excision at 6-12 months (preferred by many): Allows complete removal under vision with proper nerve division and better cosmetic result. Many hand surgeons now prefer formal excision despite the need for general anaesthetic.
Associated Syndromes
Q: A child with preaxial polydactyly is found to have an atrial septal defect. What syndrome should you consider, and what other features would you look for?
A: Holt-Oram syndrome - characterized by radial ray anomalies (including preaxial polydactyly) with cardiac defects (ASD/VSD). Other features include radial dysplasia, hypoplastic or absent thumb, and other upper limb anomalies. Cardiac echo is essential in all patients with radial-sided upper limb anomalies.
Which Thumb to Retain
Q: In Wassel IV thumb duplication, which thumb is typically retained and why?
A: The ulnar thumb is usually retained because it typically has: (1) Better FPL insertion and function, (2) Greater thenar muscle bulk, (3) Larger size, (4) Better active movement. The radial thumb is often more hypoplastic. However, always assess each case individually based on function.
Secondary Surgery Rate
Q: What percentage of patients require secondary surgery after thumb duplication correction, and what are the common reasons?
A: 15-20% require secondary procedures. Common reasons include: (1) Joint instability from inadequate ligament reconstruction, (2) Angular deformity from growth, (3) Tendon imbalance, (4) Web space narrowing. Parents should be counselled about this possibility preoperatively.
Odd vs Even Wassel Numbers
Q: How do you remember the difference between odd and even Wassel classification numbers?
A: ODD = bIfId (shared element) - Types I, III, V have a bifid bone where digits share a single element. EVEN = sEparatE (duplicated) - Types II, IV, VI have completely duplicated separate elements. Wassel IV (even) = duplicated PP, Wassel III (odd) = bifid PP.
Guidelines, Registries & Global Practice
Polydactyly is a clinical, not registry-tracked, condition, so practice is guided by national society reviews and IFSSH consensus rather than arthroplasty-style registries. The descriptive framework is converging worldwide on the Oberg-Manske-Tonkin (OMT) classification, endorsed by the IFSSH, with the Wassel (Wassel-Flatt) scheme retained for the thumb.
Global Epidemiology
- Overall: one of the most common congenital hand anomalies, roughly 1-2 per 1,000 live births worldwide.
- Postaxial (ulnar): markedly more frequent in populations of African ancestry (around 1 in 150-300), where it is often isolated and autosomal dominant; far less common (around 1 in 1,500-3,000) and more often syndromic in those of European ancestry.
- Preaxial (radial/thumb): more common in East Asian and white populations; usually sporadic and unilateral.
- Central: rare in all populations and frequently associated with syndactyly (synpolydactyly).
Side-by-Side Society Guidance
How Major Bodies Frame Polydactyly Care
| Body / Region | Classification Emphasis | Practice Position |
|---|---|---|
| OMT classification as unifying framework; Wassel retained for thumb | Promotes consistent terminology to enable cross-centre comparison | |
| Wassel-Flatt for thumb; Stelling-Turek A vs B for postaxial | Increasing shift from nursery suture ligation toward formal excision for Type B | |
| OMT and Wassel; specialist congenital hand network referral | Centralised paediatric hand surgery; collateral ligament reconstruction stressed | |
| OMT-based; emphasis on validated outcome scoring (JSSH/Tada) | Surgery in infancy by paediatric hand specialists |
High- vs Limited-Resource Practice Variation
- High-resource settings: subspecialist paediatric hand surgery, day-case excision at 12-18 months, microsurgical capability for Bilhaut-Cloquet and on-top plasty, formal outcome scoring (JSSH/Tada), genetic counselling and cardiac/renal screening for syndromic cases.
- Limited-resource settings: nursery suture ligation or surgical-clip application remains widely used for narrow-based Type B digits because it avoids general anaesthesia and theatre access; families may present late, so reconstruction is performed at an older age. Awareness of the higher residual-bump and neuroma rate with ligation should still inform consent.
- Universal principle: regardless of resources, palpable bone or a broad base reclassifies a digit as Type A (or wide Type B) and mandates formal excision rather than ligation.
POLYDACTYLY
Clinical summary
WASSEL CLASSIFICATION
- •I-VII: Distal to proximal bifurcation
- •IV = MOST COMMON (43%) - duplicated PP
- •ODD (I, III, V) = BIFID (shared)
- •EVEN (II, IV, VI) = DUPLICATED (separate)
- •VII = Triphalangeal thumb
POSTAXIAL TYPES
- •Type A: Well-formed with articulation
- •Type B: Rudimentary/pedunculated
- •1:300 in African descent
- •Autosomal dominant inheritance
- •Type B ligation controversial
THUMB SURGERY PRINCIPLES
- •Timing: 12-18 months
- •Retain more functional (usually ulnar)
- •RECONSTRUCT COLLATERAL LIGAMENTS
- •Transfer intrinsics from excised thumb
- •Correct angular deformity
BILHAUT-CLOQUET
- •For Wassel I/II equal thumbs
- •Combines both thumbs into one
- •Expect IP stiffness
- •Nail ridge deformity
- •Reserve for specific cases
ASSOCIATED SYNDROMES
- •Holt-Oram: Preaxial + ASD/VSD
- •Ellis-van Creveld: Postaxial + cardiac
- •Trisomy 13: Postaxial + poor prognosis
- •Bardet-Biedl: Postaxial + obesity + retinal
COMPLICATIONS
- •Joint instability (most common)
- •Angular deformity
- •15-20% need secondary surgery
- •Type B ligation: neuroma risk
- •Bilhaut: IP stiffness expected